
Abstract
Background:
Bone–patellar tendon–bone (BPTB) and hamstring tendon (HT) autografts are the most utilized grafts for primary anterior cruciate ligament (ACL) reconstruction. The ability of a patient to return to a preinjury level of physical activity is a key consideration in choice of graft; the influence of graft choice on this metric lacks consensus in the literature.
Purpose:
To assess the effects of autograft choice (BPTB vs HT) for primary ACL reconstruction on return to baseline level of physical activity and/or sports participation.
Study Design:
Meta-analysis; Level of evidence, 1.
Methods:
A systematic review of randomized controlled trials comparing the use of BPTB and HT autografts for primary ACL reconstruction was conducted. The electronic databases EMBASE, MEDLINE, Cochrane CENTRAL, and Web of Science were comprehensively queried through September 23, 2019. The primary outcome was return to preinjury level of activity/sports. Secondary outcomes included knee stability testing (Lachman, KT-1000 arthrometer, and pivot-shift tests) and clinical subjective knee scores (Tegner, Cincinnati, International Knee Documentation Committee, and Lysholm). Two independent reviewers were involved in the screening of titles and abstracts, data extraction, and the assessment of risk of bias. Meta-analyses were performed respecting the Cochrane Handbook for Systematic Reviews of Intervention.
Results:
A total of 29 studies (N = 3099 patients) were eligible for this review, of which 13 (n = 1029 patients) reported on return to baseline level of sports as an endpoint. The risk ratio (RR) of using BPTB vs HT on return to baseline sport level was 1.03 (0.91-1.17; P = .63). Absence of a positive pivot-shift test was the only secondary outcome, with a statistically significant RR of 0.66 (95% CI, 0.50-0.86) in favor of BPTB autografts (P = .002).
Conclusion:
In reviewing the current literature, no recommendation can be made on the optimal graft choice when using a return to baseline level of physical activity and/or sports participation as a primary metric.
Anterior cruciate ligament (ACL) tears are among the most common knee ligament injuries that athletes suffer over the course of their careers. Over time, ACL injuries can lead to chronic pain, osteoarthritis, symptomatic instability, and other structural changes within the knee.8,9 For athletes with primary ACL tear, arthroscopic reconstruction of the ligament remains an effective management option, as it reduces knee laxity, articulation instability, and the risk of late meniscal tear.11,13 Most studies show that the rate of rerupture of allografts is higher than that of autografts.30,38 Bone–patellar tendon–bone (BPTB) autograft and hamstring tendon (HT) graft are the 2 most popular graft options for ACL reconstruction surgery. However, existing trials and meta-analyses display conflicting conclusions regarding which is the most favorable tendon for athletes and active patients. Some studies suggested superiority of BPTB because of faster graft incorporation from bone-on-bone healing, 37 a potentially lower risk of graft rerupture,14,35,42 and a greater proportion of patients returning to baseline activity levels after surgery. 50 On the other hand, arguments in favor of HT autografts are the reduction of anterior knee pain, 14 long-term osteoarthritis, 26 and overall postoperative complications. 50 Recent meta-analyses that compare the use of BPTB and HT autografts do not present the proportion of patients who had returned to baseline level of physical activity at last follow-up. A systematic review by Glogovac et al 15 found that athletes might find it difficult to return to their previous level of sport after ACL reconstruction, regardless of the graft type used. It has not been conclusively demonstrated whether BPTB or HT autografts have a greater influence on successful return to preinjury activity.
The primary objective of this systematic review and meta-analysis was to assess the effect of BPTB versus HT autografts in ACL reconstruction on return to baseline level of physical activity and/or sports participation. An analysis of population subgroups based on age and HT strand number was performed.
Methods
This review was conducted in accordance with the proposed structure from the Cochrane Handbook for Systematic Reviews of Interventions. 19 The protocol for this review was previously registered in PROSPERO (ID: CRD42020154812).
Eligibility Criteria
This review includes all level 1, randomized controlled trial (RCT) comparisons of patellar versus HT (regardless of the number of strands) in the context of ACL reconstruction. Included studies were those that involved patients of any age with ACL deficiency requiring ACL reconstruction through any technique using either BPTB or HT autografts and with a minimum 1-year follow-up. There was no exclusion regarding study language or year of publication. Studies that used allografts or added a ligament augmentation device or any type of extra-articular stabilization graft were excluded.
Outcomes
The primary outcome was return to the baseline level of activity at the latest point of follow-up reported in each study. This was defined as a patient’s ability to continue participating in preinjury level of sports and activity. Secondary outcomes were objective assessments of stability (Lachman, pivot-shift, International Knee Documentation Committee [IKDC], and KT-1000 arthrometer tests), readiness for return to play, or level of sport participation as assessed by any score (Tegner, 46 Lysholm, 28 and other scores), and subjective knee scores, such as the Cincinnati score 12 or the Anterior Cruciate Ligament Quality of Life score. Timing of outcome assessment was not restricted to a specific time period, and one year minimum follow-up was used. The last point of outcome assessment was used in each study. Studies without published results or those that did not present outcomes of interest were excluded from the analysis.
Study Selection
EMBASE, MEDLINE, Cochrane CENTRAL, and Web of Science databases were searched without any language restriction. These databases were searched through September 23, 2019, inclusively. The different search strategies for all 4 databases are available in the Appendix (available in the online version of this article).
Two study reviewers (J.J.B, Q.P.S.) independently assessed the eligibility of each study resulting from the search strategy based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 34 Duplicates were removed first, using Endnote integrated function. Different reports from the same study were also excluded, as suggested by the Cochrane handbook. 19 Titles and abstracts were first screened for inclusion. The studies that fit the criteria based on title and abstract went through the full-text eligibility process and were challenged with the inclusion criteria of the review. Once the study selection was completed, both reviewers searched the included studies’ references individually to identify articles that were missed by the search strategy. Discrepancies were refereed by a third reviewer (E.L.B.) when necessary. The 2 reviewers independently extracted data from the included studies. In case of missing data, the authors of the study in question were contacted via email. If no response was received after 2 attempts spaced 1 month apart, data were left as missing.
The collected data for each study were source (author, citation), eligibility (confirmed or reason for exclusion), methods (study design, duration, method of randomization, inclusion and exclusion criteria, and outcomes), participants (number of patients randomized and available at follow-up, age [mean ± SD], and level of participation in sports), interventions (total number of intervention groups, types of grafts used for randomization, and follow-up endpoint), outcomes (definition, unit of measurement, lower and upper limits of outcomes measured as scales, and timing of collection and report), results (number of participants in each group, sample size, missing participants, and summary data for each group), and miscellaneous (funding source, key conclusions, correspondence required, and miscellaneous comments from the reviewers). Numerical results were collected as means ± SD; if data were presented as median [range], we converted the results into mean ± SD using the method described by Hozo et al. 21 For Lachman tests, the results were dichotomized into “negative” and “positive (≥3 mm)” Lachman test. A positive Lachman test was considered an event for the purpose of statistical analysis. Subgroup analyses were made regarding age (<30 years vs ≥30 years), baseline level of activity (competitive or recreational), type of sport (contact or noncontact), hamstring graft type, and risk of bias. Aside from the risk of bias subgroup analysis, the remainder of the subgroups were determined based on the biological plausibility of having an effect on functional outcome and on return to baseline level of physical activity. For hamstring graft type subgroups, we used the 2 most frequently used HT graft strand number (2 vs 4) and risk of bias.
Risk of bias in individual studies was assessed by the 2 reviewers independently at the primary outcome level using the Cochrane tool for assessing risk of bias. Studies with either all “low risk” or 1 “unclear” risk were labeled as “low risk of bias.” Studies with 1 or more “high risk” domains or at least 3 “unclear” risks were labeled as “high risk of bias.” Studies with 2 “unclear” domains but no “high risk” criterium were labeled as “unclear risk of bias.” For attrition bias, studies that had lost more than 10% of their patients at the time of the last outcome evaluation were analyzed as “high risk” for that category.
Statistical Analysis
Dichotomous outcome results were expressed as risk ratios (RR) with a random-effects model. Continuous outcome results were expressed as mean differences (MDs) with a random-effects model. Both were presented with 95% CIs. Ordinal scales were treated as continuous outcomes. Consistency between studies was assessed for each meta-analysis first by visual inspection of the forest plot, then tested by a chi-square test (significance level set at P < .05) and the I-squared value (heterogeneous if I2 > 50%). RRs between 0 and 1 or MDs <0 favor the use of a BPTB graft, whereas RRs >1 or MDs >0 favor an HT graft. For the analysis, we considered the number of patients in each study who did not return to preinjury level of participation at the time of outcome evaluation to evaluate the primary outcome.
Results
A total of 2857 studies were initially identified. After removal of 945 duplicates, the remaining 1912 articles were screened by title and abstract. A total of 1805 studies could be removed by title and abstract screening only, leaving 107 articles to go through full-text eligibility. Of those 107 studies, 42 were not randomized controlled trials (RCTs), 5 were not randomized for graft type, 16 did not present published results, 9 did not present outcomes of interest, and 6 were not the last available outcome results for that group of patients. Finally, 29 studies (N = 3009 patients) matched the inclusion criteria and were therefore included in this systematic review. Hand searching did not provide any further studies for inclusion. Figure 1 shows the flow of included and excluded studies.
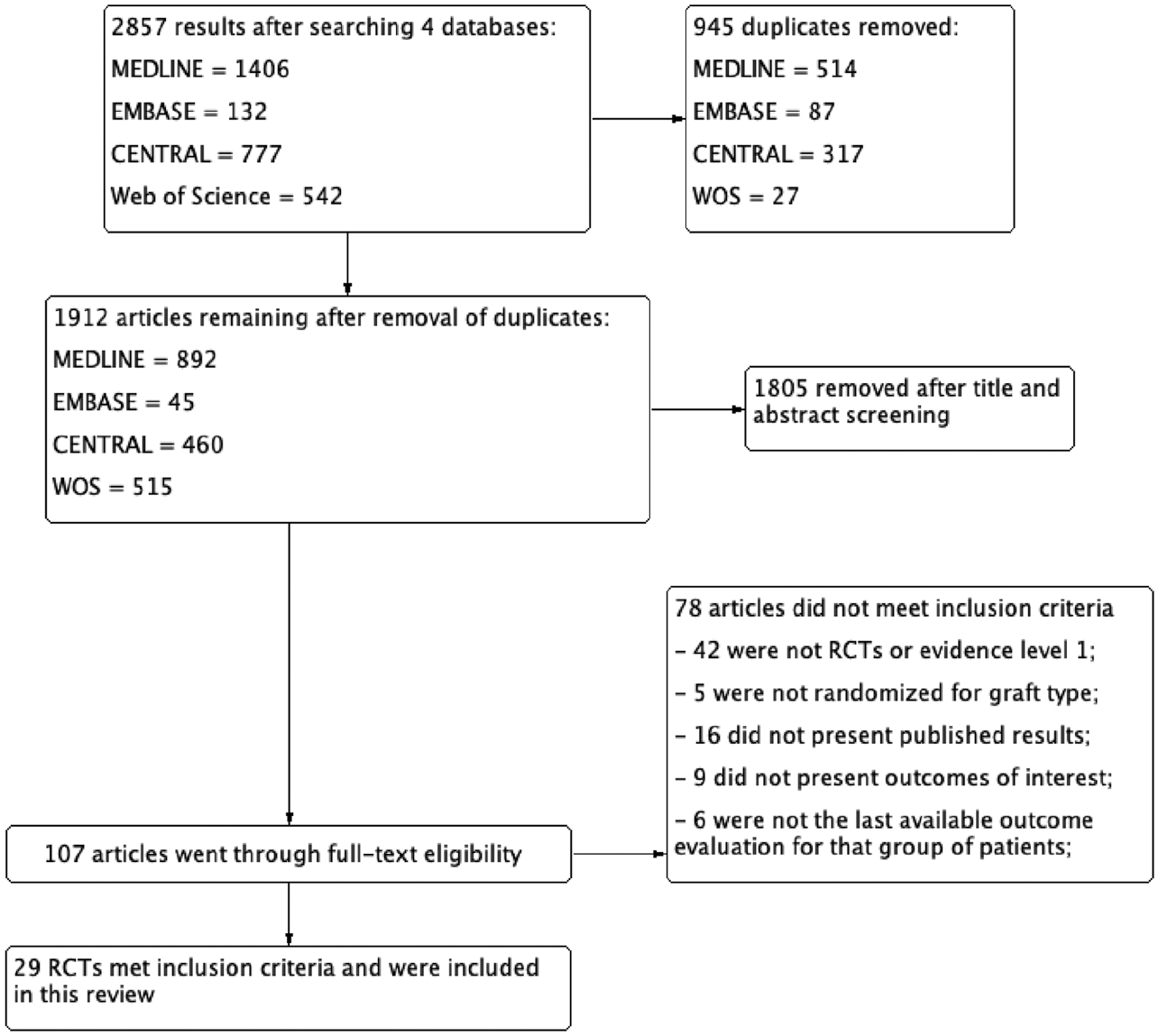
Flow diagram of included studies. RCT, randomized controlled trial. WOS, Web of Science.
Of the 29 studies that were included in this systematic review, 28 used regular patellar tendon autografts as the patellar tendon (PT) group. One study used a lateralized BPTB graft, 51 which was excluded from the analysis. Regarding HT groups, 6 studies used a 2-strand semitendinosus and gracilis (STG)3,10,22,31,44,51; only 1 used a 2-strand semitendinosus (ST) (a 6- to 7-mm graft fixed with femoral Endobutton [Acufex Microsurgical, Mansfield, MA] and tibial staples) 40 ; 14 used a 4-strand graft (double loop semigracilis or folded graft) § ; and 4 used 3- or 4-strand ST or STG grafts2,23,25,27 without differentiating between the 2. The remaining studies used 4-strand ST graft, 6 STG graft with preserved insertion, 17 or 5- or 6-strand STG grafts.24,33 Also, 2 studies had 3 different types of interventions.6,52 We included the studies in the systematic review but analyzed only the HT and PT groups. Table 1 shows the characteristics of the included studies.
Characteristics of Included Studies a
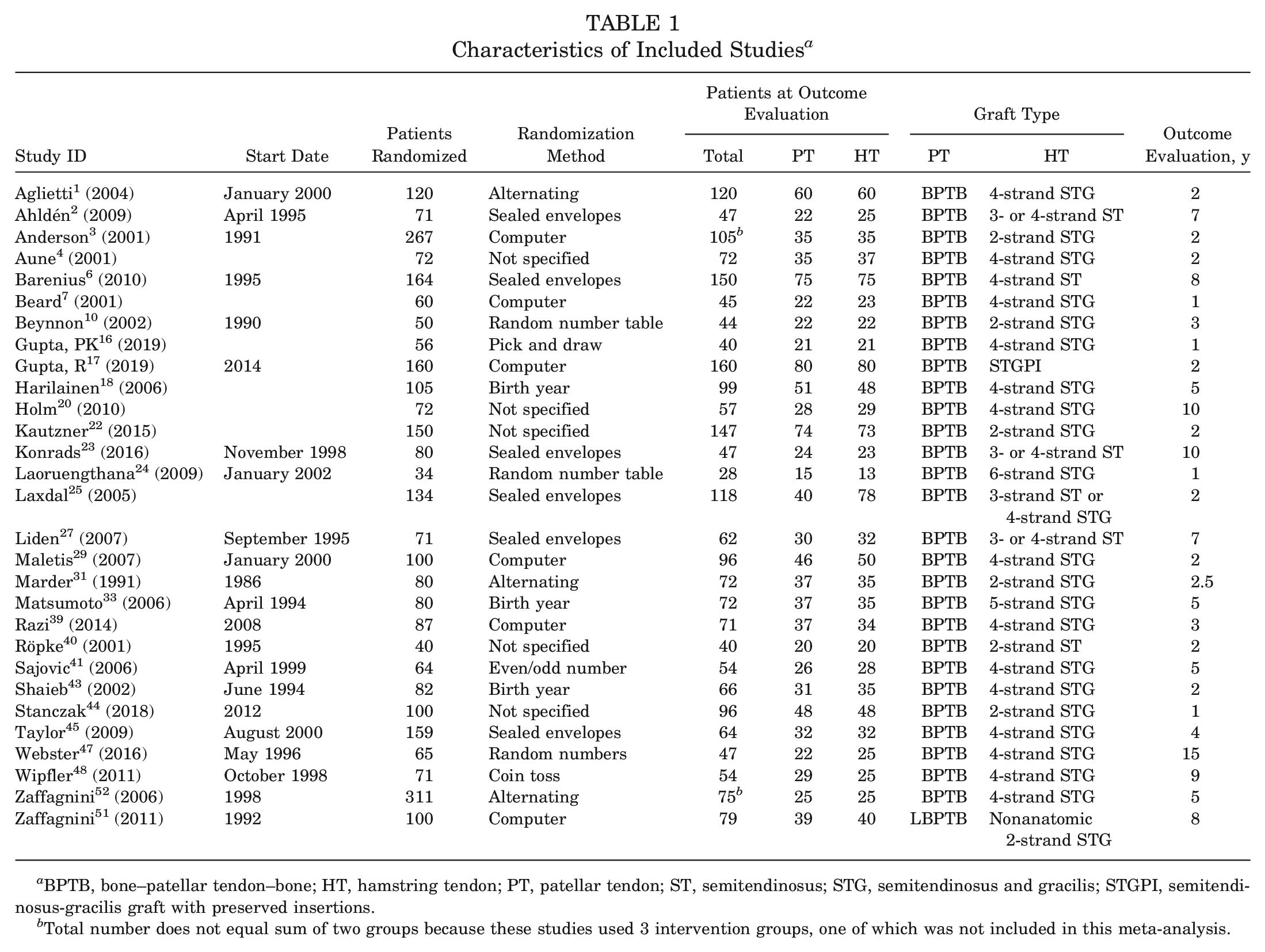
BPTB, bone–patellar tendon–bone; HT, hamstring tendon; PT, patellar tendon; ST, semitendinosus; STG, semitendinosus and gracilis; STGPI, semitendinosus-gracilis graft with preserved insertions.
Total number does not equal sum of two groups because these studies used 3 intervention groups, one of which was not included in this meta-analysis.
Of the included studies, 1 was judged as “low risk of bias” at the outcome level. 29 Selection bias was at “high risk” for 8 studies based on both sequence generation and allocation concealment.1,18,31,33,40,41,43,52 Three studies were at “low” or “unclear” risk for sequence generation but were at high risk for allocation concealment.10,36,48 Performance bias was at “low risk” for 4 of the included studies.1,2,29,45 Two studies were at “low risk” for detection bias.1,29 Twelve studies were at “low risk” for attrition bias, ‖ and most other studies had lost over 10% of their patients between surgery and outcome evaluation, so they were judged as “high risk of bias.” Selective outcome reporting was judged as “low risk” for 7 articles.4,22,23,25,27,29,44 Random sequence generation was the only domain judged as “low risk” for over 50% of included studies. Figure 2 shows the distribution of studies across each domain.
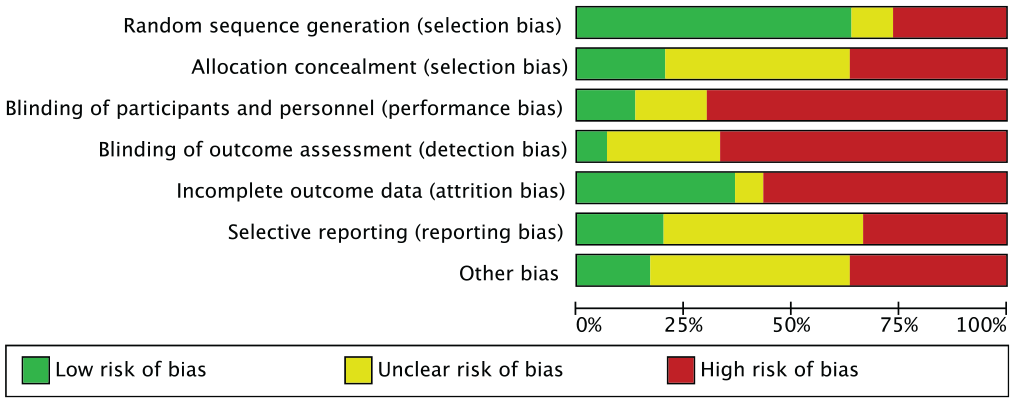
Risk of bias distribution for each domain.
Primary Outcome: Return to Preinjury Level
Thirteen studies presented the number of patients who had returned to their preinjury level of physical activity at the time of the last evaluation. Four studies published significant results. Three favored BPTB: Gupta et al 17 (RR, 1.32; 95% CI, 1.02-1.72; n = 154); Maletis et al 29 (RR, 1.92; 95% CI, 1.11-3.33; n = 96); and Taylor et al 45 (RR, 1.53; 95% CI, 1.06-2.20). Röpke et al 40 favored HT autograft (RR, 0.35; 95% CI, 0.18-0.71; n = 40). One study 52 had all of its patients returning to baseline level of sports, which made the RR not estimable for that study. The relative risk was 1.03 (95% CI, 0.91-1.17) in favor of BPTB graft (P = .63). A total of 1029 patients were evaluated for this outcome. Figure 3 presents the results of each study and the meta-analysis. In this meta-analysis, an event is defined as a return to baseline level of physical activity.
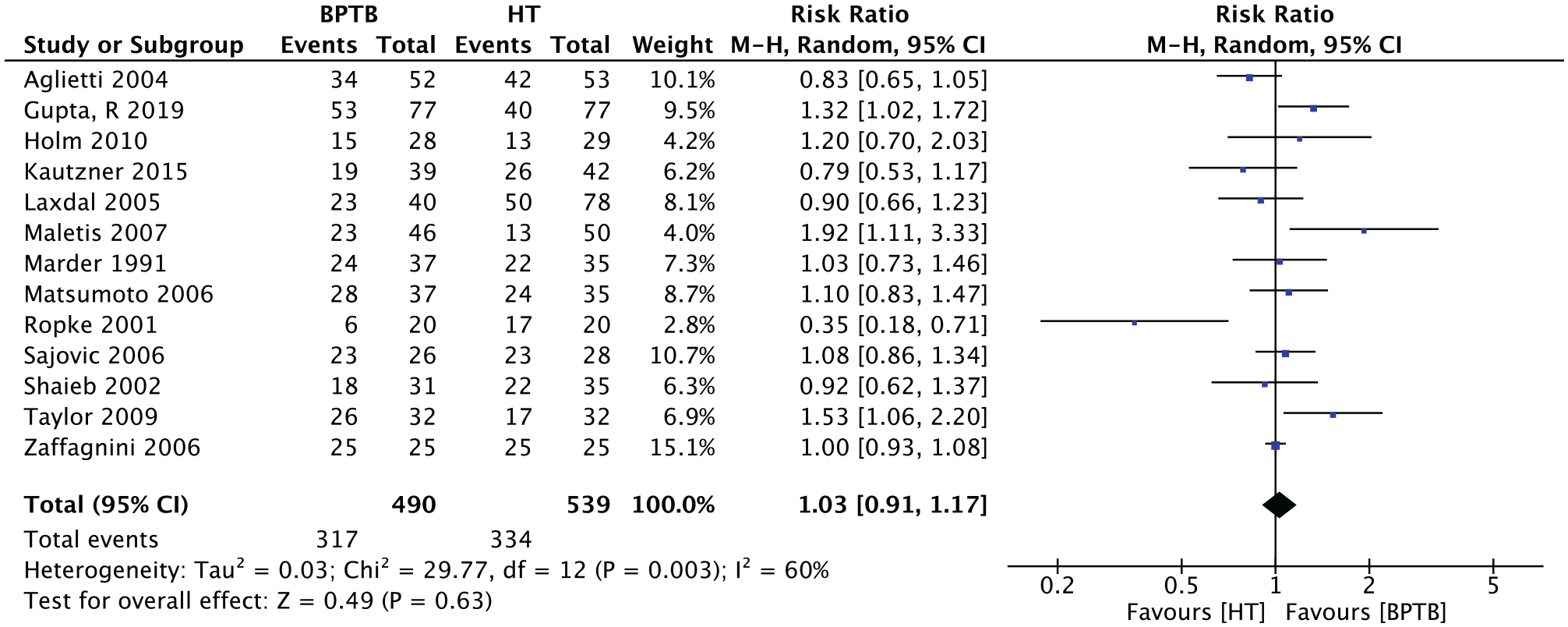
Meta-analysis of the outcome “return to preinjury level of physical activity.” BPTB, bone–patellar tendon–bone; HT, hamstring tendon; M-H, Mantel-Haenszel.
These results were not influenced by age when age 30 years was used as a threshold (Figure 4).
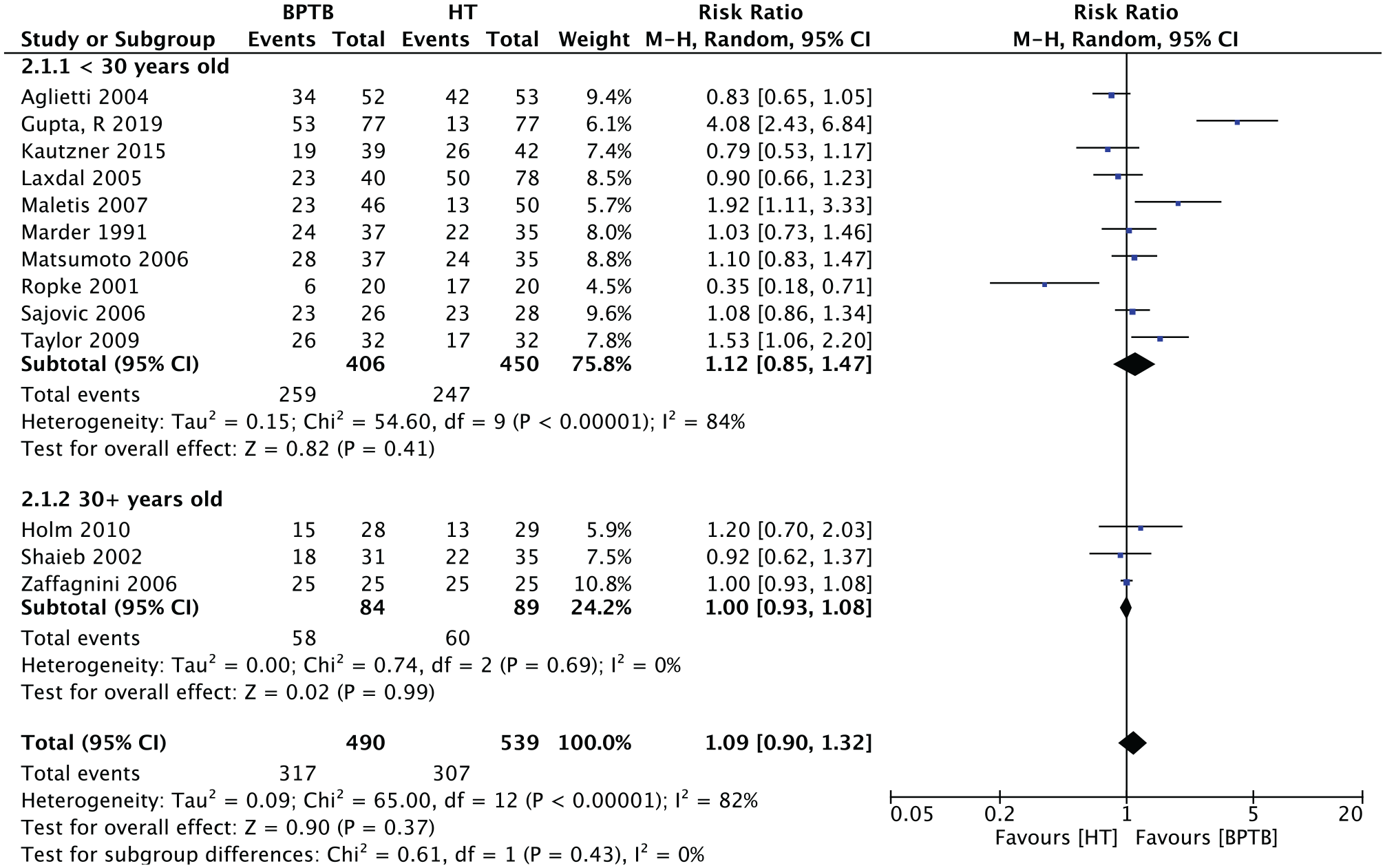
Subgroup analysis of the “return to activity” outcome by age. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; M-H, Mantel-Haenszel.
The second subgroup analysis was based on hamstring graft type. Studies that used other graft types were excluded from this analysis. In the 2-strand HT graft subgroup (3 studies; n = 193 patients) the RR was 0.71 (95% CI, 0.42-1.20; P = .20). In the 4-strand HT graft subgroup (7 studies; n = 492 patients), the RR was 1.09 (95% CI, 0.91-1.32; P = .34). The overall relative risk was 1.01 (95% CI, 0.86-1.18; P = .93). Figure 5 presents the meta-analysis for this subgroup.
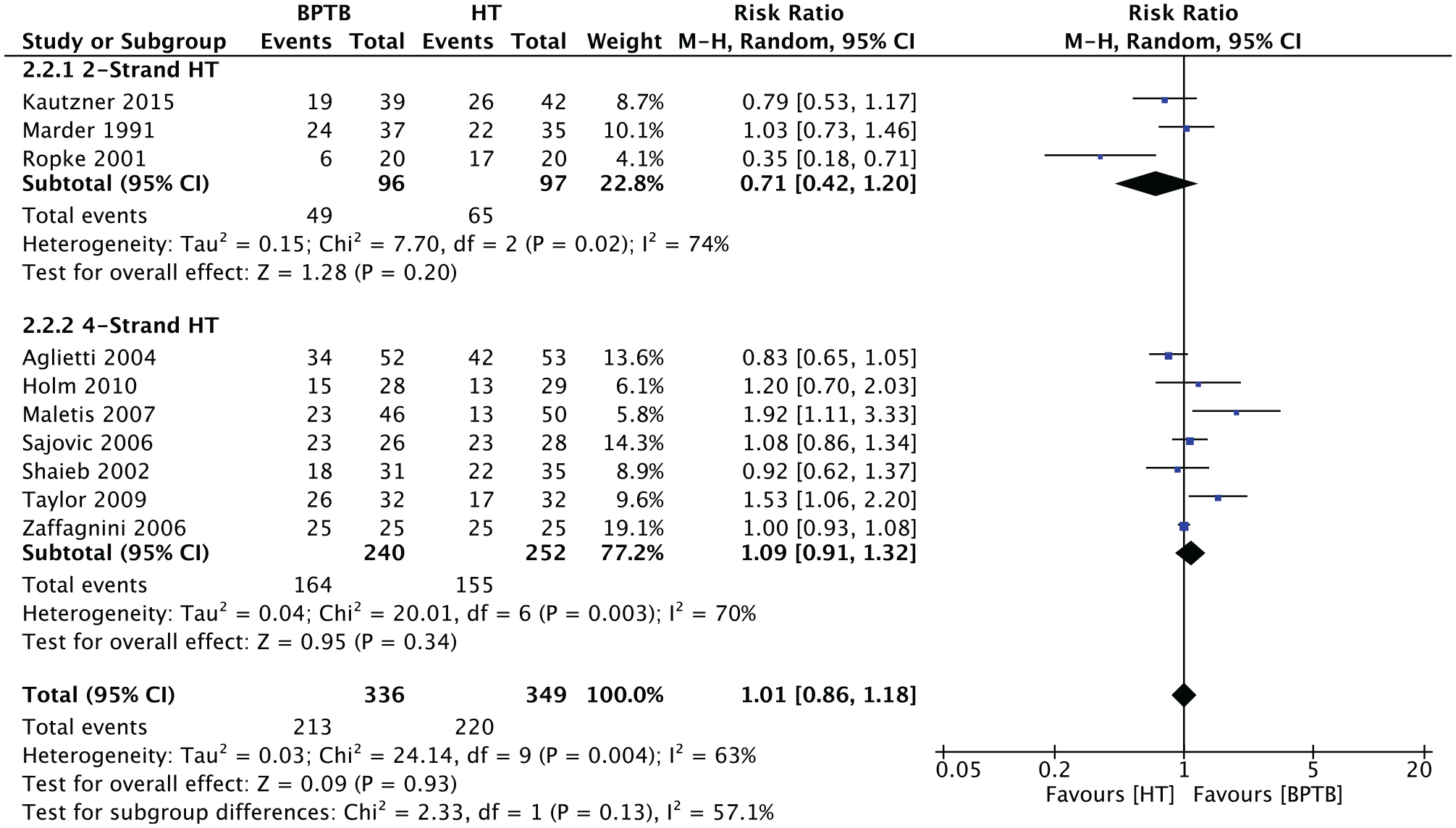
Subgroup analysis of the “return to activity” outcome by number of strands. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; M-H, Mantel-Haenszel.
Secondary Outcome: Tegner Activity Scale
Twelve studies (n = 848 patients) presented the results for the Tegner activity scale. The overall relative risk on a continuous scale for this outcome was 0.26 (95% CI, –0.44 to 0.95; P = .47) in favor of BPTB (Figure 6).
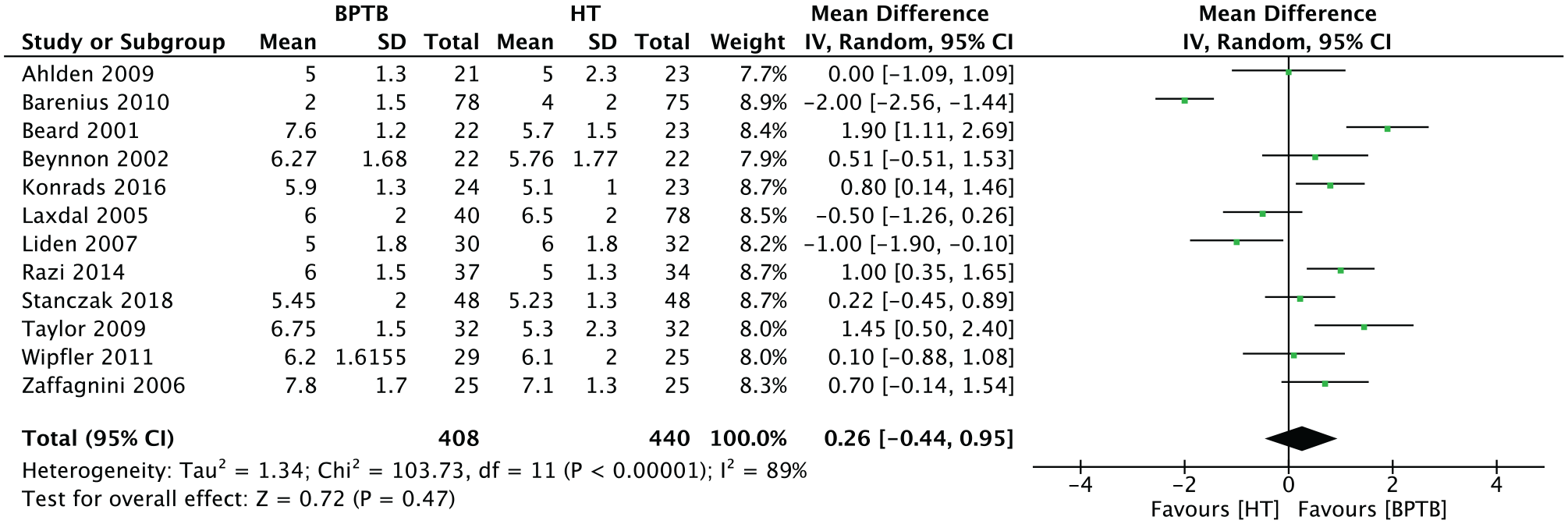
Meta-analysis for the Tegner scale. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; IV, inverse variance.
The Cincinnati Score
Four studies (n = 190 patients) presented the results of the Cincinnati score at endpoint. The overall result for this continuous outcome scale was 0.38 (95% CI, –3.74 to 4.50; P = .86) in favor of BPTB (Figure 7).

Meta-analysis for the Cincinnati score results. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; IV, inverse variance.
The Lysholm Score
Twelve studies (n = 890 patients) presented data for the Lysholm score at endpoint. The overall results were −0.79 (95% CI, –1.78 to 0.21; P = .12) in favor of HT (Figure 8).
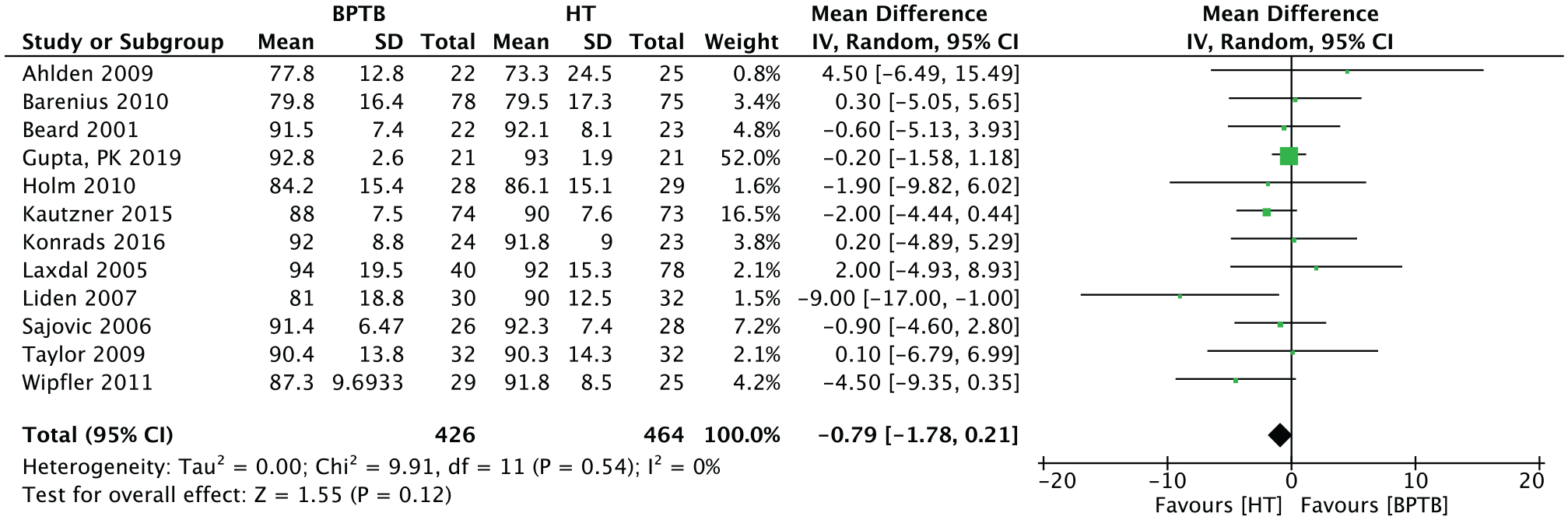
Meta-analysis for the Lysholm score results. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; IV, inverse variance.
The IKDC Score
Thirteen studies (n = 983 patients) presented results for the IKDC level of activity. The results of this dichotomous outcome were 1.01 (95% CI, 0.95-1.09; P = .72) in favor of BPTB (Figure 9).
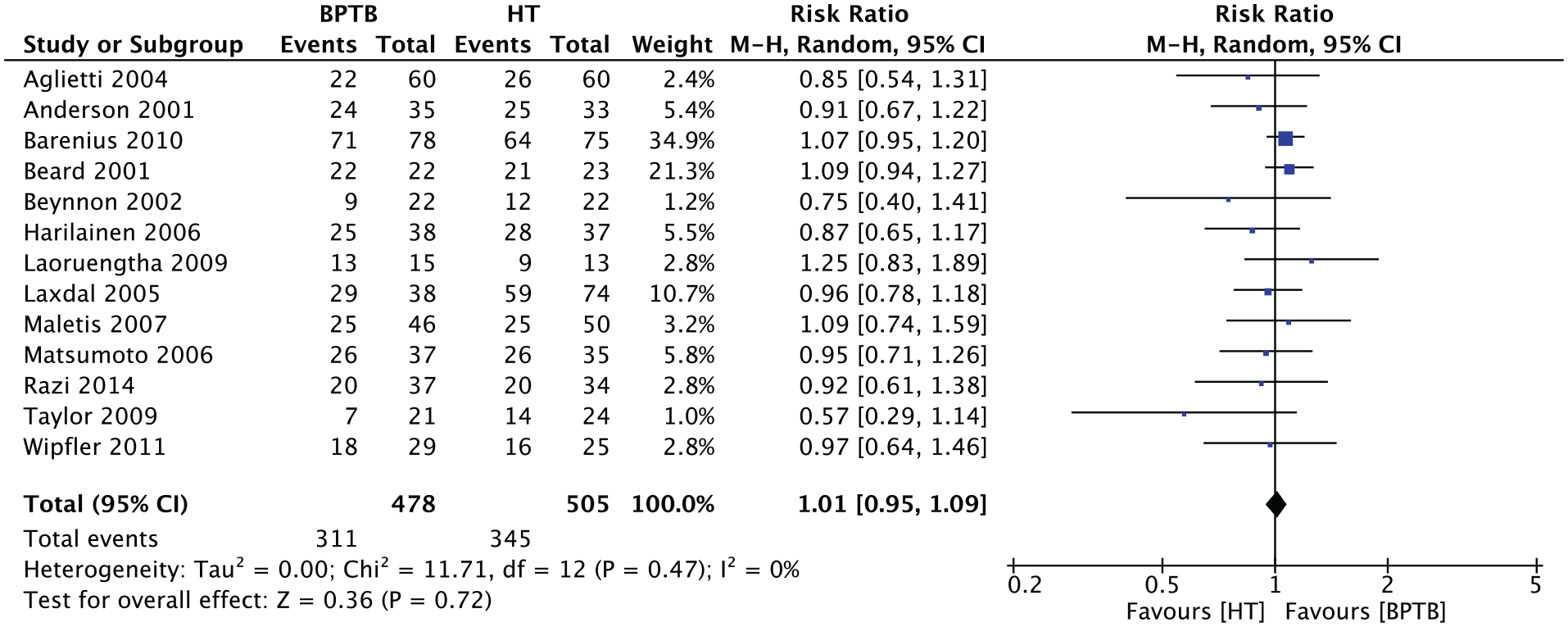
Meta-analysis for IKDC results. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; IKDC, International Knee Documentation Committee; M-H, Mantel-Haenszel.
The Lachman Test
Twelve studies (n = 832 patients) presented the results of the Lachman test for anterior tibial displacement at endpoint. The overall RR was 0.80 (95% CI, 0.56-1.14; P = .21) in favor of HT (Figure 10).
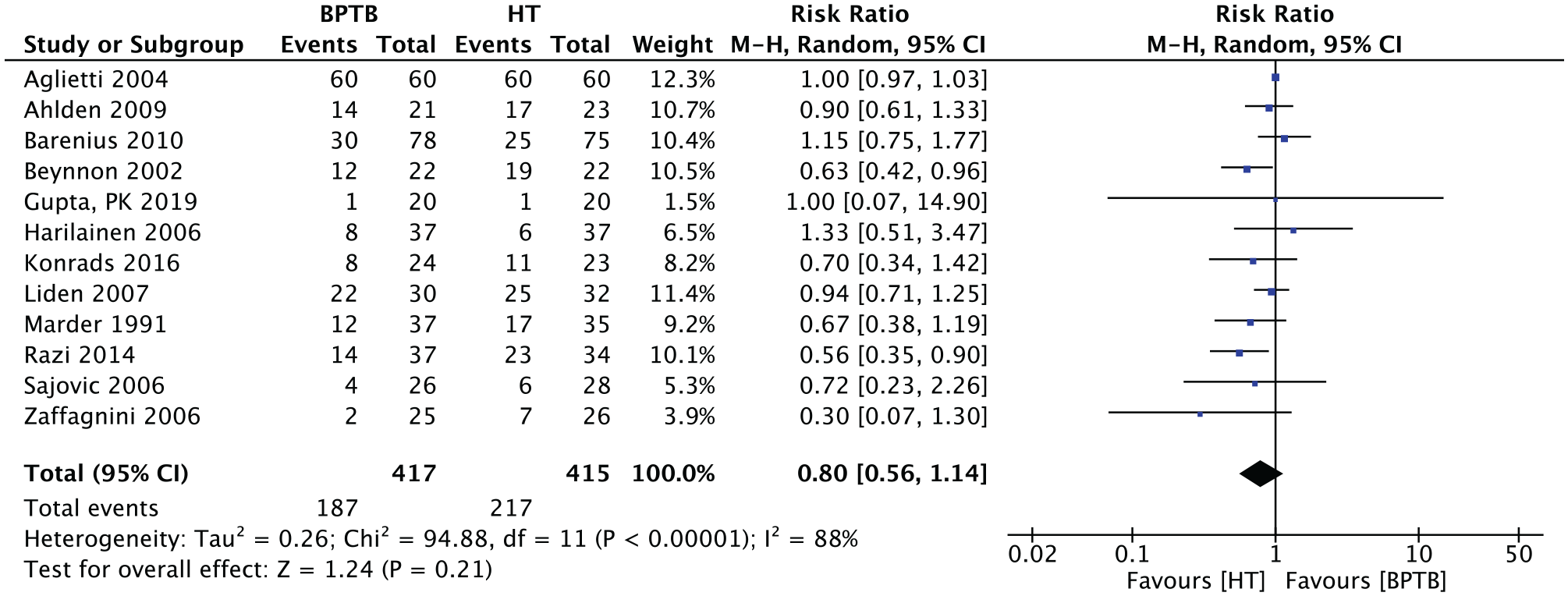
Meta-analysis for the Lachman test results. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; M-H, Mantel-Haenszel.
The Pivot-Shift Test
Thirteen studies (n = 954 patients) presented results for the pivot-shift test (+/-) at endpoint outcome evaluation. The overall RR for this outcome was 0.66 (95% CI, 0.50-0.86; P = .002), with HT grafts being more at-risk for a postoperative positive pivot-shift test (Figure 11).
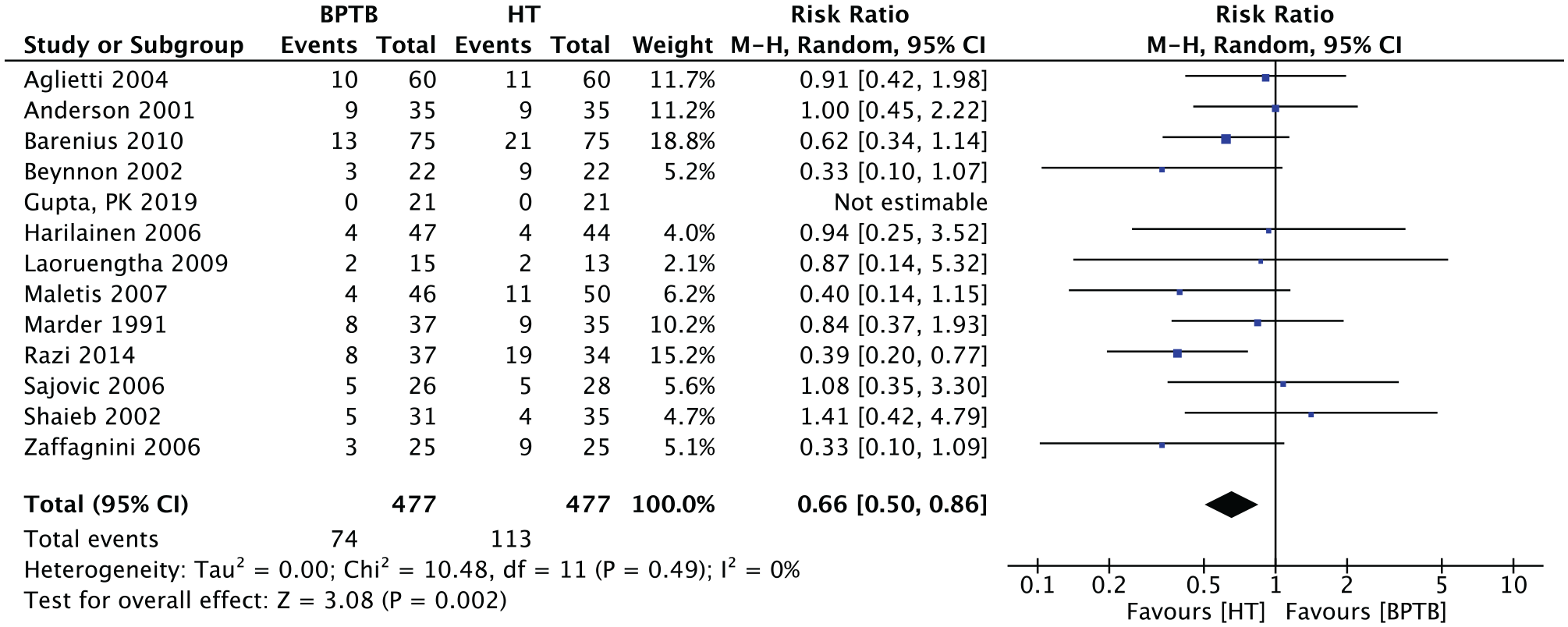
Meta-analysis for the positive pivot-shift test results. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; M-H, Mantel-Haenszel.
KT-1000 Athrometer at 134 N of Force
Eleven studies (n = 870 patients) presented results for the KT-1000 arthrometer evaluation at 134 N (30 pounds) of force at endpoint outcome evaluation. The overall results for this continuous outcome were −0.07 (95% CI, –0.35 to 0.21; P = .61) in favor of HT (Figure 12).
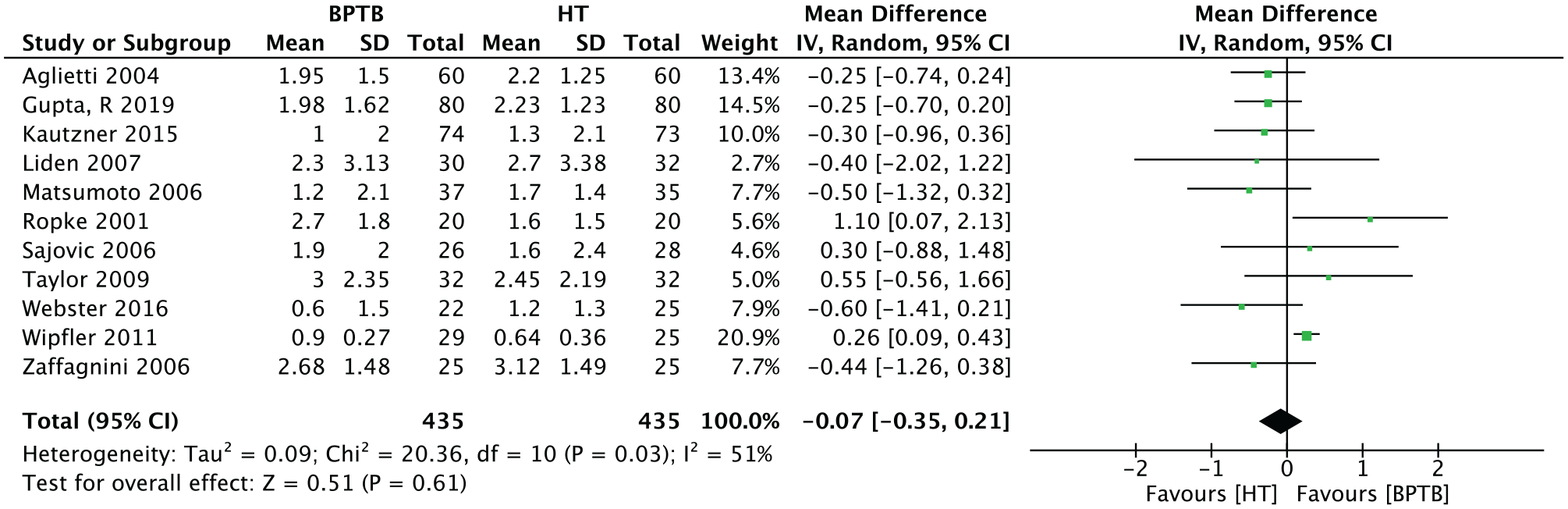
Meta-analysis for the KT-1000 arthrometer at 134 N. BPTB, bone–patellar tendon–bone; HT, hamstring tendon; IV, inverse variance.
Risk of Bias Across Studies
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was done for the return to preinjury level of activity/sports participation. The overall risk of bias was “very serious,” as every study reporting this outcome was at high risk of bias, except for 1 study (Maletis et al 29 ). Heterogeneity was substantial (I2 = 59%), so overall outcome assessment is at serious risk of inconsistency. Table 2 summarizes the GRADE approach for the main outcome of interest.
GRADE Approach for the “No Return to Physical Activity” Outcome a

GRADE, Grading of Recommendations Assessment, Development and Evaluation; RCT, randomized controlled trial.
Discussion
The most important finding of this meta-analysis was that graft type use, whether BPTB or HT autograft, does not appear to influence the return to baseline level of physical activity at a minimum 1-year follow-up based on the available evidence. This remains true in patients older or younger than 30 years. In the analysis of our secondary outcomes, patients who had their ACL reconstructed with a BPTB autograft demonstrated a significantly lower rate of a positive pivot shift at the last follow-up (RR, 0.66; 95% CI, 0.50-0.86; P = .03). The other secondary outcomes of interest (Lachman, Tegner, Cincinnati, Lysholm, KT-1000 arthrometer, and IKDC tests) did not favor any type of graft.
The ability to return to baseline level of physical activity is a crucial parameter to consider in the utilization of hamstring or patellar tendon autograft for patients with ruptured ACLs. 14 Xie et al 49 published a meta-analysis in 2015, including 14 RCTs and 8 prospective comparative studies (PCSs). Their results favored BPTB for return to preinjury level of activity with an RR of 1.48 (95% CI, 1.03-2.12; P = .03). However, the inclusion of PCSs into their review lowers the confidence we can have in these results, as comparative studies are at higher risk of bias. They observed a statistically significant difference favoring 4-strand hamstring tendon grafts, and their analysis included data from 8 studies (n = 507), of which 2 studies were PCSs. In contrast, our subgroup analysis of 4SHT versus BPTB favored the latter for return to preinjury level of activity; however, the results were not statistically significant, so no conclusions can be drawn from this analysis. The absence of effect might be because of the differences in sample size, which would make the present study more accurately representative of reality.
The metrics used to assess for return to preinjury level of activity in the included studies are very variable. An objective rating tool, such as the Marx activity rating scale, would have been more precise, although studies were not designed for this outcome. 32 We encourage future studies to use objective tools to assess return to activity.
Subgroup analysis showed that age of patients (older or younger than 30 years) did not affect the rate of return to previous level of sport. Previous large meta-analyses comparing BPTB and HT autografts have not examined age as a subgroup for this outcome.26,35,49 A prospective cohort study by Barber et al 5 compared Lysholm, IKDC, and Cincinnati scores between younger and older patients, with the age of 40 years as a cutoff, and found no difference between the 2 groups. They, however, used BPTB allografts instead of autografts. As activity level varies with age, it is not surprising that there is no difference with the age of 30 years as a cutoff. Using a younger age cutoff, such as 20 or 25 years, might have led to different results, as using these ages might separate elite and recreational athletes more accurately.
Through the analysis of our secondary outcomes, we found that BPTB favored a more stable knee when considering a pivot shift as an objective evaluation of knee stability at the last follow-up. This finding is in line with results from other reviews. Mohtadi et al 35 published a systematic review of randomized and quasi-randomized trials comparing patellar and HT grafts for the reconstruction of the ACL. Although their inclusion criteria allowed them to include more studies into their review, they had similar results regarding Tegner activity level, Lysholm score, Cincinnati score, KT-1000 arthrometer at 134 N, and Lachman test, and none of these favored one graft type over the other in the RCT subgroup analyses. The authors, however, did not present the proportion of patients who had returned to their baseline level of activity at endpoint outcome evaluation. Xie et al 49 (RR, 0.70; 95% CI, 0.53-0.93; P = .32) as well as Mohtadi et al (RR, 0.70; 95% CI, 0.54-0.89; P = .0036) found that BPTB favored a stable knee as assessed by the pivot-shift test. This contrasts with a meta-analysis by Li et al, 26 who found that HT might be more favorable to higher rotational stability assessed by pivot-shift testing. Although they had similar inclusion criteria (ie, RCTs only), the inclusion of more studies in our meta-analysis increases the confidence that one can have in the results presented. However, the subjectivity of the pivot-shift test might also explain the differences in results.
Strengths and Limitations
The Cochrane Handbook for Systematic Reviews of Interventions 19 was used as a guideline for establishing the methods of this review. This assures a certain level of thoroughness and exhaustiveness. As this is a systematic review of RCTs, this review presents the highest available quality of evidence. The quality of evidence is low, however, as shown by the GRADE approach. Weaknesses of this review include the conversion of medians into means for some of the collected data, which may not be as accurate as we would have expected. Because the search strategy did not appear to be very specific, some studies might have been missed during the first step of screening. There was only 1 study that used a 2-strand ST graft (Röpke et al 40 ); thus, its inclusion in subgroup analyses might have influenced the results for this particular subgroup. Also, the selection process for this meta-analysis might have led to the exclusion of large-number of studies that could have influenced the secondary outcome analysis. Therefore, results for the secondary outcome analysis should not directly lead to conclusions.
Conclusion
No recommendation can be made regarding the use of BPTB or HT graft for ACL reconstruction regarding return to preinjury activity level and/or sports participation. Based on the available evidence, the choice of graft does not affect return to preinjury activity level. Higher quality RCTs must be completed to confirm this and to balance out the low quality of the available body of evidence in future systematic reviews on this subject.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211017522 – Supplemental material for Return to Baseline Physical Activity After Bone–Patellar Tendon–Bone Versus Hamstring Tendon Autografts for Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211017522 for Return to Baseline Physical Activity After Bone–Patellar Tendon–Bone Versus Hamstring Tendon Autografts for Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Randomized Controlled Trials by Jeremy J. Bergeron, Quentin P. Sercia, Justin Drager, Stéphane Pelet and Etienne L. Belzile in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Dr Jörg Schröder, from Berlin, for his help with the translation of German articles.
Submitted September 23, 2020; accepted January 25, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D. has received speaking fees from DJ Orthopedics. E.L.B. has received research support from Smith & Nephew, Bodycad, CIHR, and B-Themia; speaking fees from Stryker, DePuy, ConMed Linvatec, Bodycad, and Ergoresearch; and royalties from Bodycad. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.