
Abstract
Background:
Multiligament knee injuries (MLKIs) are traumatic, limb-threatening injuries requiring surgical reconstruction, of which Schenck classification for knee dislocation (KD) 3 and 4 MLKIs are the most serious. Arthrofibrosis is a common complication of multiligament knee reconstruction (MLKR).
Purpose:
This study sought to identify risk factors for arthrofibrosis in Schenck KD 3 and 4 MLKI patients.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Patients with Schenck KD 3 or 4 MLKI who underwent MLKR with a single surgeon were identified retrospectively. Patient sociodemographics, injury characteristics, operative details, and postoperative courses were collected. Patients were divided into groups based on development of postoperative arthrofibrosis, defined as failure to reach a range of motion of 0° to 90° or extensor lag ≥10° by 6 weeks or as undergoing manipulation under anesthesia with or without lysis of adhesions. Univariate and chi-square analyses were used to identify associations with arthrofibrosis, and logistic regression was used to confirm risk factors. Statistical significance was defined as P < .05.
Results:
A total of 71 patients with a mean age of 31.5 ± 10.6 and mean follow-up time of 25.1 months were included. Of this total, 23 (32.4%) developed arthrofibrosis postoperatively. Characteristics and variables associated with arthrofibrosis were younger age (28.0 ± 10.4 vs 33.5 ± 10.4 years; P = .04), higher median household income by zip code ($107,066 ± $40,536 vs $83,911 ± $28,530; P = .007), worse preoperative flexion (98.1°± 30.5° vs 120.6°± 22.1°; P = .002), quicker time from injury to surgery (81.6 ± 74.2 days vs 232.5 ± 307.3 days; P = .03), and significantly longer time to return to weightbearing as tolerated (12.0 ± 9.0 weeks vs 7.0 ± 3.4 weeks; P = .005). There were no differences in race, sex, body mass index, insurance type, preoperative extension, use of external fixation, mechanism of injury, or concomitant meniscal repair (P > .05). Logistic regression identified younger age, preoperative flexion, and time to weightbear as risk factors for arthrofibrosis (P = .004, .014, .019, respectively).
Conclusion:
A third of MLKI KD 3 and 4 patients who underwent reconstruction developed arthrofibrosis. Younger patients, those with worse preoperative flexion, and those who take longer to return to weightbearing as tolerated are at risk of arthrofibrosis. Time to weightbearing and preoperative flexion may be modifiable by prehabilitation or manipulation under anesthesia at earlier stages.
Multiligament knee injuries (MLKIs) are some of the most complex orthopaedic injuries with potentially devastating consequences. They often occur as a result of high-energy trauma and can be limb threatening due to frequent concomitant nerve and vascular injuries.19,23 Alternatively, MLKIs can occur after low-energy mechanisms, especially in obese patients. 28 MLKIs can be classified by the Schenck Knee Dislocation (KD) system, which uses the pattern of ligamentous injury. 21 KD 3 and 4 injuries are the most severe, involving both cruciate ligaments and ≥1 collateral ligament. 21 Surgical intervention in the form of multiligament knee reconstruction (MLKR) with either single- or multistage surgery is the standard of care for KD 3 and 4 injuries.9,26
Arthrofibrosis is a known complication after MLKR and negatively affects the postoperative outcomes given its association with limitation in the knee range of motion (ROM) and pain.1,6 Certain knee injuries, including higher-grade MLKIs (KD 3 and 4), are risk factors for arthrofibrosis. 6 The development of arthrofibrosis after MLKR surgery is challenging, as it delays the recovery process and can require a return to the operating room for manipulation under anesthesia (MUA) and/or lysis of adhesions (LOA). 6 This creates additional financial and physical burdens for patients.
The development of arthrofibrosis after MLKR is not fully understood. To avoid hurdles in recovery and additional trips to the operating room, we must evaluate the patient variables and operative factors associated with this complication. This study sought to assess variables associated with postoperative arthrofibrosis in patients with Schenck KD 3 and 4 injuries.
Methods
Patient Selection
This study received approval by the University of Southern California's institutional review board. Patients diagnosed with MLKI Schenck KD class 3 or 4 injuries were retrospectively identified. To be included, patients had to have undergone MLKR with a single surgeon at 1 of 2 institutions, one of which is a tertiary care referral center. Patients were excluded if they had incomplete sociodemographic information or had <6 weeks of follow-up. Patients were not excluded based on chronic conditions or social habits including smoking, alcohol use, and so forth.
Data Collection
Patient characteristics and sociodemographics including sex, age at surgery, body mass index (BMI), race, insurance type, and median household income by zip code. The US census was used to identify median household income by patient zip code. 24 Preoperative data collected included injury mechanism, days between injury and surgery, ROM, and use of external fixation. Intraoperative data collection included staged versus unstaged surgery, concomitant meniscal procedures, and intraoperative complications. Postoperative course including complications, return to surgery, time to return to weightbearing as tolerated, and ROM were recorded. Postoperative arthrofibrosis was defined as failure to meet a ROM of 0° to 90° by 6 weeks postoperatively and/or extension lag (lack of extension of >10° compared with the contralateral side) by 6 weeks postoperatively and/or any return to the operating room for MUA with or without LOA. Patients taken back to the operating room for MUA and/or LOA were those with notable <90° ROM, for example, limited to 60°. For patients who were close to 90°, such as those at 85°, they were grouped into the arthrofibrosis category but did not return to the operating room. Patients with a lack of extension, for example, 5° to 10°, returned to the operating room.
Procedure
For MLKR, all patients underwent the same surgical techniques by a single surgeon (G.F.R.H.). Each MLKR started with an examination under anesthesia and a diagnostic arthroscopy of the knee. This was followed by reconstruction of ligaments using almost exclusively allografts. Any use of autografts will be documented within the Results section. Posterior cruciate ligament reconstructions were performed with the double-bundle technique. Posterolateral corner technique was the anatomic LaPrade 2-limbed technique. Medial collateral ligament reconstructions were performed with 2 limbs (medial collateral ligament and posterior oblique ligament) but with a single origin at the medial collateral ligament. Arthroscopic techniques were used for posterior and anterior cruciate ligaments.
Postoperative Rehabilitation
Postoperative rehabilitation varied slightly based on the institution of MLKR. Postoperative plans for all patients began with 6 weeks of nonweightbearing, at which point they advanced to full weightbearing over a 4-week period. This weightbearing protection phase is based on the philosophy and descriptions of protocols by Fanelli. 8 At one institution, hinged knee braces were used immediately postoperatively, set at 0° to 90° for the first 2 weeks and then opened to full ROM. Continuous passive motion machines were also used immediately postoperatively. The continuous passive motion machines were set at 0° to 90° on the day of surgery, with a goal of advancing to 0° to 120° by postoperative week 2. Formal physical therapy was begun 3 days after surgery. At the other institution, knee immobilizers were utilized until patients received hinged knee braces at their first postoperative office visit at 2 weeks. The recommendation for outpatient physical therapy was a minimum of 2 sessions per week over 12 weeks. No prophylactic medications for arthrofibrosis were used as part of the postoperative protocol for any patient.
Statistical Analysis
Patients were grouped by whether or not they developed arthrofibrosis. Patient characteristics, preoperative details, intraoperative data, and postoperative courses were compared between patients. Differences in demographic and surgical variables between patients with and without arthrofibrosis were assessed using the Student t test for continuous variables and the chi-square test for categorical variables. To identify independent risk factors for arthrofibrosis, multivariate logistic regression was performed, adjusting for relevant confounding variables. Statistical significance was defined as P < .05.
Results
A total of 71 patients (18.3% female) with a mean age of 31.5 ± 10.6 and a mean follow-up time of 25.1 ± 30.9 months were included. The mean time to surgery was 242 ± 538 days. Seven (10%) patients had KD 4 injuries. Of the KD 3 patients, 24 had medial KD 3 injuries and 40 had lateral KD 3 injuries. Only 3 (4%) patients’ procedures included the use of autografts.
Arthrofibrosis
Arthrofibrosis developed in 23 (32.4%) of patients. Arthrofibrosis was not associated with KD 3 versus KD 4 injuries (P = .18) or with KD 3 medial versus KD 3 lateral injuries (P = .62). Thirteen (18.3%) patients underwent MUA or LOA, 4 of whom required multiple returns to the operating room for MUA or LOA. The mean time to MUA from initial surgery was 97.53 ± 17.4 days. There were no associations between arthrofibrosis and sex, race, insurance type, BMI, time from injury to surgery, mechanism of injury, procedure staging, or use of external fixation (P > .05) (Tables 1-3). Postoperative rehabilitation protocol, which varied by institution of surgery, was not associated with arthrofibrosis (P = .92). The mean age of patients who developed arthrofibrosis was significantly lower than those who did not (28.0 ± 10.4 vs 33.5 ± 10.4; P = .04). A higher median income by zip code was also found in patients with arthrofibrosis ($107,066 ± $40,536 vs $83,911 ± 28,530; P = .007). Those who developed arthrofibrosis also demonstrated a significantly worse preoperative flexion range compared with those who did not (98.1°± 30.5° vs 120.6°± 22.1°; P = .002). Time from injury to surgery was significantly shorter in those who developed arthrofibrosis (81.6 ± 74.2 days vs 232.5 ± 307.3; P = .03). Arthrofibrosis patients also took significantly longer to return to weightbearing as tolerated (12.0 ± 9.0 weeks vs 7.0 ± 3.4 weeks; P = .005). There was no association with concomitant meniscal repair (Table 1).
Patient Sociodemographics and Courses Compared Between Patients Who Did Not Develop Arthrofibrosis and Those Who Did a

Data are presented as n (%) or mean ± SD. Bold P values indicate statisitcal significance. The t test is used for continuous variables, and chi-square is used for categorical variables. BMI, body mass index.
Percentage for categorical variables.
Insurance Payer Distribution Analysis Using Chi-Square a
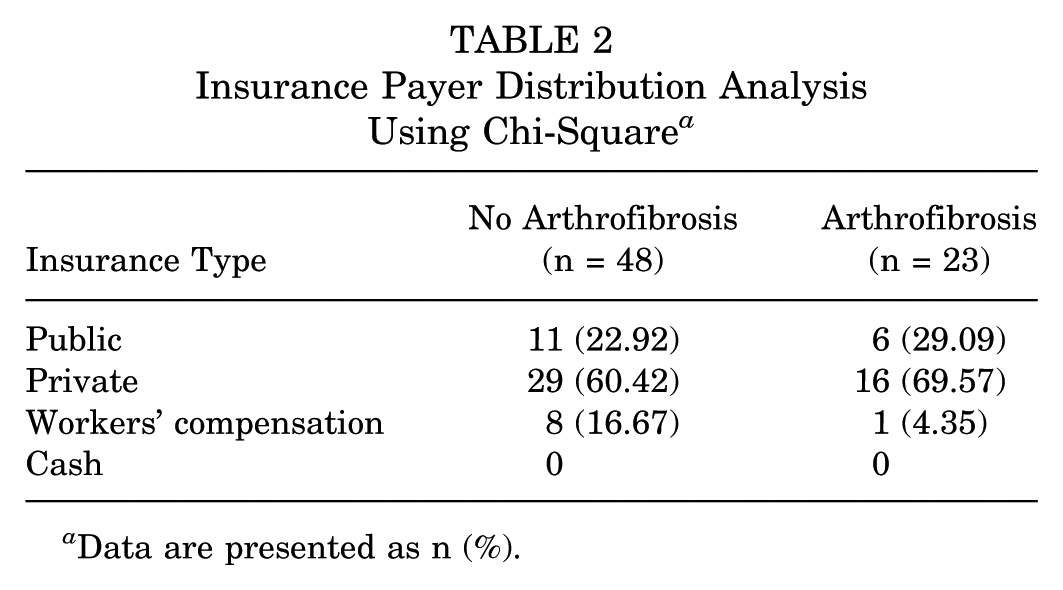
Data are presented as n (%).
Racial Distribution of Patients With and Without Arthrofibrosis Analysis Using Chi Square a

Data are presented as n (%).
Upon logistic regression, age, preoperative flexion, and time to return to weightbearing all remained significant (Table 4). Time to surgery and income by zip code were no longer significant.
Logistic Regression Identifying Risk Factors for Arthrofibrosis a
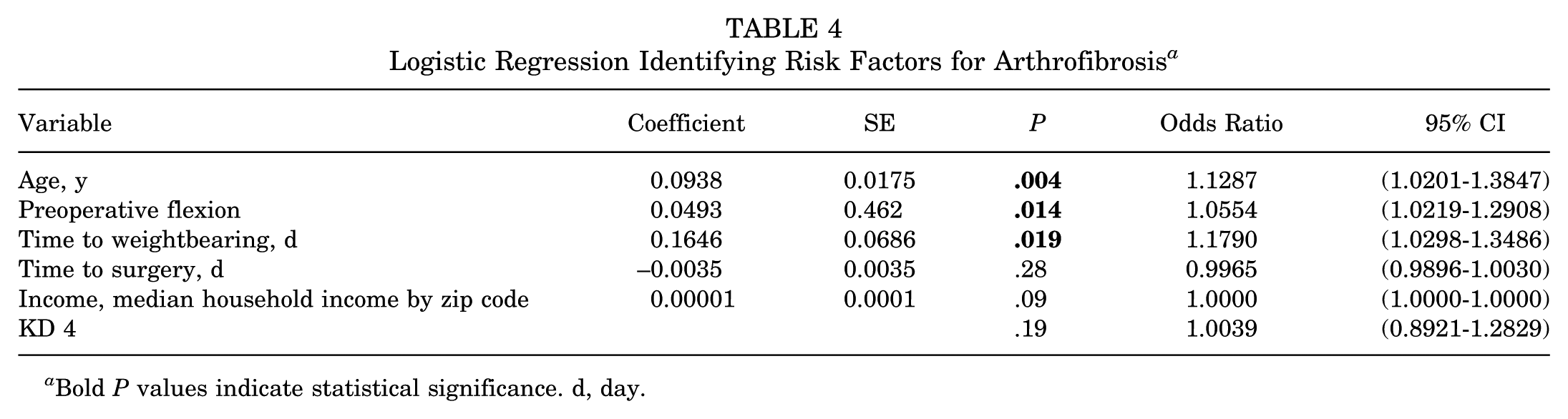
Bold P values indicate statistical significance. d, day.
Discussion
In Schenck KD 3 and 4 patients undergoing MLKR, arthrofibrosis was a common postoperative complication. Multiple patient-specific variables were associated with arthrofibrosis, including younger age and higher median household income by zip code. Preoperatively, a reduced flexion range and shorter time from injury to surgery were also associated with arthrofibrosis. Concomitant meniscal procedures did not differ between patients who developed and patients who did not develop arthrofibrosis. Those with arthrofibrosis also took significantly longer to return to weightbearing as tolerated. When accounting for confounding variables within the logistic regression, younger age, preoperative flexion, and time to weightbearing were all found to be risk factors for arthrofibrosis in Schenck KD 3 and 4 MLKI patients.
Patients who developed arthrofibrosis demonstrated a shorter time to surgery than those who did not, indicating there may be benefit in prolonging the preoperative period. In a systematic review incorporating >4,000 MLKI patients, Özbek et al 20 found that patients who underwent surgery within 3 weeks of MLKI had increased odds of postoperative stiffness. Cook et al 4 also demonstrated that patients treated acutely were more likely to require MUA. The concept of prehabilitation has been widely applied in anterior cruciate ligament reconstruction, where research consistently demonstrates better outcomes in patients who undergo rehabilitation before surgery focused on strengthening and ROM.7,11,22 Given that our study also found that patients with worse preoperative flexion ROM was a risk factor for arthrofibrosis, there may be a role for focusing on improving ROM before proceeding to surgery in MLKI patients. More research is required to determine if there is an ideal time point at which MLKR should be completed following injury and whether or not prehabilitation focused on ROM may improve postoperative outcomes.
The direction of the association between arthrofibrosis and delayed return to weightbearing is unclear. It is possible that those who developed arthrofibrosis took longer to return to weightbearing as a result of their arthrofibrosis. Alternatively, a slow return to weightbearing may have contributed to the development of their stiffness due to limited postoperative mobility. There is likely some degree of bidirectionality in this relationship. In patients undergoing total knee arthroplasty, one of the goals of rehabilitation is early mobility to prevent arthrofibrosis. 3 Weightbearing helps force increased mobility, which may be beneficial in preventing the formation of scar tissue that contributes to stiffness. The introduction of mobilization must be done gradually and carefully, though, as evidence suggests early mobilization that is too aggressive can exacerbate inflammation and fibrosis. 13 Korber et al 15 demonstrated that highly regimented weightbearing progression versus variable progression of weightbearing after MLKR did not affect patient-reported outcomes, but this study did not specifically examine arthrofibrosis. Outcomes also did not vary by use of hinged knee brace versus knee immobilizer in this study. 15 Time to return to weightbearing as tolerated may be a confounding variable given the potential bidirectionality. More research specifically investigating various postoperative weightbearing protocols is required to understand the direction of the association identified here. Surgeons should promote weightbearing in gradual, supervised fashion during the postoperative course to encourage mobility.
The association between younger age and arthrofibrosis is relatively surprising. Research on orthopaedic procedures has often demonstrated that younger patients exhibit fewer complications and better outcomes.16,17,27 This holds true for ligamentous knee procedures as well. Hopper et al 12 found that older age was associated with an increased risk of MUA or LOA in patients undergoing anterior cruciate ligament reconstruction. On the other hand, the association of increased risk of MUA or LOA with younger age has been identified within the knee arthroplasty literature. In patients undergoing total or unicompartmental total knee arthroplasties, younger patients were more likely to undergo revision due to arthrofibrosis. 25 Younger age was the strongest predictor of requiring LOA for arthrofibrosis after total knee arthroplasty in Cregar et al. 5 This has also been observed in the orthopaedic pediatric population, where Bram et al 2 demonstrated that younger patients were more likely to develop arthrofibrosis after surgery for tibial spine fractures. It is unclear why younger patients undergoing MLKR were more likely to develop arthrofibrosis. One possible explanation is that younger patients may have a stronger interest in maintaining a certain level of activity and therefore may be more likely to seek treatment for ongoing stiffness. However, the mean age of those without arthrofibrosis was 33 years, and it is unlikely that patients in their 30s are significantly less active than those in their late 20s. Another possibility is that younger patients may be less diligent or compliant with rehabilitation protocols; however, multiple studies demonstrate that noncompliance is multifactorial. 10 Although the exact mechanism is not understood, surgeons should keep in mind that younger patients may require or benefit from more rehabilitation focused on ROM.
In addition to mechanical influences of arthrofibrosis, there is also the potential for immunologic mechanisms at play in a patient's risk for arthrofibrosis. While not investigated here and lacking within the MLKI literature, immune cell populations have been shown to differ between patients with arthrofibrosis and those without arthrofibrosis in the knee arthroplasty literature. Limberg et al 18 compared the immune cell populations from tissue of the posterior capsule in patients undergoing revision total knee arthroplasty for either arthrofibrosis or for nonarthrofibrotic, noninfectious indications. This study found significant differences in immune cell concentrations in those patients with arthrofibrosis compared with those without, including differences in CD163+ macrophages and CD117+ mast cells. Limberg et al also demonstrated a correlation between immune cell populations and patient age, suggesting another potential mechanism at play in why younger patients are at higher risk for arthrofibrosis. Additional research is required to elucidate the role of immune cells in the development of arthrofibrosis in MLKI patients and to analyze whether this may affect the relationship between arthrofibrosis and patient age.
Another variable linked to postoperative stiffness was a higher median household income based on zip code. This result is unexpected, as one might assume that higher-income patients would have better access to rehabilitation resources. Multiple studies on ligamentous knee surgery have demonstrated that higher socioeconomic status is associated with better outcomes.14,29 It is unclear why MLKI patients with lower socioeconomic status were less likely to develop postoperative arthrofibrosis. To speculate, several variables may play a role in this association. For example, this variable represents the median household income of the zip code in which the patient lives and not the exact income of the patient. Patients from lower-income zip codes, though, may be more likely to live in apartments, condos, or older homes with limited accessibility features; these patients also may be more likely to rely on public transportation. As a result, patients from lower socioeconomic status may be forced to use stairs or walk further distances earlier on postoperatively, increasing their mobility. Another potential factor could be a greater urgency to return to work, which may encourage earlier mobility, particularly for those in physically demanding jobs. It is critical to note that despite being lower income relative to the nonarthrofibrosis group, their mean household income of >$80,000 is higher than the national average. Additionally, median household income by zip code is not a patient-specific number and this should be kept in mind when considering this finding; however, it is a useful measure for estimating patient socioeconomic status. There are likely several confounding variables at play in this association, which is confirmed by the lack of association identified by logistic regression.
Limitations
This study has several limitations. One of which is a relatively small patient group, as Schenck class 3 and 4 MLKIs are rare injuries, which makes them difficult to investigate. Our analysis into how KD 3 versus 4 injuries affected arthrofibrosis is underpowered due to a much larger proportion of patients in the KD 3 category. Using patients from a single surgeon strengthens the study by removing a potential confounding variable in different surgeons and varying techniques but limits the size of the patient cohort. Furthermore, the use of a single surgeon limits generalizability. However, including patients from both private and public institutions may help to improve generalizability. The inclusion of patients from both institutions, though, did create a difference in postoperative rehabilitation protocols. Importantly, as a tertiary care center, a majority of these patients were sent to our team by referral and did not present to our care until often months or years after their initial injuries. As such, we did not collect data on associated injuries, including neurovascular injuries, as these data were inaccessible for many patients and would therefore be inconsistent across the patient population. This is a notable weakness of this study, and future investigations into arthrofibrosis after MLKR would strengthen the current literature by including a specific analysis into how associated neurovascular injury may play a role.
Conclusion
Arthrofibrosis after MLKR in Schenck 3 and 4 patients is associated with younger age, higher median income by zip code, shorter time to operation, reduced preoperative flexion ROM, and longer time to return to weightbearing. Further research is required to elucidate what the ideal time to surgery is after MLKI and whether prehabilitation focusing on ROM may reduce the incidence of postoperative arthrofibrosis.
Footnotes
Final revision submitted July 13, 2025; accepted August 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.N.L. has received speaking and lecture fees from Stryker Orthopaedics and travel fees from Innocoll Biotherapeutics NA Inc. S.C.G. is involved in other professional activities with Zimmer Biomet Holdings, Inc. G.F.R.H. is a paid consultant and presenter or speaker for Arthrex Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Southern California (No. UP-21-00988).