
Abstract
Background:
Posterolateral corner (PLC) lesions and knee dislocations (KDs) have been recognized as risk factors for vascular and neurological injuries in patients with multiligament knee injury (MLKI), but an association between Schenck KD grade and neurovascular lesions has yet to be established.
Hypothesis:
The ligamentous injury pattern in MLKIs with high KD grades will be associated with a higher likelihood of vascular and neurological injuries.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Included were 144 patients from a multicenter database with surgically treated MLKI. All patients were skeletally mature, had MLKI lesion identified on magnetic resonance imaging and confirmed intraoperatively, and did not have any previous knee surgery or previous vascular or neurological lesions. Demographic data (sex, age), injury mechanism (high energy, sports injury, low energy), ligaments injured, and neurological and vascular lesions were recorded. A new classification for MLKI based on ligamentous injury pattern, and intended for all MLKIs (with and without KD) was developed, and all patients were categorized according to this classification. Associations were evaluated between the risk of vascular and neurological lesion and demographic data, injury mechanism, and new classification grade.
Results:
The mean patient age was 33.9 years (range, 15-64 years), and 72% were male. High-energy trauma was the most common injury mechanism (55.6%). Vascular injury was present in 5 patients (3.5%) and nerve injury in 17 (11.8%), with 1 patient (0.7%) having both. None of the analyzed variables were associated with the presence of vascular lesion. Univariate logistic regression showed that medial collateral ligament (MCL) lesion decreased the probability of neurological injury (odds ratio [OR], 0.29; 95% CI, 0.1-0.87; P = .03) while PLC injury increased that probability (OR, 12.66; 95% CI, 1.63-100; P = .02). Multivariate logistic regression showed that the proposed MLKI grade was significantly associated with the presence of neurological lesions, with a 2.5-fold increase in the odds of having a neurological injury for each increase in grade (OR, 2.47; 95% CI, 1.36-4.50; P = .003).
Conclusion:
PLC injuries increased the odds of neurological injury in MLKI, while MCL injuries decreased these odds. MLKI grade and presence of PLC injury was associated with the presence of neurological injury. MLKI grade was not associated with the presence of a vascular lesion.
Keywords
Multiligament knee injuries (MLKIs) are usually defined as those with tears in ≥2 of the 4 main ligaments of the knee: anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), lateral collateral ligament (LCL), and medial collateral ligament (MCL).11,16,20,22,23,28,36 MLKIs are not common, with an incidence of 0.01% to 0.2% of all orthopaedic injuries2,19 and with associated neurological injury in 15.9% to 25% of cases,2,12,15,16,18-20,22 vascular injury rate of 5% to 21%,2,5,12,15,18,19 and lower limb amputation rate of 2.55%. 18 Mortality rate in patients suffering an MLKI is 2%, mostly related to other traumatic injuries sustained at the time of MLKI. 2 Even though all knee dislocations (KDs) result in an MLKI, not all MLKIs occur as a result of a KD.11,22,23
A KD is usually defined as a total disruption of the tibiofemoral joint.11-13,20,32 The KD incidence has been reported as 0.072 per 100 patient-years, 1 representing 0.18% of trauma admissions 4 and 22.8% to 37% of patients with an MLKI.2,12,22 When considering only KD, vascular lesions have an incidence of 15% to 64%,4,6,9,12,18,29 and 3.8% to 5.5% of all KDs result in limb amputation.4,6 From the KDs that have an associated vascular injury, 12% to 15% result in limb amputation.4,9,18 Neurological injuries are present in 4% to 38.9% of all KDs.4,6,12,18,22,29 The overall mortality rate after a KD, usually associated with concomitant traumatic injury, is 2.82%. 4
Many studies have considered KDs and MLKIs to be equivalent lesions2,5,14,15,18,19,28 or have not differentiated between MLKI with and without KD.23,24,28 The foundational definition of KD categories was made by the Schenck classification, 25 but it was stated that tibiofemoral joint dislocation does not need to be confirmed for all cases of MLKI to ascribe them as KD. On top of that, the most used MLKI classification 32 (Table 1) applies the term “KD” for each MLKI category, adding more confusion to the limits between KD and MLKI.
Modified Schenck Classification for KD a
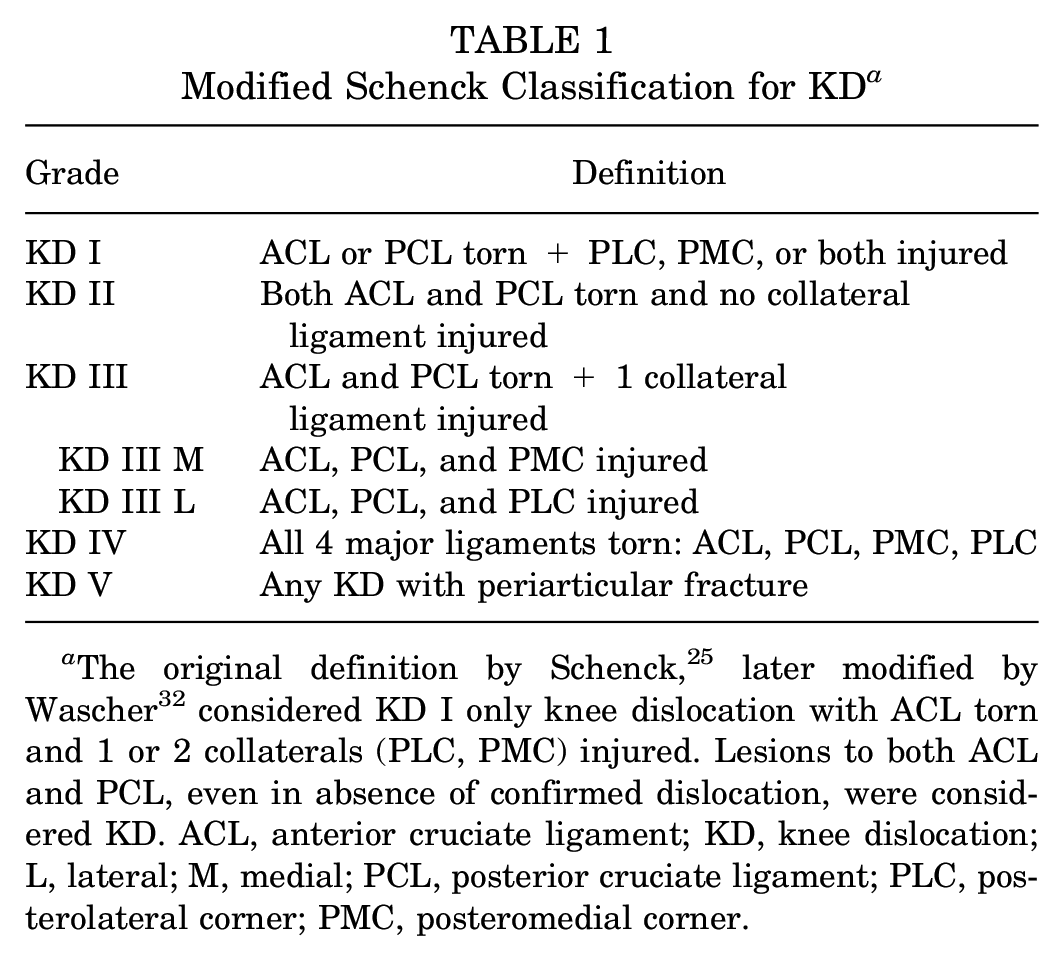
The original definition by Schenck, 25 later modified by Wascher 32 considered KD I only knee dislocation with ACL torn and 1 or 2 collaterals (PLC, PMC) injured. Lesions to both ACL and PCL, even in absence of confirmed dislocation, were considered KD. ACL, anterior cruciate ligament; KD, knee dislocation; L, lateral; M, medial; PCL, posterior cruciate ligament; PLC, posterolateral corner; PMC, posteromedial corner.
Many studies have analyzed how different factors of MLKI can affect the likelihood of vascular and neurological injuries. † Tears to the posterolateral corner (PLC) have shown the strongest association with neurological injury of all the studied factors.8,13,16,19,20,31,36 Additionally, MLKIs with documented KD have higher rates of neurological injury than those without KD.11,12,22 On the other hand, high-energy trauma and documented KD have been found to increase the odds of associated vascular injury.10-12 The subgroup of obese patients with MLKI from an ultra–low energy KD also appears to be at high odds of vascular lesion. 29 Despite the extensive research on factors associated with neurological and vascular injury in MLKI, the association between Schenck KD grade 32 and the risk of neurological and vascular injury has not been so widely investigated. 10 A better understanding of the association between MLKI injury pattern and related neurological and vascular lesions will help prompt and thorough diagnosis of these injuries, as both are determining factors to avoid major complications when treating these lesions.
The purpose of this study was to evaluate whether there is an association between patient characteristics (sex, age), mechanism of injury, lesions to the different ligaments of the knee (ACL, PCL, PLC, and posteromedial corner [PMC]) and MLKI grade with the presence of vascular and neurological injuries. The hypothesis was that ligamentous injury pattern in MLKI is associated with likelihood of vascular and neurological lesions, with an increased odds of neurological and vascular lesion in high MLKI grades.
Methods
An international multicenter study collecting data on multiligament knee injuries was conducted. Participating centers were Toledo University Hospital (Toledo, Spain), Begoña Hospital (Gijón, Spain), Clínica Espregueira (Porto, Portugal), Clínica Alemana (Santiago de Chile, Chile), St Antonius Hospital (Utrecht, the Netherlands), Hospital das Clinicas (São Paulo, Brazil) and Monica Hospitals (Antwerp, Belgium). All patients surgically treated for MLKI from January 2014 to December 2020 were included. MLKIs were considered those lesions with ≥2 of the 4 main ligaments of the knee (ACL, PCL, MCL, and LCL) torn.10,11,16,23,30,32 The study was conducted in conformity with the Helsinki Declaration and approved by the regional ethics committee of the coordinating center; additional institutional review board approval from each of the participating centers was obtained when pertinent.
Inclusion criteria comprised (1) skeletally mature patients, (2) MLKI seen on magnetic resonance imaging (MRI) and confirmed intraoperatively, (3) surgical treatment, and (4) availability of information regarding neurological and vascular lesions. Exclusion criteria were defined as (1) previous lesions of the knee, (2) previous surgery of the knee, (3) previous neurological or vascular lesions of the knee, (4) concomitant periarticular fractures of the knee, and (5) ligamentous injuries treated nonoperatively.
Data Collection
Sex, age, injury mechanism (high-energy trauma, low-energy trauma, or sports lesion), vascular injury, and neurological injury were recorded for all patients from prospectively collected data from their clinical charts. Neurological injuries were defined as partial (Medical Research Council [MRC] grades 1-4) or complete (MRC grade 0) palsies of the common peroneal nerve or the tibial nerve. 35 Vascular injuries were defined as lesions to the popliteal artery that caused disruption, complete occlusion, or partial occlusion that compromises limb viability. Angiography was indicated based on clinical findings and according to each center’s protocol.
Data on knee injury were gathered from MRI reports and later confirmed by surgical records. Final diagnosis was stated in the operation room by the treating surgeon, based on exploration under anesthesia and operative findings.3,11 Lesions to the ACL, PCL, MCL, LCL, popliteal tendon, iliotibial band, biceps tendon, menisci, and cartilage were recorded from MRI reports and confirmed using surgical records. All information was gathered on standardized spreadsheets. A torn ligament was defined as one with a complete lesion or lesion of >50% on the MRI and/or incompetence (grade III-IV laxity) with examination under anesthesia. The MRI findings and final diagnosis stated by the surgeon in the operating room were used to define a torn knee ligament. Intraoperative stress radiographs, exploration under anesthesia, and intraoperative findings were used with discretion as needed. 3 Each participating center fulfilled the spreadsheet with their patients’ data and sent it to the coordinating center for analysis. The 2 main researchers (E.S.M., B.L.H.) reviewed the information from all centers, excluded the patients that did not fulfill inclusion criteria, and pooled all the data into a single spreadsheet. Using surgical data, the KD grade according to the modified Schenck classification (Table 1)7,19,23 was assigned to each patient by an experienced orthopaedic surgeon (E.S.M.).
For statistical and analytical purposes, a new MLKI classification was developed. Each grade was defined by the ligamentous injury pattern. MLKI grade variable was considered an ordinal variable, with greater grade as more ligaments were torn, except for MLKI affecting 3 ligaments. Lesions to the ACL, PCL, and 1 collateral were coded into 2 separate categories: MLKI III for ACL, PCL, and MCL torn and MLKI IV for ACL, PCL, and LCL torn, with MLKI IV considered a more severe injury than MLKI III. When a KD was confirmed, the suffix “d” was added (Table 2). An MLKI grade of this new classification was assigned to each patient by an experienced surgeon (E.S.M.).
Classification for MLKI a
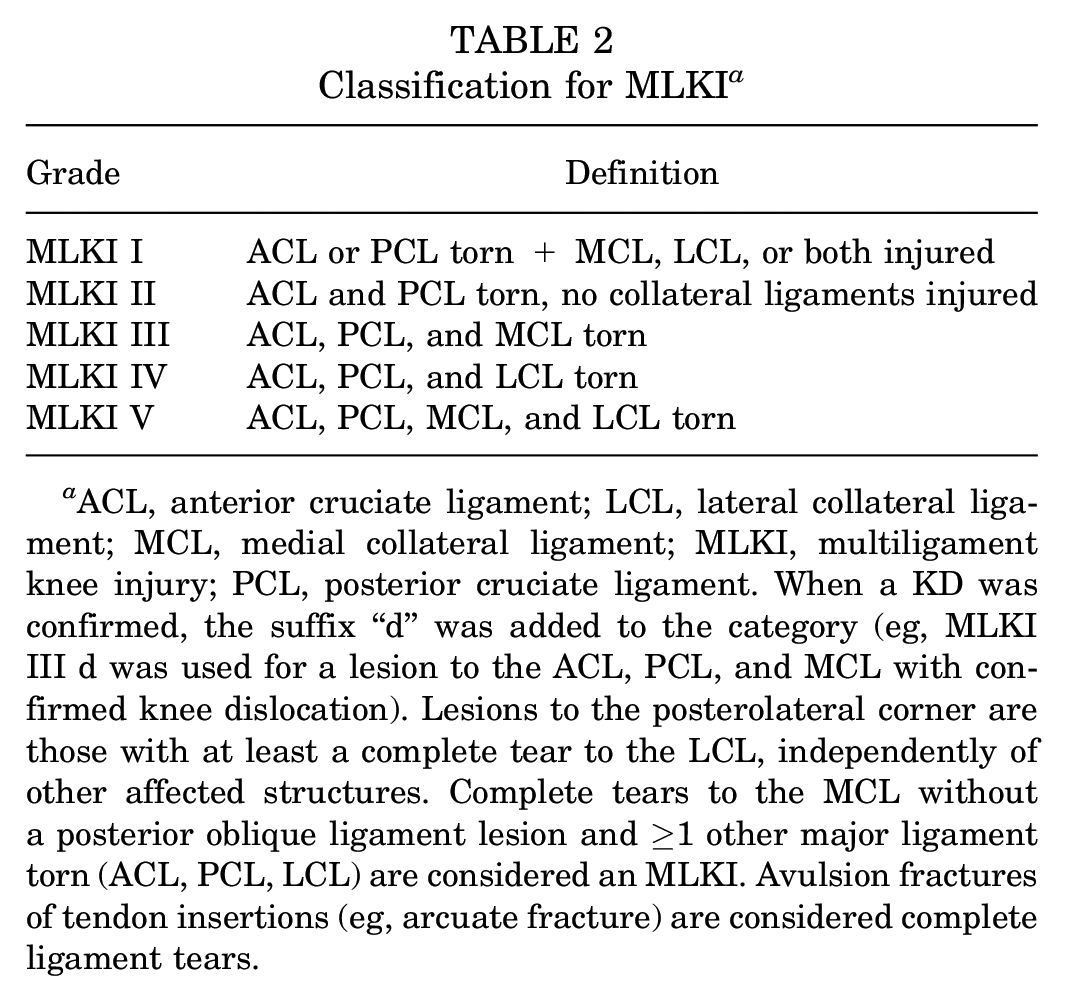
ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; MLKI, multiligament knee injury; PCL, posterior cruciate ligament. When a KD was confirmed, the suffix “d” was added to the category (eg, MLKI III d was used for a lesion to the ACL, PCL, and MCL with confirmed knee dislocation). Lesions to the posterolateral corner are those with at least a complete tear to the LCL, independently of other affected structures. Complete tears to the MCL without a posterior oblique ligament lesion and ≥1 other major ligament torn (ACL, PCL, LCL) are considered an MLKI. Avulsion fractures of tendon insertions (eg, arcuate fracture) are considered complete ligament tears.
Statistical Analysis
An independent statistician who was not involved in either the study design or the data collection carried out the statistical analysis. Descriptive data were reported either as means with standard deviations for continuous variables or as frequencies with percentages for categorical data.
Preliminary analyses were performed to determine if any factor was related to the dependent variable “vascular injury.” Analyzed factors were age, sex, mechanism of injury, torn ligaments, and MLKI grade. As statistical estimators, the Student t test was used for continuous variables with 2 groups, the analysis of variance (ANOVA) for continuous variables with >2 groups, and the chi-square test for categorical variables. For the factor “MLKI grade,” analyses were performed considering it both an ordinal variable and a continuous variable.
Preliminary analyses were also carried out to determine which factors would be associated with the dependent variable “neurological injury.” The Student t test, ANOVA, and chi-square test were again used as statistical estimators. Univariate regression was conducted for each factor that showed statistical significance in the preliminary analyses. Multivariate regression was then performed for all the variables that showed statistical significance in the univariate analysis.
The results from the regression were presented as odds ratios (ORs) with 95% CIs. The statistical software used were the STATA SE Version 14.0 (Stata Corp) and the SPSS software Version 21 (IBM Corp).
Results
Descriptive Data
After excluding patients not meeting the inclusion criteria or with incomplete data, 144 patients were included (Figure 1). The mean age was 33.9 ± 11.9 years (range, 15-64 years), and there were 104 male (72.2%) and 40 female (27.8%) patients. High-energy trauma was the most common mechanism of injury (n = 80; 55.6%), followed by sports trauma (n = 48; 33.3%) and low-energy trauma (n = 14; 9.7%). Vascular injury was present in 5 patients (3.5%) and nerve injury in 17 patients (11.8%). One patient (0.7%) had both neurological and vascular injury.
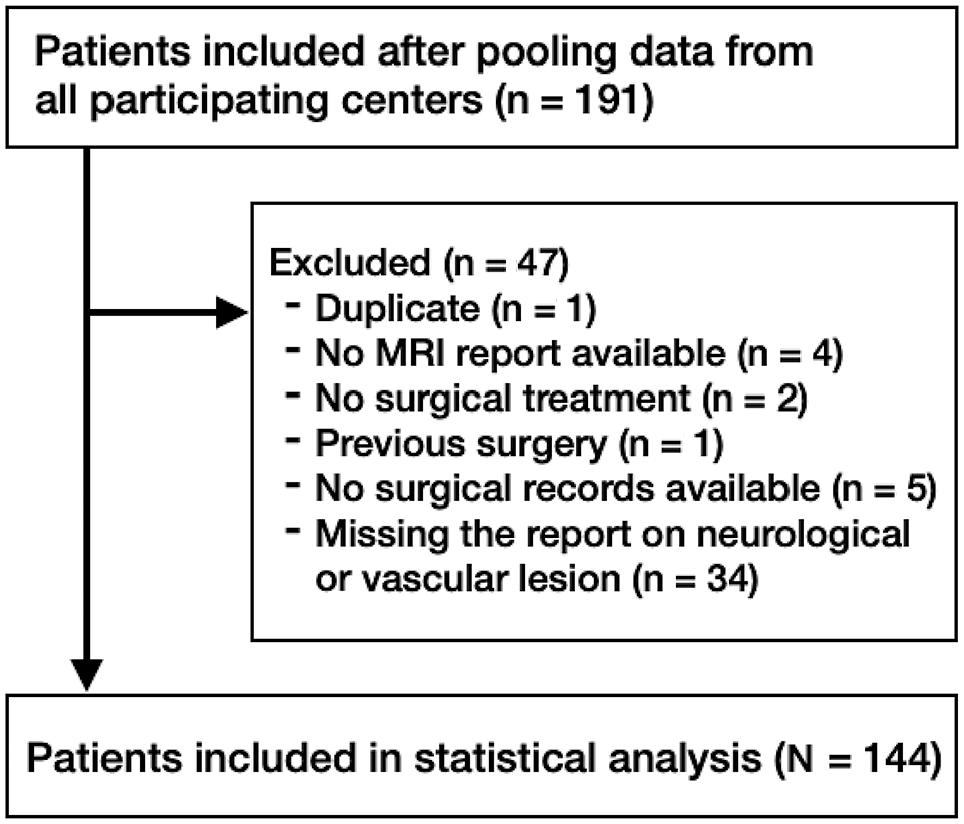
Flow diagram of patient enrollment. MRI, magnetic resonance imaging.
Using the surgical data available, patients were classified according to the proposed MLKI classification: 50 (34.7%) showed an MLKI I lesion, 7 (4.9%) MLKI II, 28 (19.4%) MLKI III, 36 (25.0%) MLKI IV, and 22 (15.3%) MLKI V. Incomplete data on surgical records prevented the assignment of MLKI grade in 1 patient (0.7%).
Vascular Lesions
Five patients (3.5%) presented with vascular lesion: 4 (80%) men and 1 (20%) woman. None of the analyzed factors were associated with the presence of vascular injury: patient sex (P = .69), age (P = .31), injury mechanism (P = .13), or injury to the ACL (P = .47), PCL (P = .17), MCL (P = .48), or PLC (P = .55). Additionally, no association was found between vascular injury and MLKI grade, either if MLKI grade was considered an independent variable (P = .23) or analyzed with ANOVA (P = .32).
Neurological Injury
Neurological injuries were present in 17 patients (11.8%): 13 men (76.5%) and 4 women (23.5%). Neither age (P = .63) nor sex (P = .68) was associated with the presence of neurological injury. MLKI grade was associated with the presence of neurological injury, when analyzed using ANOVA (OR, 0.12; 95% CI, 0.07-0.17; P < .001) and when analyzed as an ordinal variable (P < .001). Mechanism of injury was not associated with neurological injury (P = .94), nor was presence of ACL injury (P = .17). In contrast, the presence of PCL injury (P = .04) and PLC injury (P = .003) was significantly associated with the presence of neurological injury. A torn MCL (P = .02) was associated with the absence of neurological injury: incidence of neurological lesions was 18.8% in patients without MCL lesion and 6.3% in patients with MCL lesion, with this difference reaching statistical significance (P = .02).
Univariate logistic regression analysis showed that MLKI grade was positively associated with the presence of neurological injury, with the odds of having a neurological injury increasing by 2.5-fold with each increase in MLKI grade (OR, 2.08; 95% CI, 1.31-3.29; P = .002) (Table 3). The presence of PCL lesions was not a significant factor for neurological injury (OR, 6.67 [95% CI, 0.84-50]; P = .07). MCL lesions decreased the odds of associated neurological injury (OR, 0.29; 95% CI, 0.1-0.87; P = .03) while presence of PLC injury increased the likelihood of neurological injury (OR, 12.66; 95% CI, 1.63-100; P = .02) (Table 3).
Univariate Logistic Regression for Association Between Analyzed Factors and Neurological Injuries a

MCL, medial collateral ligament; MLKI, multiligament knee injury; OR, odds ratio; PCL, posterior cruciate ligament; PLC, posterolateral corner.
Multivariate logistic regression analysis showed that MLKI grade was associated with the presence of neurological injury. There was a 2.5-fold increase in the odds of having a neurological injury for each increase in MLKI grade, if considered an ordinal variable (OR, 2.47; 95% CI, 1.36-4.50; P = .003). In contrast, presence of MCL lesions decreased the odds of neurological injury (OR, 0.19; 95% CI, 0.05-0.65; P = .008) (Table 4).
Multivariate Logistic Regression for Association Between Analyzed Factors and Neurological Injuries a

MCL, medial collateral ligament; MLKI, multiligament knee injury; OR, odds ratio.
Discussion
In the analyzed cohort of 144 patients with MLKIs, frequency of vascular injury was 3.5% and frequency of neurological injury was 11.8%. The main finding of the present study was that, when using the proposed newly modified MLKI classification (Table 2), the MLKI grade was significantly associated with the likelihood of neurological injury, with the odds of neurological lesion increasing 2.5-fold for each increase in MLKI grade. Another significant finding was that tears to the MCL decrease the odds of neurological injury, while PLC lesions increase the odds of associated neurological injuries.
None of the analyzed factors showed a significant association with the presence of vascular injury. The low incidence of vascular lesions in the studied population (3.5%) might have been a potential reason for not finding any statistical significance. Although the lack of significance is not likely the result of a low of statistical power, studies with larger sample sizes may find a correlation between vascular injury and some of the analyzed variables; however, it that correlation were found, it will likely be of little clinical relevance. Our results suggest that vascular injury is not associated with any specific MLKI injury pattern; therefore, systematic and careful vascular examination to rule out vascular injury is of paramount importance in all patients sustaining MLKI.
A recent retrospective study 23 reported that 38.4% of MLKIs affected medial-side knee structures, but >94% of nerve lesions were found in MLKIs with PLC lesions. Other studies had also found an association between PLC lesions and neurological injuries2,13,19,20 and described how lesions to the PLC display a major increase in the odds of neurological injury. Vasavada et al 31 analyzed a series of 16 complete peroneal nerve palsies associated with MLKI and found that all those patients presented PLC tears. Moran et al 20 also found that the bone bruise pattern produced by varus stress forces, which typically results in PLC injury, was significantly associated with common peroneal nerve lesions. These findings are in line with those of our study and emphasize that patients with MLKI involving the PLC are at a higher risk of associated neurological injury, underpinning why these lesions must be actively ruled out. Some studies8,16 also suggested that MLKI involving PLC injury poses a risk factor for neurological injury, especially when associated with ACL injury.
In the present study, lesions to the MCL decreased the odds of neurological injury. This finding could easily be explained by the mechanism of injury, where lesions to the PMC are associated with valgus forces applied to the knee, with some extent of rotatory and translational forces. 3 In contrast, lesions to the PLC are associated with hyperextension–varus stress forces and rotation, which are the mechanism of injury to the common peroneal nerve.8,16,20 The underlying mechanism of injury for PMC tears is thus characterized by a valgus force to the knee, in contraposition to the varus force that produces common peroneal nerve injury. This injury mechanism was highlighted in a study by Essilfie, 8 in which patients with MLKI and a torn MCL were less likely to have the concomitant PLC injury pattern that is associated with common peroneal nerve injury.
In our study, ACL lesions were not associated with the presence of neurological lesions. Contrarily, PCL tears were associated with neurological lesions, but only in the preliminary analyses and not in the univariate or multivariate logistic regression. The fact that statistical significance was not reached in the univariate logistic regression, in contrast with previous preliminary analysis, may be due to insufficient statistical power (due to small sample size) and suggests that the presence of PCL lesion is not such a relevant factor for neurological injury as MLKI grade or lesions to the PLC. These findings contrast with other studies, in which common peroneal nerve injuries were associated with ACL tear8,16 and in which lesions to the PCL were rather unusual and always in association with ACL tears. 8
MLKIs are usually associated with major trauma2,6,16,22,23,27 and other medical conditions that could prevent adequate patient collaboration for diagnosis of lesions to the common peroneal nerve.2,9,16 Also, delayed or misdiagnosed nerve injury is associated with worse clinical outcomes, as preoperative diagnosis of these lesions is of paramount importance for its timely and adequate treatment.3,16 Being aware of the risk factors for neurological injuries associated with MLKI will thus help to actively rule out these lesions in high-risk patients, mitigating its delayed treatment, that could compromise the final clinical outcome.
In 1994, Schenck, 25 in a seminal article, proposed a 4-category classification for KDs based on ligamentous injury pattern, considering KDs to be those presenting with (1) loss of tibiofemoral articulation or (2) tear to both cruciate ligaments (ACL and PCL) even in the absence of confirmed articular dislocation. Later on, Wascher 32 added a fifth category including KDs with associated major periarticular fractures, using the same criteria for KDs.32,33 Ever since, the classification proposed by Wascher 32 has been widely accepted and used to characterize both MLKIs and KDs.3,7,10-12,14,19,20 But not all authors apply this classification in the same way. While some of them consider MLKIs and KDs to be equivalent injuries,2,5,14,15,18,19,28 others clearly distinguish between MLKI with and without confirmed KD.4,11,12,22,23 Moreover, the definition itself of both MLKI and KD varies among studies.2,4-6,14,15,18-20,28 The poor definition and interchangeable use of both terms leads to heterogeneity in the literature concerning MLKI, clearly reflected by the broad range of associated vascular (1.2%-26%) and neurological (6.2%-28%) injuries reported, ‡ as not all studies include the same spectrum of lesions 4 when considering MLKI,16,20 KD,4,6,11,18 or both.12,15,18,22,23,28 Some authors 23 have proposed an alternative classification for MLKIs, while others7,11 have suggested the use of specific suffixes to indicate the presence of KD in MLKIs and highlighted the need for a comprehensive new classification. Indeed, Wascher et al 34 have recently emphasized that their modified classification remains a simple and useful system for research purposes, surgical planning, and prognosis on complex knee lesions but that the classification is valid only for KDs as originally defined by Schenck in 1994. 25
In the present study, knees with complete tears (including ligament avulsions) 25 of ≥2 of the 4 main ligaments (ACL, PCL, MCL, and LCL) were considered MLKIs.11,15,16,20,22-24,28 If the MCL was torn, regardless whether the posterior oblique ligament was intact or torn, it was considered a medial-side injury and classified as MLKI III when medial-side injury was concomitant with ACL and PCL lesion. If the LCL was torn, regardless whether the other structures of the PLC (popliteal tendon and popliteofibular ligament) were torn or not, it was considered a lateral-side injury, and classified as MLKI IV if concomitant with ACL and PCL lesion. 24 Even though some authors2,20 do not consider combined complete tears of the MCL and ACL an MLKI, we believe that even in the absence of a lesion to the PMC, these lesions should be considered an MLKI,11,15,16,22-24,28,36 and thus we classified these as MLKI I. Diagnosis of the ligamentous tears was recorded as reported on MRI, as previous studies found that MRI have fair sensitivity for most ligaments in MLKI 24 and was later confirmed by exploration under anesthesia and operative findings.3,20,23 Considering the aforementioned criteria, we developed and used for the present study a classification intended for all MLKIs (Table 2) and found that, by using this classification, there was an association between MLKI grade and the likelihood of neurological injury, with a 2.5-fold increase of the odds of neurological injury for each increase in MLKI grade. Previous studies that found an association between Schenck KD grade and functional outcomes, 14 along with MRI diagnostic accuracy (when considering KD III Medial-side injuries and KD III Lateral-side injuries to be 2 different ordinal categories), 24 also supports the applicability of the proposed classification, as it has implications for risk of associated lesions, diagnostic accuracy, and clinical outcomes.
Adding the suffix “d” when the MLKI has been preceded by a documented KD (Table 2) will be useful to distinguish this subset of lesions.11,12 To define a KD, we have chosen the most accepted and used criteria: (1) imaging studies with total disruption of the tibiofemoral articulation 11 or (2) documented knee deformity of the tibiofemoral articulation that required manual reduction.12,13,20,32 Current literature supports that KD increases the risk of associated vascular and neurological lesions,4,9,11,12,20,22,31 has important implications for the prognosis and is associated with worst expected outcomes.4,27 Thus, given the increased risk of other lesions and prognosis implications in the subset of MLKIs with KD, clearly defining and identifying this condition in our proposed classification appears to us of paramount importance.
Limitations
There are certain limitations to the present study. First, even though the used data were prospectively collected, the retrospective design of the study implies some limitations. Lack of complete data for some patients prevented their inclusion in the final analysis. Also, even though representative of MLKI, our series has a selection bias, as it only included surgically treated lesions: patients with MLKI that required amputation, led to death, or were not suitable for surgery were not included in our study. MLKI commonly affect patients with associated polytrauma, major trauma injuries, or other concomitant medical conditions; however, information about these conditions was not collected neither included in the final analysis, potentially acting as confounding variables. Another limitation was that we did not analyze whether the presence of dislocation was a risk factor for the presence of concomitant injury. In contrast, the multicenter design and the large number of patients (across different continents) included in our series allows for a sound generalization of the results, as they could be extrapolated to similar scenarios. Moreover, MRI and surgical assessment of injured structures were made by blind assessors that mitigated the risk of detection bias.
Due to the complexity and heterogeneity of MLKIs and the broad range of associated factors that can influence its treatment and prognosis, further prospective multicenter studies will help elucidate validity of the proposed classification and any additional factors that could improve it. Certainly, these studies will benefit from the use of conventional statistical analysis, machine learning, and artificial intelligence–generated models. 31
Conclusion
In the current study, a new classification was developed to analyze the risk of neurological and vascular lesions in MLKI. The proposed classification was associated with the presence of neurological injury, with a 2.5-fold increase in the odds of having a neurological lesion for each grade increase on the new classification. MCL tears reduced the odds of neurological injury, and PLC tears increased the odds of neurological injury. None of the analyzed factors was significantly associated with the presence of vascular injuries.
Authors
Enrique Sanchez-Munoz, MD (Lower Limb Unit, Department of Traumatology and Orthopaedic Surgery, Infanta Elena University Hospital, Madrid, Spain; Centro Clínico Quirúrgico, Madrid, Spain); Beatriz Lozano Hernanz, MD (Knee Unit, Department of Traumatology and Orthopaedic Surgery, Toledo University Hospital. Toledo, Spain); Renato Andrade, BSc (Clínica Espregueira–FIFA Medical Centre of Excellence, Porto, Portugal; Dom Henrique Research Centre, Porto, Portugal; Porto Biomechanics Laboratory, Faculty of Sports, University of Porto, Porto, Portugal); Cristina Valente, PhD (Clínica Espregueira–FIFA Medical Centre of Excellence, Porto, Portugal; Dom Henrique Research Centre, Porto, Portugal); João Espregueira-Mendes, MD, PhD (Clínica Espregueira–FIFA Medical Centre of Excellence, Porto, Portugal; Dom Henrique Research Centre, Porto, Portugal; Porto Biomechanics Laboratory, Faculty of Sports, University of Porto, Porto, Portugal; School of Medicine, University of Minho, Braga, Portugal; ICVS/3B’s–PT Government Associate Laboratory, Braga/Guimarães, Portugal); Francisco Figueroa, MD (Clínica Alemana–Universidad del Desarrollo, Santiago, Chile; Hospital Sotero del Rio, Santiago, Chile); David Figueroa, MD (Clínica Alemana–Universidad del Desarrollo, Santiago, Chile); Kristien Vuylsteke, PhD (MORE Foundation, Antwerp, Belgium); Peter C.M. Verdonk, MD, PhD, Prof. (MORE Foundation, Antwerp, Belgium; Antwerp Orthopaedic Centre–Monica Hospitals, Antwerp, Belgium); Luís Eduardo Passarelli Tirico, MD (Orthopedic and Traumatology Institute, Hospital das Clinicas, University of São Paulo Medical School, São Paulo, Brazil); Fabio Janson Angelini, MD (Orthopedic and Traumatology Institute, Hospital das Clinicas, University of São Paulo Medical School, São Paulo, Brazil); and Jacco A.C. Zijl, MD (Department of Orthopaedic Surgery. St Antonius Hospital, Utrecht, the Netherlands); Nienke Wolterbeek, PhD (Department of Orthopaedic Surgery, St Antonius Hospital, Utrecht, the Netherlands); and Antonio Maestro Fernández, MD, PhD (School of Medicine, University of Oviedo, Oviedo, Spain; Begoña Hospital, Gijón, Spain).
Footnotes
Final revision submitted August 18, 2024; accepted August 30, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Complejo Hospitalario de Toledo (reference No. 460).