
Abstract
Background:
The most common surgical approaches in hip arthroscopy are interportal and T-capsulotomy. However, these methods may introduce capsular instability. Puncture capsulotomy preserves capsuloligamentous integrity by avoiding iatrogenic transection of the iliofemoral capsular ligament.
Purpose:
To present minimum 2-year functional outcomes for patients who underwent arthroscopic treatment for acetabular labral tears and concomitant femoroacetabular impingement using the puncture capsulotomy technique.
Study Design:
Case series; Level of evidence, 4.
Methods:
The authors conducted a retrospective review of prospectively collected data on patients who underwent arthroscopic acetabular labral tear treatment between December 2013 and May 2019. Included were patients aged ≥18 years who underwent hip arthroscopy by a single surgeon and completed a minimum of 2 years of patient-reported outcome measure (PROM) surveys. Intraoperatively, patients underwent hip arthroscopy via puncture capsulotomy to treat labral tears and any concomitant femoroacetabular impingement. Clinical outcome data consisted of PROMs.
Results:
A total of 163 hips were included; the mean patient follow-up was 30.4 months (range, 24-60 months; 95% CI, 28.5-32.3 months). Patients had a mean age of 37.9 years (range, 36.1-39.6 years), with a mean body mass index of 25.9 (range, 25.2-26.5). There were significant improvements in mean [95% CI] baseline to final follow-up scores for the 33-Item International Hip Outcome Tool (iHOT-33) (39.6 [36.8-42.4] vs 76.1 [72.7-79.6]), Hip Outcome Score–Activities of Daily Living (70.0 [67.0-73.0] vs 89.3 [87.3-91.3]), modified Harris Hip Score (60.1 [57.9-62.4] vs 84.9 [82.5-87.2]), and Hip Outcome Score–Sports Specific Subscale (41.8 [37.9-45.6] vs 75.7 [71.7-79.7]) (P < .001 for all). Additionally, the mean [95% CI] visual analog scale pain scores were noted to significantly improve throughout the duration of the postoperative period (from 6.3 [5.9-6.7] to 2.2 [1.8-2.6]; P < .001). There were no incidences of infection, avascular necrosis of the femoral head, dislocation/instability, or femoral neck fracture. At the 2-year follow-up, 81.0%, 62.0%, and 58.9% of hips achieved previously published clinically meaningful iHOT-33 thresholds for minimally clinically important difference, Patient Acceptable Symptom Score, and substantial clinical benefit, respectively.
Conclusion:
Puncture capsulotomy demonstrated significantly improved functional and clinically meaningful outcomes at a minimum 2-year follow-up, along with a minimal complication rate.
For patients with femoroacetabular impingement (FAI), hip arthroscopy has become the standard treatment because of a faster postoperative recovery, fewer complications, and reduced morbidity, with similar efficacy to open procedures. 6,15,32 With its increase in popularity since the early 1990s, 41 multiple arthroscopic techniques have been developed to enhance surgical field visualization, minimize iatrogenic hip instability, and optimize patient outcomes. 7,32 The most common surgical approaches in hip arthroscopy are interportal and T-capsulotomy. However, these techniques may introduce iatrogenic capsuloligamentous instability because of transection of the iliofemoral capsular ligament, 6,7,10,15,32 which has been implicated in dislocation, postoperative pain, microinstability, heterotopic ossification, and seroma formation. 7,13,22,40 Moreover, the iliofemoral ligament is an essential structure that stabilizes hip extension and resists anterior subluxation. 5 –7,10,15 Despite previous literature demonstrating sufficient outcomes with capsular closure, 10 there is a need for a surgical approach that avoids iatrogenic injury to the hip capsule.
To address this clinical demand, the senior author (S.D.M.) published an original technique, puncture capsulotomy, that involves preservation of the biomechanics of the hip joint. 7 This approach incorporates careful placement of multiple small portals in a manner that negates the necessity of an extended capsulotomy while still maximizing visualization. As a result, the iliofemoral ligament is spared, thus conserving capsular strength and stability. Overall, the theoretical advantages of this innovative approach include preservation of native hip biomechanics; elimination of anterior dislocation risk; minimal disruption of soft tissue, thereby decreasing the risk of heterotopic ossification; and avoidance of postoperative range of motion restrictions. 7
Because puncture capsulotomy is a novel approach, there are currently no data in the literature regarding patient outcomes. Thus, the primary aim of this study was to evaluate the midterm functional outcomes associated with the puncture capsulotomy technique in the treatment of labral tears, along with any osseous pathology resulting in FAI. Further, we aimed to assess the complications associated with the puncture capsulotomy. Given the minimally invasive nature of the approach, resulting in the conservation of hip biomechanics, we hypothesized that patients would demonstrate significantly improved functional outcomes with minimal complications at a minimum 2-year follow-up.
Methods
Study Design
The protocol for this study was approved by our institutional review board. This was a retrospective review of prospectively collected data on patients undergoing hip arthroscopy via puncture capsulotomy by a single surgeon (S.D.M.) between December 2013 and May 2019. The start date was determined as the time point when the senior author started exclusively using the puncture capsulotomy technique. The endpoint was chosen to ensure that all patients had a minimum of 2 years of clinical outcome data. All patients evaluated at the senior author’s clinic with hip pain received hip/pelvis radiographs and a detailed physical examination including provocative labral testing for evaluation of FAI. 20 Patients with positive findings on physical examination (ie, pain and/or limited range of motion with flexion, adduction, and internal rotation [FADIR] or flexion, abduction, and external rotation [FABER]) underwent magnetic resonance arthrography, diagnostic/therapeutic intra-articular anesthetic/corticosteroid injection, and a trial of a minimum of 3 months of nonoperative therapy, including core-strengthening physical therapy. Patients with persistent hip pain despite nonoperative therapy and evidence of labral tear with or without FAI were offered hip arthroscopy. Per indications previously reported in the literature, 31 labral debridement was performed if the labral tear was degenerative, hypoplastic, or isolated to a single plane involving <50% of the labrum. Labral repair was implemented if there was sufficient remaining healthy labral tissue for suture fixation or if the tear was complex with extension into the chondrolabral junction.
Patients were included in the study if they met the following criteria: age ≥18 years and completed a minimum of 2 years of patient-reported outcome measure (PROM) surveys postprocedure. As a result, this study evaluated 234 hips that underwent arthroscopy via puncture capsulotomy between December 2013 and May 2019. A total of 163 hips met the retrospective inclusion criteria and were subsequently included in the data analyses (Figure 1).

Flowchart detailing the patient-selection process. PROM, patient-reported outcome measure.
Data Collection
Baseline characteristics included age, sex, laterality, and body mass index (BMI). Preoperative imaging was utilized to identify osseous pathology (cam and/or pincer lesions), cartilage thinning, Tönnis grade, Tönnis angle, and center-edge angle and to classify the labral tear type: frayed/nondisplaced, discrete/linear, degenerative, or complex. Intraoperatively, cartilage degeneration was categorized via Outerbridge classification. 37 Additionally, the labral treatment (repair or debridement) and possible FAI decompression treatment (acetabuloplasty and/or femoroplasty) was recorded. Prospectively collected PROMs were the modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Specific Subscale (HOS–Sport), 33-Item International Hip Outcome Tool (iHOT-33), and visual analog scale (VAS) for pain. VAS pain scores were evaluated on a 0 (no pain) to 10 (worst possible pain) scale. The questionnaires were completed at baseline (preoperatively) and postoperatively at 3 months, 6 months, 12 months, and annually thereafter. In accordance with Nwachukwu et al, 36 clinically meaningful outcomes were assessed via the percentage of patients who achieved previously published threshold PROM scores for minimally clinically important difference (MCID), Patient Acceptable Symptom Score (PASS), and substantial clinical benefit (SCB). Postoperative radiographs at approximately 12 months were utilized to identify heterotopic ossification.
Abbreviated Surgical Technique From Puncture Capsulotomy Technical Note 7
With the anesthetized patient placed supine on a hip traction table, the nonoperative leg was positioned at 45° of abduction with the support of a perineal post. To allow for sufficient joint accessibility, the perineal post was utilized to position the operative hip into valgus. Then, under fluoroscopic guidance, the anterolateral portal was created 1 cm anterior to the greater trochanter at approximately 15° to 20° cephalad, parallel to the floor. Next, via arthroscopic visualization, the anterior portal was formed. As a guideline for determining the skin location for the anterior portal, a vertical line was drawn at the anterior superior iliac spine and a horizontal line was drawn at the level of the anterolateral portal. The location for the anterior portal is the intersection of these 2 lines. To confirm accurate portal placement, the scope was switched to the anterior portal for visualization of the original anterolateral portal, which could then be adjusted as needed to ensure access to both the central and the peripheral compartments, along with avoidance of labral insult. Then, at an equal distance from the anterior and anterolateral portals, the midanterior portal was placed distally. Last, at one-third the distance between the anterior superior iliac spine and the anterolateral portal, the Dienst portal was positioned, thus finalizing a quadrilateral arrangement with the other portals on the skin (Figure 2).

When all portals are placed correctly, a quadrilateral arrangement is formed on the skin. The midanterior portal is placed at a location distal to and equidistant from the anterior and anterolateral portals. The Dienst portal is placed one-third the distance between the anterior superior iliac spine and the anterolateral portal. This image depicts the right hip in the supine position. Image reproduced from Conaway and Martin 7 with permission from Elsevier.
To improve visualization of femoral cam lesions, a scope was inserted through the anterolateral portal and a switching stick was operated through the anterior portal to displace the capsule away from the femoral neck. If the cam lesion was situated more anteromedially or in the lateral gutter, an extra portal may have been made distal or proximal to the anterolateral portal, respectively, to enhance visualization. 7
Postoperative Rehabilitation
All patients analyzed in this study underwent a strict postoperative rehabilitation protocol. After operative treatment, patients were allowed immediate weightbearing as tolerated using a flat-footed gait with crutches for 6 weeks, along with once daily baby aspirin (81 mg) for 3 weeks. Furthermore, activities of daily living were not restricted during this time; however, patients were advised to avoid pivoting, active hip flexion greater than 90°, and tilting of their pelvis. Additionally, in contrast to the majority of traditional hip arthroscopy rehabilitation protocols that require bracing, 8 patients undergoing hip arthroscopy via puncture capsulotomy were not required to wear a brace during the postoperative recovery period. At 6 weeks postoperatively, patients could start using a stationary bike to slowly regain motion in a manner that limits inflammation of healing tissue. At 10 weeks, patients were allowed to swim or use an elliptical trainer with light resistance. At 4 months, strengthening exercises including hamstring curls and short-arc leg press with low weight and high reps were encouraged. At 6 months, patients were permitted to gradually resume impact-loading exercises as tolerated. 34
Statistical Analysis
Statistical analyses were performed using SPSS (Version 27; IBM). Categorical variables were analyzed with chi-square or Fisher exact tests, as appropriate, and continuous variables were compared with Student t tests or analysis of variance. Descriptive statistics are presented as means and 95% CIs, and all reported P values are 2-tailed, with the level of significance set at α = .05.
Results
The study population consisted of 84 (51.5%) female and 79 (48.5%) male hips with a mean age of 37.9 years (range, 18-64 years; 95% CI, 36.1-39.6 years). The mean BMI was 25.9 (range, 17.3-36.7; 95% CI, 25.2-26.5). Regarding laterality, there were 81 (49.7%) right hips and 82 (50.3%) left hips. Preoperative imaging demonstrated that 85 (52.1%) hips had a pincer pathology, while 47 (28.8%) hips had a combined pincer and cam lesion. Additionally, 81 (49.7%) hips had a discrete/linear labral tear, while 43 (26.4%) were frayed/nondisplaced, 23 (14.1%) were complex, and 11 (6.7%) were degenerative. Intraoperatively, 150 (92.0%) hips underwent labral repair, and 13 (8.0%) hips underwent labral debridement. For FAI, 82 (50.3%) hips underwent an acetabuloplasty, while 53 (32.5%) underwent femoroacetabuloplasty. Notably, the median Outerbridge grade was 3 (Table 1). Eleven (6.7%) patients underwent concomitant microfracture.
Baseline Characteristics, Preoperative Imaging, and Intraoperative Findings (N = 163 hips) a

a Data are reported as n (%) unless otherwise indicated. BMI, body mass index; CEA, center-edge angle; FAI, femoroacetabular impingement.
The mean final follow-up was 30.4 months (range, 24-60 months; 95% CI, 28.5-32.3 months). For all PROMs, the scores at all follow-up time points were significantly greater compared with baseline (P < .001 for all), with the exception of the 3-month HOS–Sport score (P = .410). Moreover, the VAS pain scores were noted to significantly improve throughout the duration of the postoperative period compared with baseline (P < .001 for all) (Table 2).
Prospectively Collected PROM Scores at Baseline and Follow-up a

a Boldface P values indicate a statistically significant difference compared with baseline (P < .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS–Sport, Hip Outcome Score–Sports Specific Subscale; iHOT-33, 33-Item International Hip Outcome Tool; mHHS, modified Harris Hip Score; PROM, patient-reported outcome measure; VAS, visual analog scale.
Regarding clinically meaningful outcomes, 36 132 (81.0%) hips achieved increases in iHOT-33 from baseline to 2-year follow-up that qualified as reaching MCID. For PASS and SCB, 101 (62.0%) and 96 (58.9%) hips achieved the threshold at the 2-year follow-up for iHOT-33, respectively (Table 3).
Clinically Meaningful Outcomes at 2-Year Follow-up for Puncture Capsulotomy a

a HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS–Sport, Hip Outcome Score–Sports Specific Subscale; iHOT-33, 33-Item International Hip Outcome Tool; MCID, minimally clinically important difference; mHHS, modified Harris Hip Score; PASS, Patient Acceptable Symptom Score; SCB, substantial clinical benefit.
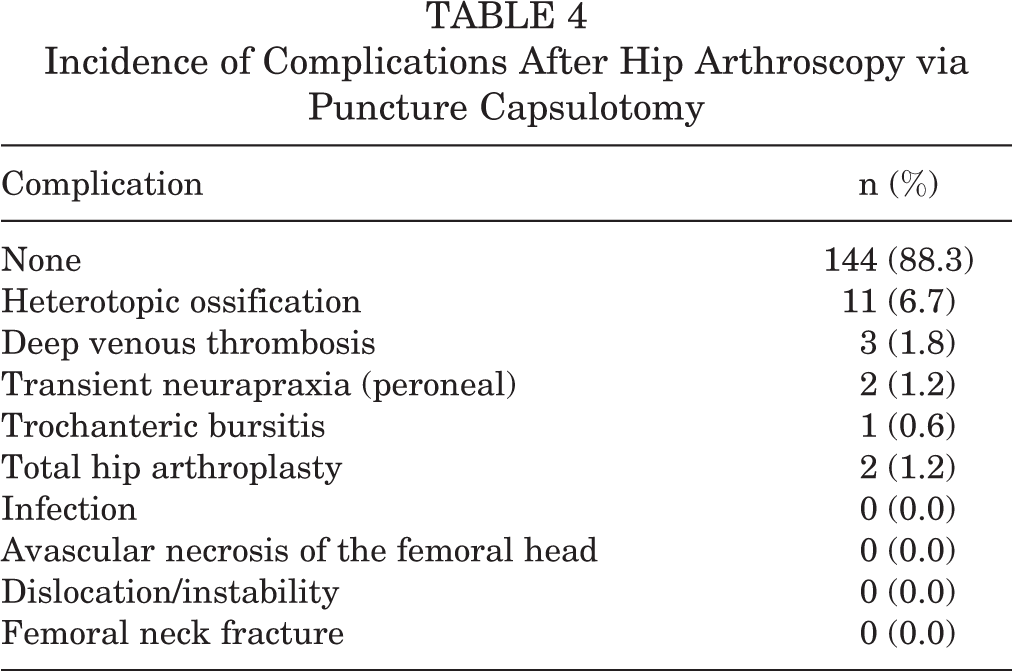
Through final follow-up, the incidences of postoperative complications after acetabular labral tear treatment via puncture capsulotomy are shown in Table 4. There were no complications in 144 (88.3%) patients. Two patients underwent total hip arthroplasty during their respective follow-up periods: A 60-year-old woman (Outerbridge grade 3) underwent labral repair and subsequent total hip arthroplasty 24 months later because of cartilage degeneration, and a 47-year-old woman (Outerbridge grade 4) underwent labral repair with acetabuloplasty and subsequent total hip arthroplasty 21 months later because of cartilage degeneration. There were no incidences of infection, avascular necrosis of the femoral head, dislocation/instability, or femoral neck fracture.
Incidence of Complications After Hip Arthroscopy via Puncture Capsulotomy
Discussion
This study evaluating the puncture capsulotomy technique for hip arthroscopy demonstrated favorable midterm functional outcomes at a mean of 30.4 months, along with a minimal complication rate. This significant improvement was seen across all prospectively collected PROMs (mHHS, HOS-ADL, HOS–Sport, iHOT-33, and VAS) and adds to the growing body of literature evaluating alternative techniques for hip arthroscopy. Moreover, the current study analyzing puncture capsulotomy compared favorably with other studies measuring functional outcomes in patients undergoing hip arthroscopy via interportal and T-capsulotomy. 9,18,29,30
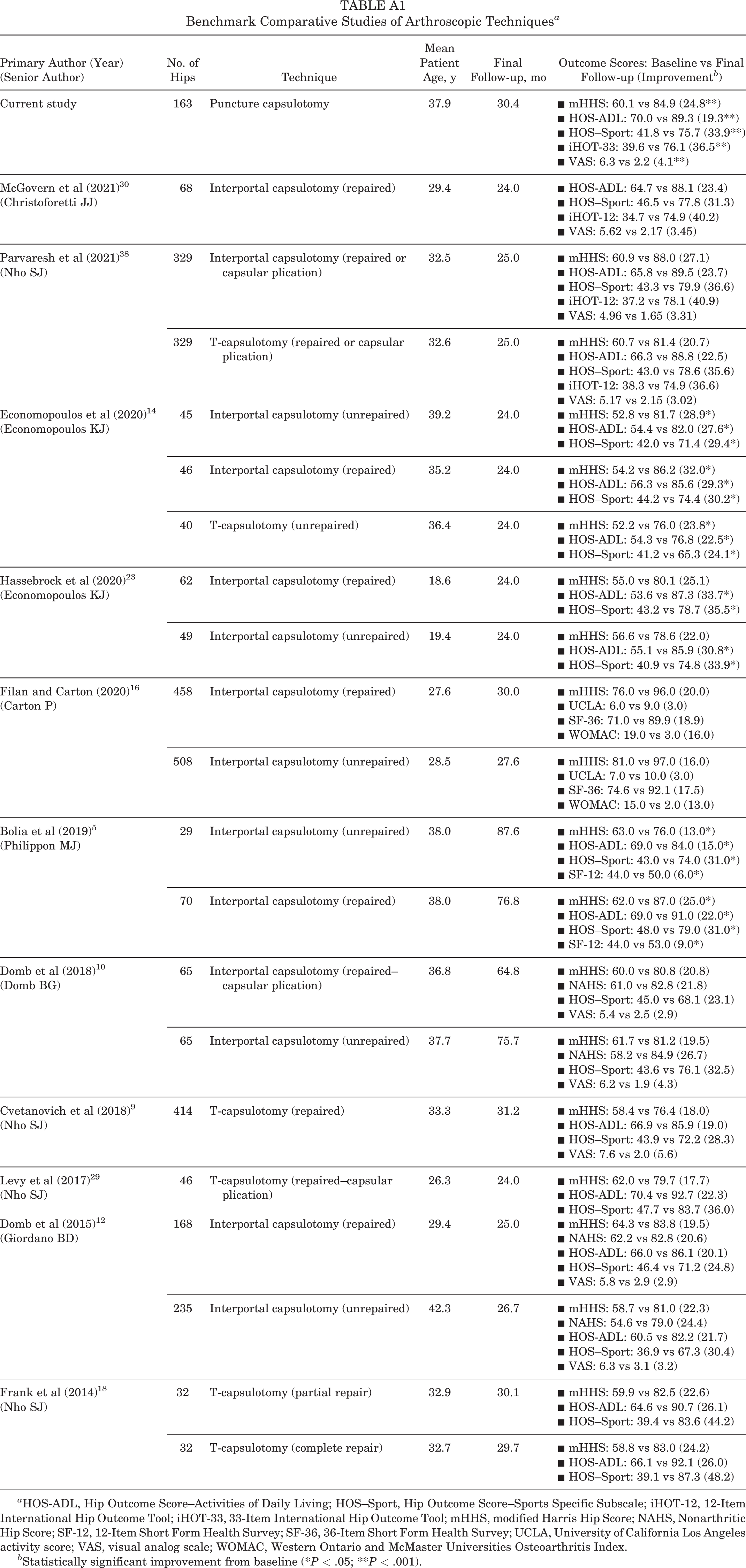
The 2-year improvements demonstrated by puncture capsulotomy can be benchmarked by those previously reported for other arthroscopic techniques # (Appendix Table A1). Notably, 100% of hips undergoing T-capsulotomy with capsular plication in the study published by Levy et al 29 were Tönnis grade 0, 89.1% of hips undergoing repaired T-capsulotomy in the study performed by Cvetanovich et al 9 were Tönnis grade 0, and 59% of patients in the study completed by McGovern et al 30 were Tönnis grade 0 for repaired interportal capsulotomy. In comparison, 69.3% of hips in this current study evaluating puncture capsulotomy were Tönnis grade 1 or worse. Overall, the midterm results of this study demonstrate evidence for the efficacy of puncture capsulotomy, an approach that minimizes violation of capsuloligamentous integrity through preservation of the iliofemoral ligament. 7
As previously mentioned, the primary methods of hip arthroscopy include interportal and T-capsulotomy. However, these surgical approaches may introduce capsular instability through transection of the iliofemoral ligament, the strongest capsular ligament and primary stabilizing structure for anterior translation. 6,7,13,15,24 In a systematic review, Duplantier et al 13 reported gross anterior dislocations for both interportal and T-capsulotomy, with or without capsular repair. Of clinical importance, dislocations can lead to osteonecrosis and arthritic progression requiring total hip arthroplasty. 13,17,43 Notably, there were no hip dislocations with the puncture capsulotomy technique. Other than macroinstability, the microinstability associated with capsulotomies has been proposed as a cause of postoperative pain. 6,19,40 Also, in addition to direct postoperative complications, the closure of large capsulotomies requires a conservative postoperative period that limits hip extension and external rotation to minimize the risk of anterior dislocation. 7,11,13 Moreover, these limitations have been associated with increased pain and stiffness. 7,11 While there is significant variability in postoperative rehabilitation protocols, other techniques advocate for early physical therapy to prevent soft tissue contractures. 21,26 However, early physical therapy may further tissue damage, slow tissue regeneration, and/or cause pain. 33 Importantly, puncture capsulotomy does not require the use of formal postoperative physical therapy, 34 thus avoiding these potential complications.
A technical note, 32 followed recently by 2-year functional outcomes, 6 proposed an analogous method to puncture capsulotomy termed “periportal capsulotomy.” Chambers et al 6 demonstrated improved clinical outcomes without postoperative instability, while avoiding capsular closure. From a technical standpoint, the periportal capsulotomy approach utilizes 2 portal entry sites that are dilated to 6 to 8 mm and 8 to 10 mm. Thus, while the periportal technique has the advantage of fewer capsular insults, a potential disadvantage is the substantially larger portal sites compared with puncture capsulotomy. 6,32 Additionally, given the anatomic constraints of the hip joint, surgical manipulation could result in stretching and further dilation of the portal sites. 24 As such, it is up to surgeons to balance the risks of portal size versus number. Regarding functional outcomes, Chambers et al showed significant increases in the mHHS, Hip Disability and Osteoarthritis Outcome Score (HOOS)–ADL, and HOOS–Sport of 21.1, 24.3, and 36.6, respectively, for periportal capsulotomy. In terms of pain relief, Chambers et al showed a significant improvement in VAS pain scores of 2.5. Clinically, the MCID rates for periportal capsulotomy were 81%, 88%, and 88% for HOS-ADL, HOS–Sport, and iHOT-12 (shortened version of the iHOT-33), respectively. 30
Given the heterogeneous calculation methods, there is not a consensus on MCID threshold reporting given the range of possible values. 25 However, because of similar inclusion criteria, the current study utilized thresholds previously established by Nwachukwu et al 36 for patients undergoing primary hip arthroscopy for FAI. In doing so, the puncture capsulotomy technique demonstrated favorable outcomes that exceeded the previously reported MCID, PASS, and SCB thresholds in a majority of study patients, thus emphasizing the potential clinical impact of this novel technique.
Consistent with previous studies that evaluated other arthroscopic techniques, 15,35 the most common complications associated with puncture capsulotomy were heterotopic ossification and transient neurapraxia. Most literature evaluating the incidence of heterotopic ossification after hip arthroscopy describe a 1% to 12% range of occurrence, with some reports as high as 46%. 1,28,39 Additionally, in patients who develop heterotopic ossification after hip arthroscopy, up to 24% to 26.5% are symptomatic and require resection. 2,4,28 For puncture capsulotomy, postoperative follow-up radiographic imaging identified heterotopic ossification in 6.7% of patients. Importantly, preservation of the capsule prevents disturbance of surrounding soft tissue and periarticular muscle, thus minimizing the risk of heterotopic ossification. 3,7
Limitations
While this is the first study to report midterm functional outcomes in patients undergoing the puncture capsulotomy technique and benefits from its large sample size, it is not without limitations. First, there was no comparison arm, and the comparative efficacy of puncture capsulotomy with other techniques was not directly assessed—prior data were provided only for benchmarking. Moreover, the calculation of clinically meaningful outcome thresholds (ie, MCID, PASS, and SCB) was extrapolated from previously published data, 36 which may not be valid for this study population despite similar inclusion criteria. 25 Also, based on the inclusion/exclusion criteria, the study sample represents only a portion of the overall population that underwent the technique procedure. Although this study did not report any hip dislocations, the puncture capsulotomy technique has not been biomechanically tested; thus, testing is needed to confirm its biomechanical advantage. Furthermore, as with hip arthroscopy in general and each new technique, there may be a learning curve. Puncture capsulotomy may be more challenging than other techniques, especially for addressing femoral lesions or patients with a higher BMI. Subject to its design and time span, there were heterogeneous radiographic views utilized, thus restricting the ability to assess performed femoroplasty. Finally, patients undergoing hip arthroscopy by the senior surgeon understood the novel technique and theoretical benefits, making them susceptible to bias. Overall, long-term evaluation of outcomes is warranted to completely encompass the benefits of puncture capsulotomy.
Conclusion
The puncture capsulotomy approach for hip arthroscopy demonstrated significantly improved functional outcomes at a minimum 2-year follow-up. Furthermore, regarding pain relief, VAS pain scores were noted to significantly improve throughout the duration of the postoperative period. Clinically, puncture capsulotomy illustrated favorable outcomes that exceeded previously published MCID, PASS, and SCB thresholds in a majority of patients. In summation, puncture capsulotomy addresses the clinical demand for an alternative arthroscopic approach that maintains capsuloligamentous integrity, provides appropriate osseous visualization, and generates improved functional outcomes compared with preoperative scores.
Footnotes
Notes
Final revision submitted July 30, 2022; accepted September 13, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support was received from the Conine Family Fund for Joint Preservation (to S.D.M.). W.K.C. has received education payments from Liberty Surgical. S.D.M. has received education payments from Kairos Surgical and honoraria from Allergan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Partners Healthcare (protocol No. 2013P000722/BWH).
APPENDIX
Benchmark Comparative Studies of Arthroscopic Techniques a
| Primary Author (Year) |
No. of Hips | Technique | Mean Patient Age, y | Final Follow-up, mo | Outcome Scores: Baseline vs Final Follow-up (Improvement b ) |
|---|---|---|---|---|---|
| Current study | 163 | Puncture capsulotomy | 37.9 | 30.4 |
▪ mHHS: 60.1 vs 84.9 (24.8**) ▪ HOS-ADL: 70.0 vs 89.3 (19.3**) ▪ HOS–Sport: 41.8 vs 75.7 (33.9**) ▪ iHOT-33: 39.6 vs 76.1 (36.5**) ▪ VAS: 6.3 vs 2.2 (4.1**) |
| McGovern et al (2021)
30
(Christoforetti JJ) |
68 | Interportal capsulotomy (repaired) | 29.4 | 24.0 |
▪ HOS-ADL: 64.7 vs 88.1 (23.4) ▪ HOS–Sport: 46.5 vs 77.8 (31.3) ▪ iHOT-12: 34.7 vs 74.9 (40.2) ▪ VAS: 5.62 vs 2.17 (3.45) |
| Parvaresh et al (2021)
38
(Nho SJ) |
329 | Interportal capsulotomy (repaired or capsular plication) | 32.5 | 25.0 |
▪ mHHS: 60.9 vs 88.0 (27.1) ▪ HOS-ADL: 65.8 vs 89.5 (23.7) ▪ HOS–Sport: 43.3 vs 79.9 (36.6) ▪ iHOT-12: 37.2 vs 78.1 (40.9) ▪ VAS: 4.96 vs 1.65 (3.31) |
| 329 | T-capsulotomy (repaired or capsular plication) | 32.6 | 25.0 |
▪ mHHS: 60.7 vs 81.4 (20.7) ▪ HOS-ADL: 66.3 vs 88.8 (22.5) ▪ HOS–Sport: 43.0 vs 78.6 (35.6) ▪ iHOT-12: 38.3 vs 74.9 (36.6) ▪ VAS: 5.17 vs 2.15 (3.02) |
|
| Economopoulos et al (2020)
14
(Economopoulos KJ) |
45 | Interportal capsulotomy (unrepaired) | 39.2 | 24.0 |
▪ mHHS: 52.8 vs 81.7 (28.9*) ▪ HOS-ADL: 54.4 vs 82.0 (27.6*) ▪ HOS–Sport: 42.0 vs 71.4 (29.4*) |
| 46 | Interportal capsulotomy (repaired) | 35.2 | 24.0 |
▪ mHHS: 54.2 vs 86.2 (32.0*) ▪ HOS-ADL: 56.3 vs 85.6 (29.3*) ▪ HOS–Sport: 44.2 vs 74.4 (30.2*) |
|
| 40 | T-capsulotomy (unrepaired) | 36.4 | 24.0 |
▪ mHHS: 52.2 vs 76.0 (23.8*) ▪ HOS-ADL: 54.3 vs 76.8 (22.5*) ▪ HOS–Sport: 41.2 vs 65.3 (24.1*) |
|
| Hassebrock et al (2020)
23
(Economopoulos KJ) |
62 | Interportal capsulotomy (repaired) | 18.6 | 24.0 |
▪ mHHS: 55.0 vs 80.1 (25.1) ▪ HOS-ADL: 53.6 vs 87.3 (33.7*) ▪ HOS–Sport: 43.2 vs 78.7 (35.5*) |
| 49 | Interportal capsulotomy (unrepaired) | 19.4 | 24.0 |
▪ mHHS: 56.6 vs 78.6 (22.0) ▪ HOS-ADL: 55.1 vs 85.9 (30.8*) ▪ HOS–Sport: 40.9 vs 74.8 (33.9*) |
|
| Filan and Carton (2020)
16
(Carton P) |
458 | Interportal capsulotomy (repaired) | 27.6 | 30.0 |
▪ mHHS: 76.0 vs 96.0 (20.0) ▪ UCLA: 6.0 vs 9.0 (3.0) ▪ SF-36: 71.0 vs 89.9 (18.9) ▪ WOMAC: 19.0 vs 3.0 (16.0) |
| 508 | Interportal capsulotomy (unrepaired) | 28.5 | 27.6 |
▪ mHHS: 81.0 vs 97.0 (16.0) ▪ UCLA: 7.0 vs 10.0 (3.0) ▪ SF-36: 74.6 vs 92.1 (17.5) ▪ WOMAC: 15.0 vs 2.0 (13.0) |
|
| Bolia et al (2019)
5
(Philippon MJ) |
29 | Interportal capsulotomy (unrepaired) | 38.0 | 87.6 |
▪ mHHS: 63.0 vs 76.0 (13.0*) ▪ HOS-ADL: 69.0 vs 84.0 (15.0*) ▪ HOS–Sport: 43.0 vs 74.0 (31.0*) ▪ SF-12: 44.0 vs 50.0 (6.0*) |
| 70 | Interportal capsulotomy (repaired) | 38.0 | 76.8 |
▪ mHHS: 62.0 vs 87.0 (25.0*) ▪ HOS-ADL: 69.0 vs 91.0 (22.0*) ▪ HOS–Sport: 48.0 vs 79.0 (31.0*) ▪ SF-12: 44.0 vs 53.0 (9.0*) |
|
| Domb et al (2018)
10
(Domb BG) |
65 | Interportal capsulotomy (repaired–capsular plication) | 36.8 | 64.8 |
▪ mHHS: 60.0 vs 80.8 (20.8) ▪ NAHS: 61.0 vs 82.8 (21.8) ▪ HOS–Sport: 45.0 vs 68.1 (23.1) ▪ VAS: 5.4 vs 2.5 (2.9) |
| 65 | Interportal capsulotomy (unrepaired) | 37.7 | 75.7 |
▪ mHHS: 61.7 vs 81.2 (19.5) ▪ NAHS: 58.2 vs 84.9 (26.7) ▪ HOS–Sport: 43.6 vs 76.1 (32.5) ▪ VAS: 6.2 vs 1.9 (4.3) |
|
| Cvetanovich et al (2018)
9
(Nho SJ) |
414 | T-capsulotomy (repaired) | 33.3 | 31.2 |
▪ mHHS: 58.4 vs 76.4 (18.0) ▪ HOS-ADL: 66.9 vs 85.9 (19.0) ▪ HOS–Sport: 43.9 vs 72.2 (28.3) ▪ VAS: 7.6 vs 2.0 (5.6) |
| Levy et al (2017)
29
(Nho SJ) |
46 | T-capsulotomy (repaired–capsular plication) | 26.3 | 24.0 |
▪ mHHS: 62.0 vs 79.7 (17.7) ▪ HOS-ADL: 70.4 vs 92.7 (22.3) ▪ HOS–Sport: 47.7 vs 83.7 (36.0) |
| Domb et al (2015)
12
(Giordano BD) |
168 | Interportal capsulotomy (repaired) | 29.4 | 25.0 |
▪ mHHS: 64.3 vs 83.8 (19.5) ▪ NAHS: 62.2 vs 82.8 (20.6) ▪ HOS-ADL: 66.0 vs 86.1 (20.1) ▪ HOS–Sport: 46.4 vs 71.2 (24.8) ▪ VAS: 5.8 vs 2.9 (2.9) |
| 235 | Interportal capsulotomy (unrepaired) | 42.3 | 26.7 |
▪ mHHS: 58.7 vs 81.0 (22.3) ▪ NAHS: 54.6 vs 79.0 (24.4) ▪ HOS-ADL: 60.5 vs 82.2 (21.7) ▪ HOS–Sport: 36.9 vs 67.3 (30.4) ▪ VAS: 6.3 vs 3.1 (3.2) |
|
| Frank et al (2014)
18
(Nho SJ) |
32 | T-capsulotomy (partial repair) | 32.9 | 30.1 |
▪ mHHS: 59.9 vs 82.5 (22.6) ▪ HOS-ADL: 64.6 vs 90.7 (26.1) ▪ HOS–Sport: 39.4 vs 83.6 (44.2) |
| 32 | T-capsulotomy (complete repair) | 32.7 | 29.7 |
▪ mHHS: 58.8 vs 83.0 (24.2) ▪ HOS-ADL: 66.1 vs 92.1 (26.0) ▪ HOS–Sport: 39.1 vs 87.3 (48.2) |
a HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS–Sport, Hip Outcome Score–Sports Specific Subscale; iHOT-12, 12-Item International Hip Outcome Tool; iHOT-33, 33-Item International Hip Outcome Tool; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; SF-12, 12-Item Short Form Health Survey; SF-36, 36-Item Short Form Health Survey; UCLA, University of California Los Angeles activity score; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Statistically significant improvement from baseline (*P < .05; **P < .001).