
Abstract
Background:
Netball is a popular sport worldwide, particularly for women. However, its nature puts players at high risk for anterior cruciate ligament (ACL) injury.
Purpose:
To determine (1) the prevalence of ACL graft rupture and contralateral ACL (CACL) rupture in Australian female netballers after ACL reconstruction (ACLR) and (2) the rate of return to sports (RTS) and psychological readiness.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A patient database identified 332 consecutive female netball players who underwent ACLR with hamstring tendon autografts performed by 2 surgeons between 2007 and 2015. Patients were retrospectively surveyed at a minimum of 7 years postoperatively—including details of a second ACL injury to either knee, RTS, and psychological readiness per the ACL–Return to Sport After Injury (ACL-RSI) score. Multivariate regression assessed the association between selected variables and repeat ACL injury.
Results:
A total of 267 patients (80%) were included with a mean follow-up of 8.4 years (range, 7-15 years). ACL graft rupture and CACL rupture occurred in 11 (4%) and 27 (10%) patients, respectively, at 7 years postoperatively. The ACL graft had a survival rate of 99%, 97%, 97%, and 96% at 1, 2, 5, and 7 years after surgery, respectively. The native CACL had a survival rate of 100%, 99%, 94%, and 90% at 1, 2, 5, and 7 years, respectively. Adolescents had a 4.5 times greater hazard for ACL graft rupture (95% CI, 1.4-14.6; P = .014) and a 2.5 times greater hazard for CACL rupture (95% CI, 1.2-5.5; P = .021) compared with adults. CACL injury was also associated with a return to level 1—including jumping, hard pivoting, and cutting—sports (hazard ratio, 10.3 [95% CI, 1.4-77.1]; P = .023). Most (62%) participants returned to netball, with those with higher ACL-RSI scores more likely to RTS.
Conclusion:
The prevalence of repeat ACL injury was higher in the contralateral knee (10%) than the ACL-reconstructed knee (4%) at 7 years postoperatively. ACLR was a suitable option for female netballers who sustained an ACL rupture with low long-term rates of graft rupture. Repeat ACL injuries to either knee were more common in adolescents and those who returned to cutting and pivoting sports.
Netball is a popular sport worldwide, with over 20,000,000 people participating annually.7,25 It is the most popular female team sport in Australia. 7 Knee injuries are common, accounting for most (42%) injury insurance claims in Australian netballers.18,27 Even with the advent of netball knee injury prevention programs, 36 anterior cruciate ligament (ACL) injuries are prevalent in both community and elite netballers,17,24,47 accounting for 25% of injuries. 47 The nature of the sport involves movement patterns such as cutting, pivoting, rapid changes of direction, and, importantly, the “footwork rule.” This rule restricts a player landing with the ball on 1 leg to only taking 1 further step before passing the ball, which increases their deceleration rate and vertical ground-reaction force and potentially increases their risk of ACL injury.12,26,39
Many patients who sustain ACL ruptures opt for surgical reconstruction to return functional stability and reduce the risk of chondral or meniscal injuries. 35 Australia has the highest rate of ACL reconstruction (ACLR) worldwide, and the incidence of ACLR has increased by 43% between 2000 and 2015. 53 Second, ACL injuries are reported to occur in 6% to 22% of patients over the first 5 years after ACLR in sporting populations.9,33,45,50,52 However, we should not assume that injury patterns are equivalent between sports given the diversity in components, especially with a unique sport such as netball. There are no long-term studies on the rate of reinjury to the ACL graft or injury to contralateral ACL (CACL) after ACLR in netballers.
One of the main goals of primary ACLR is to allow patients to return to cutting, pivoting, or jumping sports.11,19 However, a significant proportion of athletes still will not return to their preinjury level of sport. Ardern et al 4 reported that only 19% of netballers returned to competition at 12 months, the lowest rate compared with 3 other sports. Return to sports (RTS) after ACLR is variable, with up to 40% reported not returning to their preinjury level of participation. 5 One proposed reason for failure to RTS is a lack of psychological readiness.6,28 It is proposed that this psychological response is contributed to by fear of reinjury, sport locus of control, and an athlete’s estimate of the length of time it may take to RTS. 21 There is a lack of knowledge of long-term outcomes in returning to netball after ACLR.
The primary aim of this study was to determine the prevalence of ACL graft rupture and CACL rupture in Australian female netballers 7 years after ACLR. We hypothesized that the ACL graft and the CACL would have equivalent injury rates. The secondary aims were to determine the rate of RTS and psychological readiness in RTS in this cohort.
Methods
A prospective database identified 332 consecutive ACLRs performed between 2007 and 2015 using hamstring tendon autografts in female netball players who had provided informed consent. All procedures were performed by 2 experienced knee surgeons (L.P. and J.R.) at a single center. Patients were retrospectively surveyed at a minimum of 7 years after reconstruction. The study protocol received institutional review board approval.
Study Patients
All participants sustained a primary ACL rupture while playing netball at competitive or recreational levels. Those with a history of previous CACL injury were excluded. The surgical technique has previously been described 13 and involved a 4-strand hamstring tendon autograft with femoral drilling via the anteromedial portal and interference screw fixation of the ACL graft on both the femur and tibia. Postoperatively, patients underwent a standardized rehabilitation program under the guidance of the operating surgeon and the patients’ physical therapist. 42 Based on previous evidence that recognized higher graft rupture rates within 12 months after ACLR,9,33,45,46 patients were not encouraged to return to competitive team-based ball sports until after 12 months postoperatively and once rehabilitation goals had been met.
Follow-up Evaluation
Persons not involved in the index operation or the care of the patient contacted participants at a minimum of 7 years postoperatively via a secure online survey system. The survey system emailed participants a secure, individualized digital link to complete, with 2 automatic follow-up emails sent if they did not complete it. After this, if no response was obtained, an independent researcher (C.H.) contacted the participant by telephone, with a minimum of 3 follow-up telephone calls on separate occasions before they were deemed lost to follow-up.
Patients were surveyed about injury and surgery to either knee after their index ACLR. In the event of a second ACL injury, details were substantiated in most cases by a review of medical records. Questions on RTS and family history of ACL injury were also asked. Psychological readiness was assessed with the short version of the ACL–Return to Sport After Injury (ACL-RSI) scale, a validated tool developed to measure the psychological impact of returning to sport after ACLR, with higher scores indicating greater psychological preparation. 50 Activity levels were recorded using the Cincinnati Sports Activity Scale (CSAS), in which the functional levels are categorized as follows: level 1—including jumping, hard pivoting, and cutting (eg, soccer, netball, basketball, volleyball, football, and gymnastics); level 2—including running, twisting, and turning (eg, racquet sports, softball, hockey, skiing, and wrestling); level 3—including no running, but twisting and jumping sports (eg, cycling and swimming); and level 4—including no sports, but only activities of daily living. 8 Patient and surgical characteristics—including age, graft diameter, meniscal surgery, and chronicity of ACL injury—were obtained from the prospective database.
Statistical Analysis
Statistical analysis was performed using SPSS software Version 27 (IBM). Statistical significance was set a priori at P < .05. Missing data were not imputed, and a complete case analysis was performed. Age was dichotomized to ≤19 years (adolescent) and >19 years (adult), in accordance with the definition by the World Health Organization. RTS was compared with t tests for linear variables (mean CSAS and ACL-RSI score) and chi-square tests for categorical data (sex, age, family history, and chronicity of injury). Pearson correlation coefficients were calculated for linear variables of age and ACL-RSI score to determine the relationship between age and psychological readiness.
ACL and CACL survival rates were assessed using the Kaplan-Meier method. To account for the variation in the length of the follow-up across all participants, right censoring was performed at 7 years. Factors examined on the univariate analysis included a family history of ACL injury, returning to netball, returning to CSAS level 1 sport, an ACL graft diameter of <7.5 mm, a greater than one-third medial meniscectomy, a greater than one-third lateral meniscectomy, and an age of ≤19 years. A forward method was used to build the multivariate model. Factors with P < .10 on univariate analysis were entered into a stepwise multivariate Cox regression analysis until only the significant factors remained.
Results
Of the 332 female netballers, 1 revoked consent to research, and 64 (20%) were lost to follow-up. A total of 267 (80%) patients were reviewed at a minimum of 7 years from surgery (Figure 1). There was no significant difference between those reviewed at 7 years and those lost to follow-up for the mean age (P = .35), graft size (P = .638), or meniscal treatment (P = .466). The mean follow-up was 8.4 years (range, 7-15 years).

Participant flow through the study inclusion process. ACLR, anterior cruciate ligament reconstruction.
The mean patient age at the time of surgery was 30 years (range, 12-51 years), and 44 patients (17%) were aged ≤19 years. The timing of the surgery was acute (≤3 weeks) in 6 (2%) patients, subacute (1-3 months) in 213 (80%), and chronic (>3 months) in 48 (18%). At the time of ACLR, a one-third partial lateral meniscectomy was performed in 28 (11%) patients, a two-thirds or greater lateral meniscectomy in 17 (6%), and lateral meniscal repair in 15 (6%). A one-third partial medial meniscectomy was required in 2 (1%) patients, a two-thirds or greater medial meniscectomy was required in 43 (16%), and 13 (5%) had a medial meniscal repair.
Grafts were most commonly four-strand (range, 3-6), with a mean diameter of 7 mm (range, 6.5-8.5 mm). The ACL graft was most commonly fixed with a round-headed cannulated interference screw (Smith + Nephew) in 263 (99%) cases on the femoral side and 266 (99%) on the tibial side. At the time of surgery, radiographs showed that the physes were closed in 264 cases (99%) and closing in 3 (1%).
Repeat ACL Injury
ACL graft rupture and CACL rupture were reported in 11 (4%) participants and 27 (10%) participants, respectively, within 7 years (P = .001). The prevalence of any further ACL injury to either knee is shown in Table 1. The median time from ACLR to ACL graft rupture was 25 months, and that for CACL rupture was 5 months (P = .01). One patient sustained both a graft rupture and CACL injury within 7 years.
Prevalence of Any Repeat ACL Rupture Over the 7-Year Study Period a

Data are reported as n (%). Bold P values indicate statistically significant differences between groups (P < .05). ACL, anterior cruciate ligament; CACL, contralateral anterior cruciate ligament.
Adolescents were defined as patients aged ≤19 years; adults were defined as patients aged >19 years.
Survival Analysis
ACL graft survival rates were 99%, 97%, 97%, and 96% at 1, 2, 5, and 7 years after surgery, respectively (Figure 2). On univariate analysis, poorer ACL graft survival was associated with age ≤19 years (hazard ratio [HR], 4.5 [95% CI, 1.4-14.6]; P = .014) (Figure 3). Nonsignificant factors were returning to netball (P = .183), returning to CSAS level 1 sport (P = .152), an ACL graft diameter of <7.5 mm (P = .710), a family history of ACL injury (P = .918), a greater than one-third medial meniscectomy (P = .861), and a greater than one-third lateral meniscectomy (P = .564).

Kaplan-Meier survival chart of the ACL graft and contralateral ACL over 7 years. ACL, anterior cruciate ligament.

Kaplan-Meier survival chart of the ACL graft in adolescents and adults over 7 years. ACL, anterior cruciate ligament.
The native ACL in the contralateral knee had a survival of rate of 100%, 99%, 94%, and 90% at 1, 2, 5, and 7 years, respectively (Figure 2). On univariate analysis, CACL survival was associated with adolescents (HR, 3.4 [95% CI, 1.6-7.4]; P = .002) (Figure 4), returning to CSAS level 1 sport (HR, 12.7 [95% CI, 1.7-93.9]; P = .013), and returning to netball (HR, 2.9 [95% CI, 1.1-7.7]; P = .031).

Kaplan-Meier survival chart of the contralateral ACL in adults and adolescents over 7 years. ACL, anterior cruciate ligament.
The significant factors in multivariate analysis on ACL graft survival and CACL survival are shown in Table 2. Adolescents had a 4.5 times greater hazard for ACL graft rupture (95% CI, 1.4-14.6; P = .014) and a 2.5 times greater hazard for CACL rupture (95% CI, 1.2-5.5; P = .021) compared with adults. CACL injury was also associated with returning to level 1 (jumping, hard pivoting, and cutting) sports (HR, 10.3 [95% CI, 1.4-77.1]; P = .023).
Significant Predictors of 7-Year Survival of ACL Graft and CACL on Multivariate Regression Analysis a
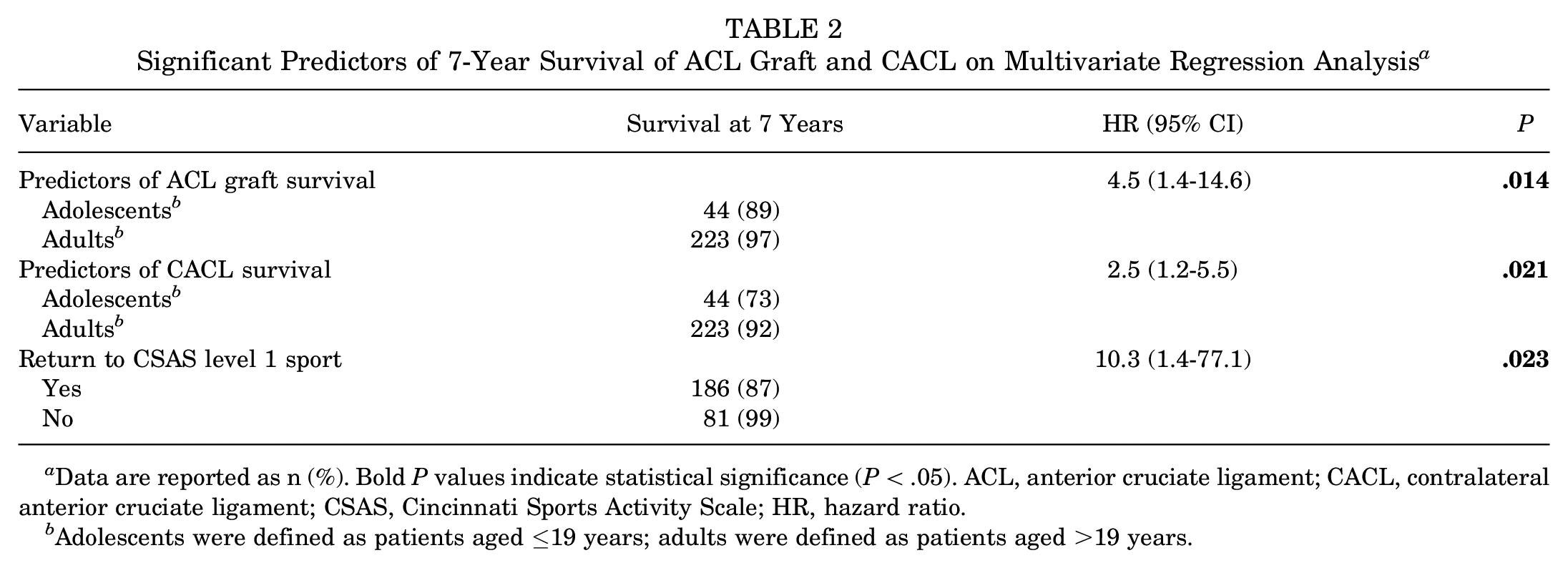
Data are reported as n (%). Bold P values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; CACL, contralateral anterior cruciate ligament; CSAS, Cincinnati Sports Activity Scale; HR, hazard ratio.
Adolescents were defined as patients aged ≤19 years; adults were defined as patients aged >19 years.
Return to Sports
A total of 165 (62%) patients reported a return to netball at any time after their surgery. Returning to netball was reported by 89% (n = 39) of adolescents and 57% (n = 126) of adults (P = .001). Results of the CACL survival analysis according to return to CSAS level 1 sport are shown in Figure 5.

Contralateral ACL survival analysis according to return to CSAS level 1 sport over 7 years. ACL, anterior cruciate ligament; CSAS, Cincinnati Sports Activity Scale.
There were 229 patients with intact ACL and CACL at the follow-up who were invited to complete subjective outcomes at a mean of 110 months (range, 60-181 months). Returning to netball was reported by 134 of 229 (58%) of these patients. Of the 96 who did not return to netball, 67 (70%) reported that it was because of their operated knee, and the remaining patients cited other reasons. The mean CSAS score was 79.
ACL-RSI Scale
Of the 229 patients with an intact ACL graft and CACL 7 years after ACLR, 217 patients completed the ACL-RSI scale, with a mean score of 53. The overall ACL-RSI score was highest in those who had returned to netball (P = .001) but was not affected by age in those without further ACL injury. Age was not significantly correlated with ACL-RSI overall (P = .108) or the Fear of Reinjury subscore (P = .560).
Discussion
The findings of this study demonstrated that ACLR with a hamstring tendon autograft is a suitable option for female netballers who sustain an ACL rupture. Graft rupture and contralateral ACL rupture occurred in 11 (4%) and 27 (10%) female netballers, respectively, at 7 years after ACLR. Returning to netball was seen in 62% of patients. Adolescents were more likely to return to netball and suffer repeat ACL injuries. As expected, greater psychological readiness was also associated with a successful return to netball.
The rate of CACL injury (10%) was more than double that of the ACL graft rupture (4%) in female netballers. In previous studies from our institution, ACL graft and CACL rupture rates were equivalent when examining large cohorts that involved all sports. 45 In a recent study of soccer players from our institution, ACL graft rupture rates were 10%, and CACL injury was 8% at 5 years when both sexes were included. 32 If only female soccer players were evaluated, the rate of ACL graft rupture was 6%, and the rate of CACL rupture was 10% at 5 years (P = .023), similar to that of the netball cohort. These results suggest that a sex bias exists with higher rates of CACL injuries compared with ACL graft injuries after ACLR seen in female netball and soccer players, a phenomenon that is not seen in men. This has implications for tailoring rehabilitation programs in women to ensure that neuromuscular retraining is completed for both knees rather than focusing on the reconstructed side.
In this study, younger age was the only significant predictor of ACL graft rupture. A subsequent ACL injury to either knee was reported by 34% of adolescents, inclusive of 11% sustaining ACL graft rupture and 23% sustaining CACL rupture. Notably, adolescents were 3 times more likely to have a repeat ACL injury of either knee compared with adults. The association between younger age and ACL reinjury after ACLR is well documented and considered multifactorial.1-3,28,41,43,46,51 Younger patients have a greater rate of RTS after ACLR.10,29,51 In this study, 89% of adolescents returned to netball, compared with 57% of adults (P = .001). Secondary to this, age may also be a proxy for other factors, such as higher participation in more strenuous activities and greater risk-taking behaviors. 51
Other considerations of a higher reinjury rate for younger age-groups are postulated to be altered neuromuscular control, biomechanics, and anatomy.22,34,51 ACL injuries in netball typically occur during a dynamic landing task, often a noncontact injury. Video analysis in netballers have described the mechanism of ACL injury associated with knee valgus collapse, with a rotating and laterally flexed trunk upon landing. 49 It is proposed that these biomechanics continue to be altered after ACLR. The JUMP-ACL study reported decreased sagittal plane loading in the reconstructed limb and increased hip adduction and knee valgus in both limbs compared with uninjured, matched controls. 20 Paterno et al 40 reported that altered biomechanics during a dynamic landing task were predictors of second ACL injury. These findings have prompted knee injury prevention programs to be designed in Australia 36 and New Zealand 37 for netball specifically, with subsequent improvements in biomechanics. 23 Heath et al 21 recently reported that although movement quality is moderately associated with physical activity levels, age was a greater predictor, with younger groups having poorer movement quality. It is important to, therefore, promote knee injury prevention programs and counsel on the risks of repeat ACL injury in adolescents.
The rate of return to netball among patients after surgery was 62% at a mean follow-up of 8 years. No other long-term studies have investigated the rates of RTS in netballers. Ardern et al 4 reported that 49% of netballers had returned to some level of the sport at 1 year. As expected, participation rates increase after 1 year. Our results are comparable with those of a meta-analysis of RTS after ACL, which reported a 63% return to preinjury level of participation at a mean follow-up of 42 months. 5 The RTS rate in the present study was slightly lower compared with the 70% rate of RTS in a soccer cohort from the same institution. 32 We hypothesized that the sex-based bias of our cohort contributed to lower levels of RTS, which is supported by results from other studies.4,10 In this study, higher rates of RTS were observed in adolescents compared with adults (89% vs 57%; P = .001). This finding is consistent with those in the ACLR literature29,30 and general sporting populations, where an age-related decline in participation has been observed. 48
Returning to jumping, hard pivoting, and cutting sports was associated with greater odds of CACL injury but not ACL graft rupture. The lack of effect of RTS on graft rupture may be due to the diluting effect of early ACL graft injuries within the first year before an RTS was permitted. After 12 months, all ACL graft ruptures were sustained during jumping, pivoting, or cutting sports. An RTS should be considered to increase the risk of further ACL injury to both knees.14,32
Mounting evidence suggests that psychological factors play an important role in whether patients return to their sports postoperatively.5,16,31 AusPlay, an Australian annual survey of sports participation, identified some top reasons to stop playing netball as “time constraints,”“injury,” and “fear of injury.” 48 There is a known discrepancy in the physical (ie, strength, stability) and activity-based outcomes (eg, International Knee Documentation Committee score) of ACL-reconstructed knees and the RTS rate.4,16 Until recently, physical and functional assessments, in combination with time points, have largely determined the safety of RTS. Increasingly, there are proposals to consider psychological readiness for RTS. In this study, the ACL-RSI score was highest in those who had returned to netball. This finding is consistent with those of previous studies,32,44 with Faleide et al 15 identifying that ACL-RSI of <47 at 9 months after ACLR is a predictor of not returning to sports. A 2020 study by O’Connor et al 38 reported that the traditional strength and power assessment after ACLR has little or no correlation to ACL-RSI scores. This finding indicates that assessing those at risk of having lower psychological readiness is important to ameliorate RTS rates.
Limitations
Because of the self-reported nature of the follow-up in this study, there is an inherent risk that the incidence of ACL graft rupture is higher than reported, as ACL status was not confirmed clinically. Atraumatic ACL graft failures may have occurred and may not be recognized, especially in low-demand patients. To minimize this issue, patients who reported further injuries to either knee during the study period were encouraged to attend an assessment in our clinic. There was a sex bias within this study because of the sports-specific nature of netball, a predominantly female-played sport. As previously discussed, women are more likely to sustain CACL injury and less likely to RTS after ACLR. Further research is needed to determine whether there are sex differences among netballers. The follow-up was achieved in 80% of patients. While we consider this an acceptable rate at 7 years postoperatively, we acknowledge that a higher follow-up rate would allow for greater confidence in the study’s findings. Reassuringly, the characteristics of those lost to follow-up were not significantly different from those reviewed at 7 years postoperatively. Patient-reported outcome measures—including the CSAS and ACL-RSI scores—were only used at the follow-up point and only investigated for those with an intact ACL graft and CACL. Further research is warranted to determine whether these scores change over time and whether they are associated with repeat ACL injury.
Clinical Implications
This study provides clinicians with netball-specific ACLR outcomes to further guide their decision-making and allow their patients to make an informed decision particular to their situation. It guides practitioners to optimize their rehabilitation protocols for those who are at risk of reinjury and suggests that we must continue to consider the psychological readiness of a patient in RTS.
Conclusion
The prevalence of repeat ACL injury was higher in the contralateral knee (10%) than the ACL-reconstructed knee (4%) at 7 years postoperatively. ACLR is suitable for female netballers who sustain an ACL rupture with low long-term graft rupture rates. Repeat ACL injuries were more common in adolescents and those who returned to cutting and pivoting sports. Adolescents had a 1 in 3 chance of repeat ACL injury after ACLR. Notably, at 7 years postoperatively, the prevalence of CACL rupture was more than double the graft rupture rate. Return to netball occurred in 62%, with adolescence and a higher ACL-RSI score being predictors for RTS. The results of this study indicate that further efforts are required to reduce the risk of reinjury in younger populations returning to netball.
Footnotes
Final revision submitted September 15, 2023; accepted October 24, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for this study was received from the Friends of the Mater Foundation and the University of Notre Dame, Sydney. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from St Vincent’s Health Network Sydney (ref No. 18/225).