
Abstract
Background:
Knot-tying suture-bridge (SB) rotator cuff repair may compromise the vascularity of the repaired tendon, causing tendon strangulation and medial repair failure. The knotless SB repair technique has been proposed to overcome this possibility and decrease retear rates.
Purpose:
To compare clinical and structural outcomes and retear patterns between the knot-tying and knotless SB techniques. We hypothesized that the knotless technique would result in lower retear rates owing to the preservation of intratendinous vascularity.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 104 patients with full-thickness rotator cuff tears were randomly and prospectively allocated to undergo knot-tying (group 1) or knotless (group 2) SB repair. Clinical outcome measures included range of motion, the visual analog scale (VAS) for pain, and the Constant score for function. Repair integrity was evaluated on magnetic resonance imaging scans using the Sugaya classification. Retears were also classified according to their pattern as type 1 (lateral) or type 2 (medial).
Results:
Overall, 88 patients (group 1: n = 42 [mean ± SD age, 54.3 ± 9.8 years]; group 2: n = 46 [mean ± SD age, 55.8 ± 8.2 years]) were included in the final analysis. The mean ± SD follow-up period was 25.4 ± 8.3 and 23.3 ± 7.2 months for groups 1 and 2, respectively. From preoperatively to postoperatively, the mean VAS pain score improved significantly in both groups (group 1: from 7.4 ± 1.7 to 1.0 ± 1.7; group 2: from 7.1 ± 1.9 to 1.3 ± 2.0; P < .0001 for both), as did the mean ± SD Constant score (group 1: from 51.7 ± 13.4 to 86.0 ± 11.5; group 2: from 49.4 ± 18.4 to 87.2 ± 14.8; P < .0001 for both). There was no significant difference between the groups for the postoperative VAS or Constant score. The retear rate was not significantly different between the groups (19.0% [8/42] in group 1 and 28.3% [13/46] in group 2; P > .05). There was a significant difference in the type 2 failure rate (75.0% [6/8] in group 1 and 23.1% [3/13] in group 2; P = .03).
Conclusion:
Both techniques showed excellent improvement and comparable clinical outcomes, and there was no significant difference in retear rates. Consistent with previously published data, the type 2 failure rate was significantly higher with the knot-tying technique.
Registration:
NCT03982108 (ClinicalTrials.gov identifier).
In recent years, advances in arthroscopic techniques and surgical instruments have led to the development of new arthroscopic rotator cuff repair (RCR) procedures. The key consideration for these breakthroughs was to obtain stronger fixation, better mechanical stability, and anatomic reconstruction of the tendon-bone junction over the footprint, with a large contact area and minimal gap to achieve a suitable environment for tendon healing. 9,12 Currently, the arthroscopic “transosseous-equivalent” or “suture-bridge” (SB) technique is widely used owing to better biomechanical properties and clinical outcomes compared with single- or double-row repair techniques. 23,24,26 However, a retear after RCR still constitutes a major concern.
The conventional arthroscopic SB technique is performed by inserting knotted anchors for the medial row. However, this technique has been suspected to compromise the vascularity of the repaired tendon by causing strangulation and eventually increasing the risk of retears at the musculotendinous junction (type 2 retears). 3 –5,31 Type 2 (medial) retears can cause impingement and are associated with pain and lower shoulder function and quality of life. 19,30 Moreover, revision of type 2 failure is more challenging. 1 Therefore, an SB RCR technique that uses knotless medial-row anchors has been developed to avoid overtensioning of the suture-tendon junction at the medial row and improve vascular inflow. 11,13,27 However, evidence is lacking regarding the superiority of the knotless technique over the knot-tying technique.
The purpose of this study was to evaluate and compare the clinical and radiologic outcomes of the medial knot-tying versus knotless arthroscopic SB RCR technique. We hypothesized that owing to its biological advantages, the knotless technique would result in lower retear rates compared with the knot-tying technique.
Methods
Study Design and Setting
This study was a randomized, prospective comparative clinical trial. A single-blinded (participants) masking and parallel assignment protocol was followed, and ethics review committee approval was obtained before the initiation of the study. The trial was registered at ClinicalTrials.gov (NCT03982108). The CONSORT (Consolidated Standards of Reporting Trials) guidelines 20 were followed when reporting study results.
Patient Selection
Patients from a single university hospital were recruited for this study between May 2017 and August 2018. Inclusion criteria were (1) full-thickness rotator cuff tears confirmed during surgery and (2) repair of the tear using either knot-tying or knotless arthroscopic SB RCR. Exclusion criteria were (1) age <18 years, (2) partial-thickness rotator cuff tears, (3) presence of a full-thickness subscapularis tear that required an intervention, (4) presence of severe glenohumeral or acromioclavicular joint arthritis, (5) any previous surgery of the affected shoulder, (6) history of a neurologic disease or rheumatic condition, and (7) revision surgery. All recruited patients received written and verbal information about the trial and provided written informed consent. All diagnoses were made by the senior author (A.E.) based on a clinical examination and preoperative magnetic resonance imaging (MRI) scans. The operative indication was the persistence of symptoms despite nonoperative treatment for at least 6 months.
Sample Size
The sample size calculation was performed on the basis of the evidence available at the time, which indicated a difference of 25.8% in retear rates (7.5% for knot-tying technique vs 33.3% for knotless technique). 16 The calculation resulted in a sample size of 38 patients for both groups with a power of 80% and a significance level of .05. The sample size calculation was performed using G*Power software (Version 3.1.9.4).
Randomization
A computer-generated random list was established using an online randomization sequencer (https://www.random.org/sequences/). Participants were randomly assigned to either knot-tying (group 1) or knotless (group 2) SB RCR following this random list with a 1:1 allocation ratio.
Surgical Procedure
All interventions were performed by the senior author with patients under general anesthesia and in the beach-chair position. After the administration of antibiotic prophylaxis and skin preparation, a posterior portal was established for diagnostic arthroscopic surgery of the glenohumeral joint. An anterior portal was then established through the rotator interval. Intra-articular abnormalities including chondral and labral lesions, long head of the biceps tendon (LHBT) lesions, and subscapularis lesions were evaluated. Tenotomy of the LHBT was performed based on the condition of the tendon as well as the age and activity level of the patient.
Then, the arthroscope was redirected toward the subacromial space. After establishing an anterolateral portal and a posterolateral portal, pathologic bursal tissue was removed, and the rotator cuff was carefully investigated for size, location, retraction, mobility, and delamination of the tear. In patients with poor rotator cuff mobility, extensive release of the capsule and the rotator cuff was performed. Routine subacromial decompression was performed to obtain a smooth and flat acromial undersurface. Subsequently, footprint preparation was performed via debridement of soft tissue using a shaver and decortication of the bone using a bur to obtain a bleeding spongy footprint.
The number of medial-row anchors was determined after considering the size and retraction of the tear. In general, 1 anchor was used for small tears, 2 anchors were used for medium and large tears, and 3 anchors were used for massive tears. In addition, 3 anchors were preferred in patients with high-grade retraction (grade 3) for better tension sharing to reduce the tendon. For knot-tying SB RCR, medial-row anchors (Healicoil Suture Anchor; Smith & Nephew) loaded with 2 No. 2 braided and nonabsorbable sutures (Ultrabraid; Smith & Nephew) were inserted just lateral to the articular margin of the humeral head. Suture limbs were passed through the tendon, lateral to the musculotendinous junction, by using 2 different suture passers (Firstpass or Accu-Pass; Smith & Nephew) to create a horizontal mattress configuration with an approximate distance of 1 cm between stitches. After medial-row repair, knots were tied using a sliding nonlocking knot, followed by 3 alternating half-hitches, to secure the knot for each suture, but suture limbs were not cut. Soft tissue overlying the bone distal to the footprint was removed, and pilot holes for knotless lateral-row anchors (Footprint PK; Smith & Nephew) were established approximately 1 cm distal to the lateral edge of the greater tuberosity. Suture limbs from each suture were then retrieved through a portal and loaded to lateral-row anchors, and these anchors were inserted into the pilot holes by adjusting the tension of the SB and reducing the rotator cuff to an adequate position over the footprint. The procedures were terminated by cutting the free suture limb ends on the lateral-row anchors (Figure 1).
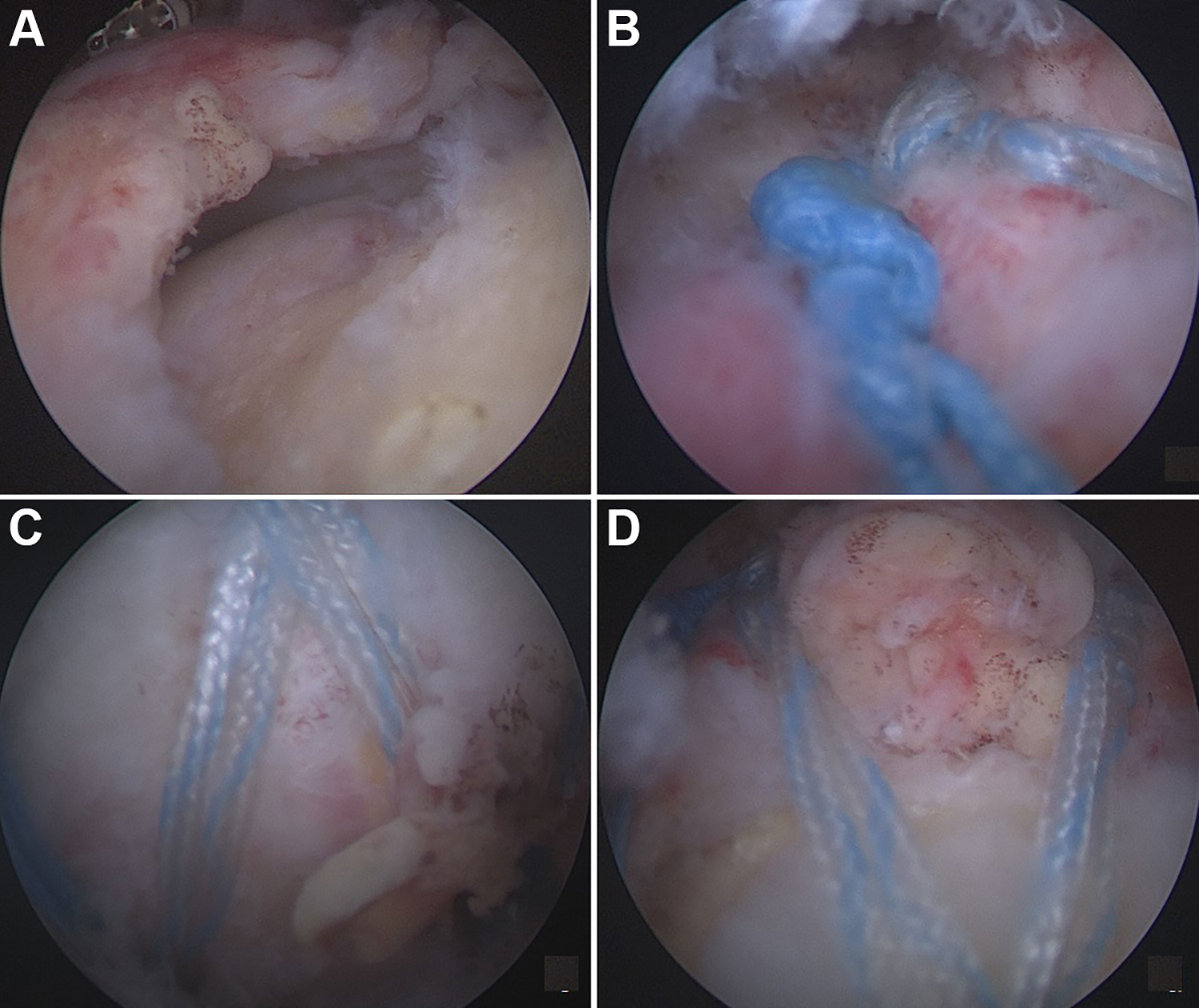
Intraoperative view of knot-tying suture-bridge rotator cuff repair. (A) View of the rotator cuff tear from the posterolateral portal. (B) View of the medial row with tied knots. (C, D) View of the suture bridge and lateral-row anchors after the completion of repair.
The same preparation procedure was followed for the knotless SB RCR technique. For this technique, medial-row anchors (Healicoil Suture Anchor) loaded with 1 No. 2 braided and nonabsorbable suture (Ultrabraid) and 1 nonabsorbable suture tape (Ultratape; Smith & Nephew) were used. Medial-row repair was performed in a similar manner to the previous technique without tying any knots. After preparing and establishing lateral-row pilot holes, 1 limb of each suture and suture tape from each anchor were retrieved through a portal and then loaded to knotless lateral-row anchors (Footprint PK). Then, these anchors were inserted in a similar manner, creating an SB over the rotator cuff with adequate tension and reduction of the tendon on the footprint (Figure 2).

Intraoperative view of knotless suture-bridge rotator cuff repair. (A) View of the rotator cuff tear from the posterolateral portal. (B) Preparation of the footprint with decortication using a bur. (C) Insertion of lateral-row anchors. (D) Final view of the repair site.
Postoperative Rehabilitation
All patients wore an abduction shoulder sling positioned in 30° of abduction and neutral rotation for 6 weeks. Active elbow motion and passive shoulder motion were allowed immediately after surgery. All patients were periodically followed up by the same physical therapist from the physical therapy unit of our clinic and underwent a standard rehabilitation protocol starting from 6 weeks postoperatively. All patients visited the physical therapist 3 times a week for 8 weeks. Active-assisted shoulder range of motion (ROM) exercises were initiated starting from 6 weeks, respecting pain-free ROM limits. Active ROM and strengthening exercises were introduced gradually at 8 to 10 weeks postoperatively. Full physical activity and return to sports were allowed 6 months after surgery according to the recovery of each participant.
Patient Assessment
All patients were clinically evaluated by the first author (K.Ş.) 1 day before surgery. Demographic data of the patients and factors that could affect tendon healing and the outcomes of surgery (smoking history, diabetes history, corticosteroid injection history to the affected shoulder) were investigated and recorded. Postoperative evaluations were performed by the same author at 2 weeks, 6 weeks, 3 months, 6 months, 12 months, and each following year after surgery. Data from the latest follow-up were used for final analysis.
Preoperative and postoperative subjective pain was evaluated using the visual analog scale (VAS). The active ROM assessment of the shoulder included abduction, forward flexion, external rotation at the side with the elbow at 90° of flexion, and internal rotation to the back. Abduction, forward flexion, and external rotation measurements were performed using a goniometer. Internal rotation measurements were performed according to the highest level that the patient’s hand reached behind the back and were categorized into 6 levels: lateral thigh, buttock, lumbosacral, lumbar, thoracolumbar, and interscapular. Preoperative and postoperative functional outcomes were assessed using the Constant score. 6 Data concerning surgery such as tenotomy of the LHBT, surgery duration, and complications were also recorded.
Magnetic Resonance Imaging
All patients underwent preoperative MRI to evaluate the rotator cuff tear and confirm the clinical diagnosis. The preoperative MRI evaluation included tear size, tear retraction, and fatty infiltration. Tear size was classified, as described by DeOrio and Cofield, 7 using T2-weighted sagittal oblique images: small, <1 cm; medium, 1 to 3 cm; large, 3 to 5 cm; and massive, >5 cm. Tear retraction was evaluated using the Patte classification 25 on T2-weighted coronal oblique images, consisting of 3 grades: (1) minimal retraction, the tear stump is lateral to the articular edge of the humeral head; (2) moderate retraction, the tear stump is between the lateral margin of the humeral head cartilage and glenoid; and (3) severe retraction, the rotator cuff is retracted medial to the glenoid. Fatty infiltration of the supraspinatus and infraspinatus muscles was assessed using the Fuchs modification 8 of the Goutallier classification 10 on T1-weighted sagittal oblique images: grade 0, no fatty infiltration in the muscle; grade 1, little amount of fatty streaks in the muscle; grade 2, more muscle than fat; grade 3, equal amount of muscle and fat; and grade 4, more fat than muscle. The higher stage between the supraspinatus and infraspinatus muscles was taken into consideration.
All patients underwent postoperative MRI at a minimum of 6 months after surgery. The postoperative radiologic assessment included structural integrity of the repaired rotator cuff and pattern of the retear when a retear was observed. Repair integrity was evaluated using the classification described by Sugaya et al 29 on T2-weighted coronal oblique and sagittal oblique images, consisting of 5 types: (1) homogeneous low signal of the tendon with sufficient thickness; (2) partial high-intensity signal present in the tendon with sufficient thickness; (3) tendon continuity is preserved, but thickness is insufficient; (4) minor discontinuity on >1 slice, suggesting a small tear; and (5) a large tear with major discontinuity. Successful repair was taken into consideration when types 1 to 3 were observed, and types 4 and 5 were considered as repair failures/retears (Figure 3). Retears were also classified according to the classification described by Cho et al 4 : detachment of the repaired rotator cuff from the footprint was considered as a type 1 retear, and the presence of failure at the medial musculotendinous junction with a laterally healed tendon on the footprint was considered as a type 2 retear (Figure 4).

Postoperative magnetic resonance imaging assessment. (A) A successfully healed rotator cuff with complete tendon integrity (Sugaya type 1). (B) A patient with maintained tendon integrity but insufficient thickness (Sugaya type 3). (C) Complete loss of tendon continuity and repair failure (Sugaya type 5).

Retear patterns on postoperative magnetic resonance imaging scans. (A) Type 1/lateral retear. (B) Type 2/medial retear.
All MRI scans were obtained using a 1.5-T magnetic resonance unit (Magnetom Aera; Siemens) with a dedicated shoulder coil and the arm positioned in a standard neutral position. T1- and T2-weighted images in the axial, coronal oblique, and sagittal oblique planes were obtained. Acquired images were stored in a DICOM (Digital Imaging and Communications in Medicine) format, and radiologic evaluations were performed using RadiAnt DICOM Viewer Software (Version 5.5.0; Medixant). All radiologic assessments were performed by a senior musculoskeletal radiologist experienced in shoulder radiology and who was blinded to patient and study data.
Statistical Analysis
All statistical analyses were performed using GraphPad Prism Software for Windows (Version 8.0.1; GraphPad Software). The mean, SD, median, interquartile range, range, frequency, and percentage were used as descriptive statistical methods to analyze the study data. The distribution of quantitative variables was assessed using the Shapiro-Wilk test, Kolmogorov-Smirnov test, histograms, and probability plots. A comparison of quantitative variables with a normal distribution was made using the Student t test. The Mann-Whitney U test was used to compare quantitative variables that were not normally distributed. Intragroup comparisons of quantitative variables were made using the paired-samples test if a normal distribution was observed and using the Wilcoxon signed rank test otherwise. Categorical variables were analyzed using the Pearson chi-square test and the Fisher exact test. Statistical significance was set at P = .05 for all analyses.
Results
A total of 123 patients underwent RCR during the study period; of these, 104 patients were enrolled in the study, and 19 were excluded (17 patients did not meet the inclusion criteria, and 2 patients declined to participate in the trial). Enrolled patients were randomly allocated to 2 groups of treatment: 51 patients to group 1 and 53 patients to group 2. Overall, 16 patients were considered lost to follow-up (postoperative MRI scans were unavailable for 6 patients, and 10 patients did not attend postoperative visits or were unable to be reached). Final analysis was performed with 88 patients (42 patients in group 1 and 46 patients in group 2; follow-up rate: 84.6%) (Figure 5).

Flow diagram of the study. MRI, magnetic resonance imaging; RCR, rotator cuff repair; SB, suture bridge.
The patients who were included in the final analysis consisted of 32 men (36.4%) and 56 women (63.6%). Details regarding demographic data, smoking history, diabetes history, preoperative corticosteroid injection history and number of injections, follow-up period, and postoperative MRI time are shown in Table 1. No statistically significant difference was observed between the groups. There was also no significant difference between the study groups in terms of preoperative tear size, tear retraction, or fatty infiltration on MRI scans (Table 2).
Descriptive Data a

a MRI, magnetic resonance imaging. Dashes indicate not applicable.
b Data are reported as mean ± SD or n (%).
c Student t test.
d Mean difference.
e Pearson chi-square test.
f Mann-Whitney U test.
g Median difference.
h Fisher exact test.
Preoperative Tear Size, Tear Retraction, and Fatty Infiltration a

a Data are reported as n (%).
b Pearson chi-square test.
Range of Motion
In both groups, the mean abduction, forward flexion, and external rotation values increased significantly from preoperatively to postoperatively (P < .0001 for all). There were no significant differences when comparing preoperative and postoperative abduction, forward flexion, and external rotation values between the 2 groups (Table 3). The comparison of shoulder internal rotation between the groups, categorized into areas that the patients could touch with their hands at their back, is shown in Table 4. The analysis revealed that there was no statistically significant difference between the groups in terms of preoperative and postoperative internal rotation values (P > .05).
Preoperative and Postoperative Range of Motion a
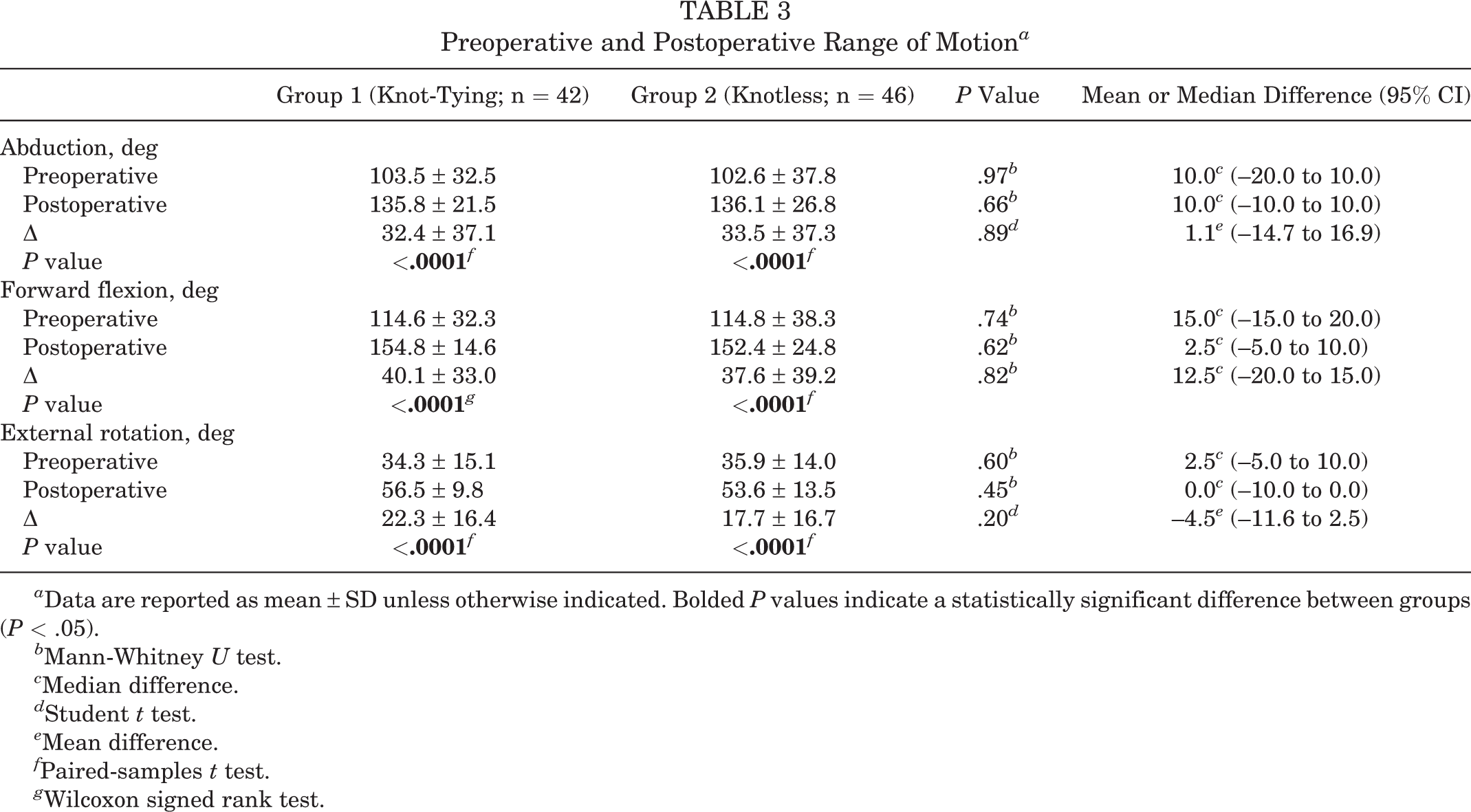
a Data are reported as mean ± SD unless otherwise indicated. Bolded P values indicate a statistically significant difference between groups (P < .05).
b Mann-Whitney U test.
c Median difference.
d Student t test.
e Mean difference.
f Paired-samples t test.
g Wilcoxon signed rank test.
Preoperative and Postoperative Internal Rotation a

a Data are reported as the number of patients who were able to reach each level with their hand behind their back.
b Pearson chi-square test.
Pain and Functional Outcomes
In both groups, the mean VAS pain score improved significantly from preoperatively to postoperatively: from 7.4 to 1.0 in group 1 and from 7.1 to 1.3 in group 2 (P < .0001 for both). Similarly, there was a significant improvement regarding the Constant score in both groups: from 51.7 to 86.0 in group 1 and from 49.4 to 87.2 in group 2 (P < .0001 for both). The between-group comparison showed no significant differences in preoperative or postoperative scores regarding both the VAS and Constant scores (Table 5).
Preoperative and Postoperative Pain and Function Scores a
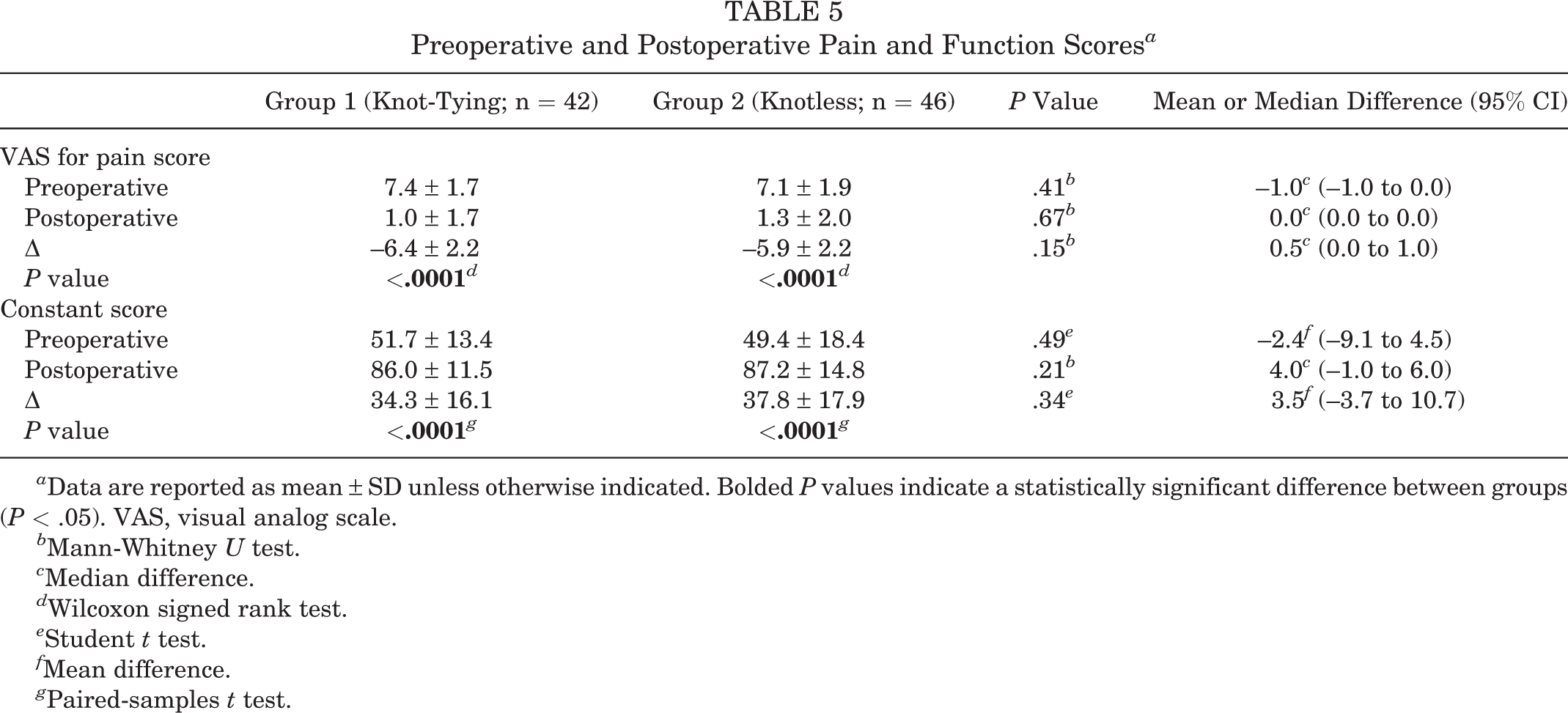
a Data are reported as mean ± SD unless otherwise indicated. Bolded P values indicate a statistically significant difference between groups (P < .05). VAS, visual analog scale.
b Mann-Whitney U test.
c Median difference.
d Wilcoxon signed rank test.
e Student t test.
f Mean difference.
g Paired-samples t test.
Complications
During the follow-up period, an early superficial postoperative infection was observed in 1 patient who underwent knot-tying SB RCR. Full recovery was obtained after the administration of oral antibiotics. Furthermore, 2 patients (1 in each group) developed postoperative frozen shoulder. These patients regained satisfactory shoulder ROM via rehabilitation at final follow-up.
Structural Outcomes
After assessing postoperative MRI data, successful repair and healing were observed in 34 of 42 patients in group 1; the retear rate was 19.0% (8/42). In group 2, successful healing was seen in 33 of 46 patients, indicating a retear rate of 28.3% (13/46). The retear rate was not significantly different between the groups.
The patients with retears were then evaluated for retear patterns. In group 1, of 8 patients with retears, 2 had type 1 retears, and 6 had type 2 retears. In group 2, of 13 patients with retears, 10 had type 1 retears, and 3 had type 2 retears. This difference in retear patterns between the groups was statistically significant (P = .03) (Table 6).
Retear Rates and Patterns on Postoperative Magnetic Resonance Imaging Scans a

a Data are reported as n (%). Bolded P value indicates a statistically significant difference between groups (P < .05). Dash indicates not applicable.
b Pearson chi-square test.
c Fisher exact test.
Discussion
The conventional SB RCR technique includes tying medial knots because the success of this fixation depends on the medial row and holding capacity of these sutures to the rotator cuff. However, several reports have raised the suspicion of an association of this technique with high retear rates, especially with type 2 repair failure. 4,32 Multiple factors that might be related to this condition have been reported. In a biomechanical study, it has been shown that strain at the medial suture site significantly increased with tied medial knots compared with knotless repair. 21 Trantalis et al 31 reported that “medial cuff failure” was associated with overtension between the tendon and suture at the medial row, overtightening of the medial knots, damage to the musculotendinous junction by passing the suture limbs through the muscle medial to the musculotendinous junction, and abrasion of the tendon caused by the passage of braided suture material. Cho et al 3 also proposed that passing the sutures medially through the musculotendinous junction might be related to strangulation and eventually necrosis of the tendon. Recently, vascularity of the rotator cuff has been considered a major factor in successful repair. Currently, we have little knowledge of the influence of SB RCR on intratendinous vascular inflow. A study with intraoperative blood flow measurements using Doppler flowmetry showed a significant intratendinous blood flow decrease with the use of knot-tying SB RCR after the insertion of lateral-row anchors. However, the effect of the knotless technique on vascular flow was not evaluated. 5 Further studies using different techniques are required to determine the implication for tendon healing.
In contrast to conventional knot-tying SB RCR, successful repair without undue tension on the tendon-suture junction at the medial row would be achieved via knotless SB RCR. 11,13 However, there are also several studies emphasizing the biomechanical advantages of medial knots. With knotless fixation, the tension of the construct would be distributed more laterally, which eventually would cause increased pull-out strength and loosening of lateral-row anchors, especially in patients with osteoporosis, and compromise tendon healing by decreasing the compression effect of the SB on the footprint. 15,17 It has also been reported that tying medial knots would improve the stability of the fixation site. 17 Moreover, Nassos et al 22 reported that knotted SB RCR had the best results for isolating the healing environment from synovial fluid, which could compromise tendon healing, compared with other techniques including knotless SB RCR.
Several studies have compared the clinical and radiologic outcomes of the 2 techniques; however, the literature still lacks high-level evidence. A recent systematic review showed that the incidence of retears ranged between 5.1% and 33.3% for knotless SB RCR and between 7.5% and 25% for knot-tying SB RCR. The authors stated that retear rates and patterns between the 2 techniques were not significantly different. 16 In a recent comparative study, Kim et al 14 reported comparable functional and pain outcomes between the 2 techniques. The retear rate was higher with the knotless SB RCR technique than the knot-tying technique (29.2% vs 16.3%, respectively); however, the difference was not significant. As the authors stated, the deficiency of a standard postoperative imaging protocol and incompleteness of preoperative imaging data might have influenced the final results. However, the results of this study were consistent with those of the present trial. In another study, Boyer et al 2 reported similar pain, ROM, and functional outcomes with both techniques. Regarding structural outcomes, compared with the knot-tying technique, the knotless SB RCR technique achieved a lower but insignificant retear rate (24.3% vs 17.1%, respectively). The authors stated that although there was not clear evidence, these findings could be explained by their use of suture tapes in knotless repair, which could provide better footprint compression and tension sharing.
Recently, Rhee et al 27 introduced an alternative knotless SB RCR technique using modified Mason-Allen stitches for medial-row fixation. According to the authors, this technique provided stronger tissue-holding capacity, a lower risk of strangulation, and a rip stop that prevented tendon pullout. Clinical outcomes of this technique were comparable to those of conventional knot-tying SB RCR. However, the retear rate was significantly lower with this modified knotless repair technique compared with the knot-tying technique (5.9% vs 18.6%, respectively). Moreover, although 72.7% of the retears in knot-tying SB RCR were type 2 failure, there were no type 2 retears in the knotless repair group. The findings of this study could be suggestive of the biomechanical limitations of the conventional knotless SB RCR technique that were mentioned above. Modification of the conventional knotless repair technique, which could provide more stable and stronger fixation, would result in better structural outcomes.
Type 2 repair failure can be related to poor shoulder function, pain, and impingement. 19 Moreover, revision surgery of type 2 retears might be technically challenging 1 because of the small amount of remaining tendon stock for repair. Therefore, the knot-tying SB RCR technique might result in serious clinical difficulties by causing strangulation of medial rotator cuff tissue, impairing vascular flow, and consequently causing necrosis of the rotator cuff and medial repair failure. For this reason, the application of a meticulous technique to reduce the type 2 failure rate plays an important role. In a recent study, Takeuchi et al 30 introduced a new knot-tying SB RCR technique: “arthroscopic medial knot-tying after suture-bridge lateral row rotator cuff repair.” In this technique, medial knots were tied after the insertion of lateral-row anchors and formation of the SB. The authors reported that with the use of this technique, lower stress concentration on the medial-row stitches could be achieved with better structural outcomes and lower type 2 repair failure rates. This technique showed a significant improvement in clinical outcomes, and the overall retear rate was 15.6%, of which 33.0% was type 2 failure. The findings of this study suggest that this technique could be related to lower type 2 retear rates; however, we believe that more data are needed to imply the superiority of this technique.
The results of the present study revealed that both knot-tying and knotless SB RCR techniques showed a significant improvement in clinical outcomes. Postoperative ROM, pain, and functional outcomes were comparable between the 2 techniques. However, contrary to our hypothesis, retear rates were higher in knotless SB RCR, but the difference was not significant. The results of this study indicate the importance of the biomechanical advantages of the knot-tying SB RCR technique despite the biological properties of a knotless construct. Another finding of this study was that the 2 techniques differed significantly regarding retear patterns. The medial (type 2) repair failure rate was predominantly higher with the knot-tying SB RCR technique, which was consistent with previous literature data. 18,27,28 Taking into account the great difficulty of revision repair of type 2 failure, a lower type 2 retear rate might be considered an advantage of the knotless technique, as it provides the preservation of tendon stock and positively affects the repair success of future revision procedures. We believe that the present trial points out important findings and greatly contributes to clinical decision making when deciding on a knot-tying versus knotless construct for SB RCR. However, future trials with larger populations are needed to support the findings of this study as definitive conclusions.
Limitations
The present study had several limitations. First, the power of this study could be questioned, and a type II error cannot be completely excluded because the results showed a rather smaller difference in retear rates between the 2 techniques compared with the data on which the sample size calculation was based. Second, the follow-up period was relatively short, and the findings of this study demonstrated the midterm outcomes of 2 repair techniques. Long-term results could have been different for both clinical and structural outcomes. Third, there was a considerable loss to follow-up rate (∼15%), which could have reduced the power of the study. Fourth, tear size and retraction were not considered as exclusion criteria. Although there was not a significant difference between the distribution of patients in the groups regarding preoperative tear size, massive tears might especially have affected retear rates. However, considering the difficulties of patient enrollment in a randomized prospective trial and to obtain results reflecting the general population, we included all sizes of tears. Fifth, the clinical assessment of patients during the follow-up period was performed by a single author (K.Ş.) who was not blinded to study data. This may have been associated with an evaluation bias. Yet, to our knowledge, this is the first randomized prospective clinical trial on this topic with a strict methodology, standardized follow-up, and standardized imaging protocol, and therefore, it makes a valuable contribution to the existing literature.
Conclusion
Arthroscopic SB RCR showed a prominent improvement in short-term to midterm clinical outcomes, regardless of the chosen technique for the medial row (knot-tying or knotless). Our results showed that there was no significant difference in retear rates between the 2 techniques. The findings of this study also suggest that the pattern of the retear was highly dependent on the technique and there was a high association between the knot-tying SB RCR technique and type 2 (medial) retears. However, these results should be interpreted with caution, and further research is needed to make definitive conclusions on this topic.
Footnotes
Final revision submitted November 18, 2020; accepted December 21, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Istanbul University.