
Abstract
Background:
Subacromial impingement syndrome (SIS) is the most common and costly cause of shoulder pain. Recent guidelines emphasize reducing surgical interventions in favor of exercise-based care, but many patients experience suboptimal outcomes.
Purpose:
To investigate the effect of prescribing a large dose of resistance exercises in addition to nonoperative care compared with nonoperative care alone, in patients with long-standing SIS at 1-year follow-up, on the following outcomes: shoulder disability, health-related quality of life, number of days of sick leave, and surgery rates.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
This study analyzed the effect at 1 year after randomization in the Strengthening Exercises in Shoulder Impingement (SExSI) trial, a pragmatic, double-blinded randomized controlled trial with a 2-group parallel design. A total of 200 participants with long-standing SIS were randomized to 16 weeks of standard nonoperative care alone (control) or standard nonoperative care plus a large dose of progressive resistance exercises targeting the shoulder (intervention). Outcomes were assessed at 1 year and included shoulder disability (using the Shoulder Pain and Disability Index [SPADI]), health-related quality of life, days of sick leave due to the shoulder disorder (reported weekly through text messages), and surgery rates.
Results:
At 1 year, no significant differences were observed between groups for improvements in SPADI scores (mean difference, 4 [95% CI, –13 to 5]) or quality of life. We observed no difference in the odds of any sick leave (odds ratio, 0.84 [95% CI, 0.30-2.30]). For those reporting sick leave, the duration was 12% shorter in the intervention group (mean ratio, 0.88 [95% CI, 0.38-2.02]), but this did not constitute a significant difference. We also did not observe any difference in surgery rates between the control and intervention groups (12.1% vs 10.8%, respectively; risk difference, –1.3% [95% CI, –10.9% to 8.3%]).
Conclusion:
Adding a large dose of shoulder strengthening exercises to nonoperative care for 16 weeks did not significantly improve long-term outcomes in terms of shoulder disability, health-related quality of life, sick leave, or surgery rates at 1 year. This demonstrates that adding a structured, high-volume exercise program to exercise therapy may not provide further benefits in the long-term management of SIS.
Registration:
NCT02747251 (ClinicalTrials.gov)
Subacromial impingement syndrome (SIS; also referred to as rotator cuff syndrome, etc 37 ) is the most common cause of shoulder pain.22,35 SIS is often long-standing, 34 and many patients are referred to orthopaedic specialist care. In specialist care settings, patients most often have symptoms lasting >6 months.1,19,23 The typical patient is aged 40 to 60 years,1,19,23 and more than half are currently employed or self-employed,19,27 despite an impaired ability to work. 19 Sick leave due to SIS is a significant contributor to societal costs, 29 and the economic burden is substantial, with indirect costs from lost productivity outweighing direct medical expenses almost 2:1 for those aged <65 years. 29
Nonoperative care, including exercise therapy, 15 is considered the first-line treatment method for SIS,12,14,18,24,32 while subacromial decompression, until recently, was considered12,18,24,32 in cases in which nonoperative care had failed. There has been a strong push toward reducing the reliance on surgical interventions for SIS. 36 Recent clinical guidelines and research advocate for prioritizing nonoperative treatment options, including exercise therapy, to manage symptoms and improve function, aiming to minimize the need for surgery and its associated risks and costs. Importantly, nonoperative care only leads to success for about half of patients, 9 leaving a significant proportion with persistent symptoms. To address this gap, we conducted the Strengthening Exercises in Shoulder Impingement (SExSI) trial,6,7 aimed at enhancing the effectiveness of nonoperative care. This trial investigated whether adding a large dose of shoulder muscle strengthening exercises to usual nonoperative care could improve outcomes for patients with long-standing SIS. In the primary trial report, 7 we described the short-term (16 weeks) effectiveness of adding a large dose of shoulder strengthening exercises to usual nonoperative care, which was the primary aim and endpoint. We found no effect of the intervention at the end of treatment (4 months), which is the time point when surgery would traditionally be considered when nonoperative care fails. At 4 months, less than half of patients had reached an acceptable symptom state. The large proportion of patients with unacceptable symptoms at the end of treatment also indicates that many patients are still in a position in which they may be willing to consider surgery, which has traditionally been the solution to failed nonoperative care. As planned a priori, we collected data at 1-year follow-up, including sick leave and progression to surgery. With this study, we therefore report on the 1-year results of the effectiveness of the add-on intervention.
The purpose of this study was to investigate the effect of prescribing a large dose of resistance exercises in addition to nonoperative care compared with nonoperative care alone, in patients with long-standing SIS at 1-year follow-up, on the following outcomes: shoulder disability, health-related quality of life, number of days of sick leave, and surgery rates.
Methods
This study analyzed the effect at 1 year after randomization in the SExSI trial, a pragmatic, double-blinded randomized controlled trial with a 2-group parallel design.6,7,11 As planned a priori, we included number of sick days and surgery rates as 1-year outcomes, as sick days are the main contributor to the societal burden of SIS 29 and surgery is typically reserved for patients in whom nonoperative care fails. 13
A full trial protocol describing the methodology is available via open access, 6 and the primary analysis with end-of-treatment effectiveness outcomes 7 has been reported elsewhere. Ethical approval was obtained from the regional research ethics committee of the Capital Region of Denmark (No. H-16016763). We implemented blinded allocation and administered outcome assessments, and patients were not informed about the specific treatment method of the 2 groups or the study hypothesis.
Interventions
Participants in the control group (CG) received standard nonoperative care, which included referral to free-of-charge general rehabilitation comprising some form of exercise-based care at the group or individual level guided by a physical therapist at a municipal clinic under Danish Health Act §140. Corticosteroid injections were utilized at the provider's discretion, and the concomitant use of oral nonsteroidal anti-inflammatory drugs was permitted according to the patient's own discretion.
In addition to standard care, the intervention group (IG) underwent an exercise program. This program incorporated a large dose of progressive resistance exercises, focusing on long periods under tension with isometric holds and slow dynamic strengthening exercises. The exercises included low contraction velocity and an isometric component to reduce peak loads on the muscles and tendons, thereby making the exercises safer and less painful to facilitate patient adherence. The primary focus was on external rotation and abduction, targeting the supraspinatus and infraspinatus muscles. Instructions were provided at baseline and at follow-up intervals (2, 5, 10, and 16 weeks) to ensure proper execution and progression.6,7 As described in detail in the trial protocol, this methodology was developed based on the current literature regarding exercise physiology and shoulder biomechanics, with a focus on delivering a high volume of targeted resistance training safely and effectively. 6 In addition, patients were instructed on the use of a progression and regression algorithm to tailor resistance based on individual patient progress and pain responses (Appendix).6,11
Outcomes
Data at 1-year follow-up were collected through weekly text messages using SMS-Track (SMS-Track ApS) and an online questionnaire administered using REDCap (Vanderbilt University) and distributed via e-Boks (e-Boks Group), a secure email system utilized by public and private organizations to contact Danish citizens.
Shoulder Disability
Shoulder disability was quantified using the Danish version of the Shoulder Pain and Disability Index (SPADI).4,5,26 The SPADI consists of 13 items measuring pain (5 items) and disability (8 items). 26 Each item is scored from 0 to 10 (10 = worst); the pain and disability items are summed separately and, weighted equally, combined for a total score ranging from 0 to 100 (100 = worst). 5 The psychometric properties of the Danish SPADI have been investigated in a population comparable with the one included in the current study, showing good reliability (intraclass correlation coefficient = 0.88) and validity. 5 As a supplement, we report pain and disability separately, as suggested by Christensen et al, 4 adjusting SPADI pain subscores for differential item functioning by age and omitting items 8 and 12 from the SPADI function subscale.
Health-Related Quality of Life
Health-related quality of life was quantified using the EuroQol–5 Dimensions–3 Levels (EQ-5D-3L) questionnaire. The EQ-5D-3L consists of 2 parts; the first part is used to calculate summary index values reflecting the health state of the general population, 25 with a Danish value set,28,30 for both time tradeoff (EQ-5D TTO index) and the visual analog scale (EQ-5D VAS index). The second part is a visual analog scale of self-rated health (EQ-5D-VAS), with “best imaginable health” and “worst imaginable health” as external anchors, 31 and reflects the respondent's own assessment of his or her health state. 25
Sick Days Due to Shoulder Disorder
Sick days due to the shoulder disorder were quantified as the number of workdays that a participant had been unable to work because of the shoulder disorder. Data on sick days were collected through answers to automatically generated standardized SMS questions prospectively, as participants each week during the 1-year follow-up period (52 weeks) were asked to report the number of days lost from work because of their shoulder disorder.
In addition, the 1-year follow-up questionnaire prompted participants to report the number of workdays that they had been unable to work because of their shoulder disorder since entering the study. We used this response for participants who replied to <80% of the text messages (≤41 weeks). For patients replying to <80% of the text messages who also did not complete the 1-year follow-up questionnaire, we used available text message data. Data were considered missing for participants who did not complete the 1-year follow-up questionnaire and also did not reply to any text message.
Surgery
Data on surgery (yes/no) were collected through the 1-year follow-up questionnaire, as patients were prompted to report if they had undergone surgery in the affected shoulder since they were enrolled in the project. This information was confirmed by prospectively collected information during the trial and reported visually in the primary trial report's flow chart. 7
Statistical Analysis
Shoulder disability quantified using the Danish version of the SPADI is reported as the mean with standard deviation at baseline and 1 year as well as the change in scores; scores were compared between groups using a linear regression model and are reported as the mean difference with 95% confidence interval (CI). Health-related quality of life quantified using the EQ-5D TTO index, EQ-5D VAS index, and EQ-5D-VAS is reported as the mean with standard deviation at baseline and 1 year as well as the change in values; values were compared between groups using a linear regression model and are reported as the mean difference with 95% CI.
The number of sick days due to the shoulder disorder is reported as the median and interquartile range (IQR) and was compared between groups using a zero-inflated negative binomial model. 3 Briefly, this model assumes the study population to consist of 2 latent subpopulations: participants with a high probability of having no sick days and participants with a high probability of having ≥1 sick days. We report the estimated odds ratio of subpopulation membership and the estimated mean ratio, both with corresponding 95% CIs. Surgery rates are reported as the proportion and were compared between groups, described as the risk difference with 95% CI.
If >10% of outcomes were missing, multiple imputation by chained equations in which 10 complete data sets were generated by imputing values for the missing outcomes and estimates from 10 complete case analyses were then combined. 33 Imputed values were generated based on allocation, sex, age, height, weight, and other available outcomes (if any). To calculate the sample size, the original trial was powered to detect a 10-point difference in the SPADI score at 4 months with 95% power at the 5% significance level and included 100 participants in each group.
Results
Participants
A total of 200 participants were randomly assigned to either the IG or CG (Figure 1). At 1-year follow-up, days with sick leave due to the shoulder condition were available for 97% of participants (93 in IG, 100 in CG), although 57 participants replied to <80% of the text messages (≤41 weeks). Of these, 33 participants provided a response through the 1-year follow-up questionnaire, while 17 participants only provided some data through text messages (14 weeks, on average). Data on surgery since baseline were available for 84% of participants (80 in IG, 87 in CG), the SPADI score was available for 83% of participants (80 in IG, 86 in CG), and data on health-related quality of life were available for 82% of participants (77 in IG, 86 in CG). Baseline data for participants who completed 1-year follow-up are presented in Table 1.

Flow chart.
Participant Characteristics a

Data are presented as n (%) unless otherwise specified.
One missing answer.
Shoulder Disability and Health-Related Quality of Life
The total SPADI score decreased by 27 and 31 points in the CG and IG, respectively. The mean difference of 4 points (95% CI, –13 to 5) was not statistically significant (Table 2). For the EQ-5D TTO index, EQ-5D VAS index, and EQ-5D-VAS, the change in values was not statistically significantly different between groups (Table 2). For further details, see Table 3.
Mean Change Within Groups and Difference/Ratio Between Groups a
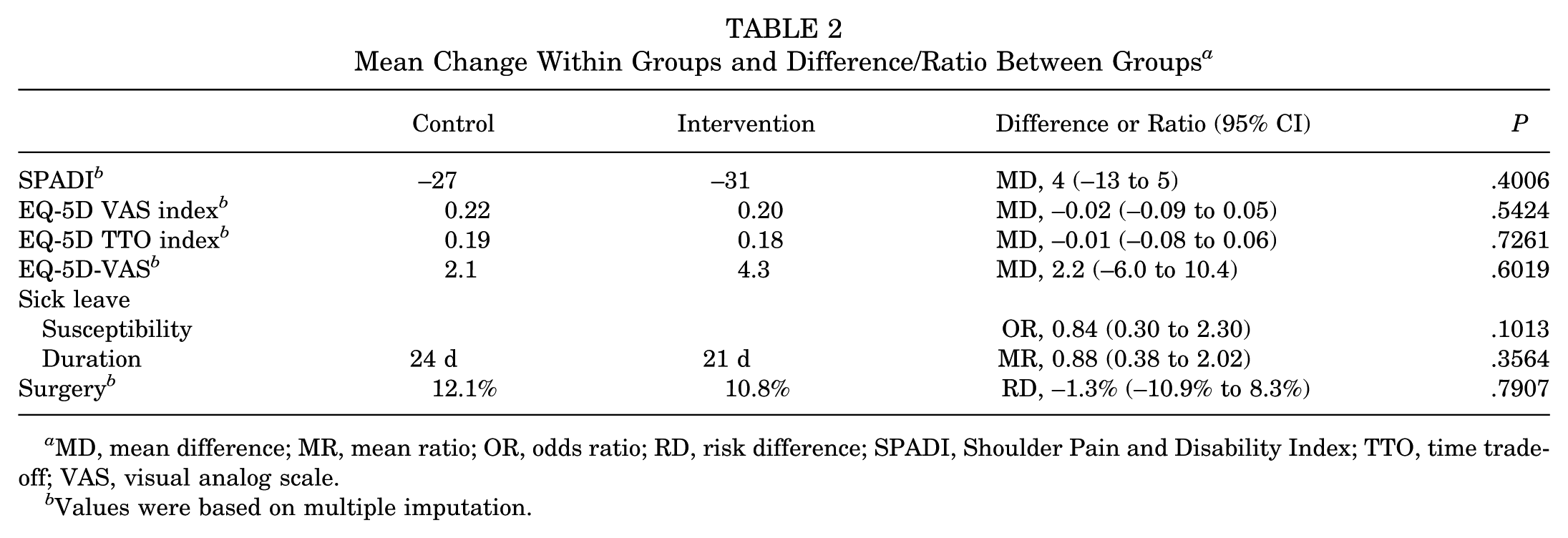
MD, mean difference; MR, mean ratio; OR, odds ratio; RD, risk difference; SPADI, Shoulder Pain and Disability Index; TTO, time tradeoff; VAS, visual analog scale.
Values were based on multiple imputation.
Shoulder Disability and Health-Related Quality of Life at Baseline and 1-Year Follow-up a

Data are presented as mean ± SD. SPADI, Shoulder Pain and Disability Index; TTO, time tradeoff; VAS, visual analog scale.
Sick Days and Surgery
There was no significant effect of the intervention on sick leave due to the shoulder condition. The probability of being susceptible to any sick leave favored the IG (odds ratio, 0.84 [95% CI, 0.30-2.30]) (Table 2), and regarding the duration of sick leave, the mean duration was 12% shorter in the IG group (mean ratio, 0.88 [95% CI, 0.38-2.02]) (Table 2).
The average number of sick days was 23 days across groups, with a median of 0 days (IQR, 0 to 8 days). For the CG, the average number of sick days was 24 days (IQR, 0 to 10.5 days), and for the IG, it was 22 days (IQR, 0 to 8 days) (Figure 2). The rates of surgery were 12.1% and 10.8% in the CG and IG, respectively; the difference was not statistically significant (Table 2).

Distribution of days of sick leave in the control and intervention groups.
Discussion
Our study found no significant improvements in shoulder disability (SPADI) and quality of life (EQ-5D-3L) at 1-year follow-up with the addition of a large dose of shoulder strengthening exercises to standard nonoperative care. These results are consistent with our short-term findings at 16 weeks. 7 Importantly, improvements in shoulder disability beyond the 16-week primary endpoint were minimal, with only a few additional points of improvement at 1-year follow-up. This aligns with the findings of Hopewell et al 17 in a large multicenter randomized controlled trial involving 708 participants with a rotator cuff disorder, with most of the improvement from baseline to 1 year already observed at 6-month follow-up.
In contrast, improvements in quality of life were more pronounced from the time between end of treatment and 1-year follow-up. Observed improvements from baseline to 16 weeks (from 0.04 to 0.06 points) were below the threshold of clinical importance for nonoperative care 2 (0.07-point improvement when the baseline value is 0.54). Baseline to 1-year improvements exceeded 0.2 points, suggesting that the relative persistence of symptoms does not necessarily translate to a similar stagnation in quality of life. A similar pattern is not evident for self-rated health, an outcome that is less responsive to changes. 38
The mean number of sick days due to the shoulder disorder from baseline to 1-year follow-up was 23 days. This high number underscores the significant societal and economic burdens of SIS. Ketola et al 20 reported similar findings, emphasizing that sick leave constitutes the primary societal cost associated with this condition. Similarly, Sørensen et al 29 found that shoulder pain leads to considerable work absenteeism, further emphasizing the need for effective management strategies. Our study did not show a significant reduction in sick days with the addition of high-dose resistance exercises, highlighting that exercise-based care may not adequately address work-related effects. Surgery does not seem to be a solution to this issue, as Ketola et al 20 found no significant difference between surgery and nonoperative care at 5 years. A slight reduction in sick days in the past 3 months was evident at 2 years after surgery, 20 but the initial high level of absenteeism related to undergoing surgery observed in previous studies 10 overshadows any potential and minor benefits of surgery. Over the full 5-year period, a nonsignificant tendency toward less sick leave was in favor of nonoperative care.
Our study did not find a significant reduction in surgery rates between the IG and CG. In contrast, Holmgren et al 16 reported that a higher dose of exercises significantly decreased the need for surgery compared with a very low dose of exercises. Importantly, the findings of Holmgren et al 16 have likely influenced standard care practices, and our study, comparing standard care with an even higher dose, reflects the optimized standard care already informed by such results. Additionally, our surgery rates were lower than the 25% reported by Beard et al 1 for patients assigned to “no treatment” and indicate that while increasing the dose of resistance exercises does not further reduce surgery rates, the optimized standard care already reduces the perceived need for surgical interventions beyond that of a no treatment approach.
While the relatively low surgery rates align with current recommendations, 36 the persistence of symptoms and proportion of refractory cases highlight the importance of continued efforts to improve care. Specifically, the magnitude of sick leave due to the shoulder disorder points to a specific focus on reducing work absenteeism related to shoulder pain to mitigate the economic burden associated with this condition. The relevance of such initiatives is further supported by qualitative evidence regarding the potential individual consequences of sick leave, 21 including the inactivity and isolation caused by sick leave resulting in an increased focus on pain, which in turn may lead to a depressed mood, stress, restlessness, and a tendency to become trapped in a negative sick role.
This study has notable strengths, including the use of a clinical population of consecutive patients, the weekly collection of sick leave data, and a robust follow-up rate of 82% to 97% across outcomes. Nonetheless, certain limitations must be acknowledged. The potential for measurement bias in the intention-to-treat estimates, particularly regarding sick leave data, cannot be excluded. Although we do not anticipate that group allocation influenced the response pattern (eg, the number of responses to text message questions), incomplete weekly text message responses may have led to an underestimation of sick leave. To address this, responses from 1-year follow-up were used when >20% of weekly responses were missing. Acknowledging that such an approach introduces the inherent challenge of recall in a 1-year follow-up questionnaire, this strategy was adopted to ensure a balanced representation of the sick leave burden while reducing the effect of missing data. Lastly, it is important to understand that the current trial is a pragmatic effectiveness trial designed to investigate if being prescribed a larger dose of exercises compared with usual care improves outcomes in real (clinical) life. 8
In conclusion, our study found that adding a large dose of shoulder strengthening exercises to nonoperative care for 16 weeks did not significantly improve outcomes in terms of shoulder disability, health-related quality of life, sick leave, or surgery rates at 1 year. These results highlight the need for further research to optimize nonoperative care strategies for SIS.
Footnotes
Appendix
Acknowledgements
The authors acknowledge all orthopaedic specialists and nurses at the Sports Orthopedic Research Center–Copenhagen, Department of Orthopedic Surgery, Copenhagen University Hospital–Amager and Hvidovre, for helping with the implementation of this trial.
Final revision submitted May 6, 2025; accepted May 20, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was provided by Fysioterapipraksisfonden and the Danish Rheumatism Association. T.B. has received speaking fees from Zimmer Biomet and Novartis. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Capital Region of Denmark (No. H-16016763).