
Abstract
Background:
Multiligament knee injuries (MLKIs) due to high-energy (HE) or polytraumatic (PT) mechanisms result in worse patient outcomes after surgery versus low-energy (LE) or nonpolytraumatic (NPT) mechanisms. There remains a paucity of research in the literature investigating MLKIs resulting from these mechanisms of injury.
Purpose:
To characterize differences in ligamentous injury/surgery patterns between different mechanism groups: HE versus LE and PT versus NPT.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This is a retrospective chart review of consecutive surgical MLKIs from a single institution. Demographics, clinical/radiographic findings, and intraoperative variables were obtained. HE versus LE mechanisms were stratified. Patients with inadequate data were excluded. PT versus NPT classifications were based on presence of concurrent nonknee injuries. Subgroup comparisons were made based on body mass index, age, sex, number/type of ligaments injured, and surgeries performed.
Results:
From a total of 226, 176 (78%) patients were included (41 PT [23%] and 135 NPT [77%]; 62 HE [35%] and 114 LE [65%]). PT mean age was 30.7 ± 13.7 years (male, 32 [78%)], while NPT mean age was 27.1 ± 12.3 years [male, 91/135 [67%]). HE mean age was 31.4 ± 13.1 years (male, 49/62 [79%]), and LE mean age was 25.6 ± 11.8 years (male, 73/114 [64%]). Posterior cruciate ligament (PCL) injuries were higher in PT (27/41 [66%]) and HE (42/62 [68%]) versus NPT (58/135 [43%]) and LE (44/114 [39%]), respectively. Lateral collateral ligament (LCL) injuries were higher in PT (29/41 [71%]) and HE (41/62 [66%]) versus NPT (66/135 [49%]) and LE (55/114 [48%]), respectively. The mean number of ligaments injured was higher in PT versus NPT (2.9 vs 2.4) and in HE versus LE (2.8 vs 2.4). LCL surgical interventions were more common in PT (23/41 [55%]) versus NPT (49/135 [36%]) and in HE (33/62 [53%]) versus LE (39/114 [34%]). No other differences in injuries/surgeries existed between PT and NPT or HE and LE, in anterior cruciate, medial collateral, or medial patellofemoral ligaments.
Conclusion:
PT and HE MLKIs are characterized by increased rates of PCL and LCL injuries compared with LE and NPT. HE and PT patients experience more injured ligaments than LE and NPT and are more likely to require reconstruction/repair of the LCL. These findings suggest injury severity and mechanism may facilitate clinical decision making in MLKIs.
Multiligament knee injuries (MLKIs) are severe injuries to the knee joint and can present with heterogeneous injury patterns from varying mechanisms. 15 MLKIs involve partial or complete disruption to ≥2 of the primary knee ligaments: the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and the lateral collateral ligament (LCL). Knee dislocations account for a relatively small fraction of orthopaedic injuries, with a prevalence of approximately 0.02% to 0.2%. 19 They disproportionately affect the male population and are predominantly associated with greater energy incidents, notably motor vehicle accidents,5,16,20 although low- and ultra–low energy mechanisms are also possible. 15 The challenges inherent to MLKI can partially be attributed to their impact on patient functionality and quality of life, as they often occur alongside chondral, meniscal, nerve, and vascular injuries in the knee, or in the setting of polytrauma.1,6,7,15,18
The complexity of MLKIs lies not only in their rarity but also in the broad spectrum of injury severities and patterns they encompass, each presenting unique challenges.1,10 These injuries range from isolated, closed ligamentous disruptions without additional structural damage, to complex polytraumatic (PT) injuries involving additional musculoskeletal and/or nonorthopaedic injuries. It is often the nonligamentous injuries that predict a patient’s functional outcome. 23 This variability necessitates a highly individualized approach to treatment, spanning from nonoperative methods such as limb immobilization to, more commonly, surgical interventions including acute and delayed ligament repair and/or reconstruction.1,10,14 The relative infrequency of these injuries has led to a dearth of large-scale, definitive clinical studies, resulting in an ongoing debate and lack of consensus regarding key management strategies.2,3,9,12,17,20
It is widely known that MLKIs can result from a variety of different injury mechanisms, including motor vehicle crashes, sports injuries, falls from height, and ground-level falls. Previous studies have commonly used the terms “high energy” (HE), “low energy” (LE), and “ultra-low velocity.” Similarly, previous studies have also categorized MLKIs to evaluate those injuries occurring in the PT setting and those not occurring in the PT setting (NPT) to study the differences in postoperative outcomes.1,4,5,7,14,16,22,23 There is a paucity of research in the literature investigating MLKI in the presence of PT injuries. PT MLKI, characterized by concurrent traumatic injuries to the head, spine, extremities, abdomen, and/or pelvis, is inherently more complex due to the potential for life-threatening injuries. These may naturally take precedence over any semielective musculoskeletal intervention. 20 However, there remains a paucity of information on how these distinct mechanism types—HE and PT—directly relate to MLKI injury patterns.
The objective of this study was to analyze the demographic profiles, ligamentous injury patterns, and surgical treatment patterns stemming from different severity levels of injury (PT vs NPT) and mechanisms (HE vs LE) leading to MLKI. We hypothesized that HE and PT MLKIs would involve different ligamentous injury patterns and surgical treatments, as well as a higher number of injured ligaments, when compared with LE and NPT MLKIs.
Methods
Patient Selection and Clinical Characteristics
All patients surgically treated with ≥2 ligamentous reconstructions/repairs for MLKI at a tertiary academic medical center between April 2008 and October 2022 were retrospectively reviewed. Inclusion criteria consisted of (1) patients diagnosed with MLKI with ≥2 surgically treated ACL, MCL, PCL, and/or LCL, (2) documentation of the mechanism leading to MLKI, (3) availability of magnetic resonance imaging (MRI) reports, and (4) availability of operative reports. Exclusion criteria consisted of (1) revision MLKI surgery, (2) patients treated nonoperatively or with arthroplasty, and (3) patients with chronic MLKI (>1 year from injury to surgery). MLKIs were identified by reviewing operative reports where ≥2 of the ACL, MCL, PCL, and/or LCL were surgically treated through repair or reconstruction. MRI reports were subsequently reviewed to confirm injury patterns and to tabulate all injured ligaments identified. MCL and LCL injuries were graded on a standardized scale from grade 1 to grade 3, with grade 1 indicating mild sprain with minimal fiber disruption, grade 2 representing partial tear with moderate laxity, and grade 3 corresponding to a complete tear with significant instability. Ligamentous injuries on MRI or intraoperatively that were treated nonsurgically, such as partial tears, were included in the data analysis. Demographic variables such as patient age, sex, and body mass index (BMI) were gathered from the patient chart using an electronic medical record (Epic; Epic Systems Corporation). Vascular and peroneal nerve injuries at the time of injury were identified through clinical records and physical examinations, respectively. All clinical data were compiled and maintained in a longitudinal Research Electronic Data Capture (REDCap; Vanderbilt University) database.
Classifications of Mechanisms
MLKIs were classified based on characteristics of the injury mechanism to categorize the mechanism severity: PT or NPT MLKI and HE or LE MLKI. PT MLKIs involve additional traumatic injuries to the head, spine, extremities, abdomen, and/or pelvis. This contrasts with NPT MLKIs, which do not include additional traumatic injuries outside of the knee joint. HE MLKIs are those that typically result from significant external forces such as motor vehicle accidents or falls >1.5 m, which are contrasted with LE MLKI and result from less severe mechanisms like ground-level falls or sports injuries. 16 Ultra–low velocity mechanisms in MLKI are typically seen in the morbidly obese. Due to the low incidence of ultra–low velocity injuries (n = 4), these cases were included in the LE cohort for analysis. Comparisons were made between PT and NPT, and between HE and LE, regarding age, sex, BMI, overall number of ligaments injured, individual ligament injury incidence, and individual ligament injury treatment (repair, reconstruction, or nonsurgical).
Statistical Analysis
Data were exported from the REDCap database and imported into SPSS Version 27 statistical software (IBM Corp). Shapiro-Wilks test for normality of data was completed to assess normality. Student t test was used for continuous variable comparisons. Chi-square analysis to test association was completed for all categorical variable comparisons. Statistical significance was set at P < .05.
Results
Demographics and Injury Mechanisms
From an initial database of 226 patients, 176 patients (78%) with MLKIs met the inclusion criteria, including 41 (23%) PT and 135 (77%) NPT injuries, respectively. The PT mean age was 30.7 years (range, 12-65; SD, 13.7), while the NPT mean age was 27.1 years (range, 5-63; SD, 12.3) (P = .17). The mean BMI was 29.5 kg/m2 (SD, 8.4) for the PT group, compared with 28.3 kg/m2 (SD, 7.5) for the NPT group (P = .39). There was no difference in sex distribution for PT versus NPT: male patients, 78% (32/41) versus 67% (91/135), respectively (P = .09) (Figure 1 and Table 1).

Flowchart of patient inclusion and exclusion criteria.
Demographics of Polytraumatic and Nonpolytraumatic MLKI Cohorts a

Data are reported as mean ± SD or n (%). BMI, body mass index; MLKI, multiligament knee injury; MVC, motor vehicle collision.
The HE versus LE MLKI analysis included 176 patients, with 62 (35%) HE and 114 (65%) LE mechanisms. The mean age of 31.4 years (SD, 13.1; range, 12-65 years) for the HE subgroup was significantly higher than the LE subgroup’s mean of 25.6 years (SD, 11.8; range, 5-63 years) (P = .003). The mean BMI did not differ: 29.5 kg/m2 (SD, 8.4) for HE and 28.0 kg/m2 (SD, 7.2) for LE (P = .21). Male patients comprised 79% of the HE subgroup and 64% of LE (P = .11) (Table 2). In terms of mechanisms, the most common mechanism for PT and HE MLKI was motor vehicle collisions at 85% and 68%, respectively. The highest frequency of NPT and LE MLKI was sports injuries at 56% and 68%, respectively (Tables 1 and 2). Among the PT cases, 85% (35/41) occurred due to HE mechanisms, while the remaining 15% (6/41) were attributed to LE mechanisms. Conversely, in the NPT group, 20% (27/135) were associated with HE mechanisms, whereas 80% (108/135) resulted from LE mechanisms. This overlap analysis highlights the predominant association of PT injuries with HE mechanisms, in contrast to NPT injuries, which were more frequently linked to LE mechanisms (Figure 2).
Demographics of HE and LE MLKI Cohorts a

Data are reported as mean ± SD or n (%). BMI, body mass index; HE, high energy; LE, low energy; MLKI, multiligament knee injury; MVC, motor vehicle collision. The mean age of HE was statistically greater than those of LE mechanisms at a significance threshold of P < 0.05, shown in bold text.
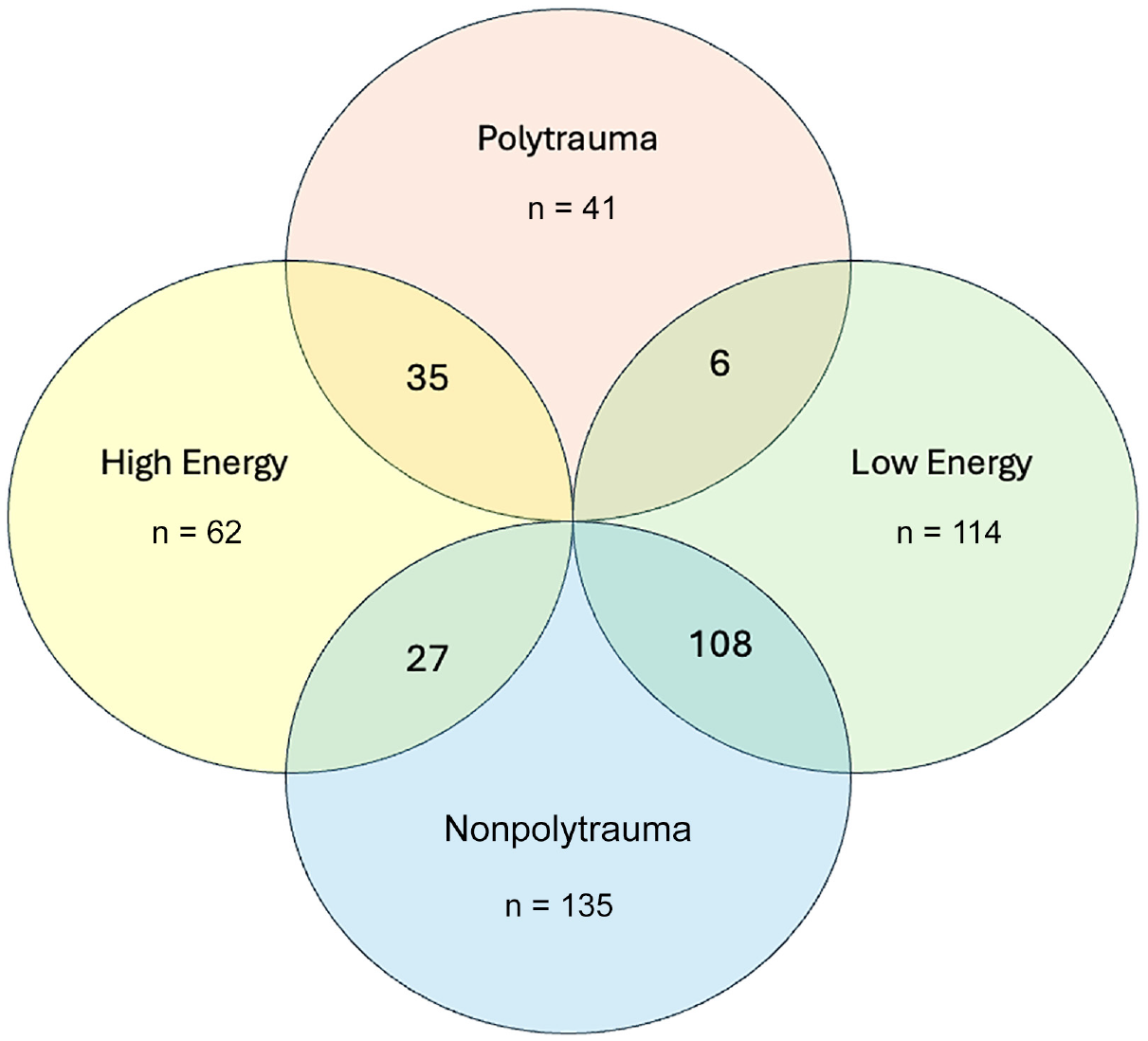
Venn diagram depicting the convergent characteristics of patient cohorts with multiligament knee injury: high energy, low energy, polytrauma, and nonpolytrauma.
Injury and Surgical Intervention Frequencies and Patterns
Incidence of PCL injuries in PT and NPT cases were 66% (27/41) and 43% (58/135), respectively (P = .01). Incidence of PCL injuries in HE and LE were 68% (42/62) and 39% (44/114), respectively (P < .001). The incidence of LCL injuries in PT and NPT cases were 71% (29/41) and 49% (66/135), respectively (P = .01). Incidence of LCL injuries in HE and LE cases were 66% (41/62) and 48% (55/114), respectively (P = .02). The mean number of ligaments injured in PT and NPT cases was 2.9 and 2.4, respectively (P = .006). HE and LE were found to have a mean number of ligamentous injuries of 2.8 and 2.4, respectively (P < .001) (Tables 3 and 4). Bicruciate (ACL and PCL concurrently) MLKIs comprised 37% (15/41) of the PT group, while in the NPT group this pattern was seen in 28% (38/135) of cases (P = .30). In HE mechanisms, bicruciate MLKIs were present in 35% (22/62) of cases, while in LE mechanisms they were present in 27% (31/114) of cases (P < .25). Concerning LCL surgical intervention, PT cases had a rate of 56% (23/41), while NPT cases had a rate of 36% (49/135) (P = .04). The rate of LCL surgical intervention in the HE cases was 53% (33/62), while LE cases had a rate of 34% (39/114) (P = .01). There were no other differences in rates of ligamentous injury or surgical intervention (ACL, MCL, MPFL) based on energy of injury nor incidence of additional trauma (Tables 3 and 4).
Ligamentous Mechanism, Injury and Radiographic Grading, and Surgeries a

Data are presented as n (%) unless otherwise indicated. Rates of PCL injury, LCL injury, grade 2 LCL injury, LCL surgery, and mean number of ligaments injured were significantly increased in the polytrauma group compared to the non-polytrauma group at a significance level of P < 0.05, shown in bold text. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; MPFL, medial patellofemoral ligament; PCL, posterior cruciate ligament; STD, standard deviation.
Ligamentous Mechanism, Injury and Radiographic Grading, and Surgeries a

Data are reported as n (%) unless otherwise indicated. Rates of PCL injury, LCL injury, grade 2 LCL injury, LCL surgery, and mean number of ligaments injured were significantly increased in the high energy mechanism group compared to the low-energy group at a significance level of P < 0.05, shown in bold text. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; MPFL, medial patellofemoral ligament; PCL, posterior cruciate ligament; STD, standard deviation.
The incidence of vascular injury in the PT and NPT cases was 7% (3/41) and 4% (5/135), respectively (P = .65). Vascular injuries were found in the HE and LE cases at rates of 3% (2/62) and 5% (6/114), respectively (P = .70). Incidence of peroneal nerve injury was found to be 24% in both the PT (10/41) and the NPT (33/135) cohorts (P = .68). The incidence of peroneal nerve injury in HE and LE cases was 29% (18/62) and 22% (25/114), respectively (P = .32).
Discussion
Our study elucidates an association between the mechanism of MLKIs and their severity, with HE and PT mechanisms more likely involving PCL and LCL injuries and necessitating greater rates of LCL surgical intervention. Additionally, the mean number of ligaments injured in MLKIs resulting from HE and PT mechanisms is greater compared with those from LE and NPT mechanisms. These observations are critical for understanding the complex nature of MLKI patterns and planning effective orthopaedic surgical interventions.
To date, no universally accepted classification specifically dedicated to describing mechanisms leading to MLKIs has been established. Most classifications for describing ligamentous patterns in MLKI are descriptive in nature. A 2018 study by Everhart et al 8 provided evidence that the commonly used system, the Schenk classification, does hold prognostic value. However, other studies have demonstrated that this may not be the case.11,21 Systems for classifying the mechanisms causing knee dislocation have commonly been adapted for this purpose. One classification system used as such is the Energy of Injury Classification. It is divided into high, low, and ultra-low energy mechanisms. 19 Previous research using this adapted classification system for MLKI has focused on associated vascular injury and postoperative outcomes. A study by Wascher 22 reported the increased incidence of vascular injury in HE MLKI mechanisms. A study by Engebretsen et al 7 evaluated the postoperative knee function of patients suffering MLKI sustained in HE and LE mechanisms, demonstrating favorable outcomes in the LE mechanism group. Alternatively, Dean et al 5 demonstrated in a meta-analysis that while postoperative activity levels are higher in LE patients, the functional outcomes do not differ. There remains a paucity in the literature, however, linking the mechanism severity to ligamentous injury patterns. The present study presents a delineation in the injury pattern observed in MLKIs with varying degrees of defined mechanism severity.
It is known that PT mechanisms causing MLKIs produce worse outcomes when compared with those caused by NPT mechanisms. 23 The occurrence of MLKI in conjunction with other PT injuries is not uncommon and introduces clinical complexities that can alter the course of treatment. This population of patients with MLKIs must be handled on a case-by-case basis, as the concurrent injuries sustained can delay and/or prolong rehabilitation postoperatively and lead to worse outcomes due to factors other than the knee. 23 Previous studies have demonstrated that PT MLKIs with other complicating injuries result in worse outcomes than those without complicating injuries postoperatively.4,23 A study by Darcy et al 4 found that patients suffering PT MLKIs had worse outcomes at 12 months. Similarly, a matched-cohort study of 31 patients by Woodmass et al 23 demonstrated that, despite restoration in similar range of motion and knee stability, PT MLKIs result in worse functional outcome scores than those of NPT MLKIs. These studies have elucidated a pivotal aspect of MLKI management, underscoring the criticality of data stratification in accordance with polytrauma status, as these mechanism factors lead to significantly different trajectories for patient outcomes. However, while these studies help characterize the increased severity of MLKI with concurrent PT injuries, they do not elucidate how mechanism severity causing concomitant PT injuries relates directly to the ligamentous patterns observed in MLKI. The present study adds to previous literature by demonstrating the differences in both injury patterns and surgical fixation of MLKIs in the setting of HE, LE, PT, and NPT mechanisms leading to injury.
MLKIs and knee dislocations are often used interchangeably and studied simultaneously in the literature. However, this approach does not consider the types of injuries incurred as it pertains to the level of injury sustained. Previous studies have commonly relied on analyzing the incidence of MLKI in relation to knee dislocations. 16 A study by Kaeding et al 13 found the ACL to be the most injured ligament, involved in 99.2% of their retrospective study of 279 MLKI cases. The study further detailed the frequency of other ligamentous injuries in descending order: MCL, fibular collateral ligament (FCL), and PCL. 13 The findings of the present study are concordant with their reported incidences. However, the study conducted by Kaeding et al overlooks a crucial aspect in its analysis: the categorization and differentiation of MLKIs based on their mechanism of injury. As previously elucidated, the causative mechanism of MLKI plays a substantial role in determining patient outcomes. When contextualized with the current state of the literature, it becomes evident that HE and PT mechanisms leading to MLKIs lead to increased PCL and FCL injuries and ultimately increased rates of FCL surgical intervention. This is especially relevant at level 1 trauma centers, where knee surgeons are more likely to encounter and treat MLKI of these mechanisms compared with those in community hospitals. As described above, these injury patterns may suggest worse postoperative activity levels or functional outcomes. Additionally, the current study revealed that, if present, MPFL injuries were not likely to undergo surgical intervention regardless of injury mechanism.
Limitations
This investigation acknowledges several inherent limitations. First, the retrospective design of this study poses constraints, particularly in terms of data availability and potential biases inherent in historical data collection and surgeons’ selection biases. Second, the sample size of this study, though adequate, remains comparatively smaller than that of previous research delving into MLKI injury patterns. However, when compared with studies investigating mechanism severity in MLKI injuries, the present study comprises a much larger cohort. Furthermore, although the definitions of HE and LE injuries have been established previously in the literature, there is no way to quantify the extent of energy imparted from an injury mechanism. Thus, there may be “low energy” injuries that in reality resulted from an excessive amount of force but were classified as such based on the mechanism described. Despite this, the classification scheme utilized has been published prior 5 and has provided a clean way to subgroup our patients’ injuries. An additional limitation arises from the study’s patient population’s being exclusively drawn from a single hospital system. While this may raise concerns about the representation of the findings, it is important to note that the data were meticulously compiled by 4 distinct orthopaedic sports surgeons (J.J.E., S.K.A., T.G.M., P.E.G.) at a tertiary academic (level 1 trauma) center that receives MLKI referrals from ≥5 surrounding states. This approach offers a comprehensive perspective that we believe mirrors broader patient demographics and injury patterns. Consequently, while acknowledging these limitations, we maintain that the insights gleaned from this study contribute valuable understanding to MLKI injury research.
Conclusion
MLKIs caused by HE mechanisms or in PT patients cause increased rates of injury to the PCL and LCL as compared with LE and NPT. As suspected, HE and PT patients experienced a greater number of injured ligaments than LE and NPT. HE and PT were also more likely to require reconstruction/repair of the LCL. These findings highlight the importance of considering both injury severity and mechanism in clinical decision making for the treatment of MLKIs.
Footnotes
Final revision submitted September 5, 2024; accepted September 12, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.F. has received hospitality payments from Stryker and Globus Medical. T.G.M. has received nonconsulting fees from Arthrex, consulting fees from Arthrex, and education payments from Active Medical and Arthrex. S.K.A. has received consulting fees from Stryker. J.J.E. has received consulting fees from Medical Device Business Services and DePuy Synthes Products; a grant from Arthrex; education payments from Arthrex, Gemini Mountain Medical, and Smith & Nephew; and hospitality payments from DePuy Synthes Sales. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.