
Abstract
Background:
Hip instability and postoperative laxity negatively affect patient outcomes after hip arthroscopy. With the hip capsule playing a substantial role in stability, unrepaired capsulotomies and decreased capsular thickness have both been demonstrated to contribute to increased hip distractibility on axial traction studies. While capsular violation increases distractibility, the role of capsular defect size is less understood.
Hypothesis/Purpose:
It was hypothesized that there would be a statistically significant association between hip capsule defect size on magnetic resonance arthrogram (MRA) and hip distraction. This study evaluates the relationship between capsular defect size on MRA and hip distractibility in revision hip arthroscopy.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review of a single-surgeon database of revision hip arthroscopy patients with capsular defect on preoperative MRA and available traction data was queried. Patients <18 years or a history of a previous ipsilateral hip surgery were excluded. Capsular defect was also measured on preoperative MRA (mm2), utilizing coronal and axial sequences. Axial traction was applied on a post-free traction table at intervals of 0 to 100 pounds of force, with distraction distance defined as the hip joint space.
Results:
Of 94 charts reviewed, 67 patients met the inclusion criteria. The mean age was 33.2 ± 9.6 years, 83.6% were women, the mean body mass index was 27 ± 6.2 kg/m2, and 39 (78%) patients had Beighton scores of <4. The mean distraction distance at 100 pounds of axial force was 8.3 ± 3.6 mm, the mean capsule defect size was 87.1 ± 77.5 mm2, with a mean length of 7.8 ± 4.6 mm, and a mean width of 10.3 ± 4.7 mm. Linear regression demonstrated no statistically significant relationship between overall distraction distance and the size (β = −0.002; R = 0.396; P = .773), length (β = −0.046; R = 0.398; P = .681), and width of the hip capsule defect (β = −0.040; R = 0.397; P = .695).
Conclusion:
No significant correlation was found between capsule defect size on MRA and hip distraction distance. Given that hip distractibility increases with capsular violation, we suspect that capsular disruption itself is a critical determinant of stability as opposed to the size of the defect.
Hip instability and postoperative hip laxity are of increasing interest given their established negative effects on patient outcomes after hip arthroscopy. 9 The hip capsule has been identified as an important contributor to overall hip stability, with capsular management after hip arthroscopic procedures undergoing increasing investigation.8,18,20,23 Previous research has established that disruption of the hip capsule through unrepaired capsulotomies and decreased hip capsule thickness contribute to increased ease of joint distraction with axial traction, which may manifest as clinical symptoms of hip instability.17,18,20,23 Patients who experience postoperative hip instability typically have lower postoperative satisfaction and are at a higher risk of needing revision surgery compared with those without.20,24,32
With regard to the size of capsular violation biomechanics, 1 study from Khair et al 12 found that increasing the size of the interportal capsular incision in cadaveric hips resulted in less force to distract the hip to 6 mm. 12 Another study from Weber et al 31 found similar results of increasing the size of interportal capsular incisions, resulting in decreased force required for distraction in cadaveric hips. However, Weber et al 31 found no difference in ease of distraction when the interporal was converted to a T-capsulotomy and when the T-capsulotomy was extended. While these studies suggest that physical violation of the hip capsule contributes to increased distractibility, which is supported by multiple studies looking at capsulotomy repair, this does not specifically address the association of hip distractibility and hip capsule defects.1,3,10,29 Furthermore, the association of capsular defect size and distractibility has not been investigated in the revision hip population.
This study aimed to evaluate the relationship between the size of hip capsule defects on magnetic resonance arthrography (MRA) and the distraction profile of the hip in response to axial traction on an examination under anesthesia before revision hip arthroscopy. We hypothesized that there would be a statistically significant association of hip capsule defect size with hip distraction distance on MRA.
Methods
Cohort Identification and Characterization
A retrospective review of a single-surgeon (S.K.A.), prospectively collected database of revision hip arthroscopy patients was performed from January 2019 through July 2021 following institutional review board (IRB) approval (IRB No. 00055341). The inclusion criteria were as follows: (1) identification of a capsule defect on preoperative imaging; (2) completion of the study traction protocol before arthroscopy; and (3) confirmation of a capsular defect intraoperatively. The exclusion criteria were as follows: (1) patients <18 years at the time of surgery and (2) a previous surgery on the operative hip. Variables collected from the electronic medical record included age at the time of surgery (in years), patient sex, Beighton score, and body mass index (BMI). 4 The clinical indication for revision surgery, per the treating surgeon at the time of revision, was also collected and reported. However, initial indications were not available in all cases, as not all index surgeries were performed at our institution. A combination of patient history, clinical examination, and radiographic review was used to determine whether the patient was primarily unstable, had a residual CAM lesion, or both.
Imaging Review
Standard radiographic parameters in the workup for revision hip arthroscopy patients were collected for our analysis. The lateral center edge angle (LCEA) to the acetabular sourcil and the alpha angle on lateral radiographs, either frog leg lateral or Dunn lateral, were measured and reported.2,33,34 Measurement of the capsule defect was performed on preoperative MRA studies (in mm2). Measurements were taken on coronal sequences (length) and axial sequences (width) and assessed in a straight-line fashion across the defect at its largest discrepancy in the imaging study, assuming the defect was largely rectangular. An example of this is provided in Figure 1.

Right hip MRA of a patient with a hip capsule defect. Measurements on the (A) axial and (B) coronal sequences are demonstrated with the black arrows. MRA, magnetic resonance arthrogram.
Traction Protocol
Patients underwent an intraoperative traction protocol before instrumentation for their revision procedure, but after initiation of general anesthesia without paralytics, which has been previously described in the literature.17,19,25 Patients were placed on a foam pad before distraction, and lower extremities were placed into traction boots attached to the traction table (Stryker Guardian Table; Stryker), with the leg in neutral position and 0° to 5° of Trendelenburg. The traction protocol consisted of axial traction intervals of 0 and 100 pounds on a post-free traction table, with anteroposterior fluoroscopic images of the hip obtained at these traction intervals. This was done before any venting or air arthrogram that may have been used to improve compartment access. Distraction distance was calculated as the difference in joint space on fluoroscopic images between these 2 intervals. Measurements in pixels were made in a straight-line fashion from the lateral edge of the acetabular sourcil to the femoral head, in addition to the diameter of the femoral head; preoperative radiographs were then utilized to measure the actual size of the femoral head diameter, and a simple ratio between these values was used to solve the overall distraction distance at these intervals.17,19,25 An example of this is provided in Figure 2.
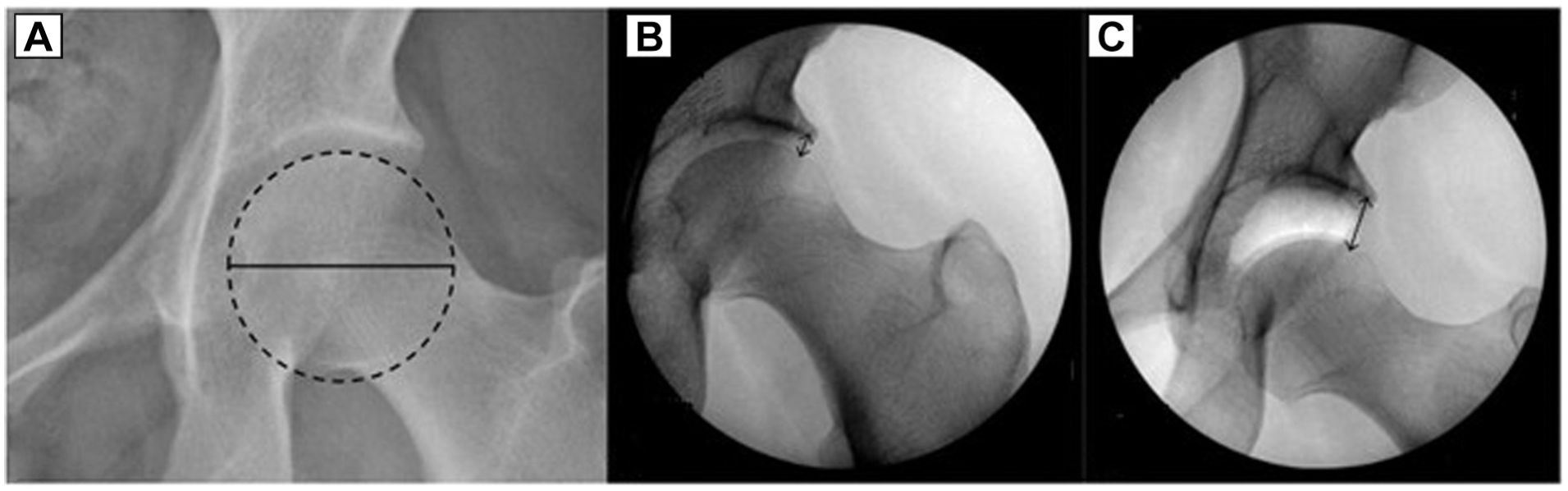
Representative images of calculating the distraction distance using preoperative radiographs and fluoroscopy. (A) The black circle demonstrates the assessment of the diameter of the femoral head. (B and C) The black arrows illustrate the measurement of the joint space on fluoroscopic images.
Statistical Analysis
Descriptive statistics were calculated for cohort demographic, imaging, and traction variables. Linear regression was performed with overall distraction distance as the independent variable. Variables included in the regression equation were age, sex, BMI, LCEA, and capsule defect size. As there is relatively limited literature on capsule defect size and hip distraction, a post hoc power analysis was performed to evaluate power in our study as opposed to an a priori power analysis. Intraclass correlation coefficients (ICCs) were determined for the measurement of the capsule defect area between 3 reviewers (A.K.M., A.Z.K., and C.D.R.H.) using a 2-way random-effects model with absolute agreement and 95% CIs. The senior author (S.K.A.) completed training for measurements. The reviewers consisted of a first-year orthopaedic surgery resident (A.K.M.), a third-year medical student (A.Z.K.), and a second-year medical student (C.D.R.H.). An excellent agreement was calculated 13 as an ICC value of >0.9. P < .05 was utilized to indicate statistical significance. Statistical analysis was performed using SPSS (Version 27; IBM) and G*Power Version 3.1.9.6 (Heinrich Heine Universität, Düsseldorf, GER).
Results
A total of 94 patients were chart reviewed. Twelve patients were excluded for missing MRA and/or incomplete traction protocol, 5 patients were <18 years, and 10 were excluded for previous surgery other than index hip arthroscopy, resulting in 67 patients meeting the inclusion criteria and demonstrating adequate power of the present study (Figure 3). The mean age of the study cohort was 33.2 ± 9.6 years, and 83.6% were women, and had a mean BMI score of 27 ± 6.2 kg/m2 (Table 1). A total of 39 (78%) patients had a Beighton score of <4 points. The mean LCEA was 29.4°± 5.8°, with the mean alpha angle of 43.9°± 9.2°. A total of 42 patients were indicated for revision surgery based on pure instability (62.7%), with the rest undergoing revision surgery for a combination of residual cam lesion and instability (37.3%).

A flow diagram demonstrating the application of inclusion and exclusion criteria for our cohort, with a final sample size of 67 patients included in the analysis. MRA, magnetic resonance arthrogram.
Overall Cohort Characteristics a

BMI, body mass index.
Reported for 50 patients.
The mean distraction distance was 8.3 ± 3.6 mm, while the mean capsule defect size was 87.1 ± 77.5 mm2, with a mean length of 7.8 ± 4.6 mm2 and a mean width of 10.3 ± 4.7 mm2. Linear regression demonstrated no statistically significant relationship between the overall distraction distance and the size (β = −0.002; R = 0.396; P = .773), length (β = −0.046; R = 0.398; P = .681), and width of the hip capsule defect (β = −0.040; R = 0.397; P = .695) (Table 2). Results of our post hoc power analysis are displayed in Table 3 and demonstrate appropriate power in our study, utilizing the Cohen calculation of the effect size, with a power of >0.90 based on our sample size. 6 ICCs demonstrated excellent agreement between reviewers at 0.997 (95% CI, 0.995-0.998).
Multivariable Linear Regression Analysis With Hip Distraction Distance as the Dependent Variable a

BMI, body mass index; LCEA, lateral center edge angle.
Results of Post hoc Power Analysis

Discussion
Our results demonstrate no statistically significant correlation with capsule defect size on MRA and overall distraction distance of the hip when subjected to axial traction before hip arthroscopy. Increasing hip distraction distance at a standardized force may serve as a surrogate for native hip instability. However, the size of the capsular defect does not appear to have a significant effect in this cohort. We hypothesized that any disruption of the capsule would weaken the suction seal between the femoral head and acetabulum, such that increasing the defect size would have a comparatively minimal effect, as demonstrated in Figure 4.

(A and C) Comparison of right hip capsule defects in 2 female patients on MRA, representing (A) a small (5.4 mm) hip capsule defect and (C) a large capsule defect (14.7 mm). (B and D) Fluoroscopic images from the study traction protocol at 100 pounds of axial traction for the (B) small capsule defect and the (D) large capsule defect. Both patients demonstrate similar overall distraction (~11 mm). MRA, magnetic resonance arthrogram.
Numerous biomechanical studies have demonstrated that surgically induced capsular violation results in increased ease of hip distraction and that subsequent capsular repair can restore resistance.3,11,16 Specifically, unrepaired T-type, interportal, and periportal capsulotomies increase ease of distraction. However, the effect of their resulting defect size in the unrepaired portal is controversial. Khair et al 12 found that increasing interportal incision size increased ease of distractibility. 12 Weber et al 31 also found that the size of interportal incision significantly increased ease of distractibility, but converting to a T-capsulotomy and extending the T-capsulotomy did not substantially change distractibility. This may be in part due to the direction in which the capsule is incised (parallel vs perpendicular to the fibers). However, it still highlights the complexity of hip stability and underscores the need for a more detailed description of the nuances of capsular defects. While our distraction data demonstrated that the defect size does not matter, the location of the defect may be important, given the nuances in the aforementioned studies. Future research should investigate whether the size of the anatomic defect specified by location in various surgical approaches results in different distraction data. However, we believe that the capsule defect produces a similar phenomenon to venting the hip capsule, with lowering the effect of the suction seal and increasing distractibility, which has been previously demonstrated in the literature. 19
Previous work has established that patients going for revision hip arthroscopic procedures demonstrate increased distraction under similar traction forces to native hips. 21 Mortensen et al 21 examined 47 patients undergoing revision hip arthroscopy and tested their resistance to axial traction at the time of revision surgery, with 85% of these patients being indicated for revision surgery at least in part due to clinical hip instability. They compared distractibility between the operative hip and the contralateral native hip and found that, at the time of revision surgery and before instrumentation, hips undergoing revision surgery demonstrated significantly increased distraction distance at 50, 75, and 100 lbs. While evaluation of capsule defects was not the primary focus of this previous work, all patients included were found to have capsule defects on arthroscopic evaluation. This study complements the findings of the present study and other earlier works, demonstrating that capsule defects contribute to hip laxity and capsule compromise in the revision setting after hip arthroscopy.
An additional study by McCormick et al, 15 looking at revision hip arthroscopy patients, found that 78% of patients had imaging evidence of capsular and iliofemoral irregularities. These findings, along with the present study indicating no significant differences in distractibility based on defect size, suggest that the integrity of repair may be more important than the size of the defect in the revision population, as it pertains to restoring resistance to axial distraction of the hip. This claim is substantiated by the body of the literature showing that capsular repair and reconstruction significantly increase the force required to distract compared with an unrepaired defect.7,18,26
Clinically, achieving ideal outcomes in patients undergoing revision hip arthroscopy can be challenging. While these patients typically achieve significant improvements compared with their preoperative state, their improvement is generally less than that found in the primary patient.14,32 Instability is a common reason for patients requiring revision arthroscopy, with 1 study 28 citing this as a significant reason for revision in 35% of patients, which may partly be due to a lack of capsular restoration at index surgery. While recent articles are showing improved patient-reported outcomes after capsular closure in revision arthroscopy, there has been no defined consensus on closure versus nonclosure in reducing the risk of needing revision hip arthroscopy.14,22,27 One study from Bolia et al 5 did find that capsular repair in hip arthroscopy had lower rates of conversion to total hip arthroplasty compared with an unrepaired cohort. However, they did not find a difference in future revision arthroscopy rates between an unrepaired versus a repaired capsular closure. We hypothesized that instability in patients may be partly due to capsular defects from unrepaired capsulotomies. Future studies should correlate defects and their size with clinical outcomes, both pre- and postsurgical intervention, to investigate this claim.
Limitations
This study is not without limitations. The surgeries were performed at a single institution by a single surgeon in a predominantly female population, which limits external validity. Measurements of the capsule defect can vary among reviewers; However, ICCs were >0.9 for this particular study. Moreover, this study only captures hip distraction in defects immediately before revision surgeries. Some patients may have postoperative defects that are small enough to heal over time or are asymptomatic and are not captured in this cohort. Furthermore, the location of the defect was not specified in this study and may play a role in the biomechanical properties of hip distraction. Moreover, it can be difficult to determine the overall characteristics of a capsule defect on preoperative imaging, such as a complete defect versus a more patulous nature of the capsule, which may influence distractibility in this cohort. While we measured the apparent capsular defect, scarring on the MRA may mimic an intact capsule and distort the true capsular deficiency. The amount of contrast injected into the joint and the positioning of the leg may also affect capsular measurements, as this was not standardized. During the traction examination, slight intraoperative variations may also affect distraction distance, such as friction with the operating table, degrees of Trendelenburg (0-5), patient weight, and calibration of the distraction table tensiometer. Patient-reported outcomes were also not routinely collected, therefore limiting the clinical implications of these findings. Furthermore, all patients in this study exhibited some degree of clinical instability, which may have affected the distraction distance and the results of this study. Moreover, the Beighton criteria were not included in the regression analysis due to an incomplete collection rate. Finally, labrum size and tears were not included in the regression analysis, as they may affect distractive stability, as per previous literature. 30
Conclusion
Our results indicate no significant correlation between capsule defect size on MRA and hip distraction distance. This suggests that the size of the capsule defect may not be the main factor in determining distractibility, which may represent overall hip stability in this patient population. Given that hip distractibility increases with capsular violation, we suspect that capsular disruption itself is a critical determinant of stability, as opposed to the size of the defect in revision hip arthroscopy patients. Future studies should evaluate the relationship between capsule defect size and patient-reported outcomes after arthroscopic hip surgery.
Footnotes
Final revision submitted April 24, 2025; accepted May 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.K.A. is a paid consultant for Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Utah (No. 00055341).