
Abstract
Background:
The anterolateral ligament of the knee (ALL) is a component of the lateral complex that stabilizes the structure against rotational force and may be associated with the outcome of anterior cruciate ligament (ACL) reconstruction (ACLR).
Purpose:
To (1) find whether the visibility of the structure of the ALL is different in primary and revision ACLR groups, (2) determine whether the abnormal findings of the ALL structure on magnetic resonance imaging (MRI) scans are associated with type of trauma in ACL injury and mode of graft failure, and (3) determine whether there are differences in knee functional scores between patients with or without abnormal findings of the ALL structure on MRI scans in primary and revision ACLR groups.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective study included 40 patients who underwent primary ACLR and 39 patients who underwent revision ACLR. Conventional MRI (1.5-T) scans taken before primary or revision ACLR were obtained and analyzed for visibility of the ALL, frequency and degree of injury of the ALL, and ALL signal anomalies. We also evaluated 1-year postoperative functional knee scores using the subjective International Knee Documentation Committee and Lysholm scores.
Results:
Visibility of the ALL was better in the primary ACLR group than the revision ACLR group (38% vs 14%; P = .041). The primary ACLR group showed a lower degree of injury across the femoral, meniscal, and tibial attachment sites than did the revision ACLR group (30% vs 13%, 41% vs 8%, and 62% vs 26%, respectively). Relative signal anomaly of the ALL was more frequent in the case of contact versus noncontact trauma of the ACL (85% vs 15%; P = .035), while absolute signal anomaly was equally observed between cases of contact and noncontact trauma in the primary ACLR group (50% vs 50%). No association was observed between ALL signal anomalies and 1-year postoperative functional knee scores.
Conclusion:
The revision ACLR group offered less visibility and showed a tendency for more frequent, higher degree of injury to the structure of the ALL. Regardless of observational differences between the 2 groups, no definite relevance was observed between the image and the functional outcome. For the assessment of the ALL, routinely performed conventional MRI alone is insufficient to make a clinical decision.
The anterolateral ligament (ALL) of the knee is claimed to be a component of the lateral complex that stabilizes the structure against rotational force. 26 Rotational stability is associated with a better outcome of anterior cruciate ligament (ACL) reconstruction (ACLR), and failure to recognize concurrent instability is reported to be a cause of failure of the ACLR graft. 19 The recent literature has suggested ALL injury as a culprit for the suboptimal outcome of ACLR. 6,17,27 To ensure a better outcome after ACLR, restoration of the rotational stability is important. 4 However, the treatment of the ALL during treatment of patients with ACL injury is still controversial because of its anatomic obscurity and mostly because of lack of a gold standard assessment modality of a gold standard. 3
The assessment of the ALL is even more difficult in the case of revision ACLR, which is more complex. 5 As magnetic resonance imaging (MRI) is the tool of choice in evaluating ligamentous structures, a few previous studies have endeavored to utilize MRI to assess the structure of the ALL. 7,8,16,23 The assessment of a damaged ALL has remained elusive because of the location of the ligament, which is adjacent to the lateral collateral ligament and the popliteal tendon. 16 In theory, an injury to the ALL of the knee would reflect more severe damage of the ACL, with a higher incidence of concurrent injury to other structures of the knee. As a result, an ACL structure injured repetitively, as seen in a revision surgery case, would be more prone to show injuries to the ALL.
There is a paucity of literature on abnormal findings of the ALL structure on MRI scans and the consequential functional score of the knee. 14 Reports from previous studies have supported that integrity of the ALL is related to the retear rate of the ACL 21 ; however, it is not obvious whether abnormal findings of the ALL structure on MRI scans reflect the worse clinical outcome after an ACLR. Although ALL reconstruction surgery is often performed with revision ACLR, it is not known how this additional ligament reconstruction influences the clinical outcome of revision ACLR. Evidence surrounding diagnosis and treatment of ALL injuries is scarce.
In this study, we aimed to determine whether the visibility of the ALL on conventional MRI scans and the incidence of abnormal findings of the ALL structure on MRI scans were different between primary and revision ACLR cases. We hypothesized that the structure of the ALL would have a lower visibility in the revision ACLR group. In addition, we hypothesized the abnormal findings of the ALL structure on MRI scans would be associated with the type of trauma in ACL injury and the mode of graft failure after an ACLR. Finally, we also sought to determine whether there was a difference in knee functional scores between patients with and without abnormal findings of the ALL structure on MRI scans in primary and revision ACLR groups.
Methods
This institutional review board–approved study was based on 79 cases of ACLR, both primary and revision, performed at our institution between 2014 and 2018. We reviewed ACLR cases that included 40 cases of primary ACLR (mean ± standard deviation [SD] age, 33 ± 12.6 years; 3 women and 37 men) and 39 cases of revision ACLR (mean ± SD age, 32 ± 12.2 years; 2 women and 37 men) performed at our institution. The general indication for primary and revision ACLRs is instability described by a patient, with objective findings on conventional MRI and physical examinations (grade ≥1 on the pivot-shift test and/or grade ≥2 on the Lachman test). 1
MRI (1.5-T Gyroscan Intera; Philips) scans taken before primary or revision ACLR were obtained and analyzed using the picture archiving and communications system and the Digital Imaging and Communications in Medicine viewer. For evaluation, the axial proton density (PD)–weighted fast spin-echo sequence (repetition time/echo time, 2300-3700 milliseconds/6-15 milliseconds) was used as a scout image to locate the approximate location of the femoral attachment. The coronal fat saturated T2- and PD-weighted fast spin-echo sequence (repetition time/echo time, 2500-3500 milliseconds) views were oriented according to the femoral position, parallel to the femoral condyle.
The ALL was assessed for its visibility (nonvisible or visible) regarding attachment sites and the degree of signal intensity on MRI scans. Visibility of the ALL was evaluated in detail regarding its 3 portions of attachment: femoral, meniscal, and tibial (Figure 1).

(A) Schematic drawings of the ALL of the knee and (B) the corresponding coronal and axial magnetic resonance imaging scans. F, M, and T represent the femoral, meniscal, and tibial attachments of the structure. ALL, anterolateral ligament; ITB, iliotibial band; LCL, lateral collateral ligament; LM, lateral meniscus.
Considering its known anatomic structure, which has a mean ± SD length of 38.5 ± 6.1 mm and width of most narrow point at 6.7 ± 3 mm, our 3 mm–thickness MRI scan was able to detect 1 or 2 images in the coronal view at most. 3 For this reason, we labeled the structure as visible when it was observable at least in 1 image cut. 3,8 The degree of ALL signal intensities was graded according to the collateral ligament injury grading criteria introduced by Schweitzer et al 20 and described by others. 5,10,11,25 The absolute signal anomalies of the ALL were defined as (1) grade 3 signal observed at ≥1 attachment or (2) grade 2 signals observed at ≥2 attachments. Cases in which structural configuration could not be observed were also considered as an absolute signal anomaly. The relative signal anomaly was defined as grade 2 signal observed at <2 attachment sites or grade 1 signal observed in all 3 attachments.
Whether the event of trauma or type of trauma (contact or noncontact) affected the injury was reviewed using medical records and considered in the analysis of ALL injury in the primary ACLR group. For the revision ACLR group, instead of types of trauma, we compared types of failure because of the graft from the primary reconstruction.
All images were assessed by 2 knee fellowship--trained orthopaedic surgeons (D.S., M.J.C.) and a radiologist with a musculoskeletal specialty. All images were independently reviewed and graded using the picture archiving and communications system, and then the results of the assessment were compared. Each portion (femoral, meniscal, and tibial) of the ALL and the visibility, injury grade, and signal anomaly assessments were performed separately and matched to the patient’s medical records. The assessment was performed twice for each observer over the period of 1 week. The subjective International Knee Documentation Committee (IKDC) and Lysholm scores were used for functional evaluation of the knee after reconstruction surgery. At the time of postoperative follow-up at the outpatient clinic 6 months and 1 year after the surgery, patients completed the questionnaires, which were scored accordingly.
Descriptive data were described using means and SDs. The view of each portion of the ALL according to attachment sites regarding visibility, degree, and type of trauma in relation to the degree of abnormal signal intensities of the ALL was described using numbers and proportions. To compare primary and revision ACLR groups, these numbers and proportions were evaluated for statistical significance using the chi-square test. Knee functional scores were described using means and SDs and were tested using the Student t test. The intra- and interobserver reliability of the image assessments was measured using the kappa statistic, in which values may range from -1 to 1 (-1 = complete disagreement; 0 = chance agreement; 1 = complete agreement).
Results
Visibility of the ALL in the primary ACLR group was better than that in the revision ACLR group (Table 1).
Number of Views and Percentage Viewing of Each Portion of the ALL Separately and All 3 Portions Together in MRI Evaluation a
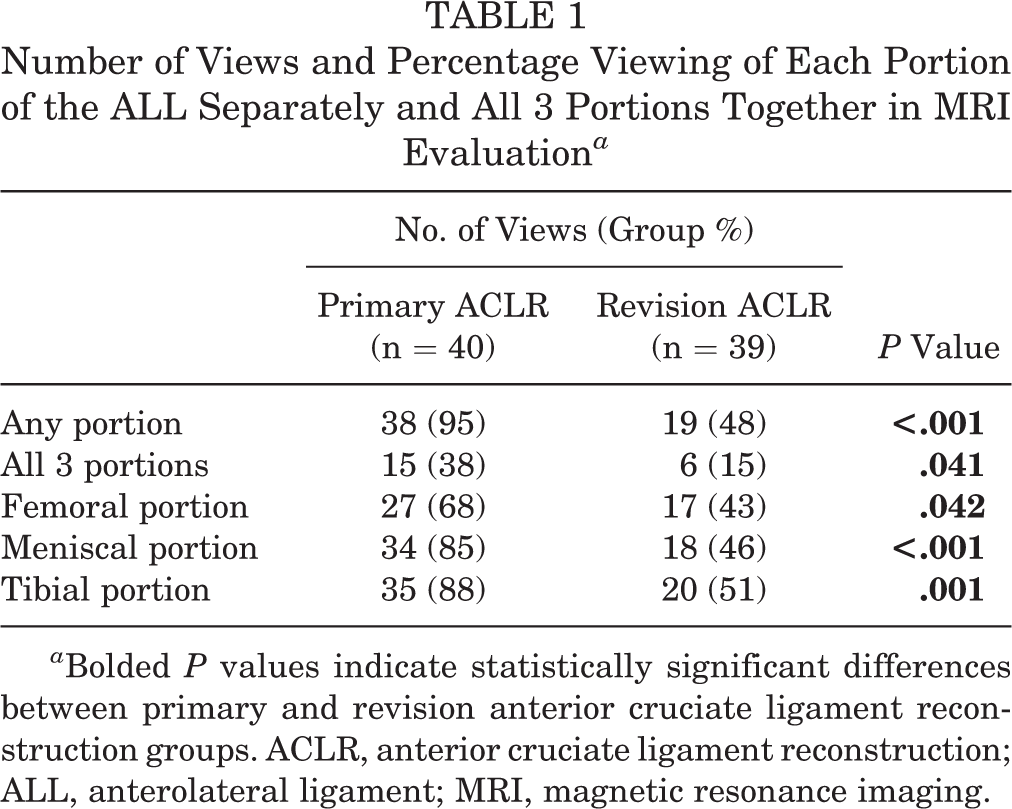
a Bolded P values indicate statistically significant differences between primary and revision anterior cruciate ligament reconstruction groups. ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; MRI, magnetic resonance imaging.
In the primary ACLR group, any portion of the ALL was visible in 38 cases (95%), while the ALL was visible in all 3 portions only in 15 cases (38%). In comparison, the revision ACLR group yielded less visibility. Any portion of the ALL was visible in 20 cases (51%), while the ALL was visible in all 3 portions only in 6 cases (15%). High-grade signal anomalies across the femoral, meniscal, and tibial portions were higher in the revision ACLR group (Table 2). Grade 3 signals were more common in the femoral portion than in the meniscal or the tibial portion in both primary and revision ACLR groups.
Number of Views and Percentage Viewing of Each Portion of the ALL Separately According to Degree of Injury Grading System a

a Data are presented as No. of knees (group %). Bolded P values indicate statistically significant differences between primary and revision ACLR groups. ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament.
There were significant differences in signal anomalies according to the type of trauma (contact, 26 cases; noncontact, 12 cases) in the primary ACLR group. The relative signal anomaly of the ALL was more frequent in cases of contact trauma, while the absolute signal anomaly was more frequent in noncontact trauma cases (P = .035) (Table 3).
Types of Trauma in Primary and Types of Graft Failure in Revision ACLR Groups a

a Data are presented as No. of knees (group %). The bolded P value indicates a statistically significant difference in signal anomaly between contact and noncontact trauma. ACLR, anterior cruciate ligament reconstruction.
The absolute signal anomaly group had 9 cases of contact and 9 cases of noncontact trauma, while the relative signal anomaly group had 17 cases of contact and 3 cases of noncontact trauma. On the contrary, such differences in signal anomalies were not apparent in the revision ACLR group. The overall graft failure was more frequently related to the event of trauma both in absolute and relative signal anomalies of the ALL. The number of traumatic graft failures was 18 cases in the absolute signal anomaly group and 7 cases in the relative signal anomaly group. Nontraumatic failure occurred in 10 cases in the absolute signal anomaly group and 4 cases in the relative signal anomaly group (Table 3). Kappa values for intraobserver reliability and interobserver reliability were ≥0.93 (range, 0.93-0.98) and ≥0.91 (range, 0.91-0.98), respectively, indicating excellent agreement.
At 1-year follow-up, knee functional scores in the primary and revision ACLR groups were not different, regardless of the status of the ALL (Table 4). In primary and revision ACLR groups, knee function, checked using the IKDC and Lysholm scores, was not different between absolute and relative signal anomaly groups.
Postoperative IKDC and Lysholm Scores at 1-Year Follow-up in Relation to ALL Absolute and Relative Signal Anomalies in Primary and Revision ACLR Groups a

a Data are presented as mean ± SD. ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; IKDC, International Knee Documentation Committee.
Discussion
The main findings of our study were that (1) visibility of the ALL structure was significantly better in the primary ACLR group compared with the revision ACLR group; (2) the frequency of high-grade signal anomaly across the femoral, meniscal, and tibial portions was higher in the revision ACLR group; (3) signal anomalies of the ALL differed among types of trauma in the primary ACLR group; and (4) there was no relationship between functional knee scores after surgery and degree of the signal anomalies in the ALL structure in the primary and revision ACLR groups.
Our findings showed that conventional MRI scans depict the structure of the ALL, as suggested in the previously reported literature. ∥ It was possible to observe the structure pertinent to the condition of surrounding structures of the lateral complex of the knee. As we hypothesized, in the revision ACL group in which cumulative and/or higher degree of combined injury would have occurred, more frequent signal anomalies were observed in the ALL structure within its known attachment sites. On the other hand, our observation of visibility of the uninjured ligament was comparable with that of previously reported literature on uninjured ALLs. 12 Although this contrast cannot explain every aspect of the status of the ALL in the 2 groups, a tendency for a condition that makes it more difficult to assess the structure is certain.
To our knowledge, the degree of ALL injury in the primary and revision ACLR groups had little comparable data from previously reported literature. We found that this degree and the frequency of ALL injury was lower in the primary ACLR group, with grade 1 or 2 injuries, most of which occurred at the tibial attachment. The revision ACLR group showed more grade 2 or 3 injuries in the meniscal and the femoral attachment portion. These differences between the 2 groups suggest that ALL injury could be more severe in the revision ACLR group and may require more medical attention and/or additional procedures. Our findings regarding the status of the ALL are in accordance with the context of a previous report by Saithna et al 19 who included revision ACLR as their indication for ALL reconstruction because of similar concerns about increased risk of ACL graft failure. 19 Although no study has observed functional differences resulting from such procedures, the finding may support the rationale behind advocating for the combined ACL and ALL reconstruction surgery. 21
Contact or noncontact damage done to the ACL structure showed different results between absolute and relative signal anomaly of the ALL in the primary ACLR group. In contrast, ACL graft failure in the revision ACLR group, whether related to a traumatic or nontraumatic event, was not relevant to signal anomalies. This observation reflects the possibility of the cumulative nature of injury influencing the structure of the ALL and reveals uncertainty of interpretation in revision ACLR cases.
Our findings regarding the knee functional score and its relation to signal anomaly did not support the hypothesis, in that it would be possible to observe consequential relevance between signal anomalies of the ALL and the actual knee functional score. In our current study, the difference in signal anomalies of the ALL observed in the 2 groups did not translate into a visible clinical outcome. In accordance with our finding, Lee et al 14 reported clinical scores including the IKDC, Lysholm, and Tegner scores of the ACLR group and the combined ACL and ALL surgery group after a 1-year follow-up to be similar (77 ± 17 vs 79 ± 19, 85 ± 18 vs 89 ± 17, 7 ± 1 vs 7 ± 1, respectively). Thus, it is yet to be determined whether the prediction of the functional outcome could be expected from signal changes in conventional MRI. Both the previous and our current report suggest that MRI is not a definitive imaging method when it comes to observation of the ALL structure. Nevertheless, it is one of the most accessible, if not the only, perioperative assessment tools surgeons can have in their arsenal. 7,12,24 We deem this assessment needs to be complemented by a compensatory diagnostic modality to be fully effective in further research.
A few limitations to the current study should be considered. First, because it was a retrospective study, we could not observe index MRI scans, which is the image collected prior to the primary reconstructive procedure, and thus we had limitations in explaining the status of the ALL. Also, we could not specify the time from trauma to MRI because of missing information and thus could not report how acute the situation was regarding the status of the ALL in the primary ACLR group. Prospective and randomized studies may yield more refined interpretation and control over the settings of the cohort. Second, we used 1.5-T MRI, which had limited resolution that could have affected interpretation. A scan with a better resolution and a thinner section with an image mode specifically matched to the structure of the ALL would offer more solid data for analysis. Third, as reported in the previous literature, researchers have not reached a consensus on how to assess the condition of the ALL when findings are abnormal. 7 Controversies surrounding the structure itself should be resolved in due time. Fourth, because we utilized certain standards to assess the integrity of the ALL to render objectivity to our observation, we considered situations where the ligament could not be observed to be an absolute signal anomaly, while it might have been simply omitted from the scan range of conventional MRI. This technical limitation could be overcome using more refined imaging protocols and better equipment. To deal with these currently limiting issues, we used a consistent definition to depict the terms of integrity of the ligament and signal anomaly to minimize potential errors from the subjective nature of the assessment. With similar standards, definition, and modality, we believe our result to be reproducible. Fifth, because the follow-up period after surgery was relatively short, we could not state whether there were any correlations with clinical scores at a longer period of time.
Conclusion
The primary ACLR group yielded better visibility and offered more solid ground to assess the ALL. The revision ACLR group offered less visibility and showed tendency for more frequent, higher degree of injury to the structure of the ALL. Regardless of these differences between the 2 groups, no obvious clinical relevance was observed between image findings and functional outcome. Thus, for the perioperative evaluation of the ALL, assessment using routinely performed conventional MRI alone is insufficient to make clinical decisions and should be complemented with yet another diagnostic modality.
Footnotes
Notes
Final revision submitted January 31, 2021; accepted February 28, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Bio & Medical Technology Development Program of the National Research Foundation funded by the Korean government (2017M3A9D8063538). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Boramae Medical Center (IRB No. 20190405/10-2019-33/051).