
Abstract
Background:
Femoral and tibial tunnel malposition for anterior cruciate ligament (ACL) reconstruction (ACLR) is correlated with higher failure rate. Regardless of the surgical technique used to create ACL tunnels, significant mismatches between the native and reconstructed footprints exist.
Purpose:
To compare the position of tunnels created by a standard technique with the ones created based on preoperative 3-dimensional magnetic resonance imaging (3D MRI) measurements of the ACL anatomic footprint.
Study Design:
Controlled laboratory study.
Methods:
Using 3D MRI, the native ACL footprints were identified. Tunnels were created on 16 knees (8 cadavers) arthroscopically. On one knee of a matched pair, the tunnels were created based on 3D MRI measurements that were provided to the surgeon (roadmapped technique), while on the contralateral knee, the tunnels were created based on a standard anatomic ACLR technique. The technique was randomly assigned per set of knees. Postoperatively, the positions of the tunnels were measured using 3D MRI.
Results:
On the tibial side, the median distance between the center of the native and reconstructed ACL footprints in relation to the root of the anterior horn of the lateral meniscus medially was 1.7 ± 2.2 mm and 1.9 ± 2.8 mm for the standard and roadmapped techniques, respectively (P = .442), while the median anteroposterior distance was 3.4 ± 2.4 mm and 2.5 ± 2.5 mm for the standard and roadmapped techniques, respectively (P = .161). On the femoral side, the median distance in relation to the apex of the deep cartilage (ADC) distally was 0.9 ± 2.8 mm and 1.3 ± 2.1 mm for the standard and roadmapped techniques, respectively (P = .195), while the median distance anteriorly from the ADC was 1.2 ± 1.3 mm and 4.6 ± 4.5 mm for the standard and roadmapped techniques, respectively (P = .007).
Conclusion:
Providing precise radiological measurements of the ACL footprints does not improve the surgeon’s ability to position the tunnels. Future studies should continue to attempt to provide tools to improve the tunnel position in ACLR.
Clinical Relevance:
This cadaveric study indicates that despite the use of 3D MRI in understanding the ACL anatomy, re-creating the native ACL footprints remains a challenge.
Keywords
Anterior cruciate ligament (ACL) reconstruction (ACLR) is a commonly performed surgical procedure. 10 In the past few decades, significant advancements in ACLR techniques were made, aiming to improve their clinical outcomes and lower their failure rates. 3,4,7,19,36 Among technical factors, imprecise position of the graft tunnels, particularly the femoral tunnel, is known to contribute to ACLR failure. 5,15,21 Therefore, in recent years, there has been an increased interest in understanding the precise anatomy of the ACL and its tibial and femoral footprints. Re-creating the patient’s own anatomy through anatomic ACLR has been shown to improve postoperative outcomes by restoring native knee kinematics and stability, as well as lowering the risk of subsequent knee osteoarthritis. 5,15,22,28,29,34,35
Identifying the correct position of the femoral footprint during arthroscopic ACLR remains a challenge for the surgeon. 18,21 To help guide tunnel placement, surgeons use a combination of anatomic landmarks and tunnel drilling guides during surgery. 1,8,9,13,16,25,26 Moreover, various techniques for the creation of the femoral tunnel presently exist, including the endoscopic transtibial technique, anteromedial (AM) portal technique, outside-in technique, and outside-in retrograde drilling technique. 3,5,7,19 The transtibial technique has fallen out of favor since it was found that drilling for the femoral tunnel using this technique leads to a more vertical tunnel with vertical ACL graft orientation, especially if the tibial tunnel was started more distal and lateral, making it impossible to get to the proper location on the lateral wall of the notch and thus placing the tunnel high in the notch, which results in suboptimal rotational stability and clinical outcomes. 5,18,23 Other procedures such as the medial portal drilling or outside-in techniques, on the other hand, seem to create a more accurate femoral tunnel placement. 2,5
Owing to variations in the anatomy of the ACL footprints among patients, creating anatomic ACL tunnels is challenging despite the various techniques and tools available to surgeons. 6,11,14,17,20,30 In previous studies using 3-dimensional magnetic resonance imaging (3D MRI), 6,11,14,20,30 significant mismatch between the native footprint and the reconstructed ones has been reported. The aim of this study was to compare the position of the tunnels created by a standard technique with the ones that are created using preoperatively assessed 3D MRI measurements of the anatomic footprint of the ACL (roadmapped technique).
Methods
Study Protocol
This study received the ethics approval of an institutional review board. Eight matched pairs of frozen cadaveric knees (16 knees) were used for the experiment. The cadavers were obtained from the department of anatomy of McGill University for the purpose of research. Four (50.0%) were male specimens, and the mean age was 76.2 ± 12.6 years (range, 62-98 years).
The original ACL footprints of each knee were identified and measured using 3D MRI before performing any procedure on the cadavers. With a 1.5-T TwinSpeed Excite high-definition MRI scanner (GE Medical Systems), the 3D MRI was performed using the same technique described by Han et al. 12 An 8-channel high-definition surface coil was applied to the knees that were positioned in near full extension. An oblique-coronal proton density sequence along the plane of the ACL was acquired, with slice gaps of 0.6 mm for 3D reconstruction. The 3D reconstruction allows for visualization of the ACL along its course, in addition to displaying the footprints and their centers “en face.” Using a PACS (picture archiving and communication system) workstation with embedded multiplanar software (InteleViewer; Intelerad Medical Systems), multiplanar reconstructions and footprint measurements were performed (Figures 1 and 2).

Multiplanar reconstruction of 3-dimensional magnetic resonance imaging to visualize the anterior cruciate ligament’s femoral footprint on the lateral femoral condyle.

Multiplanar reconstruction of 3-dimensional magnetic resonance imaging to visualize the anterior cruciate ligament’s tibial footprint on the tibial plateau.
On the femoral side, the 3D sequence was reformatted in pure axial and sagittal planes relative to the knee joint using the coronal and sagittal sequences from examination. On the axial plane, the AM and posterolateral (PL) bundles of the ACL were identified and followed to their insertion points on the femur. The footprint of the ACL was noted and marked using the axial and sagittal sequences. Once the footprint was established, the axial sequences were utilized to find the change in angle between the AM and PL bundle facets. Once the change in angle was noted, a mark was placed at the intersection of the intercondylar and bifurcate ridges. Then, the apex of the deep cartilage (ADC) was marked, and the pure anterior and distal distances between the center of the femoral footprint and the ADC were measured (Figure 3A).
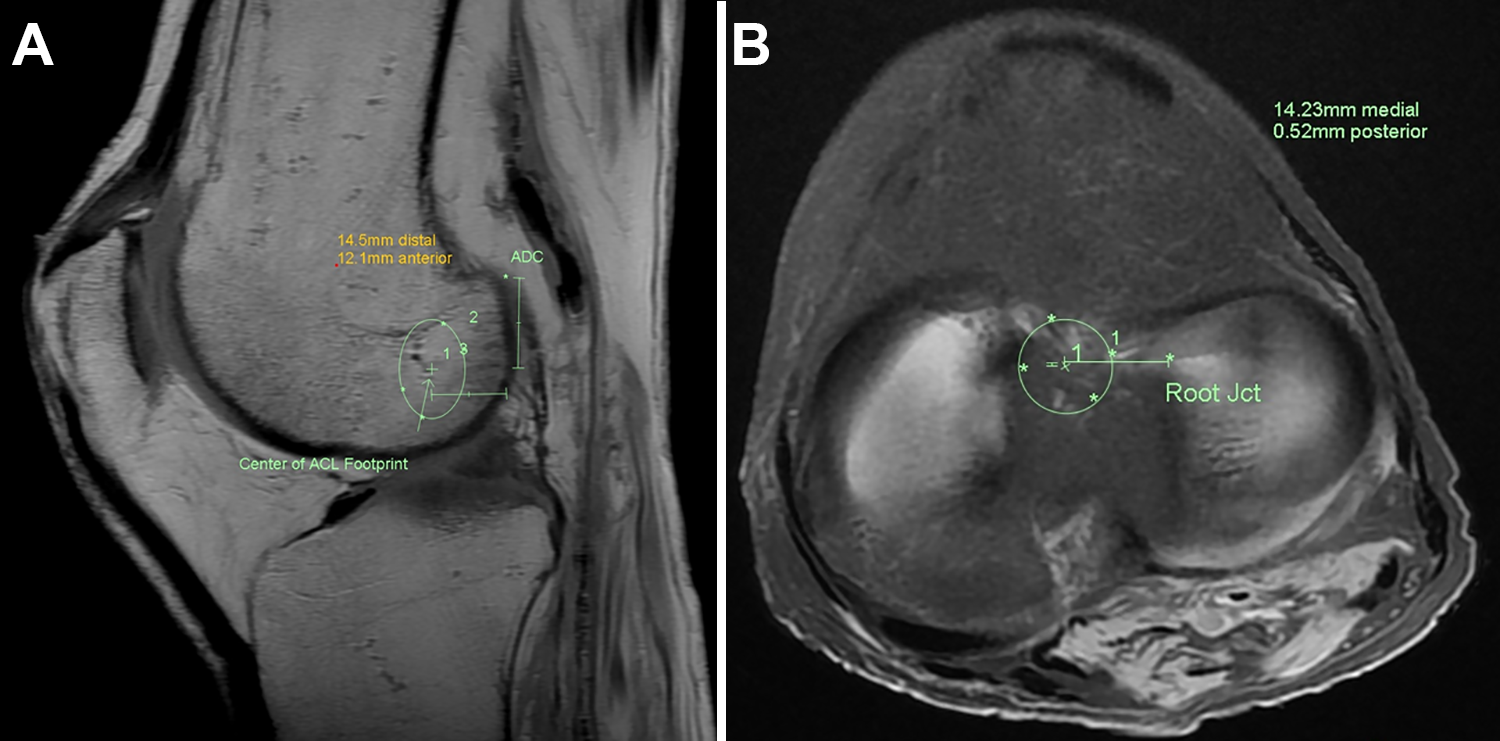
Three-dimensional magnetic resonance imaging demonstrating measurements of the center of the (A) femoral and (B) tibial anatomic footprints of the anterior cruciate ligament (ACL) in relation to the apex of the deep cartilage (ADC) on the femoral side and root junction (Jct) of the anterior horn of the lateral meniscus on the tibial side. On the femoral side, lines 1 and 2 are distances (in millimeters) from the ADC to the center of the footprint. The 2 lines are at 90° to each other and follow the distal femoral diaphysis. On the tibial side, the line represents the distance between the Jct and the center of the footprint.
On the tibial side, 3D sequence reformatting and both the AM and PL bundles of the ACL were also followed to find the tibial footprint using sequences similar to what were used to identify the femoral footprint. Once the tibial footprint was found and outlined, the center of the footprint was marked. The center was marked with a circular region of interest tool that incorporated, to the best possible fit, the outlined footprint (footprint is not circular, and hence, there might be a minor degree of error). A pure medial and anterior or posterior distance was measured from the root of the anterior horn of the lateral meniscus (AHLM) to the center of the tibial footprint (Figure 3B).
We compared ACL graft tunnel positions created by a standard ACLR technique versus tunnels created based on the measurements obtained by 3D MRI (roadmapped technique). On the 8 cadavers, 4 right knees and 4 left knees were randomly assigned to the standard ACLR group, and the contralateral knees were assigned to the roadmapped technique. After drilling the tunnels, all knees once again underwent 3D MRI to determine the position of the tunnels in comparison with the native ACL footprint. The difference in the distance from the center of the anatomic footprint to the center of the created tunnel was measured according to specific anatomic landmarks.
Surgical Technique
All procedures were done arthroscopically by a single orthopaedic fellowship–trained surgeon (J.B.). For the standard ACLR group, the ACL was completely resected via the AM and anterolateral portals. The ADC, lateral intercondylar ridge, and the bifurcate ridge were identified to help determine the position of the femoral tunnel. The center of the footprint was marked using a microfracture awl (Smith & Nephew). A standard offset 7-mm ACL femoral drill guide (Smith & Nephew) was passed through the AM portal to the marked footprint, and the knee was then flexed to 120°. A guide wire was then placed in the lateral femoral condyle, and a cannulated 8-mm femoral rigid drill bit was then passed through the guide wire to create the femoral tunnel. On the tibial side, the root of the AHLM and the center of the tibial footprint of the ACL were identified by the surgeon. A guide wire (Acufex Director set at 50°; Smith & Nephew) was passed through the proximal tibia to the ACL tibial footprint, and the tibial tunnel was created using a cannulated 8-mm rigid drill bit.
For the roadmapped technique, the surgeon was given the 3D MRI measurements of the native ACL footprint to help position the graft tunnels. After arthroscopic exposure and ACL resection, the anteroposterior depth and craniocaudal position of the ACL femoral footprint were determined using a depth gauge (TRUKOR Depth Gauge; Smith & Nephew) and ruler based on the same anatomic landmarks used in the 3D MRI. The measured tunnel position was marked using a microfracture awl. The knee was then flexed to approximately 100°, and a flexible guide wire (CLANCY Flexible Drill Guide System; Smith & Nephew) was inserted in the center of the footprint at the lateral femoral condyle through the AM portal. The flexible guide wire was used because it has a freehand aimer that can be positioned anywhere without specific referencing to ease the localization of the drilling site. A flexible 8-mm drill bit was then passed through the same tunnel on the guide wire, and the femoral tunnel was created. The tibial tunnel location was determined using the depth gauge and ruler based on the 3D MRI measurements in relation to the root of the AHLM. The same tools used for the standard ACLR were used to create the tibial tunnel for the roadmapped technique; this was, however, based on the 3D MRI measurements of the anatomic footprint.
Statistical Analysis
A priori sample size calculation was performed for matched-pair mean comparison analysis aiming for a power above 80%, P < .05, and a clinical effect size of 1.5 mm, leading to the selection of 16 samples (8 matched pairs).
Data were analyzed using the IBM SPSS Statistics 23.0 software (SPSS Inc). The paired-samples t test was used to assess the association between qualitative and normally distributed quantitative variables (ie, center of ACL pre- and postdrilling), while the Mann-Whitney U test was used to assess the association between qualitative and not normally distributed quantitative variables (ie, comparing the difference in the median distances between the anatomic footprints and tunnels created between the 2 groups). A P value of <.05 was considered the cutoff level of statistical significance.
Results
Table 1 demonstrates the location of the native ACL anatomic footprint and the position of the tunnels created using the standard and roadmapped techniques. On the tibial side, the mean distances from the root of the AHLM medially to the center of the ACL footprint and the center of the created tunnel were 13.7 and 12.9 mm, respectively, for the standard technique, while the same distances for the roadmapped technique were 12.5 and 14.7 mm, respectively. On the other hand, the mean anteroposterior distances of the ACL footprints and the center of the created tunnels in relation to the root of the AHLM for the standard technique were 0.6 and –1.1 mm, respectively, while the distances for the roadmapped technique were 2.2 and 0.7 mm, respectively. On the femoral side, the mean distances between the center of the anatomic ACL footprint and the tunnels created using the standard technique in relation to the ADC distally were 10.8 and 10.0 mm, respectively, while the distances for the roadmapped technique were 11.0 and 11.7 mm, respectively. The mean distances in the anterior direction in relation to the ADC for the center of the anatomic ACL footprint and the tunnels created using the standard technique were 9.1 and 9.7 mm, respectively, while the distances for the roadmapped technique were 9.6 and 12.9 mm, respectively. The only significant difference was seen in the roadmapped technique in the distance from the root of the AHLM medially pre- and postdrilling (P = .012).
Location of the ACL Anatomic Footprints and the Tunnels Created in Relation to Specific Anatomic Landmarks on 3D MRI a

a Data are reported as mean ± SD. 3D MRI, 3-dimensional magnetic resonance imaging; ACL, anterior cruciate ligament; ADC, apex of the deep cartilage; AHLM, anterior horn of the lateral meniscus.
b Paired-samples t test.
c Statistically significant difference between the native anatomic footprint and the tunnel (P < .05).
d Negative value indicates posterior position and positive values indicate anterior position.
Table 2 demonstrates the difference between the center of the ACL anatomic footprint and the center of the tunnels created using the standard and roadmapped techniques. On the tibial side, the median distance between the center of the native and reconstructed ACL footprints in relation to the root of the AHLM medially was 1.7 and 1.9 mm for the standard and roadmapped techniques, respectively, while the median distance anteriorly/posteriorly was 3.4 and 2.5 mm, respectively. On the femoral side, the median distance in relation to the ADC distally was 0.9 and 1.3 mm for the standard and roadmapped techniques, respectively, while the median distance anteriorly was 1.2 and 4.6 mm, respectively. Only this last measurement was statistically significantly different between the 2 techniques (P = .007).
Distance Between the Center of the ACL Anatomic Footprint and the Center of the Tunnels in Relation to Specific Anatomic Landmarks on 3D MRI a

a Data are reported as medial (IQR). 3D MRI, 3-dimensional magnetic resonance imaging; ACL, anterior cruciate ligament; ADC, apex of the deep cartilage; AHLM, anterior horn of the lateral meniscus; IQR, interquartile range.
b Mann-Whitney U test.
c Statistically significant difference between techniques (P < .05).
Table 3 and Figure 4 demonstrate the position and distance between the centers of the native and the reconstructed ACL footprints created by the 2 different techniques for each of the included cadavers. On the tibial side, the smallest and largest error distances seen with the standard technique were 0.3 and 8.3 mm, respectively, while the smallest and largest error distances for the roadmapped technique were 0.3 and 4.6 mm, respectively. On the femoral side, the smallest and largest error distances seen with the standard technique were 0.3 mm and 4.2 mm, respectively, while the smallest and largest error distances for the roadmapped technique were 0.7 mm and 8.3 mm, respectively.
Distance Between the Center of the ACL Anatomic Footprint and the Center of the Tunnels in the 16 Knees a

a ACL, anterior cruciate ligament.
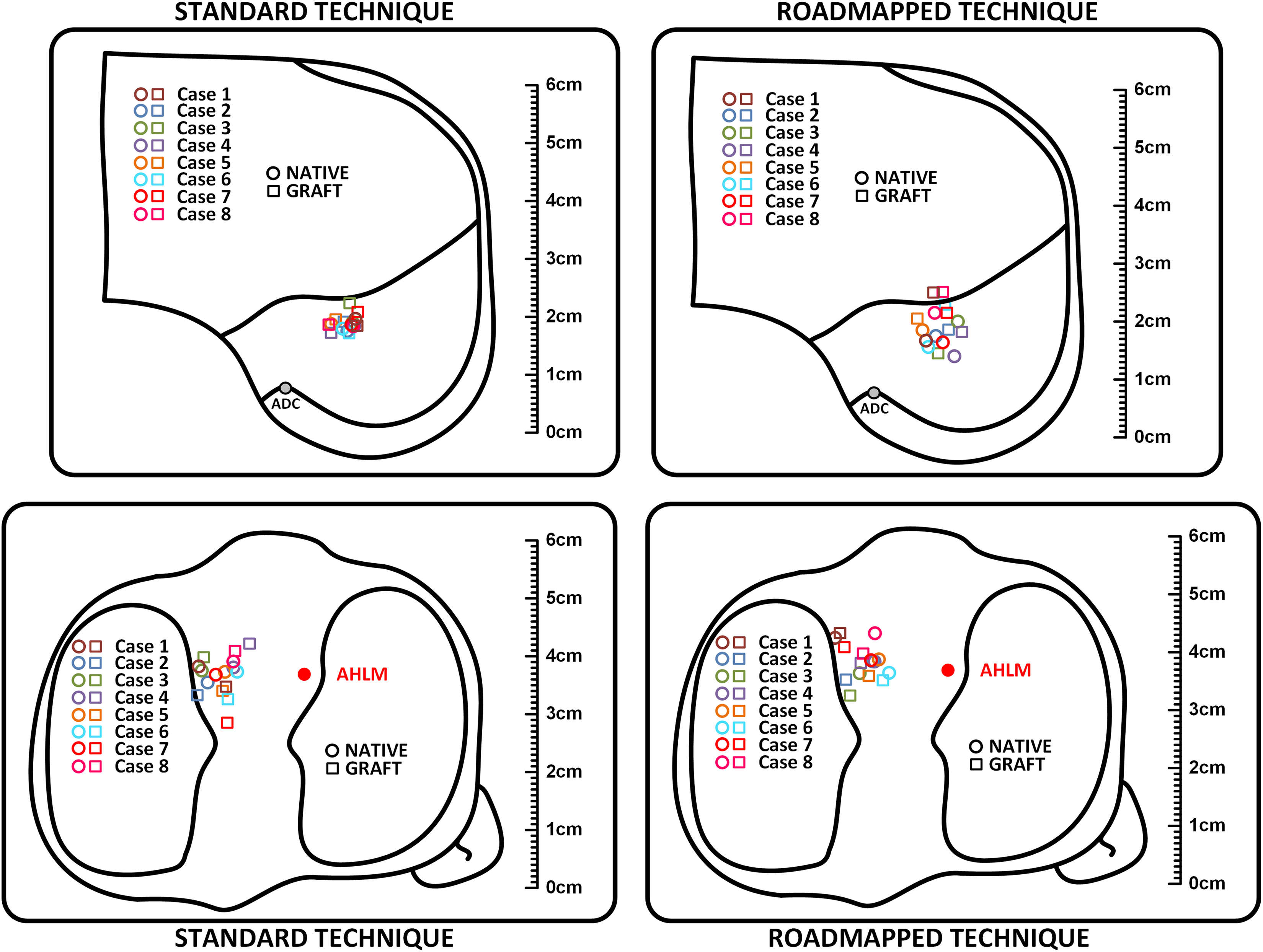
Scaled schematic diagram showing the native and reconstructed anterior cruciate ligament footprints created by the 2 different techniques. Each cadaver is represented by a circle and square of corresponding colors. On the femoral side, the diagram is a sagittal plane anatomic drawing of the lateral wall of the femoral intercondylar notch showing the Blumensaat line and the apex of the deep cartilage (ADC). On the tibial side, the diagram is an axial plane anatomic drawing of the proximal tibia showing the menisci and the anterior horn of the lateral meniscus (AHLM).
Discussion
This experiment showed that the roadmapped technique for ACLR is not superior to the standard ACLR technique. When provided with the 3D MRI measurements of the anatomic ACL footprint, the surgeon did not drill the graft tunnels in a better anatomic position. In fact, the use of arthroscopic landmarks and standard surgical decision-making resulted in tunnels that are positioned closer to the anatomic footprints of the ACL when compared to the roadmapped technique. The use of preoperative 3D MRI may help surgeons understand patient-specific footprint anatomy, but providing precise radiological position measurements preoperatively did not improve the surgeon’s ability to position the tunnels. Errors in creating tunnels at the native ACL tibial and femoral footprints existed in both techniques.
With the renewed interest in the insertional anatomy of the ACL on the tibial and femoral sides, an effort was made by Dhawan et al 5 made to reproduce the exact anatomic location of the ACL during ACLR. It was assumed that independent creation of the femoral tunnels through the AM portal would allow anatomic position of the ACL graft when compared with the transtibial technique of drilling the femoral tunnel. 5 With biomechanical testing, ACLR using the transtibial technique demonstrated an additional average of 2.2 mm in anterior tibial translation on simulated Lachman testing and 3.36 mm more anterior tibial subluxation on simulated pivot-shift test when compared with that done with the independent femoral drilling technique. 27 Despite these superior biomechanical findings, the overall short- and long-term clinical results were comparable. 5 In these previous studies, the position of the ACL graft tunnels was not assessed precisely; it was assumed that tunnels created using an independent femoral drilling technique were anatomic. Using 3D MRI, it was previously demonstrated 14 that a precise anatomic position of the femoral tunnel could not be achieved regardless of the femoral tunnel drilling technique used during surgery.
During the past few years, an effort has been made to understand the precise anatomy of the ACL footprints on the tibial and femoral sides by using 3D MRI and computed tomography scans to improve tunnel position and, eventually, clinical outcomes. 1,12,14,24,31 –33 In a cadaveric study by Han et al, 12 it was demonstrated that 3D MRI localization of the femoral and tibial footprints of the ACL is comparable with open dissection. Using the same 3D MRI technique, Hart et al 14 evaluated the tunnel positions that were created by 4 different orthopaedic sport surgeons for a series of patients in comparison with the native ACL footprint of the patients. They found that despite the technique used for ACLR and tunnel drilling, there was a mean error of 3.6 mm in graft position from the native femoral footprint, and 29% of the grafts were placed with more than half their area outside the anatomic femoral footprint. 14 Our study used the same 3D MRI technique that was used in these 2 previous studies. 12,14 We found that providing the surgeon with the precise anatomic location of the ACL footprints in relation to specific anatomic landmarks did not help improve the tunnel positions. Therefore, the information obtained from 3D MRI scans should be utilized in future studies to develop tools that can help better position the ACL tunnels. It is important to note, however, that experienced surgeons might be more competent in producing an anatomic position of the tunnels based on arthroscopic landmarks when compared with surgeons in their early years of practice; therefore, the 3D MRI measurements might be more helpful for the less experienced surgeons. Future studies are needed that compare 3D MRI with standard 2D radiographs and provide surgeons with feedback about their tunnel position with an aim to improve tunnel accuracy.
Several limitations exist in this study. First, the number of cadavers might be considered low; however, the measurements obtained by the 3D MRI were tightly grouped, and the fact that samples were matched pairs allowed for the use of a small sample size. Second, the mean age of the cadavers was higher than that of the usual ACLR patient. These cadavers, however, did not have significant arthritic changes that distorted the morphology of the anatomic landmarks of the knees. Finally, different drilling techniques were used to create the femoral tunnels between the 2 groups to help reach the footprint. This could have resulted in the differences of the location of the created femoral tunnels seen between the 2 groups. However, the surgeon who performed the procedures is accustomed to performing both techniques in his practice.
Conclusion
Providing preoperative 3D MRI measurements of the specific position of the native ACL footprint to the surgeon did not help improve the position of the tibial and femoral tunnels for ACLR. Future studies should continue to attempt to provide tools to improve the tunnel position in ACLR, because tunnel positioning overall is still not error free and can be made more accurate and reproducible.
Footnotes
Final revision submitted November 29, 2019; accepted December 17, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from McGill University (ref. No. 2018-4470).