
Abstract
Background:
The management of revision anterior cruciate ligament reconstruction (ACLR) presents unique challenges that require careful consideration of graft selection and the role of anterolateral complex (ALC) augmentation. Although surgical techniques continue to evolve, there is variability in clinical practice patterns for revision ACLR.
Purpose:
To assess current trends in revision ACLR, including ALC augmentation indications, preferred augmentation techniques, and choice of graft type.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A survey was distributed by email to all members of the American Orthopaedic Society for Sports Medicine (AOSSM). The survey included a demographics section (5 questions) and a revision ACLR section (12 questions). Descriptive statistics were performed.
Results:
There were 469 responses (response rate, 14%), with respondents more commonly being male (90%), fellowship-trained (95%), and in private practice (42%). The revision ACLR volume rose with the number of years in practice (P = .008). The autograft patellar tendon (47%) was the most frequently selected revision graft, followed by the quadriceps tendon (22%). The graft choice was associated with fellowship training (P = .006), years of experience (P < .001), and type of practice (P = .015). ALC augmentation was used by 70% of respondents, mostly for multiple (52%) or single (37%) previous ACLR failures and contact athlete status (17%). Its use was more common among early-career (88%; P = .006) and academic (87%; P < .001) surgeons. Practice setting correlated with the choice between lateral extra-articular tenodesis (LET) and anterolateral ligament reconstruction (ALL) (P = .03), with academic surgeons utilizing LET at the highest rate. ALL was favored in patients with a body mass index of >35 kg/m2 (P = .003) and LET in contact sport athletes (P = .006). Altogether, 80% of the surgeons preferred LET over ALL as their primary choice for augmentation.
Conclusion:
Revision ACLR practices vary widely, with no uniform consensus on graft choice and indications for ALC augmentation. ALC augmentation is most frequently indicated for patients with multiple previous failures. LET is the preferred augmentation technique, and the autograft patellar tendon is the most utilized graft in revision ACLR. Long-term outcomes of revision ACLR should be further studied to define ideal indications for augmentation and graft selection to address the relatively poor outcomes observed in patients undergoing revision ACLR.
Anterior cruciate ligament reconstruction (ACLR) is a common procedure performed in orthopaedic sports medicine. Each year, 120,000 reconstructions are performed in the United States.1,13,14 The incidence of failure varies from 3% up to 27%, which often necessitates revision ACLR.5,15,22 Revision ACLR produces inferior results when compared with primary ACLR. Revision patients have higher postoperative instability, higher reinjury rates, and lower return-to-sport rates.6,16,24 The continual improvement of revision ACLR technique remains a focus in sports medicine.
Anterolateral complex (ALC) augmentation has gained support as a strategy for increasing rotational stability of the knee and decreasing the risk of graft failure in high-risk ACLR patients. 21 Lateral extra-articular tenodesis (LET) and anterolateral ligament reconstruction (ALL) are ALC augmentation techniques that have been reported to increase knee stability and decrease graft rupture rates in patients with grade ≥2 pivot shifts or ≥1 previous ACL failure.7,9,18 Currently, there is wide variability in utilization, with no agreement on indications for extra-articular reconstruction and when to use LET over ALL. The optimal graft choice is also ill-defined in revision ACLR. In general, an autograft tendon is preferable to an allograft. However, current graft types (eg, bone-patellar tendon-bone, hamstring tendon, and quadriceps tendon) each have advantages and disadvantages dependent upon surgeon preference and patient factors. 23 Current trends for ALC augmentation in revision ACLR are not well described in the literature.
This study surveyed AOSSM membership orthopaedic surgeons to assess current indications for ALC augmentation, surgeon preferences for augmentation technique, graft selection, and factors influencing these decisions. We hypothesized that surgeon preference for augmentation technique and graft selection would be associated with their fellowship training, years in practice, and practice setting, and excess anterolateral instability—defined as laxity on pivot shift testing—would be an indication for ALC augmentation.
Methods
An online survey was sent by email on January 21, 2022, to participants of the AOSSM. One reminder email was sent 2 weeks later, on February 4, 2022, to increase the response rate. The survey was open for 1 year. All study procedures were approved by the university institutional review board (STUDY00147733). All participants signed a consent form, and no exclusion criteria were used. The AOSSM is a national society representing over 3600 orthopaedic sports medicine surgeons. After exclusion of invalid email addresses, the survey was sent to 3262 members. AOSSM members had the option not to participate.
The survey was created in English and administered via the software, REDCap (Research Electronic Data Capture). The study team developed the survey questions and went through an internal review by orthopaedic faculty at the University of Kansas Medical Center to verify content before distribution. No pretesting with a small cohort was performed due to the topics being descriptive questions regarding the respondents’ practice and individual decision-making. The survey contained 17 questions that were divided into 2 sections. A third section on return-to-sport rates was excluded from this analysis, as it is beyond the scope of the present study. There were 5 questions in the demographics section and 12 questions in the revision ACLR section. Survey questions pertaining to this study are listed in Appendix A, and the entire survey form can be found in the supplemental information. The survey was designed for AOSSM members who are primarily orthopaedic sports medicine surgeons. Participants were allowed to defer any question without providing a reason.
The raw data were stored in REDCap and imported into Excel (Microsoft) and R (R Foundation for Statistical Computing) for analysis. No power analysis was conducted beforehand since the aim was to collect the highest possible number of responses from a national sports medicine society. Surveys with unanswered questions were not excluded from the analysis. Results were analyzed by counts and percentages. Associations were calculated by chi-square or Fisher exact tests where appropriate. All statistical comparisons were made with significance set at α = .05.
Results
Demographic Characteristics and Clinical Practice
There were 469 respondents who completed the survey among 3262 contacted for participation (response rate, 14%). Most participants were male (90%), while female respondents made up 8% of the total. Nearly all respondents (95%) were fellowship trained. Respondents represented a wide range of clinical experience levels. The 2 most common groups were those with 6 to 10 years and 11 to 15 years of experience, each accounting for 20% of the total. Early career surgeons (0-5 years of experience) comprised 13% of the respondents, and 14% had >30 years of experience. Demographic information was not available for nonresponders in this study.
All major practice models were represented (Table 1). Private practice was the most common (42%), followed by academic institutions (27%) and hospital-employed surgeons (17%). Privademic practices, which combine academic and private factors, accounted for 11% of respondents. Solo practitioners were less represented at 3%.
Respondent Characteristics and Clinical Practice Responses a

Data are presented as n (%).
Practicing academic medicine within a private practice setting.
Revision ACLR
Years of practice were significantly associated with the number of revision ACLRs performed per year (P = .008), with the highest percentage of surgeons performing >25 revisions per year having >30 years in practice (43%), followed by those with 26 to 30 years (36%), 16 to 20 years (33%), and 11 to 15 years (28%). However, there was no correlation between practice environment and the number of revision ACLRs performed annually (P = .46). Fellowship training was correlated with the number of revision ACLRs performed annually, with 23% (104/447) of fellowship-trained surgeons reporting >25 cases compared with 41% (9/22) of non-fellowship-trained surgeons (P = .007).
A summary of revision ACLR responses can be found in Figure 1. The autograft patellar tendon was the most selected revision ACL graft type (47%). Graft selection varied significantly between fellowship-trained and non-fellowship-trained surgeons (P = .006). Autograft quadriceps tendon soft tissue was the second most common graft (22%), and only fellowship-trained surgeons opted for it. Moreover, practice setting and years of practice were also found to be associated with graft choice (P = .015 and P < .001, respectively). However, there were no discernible trends as the autograft patellar tendon remained the most frequent graft selected regardless of practice setting or years of practice.
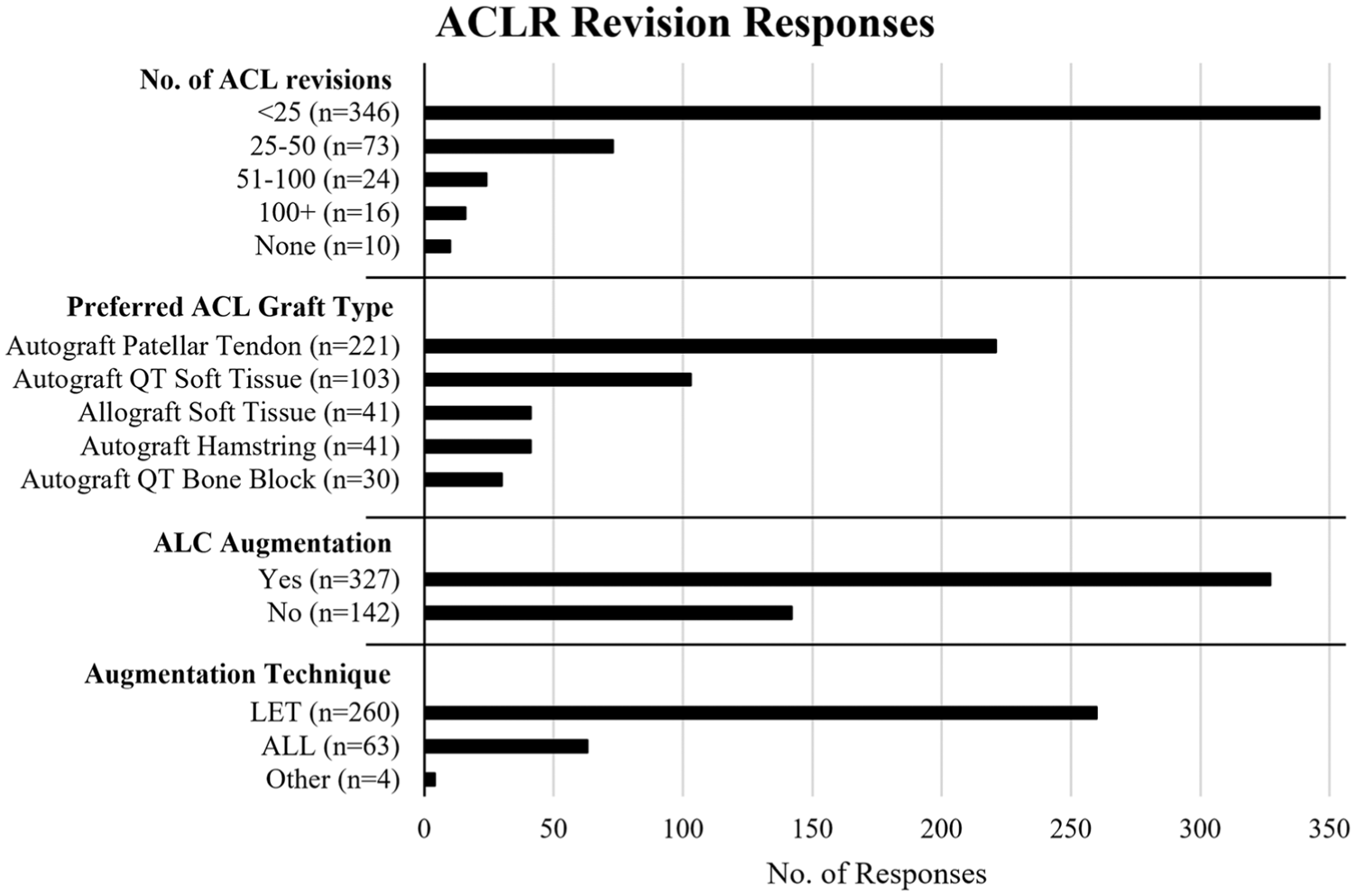
Summary of responses for annual volume of ACLR cases and associated graft choices/augmentation techniques. ACL, anterior cruciate ligament; ALC, anterolateral ligament complex; ALL, anterolateral ligament; LET, lateral extra-articular tenodesis; QT, quadriceps tendon.
Of participants, 70% (n = 327) reported performing ALC augmentation, and the technique was influenced by years in practice (P = .006). The highest proportion of surgeons who reported using augmentation was those with 0 to 5 years of experience (88%), followed by those with 6 to 10 years (76%), and those with 11 to 15 years and 26 to 30 years, at 70% each. Additionally, practice setting was associated with ALC augmentation use (P < 0.001), with academic surgeons demonstrating the highest rate of utilization (87%). The utilization of ALC augmentation did not differ significantly between fellowship-trained and non-fellowship-trained surgeons (P = .177).
Table 2 outlines current indications for ALC augmentation. In total, 80% (260/327) of surgeons favored LET over ALL as their augmentation method of choice. The choice of augmentation technique was influenced by the type of practice (P = .03), with academic practices showing the highest proportion of LET to ALL preference (7:1), followed by private practice (4:1). Also, the indications for ALC augmentation varied between the 2 techniques. Surgeons performing ALL were more likely to cite an elevated body mass index (BMI) >35 kg/m2 (P = .003) as an indication for the procedure, with 12% of ALL cases including it as a reason for ALL compared with 3% for LET. In contrast, contact athlete status was more frequently cited as an indication for LET (P = .006), with 37% citing this factor for LET compared with 1% in ALL. The most reported indications for ALC augmentation overall included multiple previous failed ACLR (52%), a single previous failed ACLR (37%), and contact athlete status (17%).
ALC Augmentation Indications a

ACLR, anterior cruciate ligament reconstruction; ALC, anterolateral ligament complex; ALL, anterolateral ligament; BMI, body mass index; LET, lateral extraarticular tenodesis.
P value calculated using the chi-square test.
P value calculated using the Fisher exact test.
Connective tissue disorders include, but are not limited to, Ehlers-Danlos syndrome and Marfan syndrome.
Among surgeons performing ALC augmentation, the preferred graft for the revision ACL was the autograft patellar tendon. A comparison between the LET and ALL groups showed a significant difference in graft preference (P = .013), with no definite trend (Figure 2).

Summary of preferred graft types for revision ACLR among surgeons performing ALL reconstruction or LET. ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; LET, lateral extra-articular tenodesis; QT, quadriceps tendon.
Discussion
The most important finding in this study is that orthopaedic sports medicine surgeons within AOSSM vary by practice setting, fellowship training, and years of practice in their approach to revision ACLR with ALC augmentation. ALC augmentation, both LET and ALL, was commonly performed (70%), with utilization impacted by type or practice and number of years in practice. The patellar tendon autograft was the most preferred graft type in revision ACLR (47%). The patellar tendon autograft is known for its low association with graft failure and infection, making it a preferred graft type for revision ACLR. 3 Consistent with previous literature, this study found that 47% of respondents selected the patellar tendon autograft for revisions.11,19 Indications for LET and ALL varied, with contact athlete status more frequently selected for LET, and elevated BMI (≥35 kg/m2) commonly indicated for ALL.
A limited number of clinical studies have investigated the effects of augmentation with revision ACLR. 8 Most existing research has primarily focused on augmentation in primary ACLR. While our study observed a high utilization rate of ALC augmentation, other studies have questioned its benefits to patient outcomes. These studies report no clinical difference in knee stability, patient-reported outcomes, and failure rates between revision ACLR performed with and without ALL or LET augmentation.8,20 Although our study shows that a greater proportion of surgeons perform LET compared with ALL, previous research has reported no statistically significant differences in outcomes when directly comparing the 2 procedures in primary ACLR. 2 Such comparisons are lacking in the context of revision ACLR.
Several risk factors have been linked to ACL graft failure, some of which include female sex, younger age, elevated body mass index, inconsistent rehabilitation, pivoting sports participation, higher preoperative knee laxity, and posterior tibial slope >12°. 21 Many of these factors are taken into consideration when deciding on graft augmentation to reduce the risk of reinjury, as supported by the present study. The patellar tendon autograft is often preferred for revisions, 17 as was also seen within the present study. Surgeon factors, including fellowship training and location, affect graft choice for primary ACLR, 12 and this study concludes a similar effect in revision ACLR. Graft failure rates and associated expenses are considerations during the graft selection process for ACLR.4,12 This study indicated that LET is used more frequently than ALL. The study results may reflect surgeon familiarity, perceived technical advantages, or extrapolation from primary ACLR literature supporting LET use compared with ALL. 10
A limitation of this study is that it used a survey methodology and surveyed a subset (469 out of 3262 contacted) of orthopaedic sports medicine practitioners. Although the sample was diverse in terms of practice settings and years of experience, it might not be representative of the broader range of practices in revision ACLR. The deferral of answers to questions also restricts the interpretability of the results. Additionally, there is no demographic information available on nonresponders, which limits comparison between our subset of respondents and the overall AOSSM membership. A main limitation of this study is the risk of responder bias, with surgeons who are more active within the AOSSM, research, or academic practice potentially more likely to participate. Furthermore, reliance on self-reported data introduces the potential for recall bias affecting the accuracy of reported results.
Conclusion
Variability exists among AOSSM members in the indications for ALC augmentation and graft selection during revision ACLR. Within this subset of respondents, LET is the most common augmentation technique, and the autograft patellar tendon is the main graft used in the revision setting. ALC augmentation is often indicated for patients with multiple failed previous reconstructions. Further studies are necessary to determine which patient populations receive maximal benefit from ALC augmentation techniques and certain graft types in revision ACL reconstruction.
Footnotes
Appendix A
Final revision submitted August 25, 2025; accepted September 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.V. reports serving in consulting or advisory roles for Artelon and Stryker; and holds equity or stock in Altior, Carbon 22, and Spinal Simplicity. A.J.V. has received consulting fees from Arthrex and Stryker; non-consulting compensation from Arthrex and Smith & Nephew; educational payments from Gemini Mountain Medical; hospitality payments from Bodycad; and honoraria from Vericel. P.J.M. reports receiving royalties and consulting income from Arthrex; and holds stock in VuMedi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Kansas Medical Center Human Research Protection Program (STUDY00147733).