
Abstract
Background:
Exercise therapy (ET) is the main and initial treatment modality for treating subacromial impingement syndrome (SIS). The isolated or combined use of platelet-rich plasma (PRP) applications in treating SIS is increasing and promising. A comparison was made on the effectiveness of ET alone and in combination with PRP on pain, functionality, and quality of life (QoL) in patients with SIS.
Purposes/Hypothesis:
The purposes of this study were to (1) investigate the possible positive effects of PRP injections combined with ET in treating SIS on pain, functionality, and QoL and (2) propose an alternative treatment protocol. It was hypothesized that the group receiving PRP applications in addition to ET would have a better QoL due to less pain and higher functionality 6 months after treatment.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
Volunteer patients diagnosed with SIS were included based on history and physical examination findings. All participants underwent magnetic resonance imaging to confirm the diagnosis and exclude possible accompanying pathologies. The patients were randomly divided into 2 groups. The first group underwent ET at home for 8 weeks (ET group), and the second group received the same ET program and an additional 2 PRP injections, at the beginning of the study and the end of the fourth week (PRP group). Patients were evaluated initially and 6 months after the treatment using the visual analog scale (VAS) for pain score, Constant-Murley Score (CMS), and the 36-Item Short Form Health Survey (SF-36). The Kolmogorov-Smirnov test determined the conformity of the data to a normal distribution, chi-square analysis was used to compare categorical variables between groups, and the Mann-Whitney U test was used to compare continuous and intergroup variables. Intragroup changes before and after treatment were evaluated with the Wilcoxon signed-rank test. P < .05 was considered statistically significant.
Results:
A total of 67 patients were initially enrolled; 5 were excluded and 6 were lost to follow-up (1 because of a COVID diagnosis). Thus, 56 patients (56 shoulders) were included for analysis. There were 28 patients in the ET group and 28 patients in the PRP group. There were no statistical differences between groups regarding participant characteristics and clinical evaluations before treatment. A statistically significant improvement was observed in pain (VAS subgroups), functionality (CMS subgroups), and QoL (SF-36 subgroups) evaluations of patients in both the ET and the PRP groups compared with before the treatment and 6 months after treatment (P < .05). At the 6-month posttreatment evaluation, the PRP group was statistically significantly superior to isolated ET in terms of VAS rest (P = .001) and night (P = .004) scores. This superiority was also in favor of the PRP group in flexion strength (P = .001), abduction strength (P = .046), and abduction degree (P = .041) measurements. There was no significant difference between ET and PRP groups regarding VAS activity, CMS, and SF-36 scores (P > .05) at 6 months.
Conclusion:
Our study showed that both isolated ET and additional PRP application to ET are effective methods in SIS treatment regarding pain, function, and QoL. Combining ET with PRP was superior in reducing pain and improving abduction degree and strength.
Keywords
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Biruni University (reference No. 2015-KAEK-59-22-04).
Subacromial impingement syndrome (SIS) is the most common shoulder disorder, accounting for 44% to 65% of all shoulder pain complaints. This disorder results from inflammation and degeneration of subacromial anatomic structures.2,10 The most common clinical complaints of SIS include pain in daily activities and in lying on the affected shoulder at night, difficulty in arm elevation and abduction, muscle spasms, and stiffness.2,11,22 Empty can, full can, painful arc, and impingement-specific shoulder tests are frequently used in clinical diagnosis. Subacromial injection tests and imaging methods are essential in differential diagnosis.2,11,16,22
Rest, nonsteroidal anti-inflammatory drugs (NSAIDs), exercise therapy (ET), subacromial corticosteroid (CS) injections, and physical therapeutic modalities (therapeutic ultrasound, electrotherapy, manual therapy, Kinesio taping, etc) are the main nonoperative treatment options.10,11,31,36 Arthroscopic or open subacromial decompression options may be considered in the presence of resistant symptoms to conservative treatment.10,11,22
Platelet-rich plasma (PRP) is a blood product obtained from centrifuged autologous blood with high platelet concentration and rich in growth factor.5,27 Wound healing mechanisms are supported by platelets, cytokines, bioactive mediators, and growth factors, and damaged tissues are repaired. 4 Several in vitro studies have reported that PRP positively contributes to the proliferation of human muscle, bone, and tendon cells and the soft tissue healing process.13,23 Although controversial for rotator cuff tears, the benefits of PRP in rotator cuff tendinopathy and subacromial pain syndrome, which describe the same clinical picture, are emphasized in the current literature.1,4,20,25,26,30,38
Our research aimed to investigate the possible additional benefits of PRP on pain, functionality, and quality of life (QoL) by comparing the combination of ET and PRP with isolated ET treatment and presenting an alternative combined treatment protocol to nonoperative treatments. We hypothesized that the group receiving PRP applications in addition to ET would have a better QoL due to less pain and higher functionality 6 months after treatment.
Methods
The local ethical committee approval was obtained from Biruni University/Clinical Research Ethical Committee. All participants signed the informed consent form. The 2 researchers, both experienced in shoulder surgery (N.Z.) and musculoskeletal rehabilitation (Y.Ş.), confirmed that all procedures applied to participants followed the relevant guidelines and regulations. Patients who applied to the clinic with a complaint of shoulder pain between February and September 2022 and were diagnosed with SIS by the investigative orthopaedic surgeon (N.Z.) according to predetermined valid criteria were included in the study. 24
Inclusion and Exclusion Criteria
Patients between the ages of 35 and 65 years who were diagnosed with SIS due to history, imaging, and physical examination findings and volunteered to participate in the study were included. All patients underwent magnetic resonance imaging to support the diagnosis and rule out possible additional pathologies.
Patients who had recent trauma and acute onset (<3 months) complaints, partial or complete rotator cuff tear, or frozen shoulder, ultimately normal magnetic resonance imaging findings, CS injection in the past 6 months, history of fracture/dislocation or surgery in the shoulder girdle, cervical radiculopathy, neuromuscular disease, cancer, unstable angina, systemic inflammatory joint disease, pregnancy history, or contraindications to exercise were excluded from the study.
All patients meeting the inclusion criteria were diagnosed at the outpatient clinic by the same physician (N.Z.). Sociodemographic data and contact information were recorded. The double-blind randomized controlled trial method was explained.
Randomization Process
The first evaluation of the participants was made by a physical therapist (Y.Ş.) before randomization. Participants were educated about ET and the treatment process. Groups were determined by a random selection of sealed, numbered envelopes without layers and blocks (sealed envelope randomization method) by a colleague blinded to the process. The participants were divided into the group that treated with isolated ET (ET group) and the group that additionally applied 2 doses of PRP (PRP group). ET group participants were discharged with a home therapy program (detailed in the ET protocol) that they would apply every day for 8 weeks. PRP group participants trained with the same ET program were injected with the first dose application by one of the authors (N.Z.) (detailed in the PRP protocol). PRP group participants were called to apply the second dose to repeat the same process. PRP preparation and applications were made in hospital facilities. 9 To standardize the analgesic use, participants were prescribed 600 mg of ibuprofen 2 times per day, which they could use for a few days if needed. Final evaluations were made at the end of the 6-month mark by an experienced assistant physical therapist who was blinded to the entire research process.
Outcome Measures
Pain severity was evaluated with the visual analog scale (VAS), shoulder functionality was evaluated with Constant-Murley Score (CMS), range of motion (ROM) was evaluated with a universal goniometer, muscle strength was evaluated with a handheld dynamometer, and QoL was evaluated with the 36-Item Short Form Health Survey (SF-36). All evaluations and measurements were made at the beginning of the study and repeated 6 months after the end of treatment.
Visual Analog Scale
Participants were asked to select the point where they felt their pain on a 10-cm horizontal line. A score of 0 meant no pain and 10 meant unbearable pain. Pain conditions were evaluated separately at night, during activity, and at rest. 28
Constant-Murley Score
This scoring system evaluated shoulder functionality based on objective and subjective data. Pain consisted of activities of daily living, movement, and strength parameters. It was evaluated out of 100 points in total. Increasing scores indicated improvement in the patient’s clinical condition. The reliability and validity of the Turkish version of the CMS have been established. 8
Universal Goniometer
Goniometric measurement is a method frequently used in the clinical evaluation of joint ROM. In addition to ROM, it was used in this study to determine the functional capacity, decide on the treatment program, and determine the treatment's effectiveness.
Handheld Dynamometer
Compared with isokinetic devices, we considered this a more valid method for measuring muscle strength due to its advantages such as cost, portability, and ease of application.
36-Item Short Form Health Survey
This survey consisted of 36 questions and 8 subdimensions (physical and social functionality, role limitation [physical and emotional], vitality, pain, general and mental health). Each subdimension in the scale provided a score between 0 and 100. Increasing scores on the scale indicated increased health-related QoL. 39
Treatment Protocols
An isolated home exercise program was applied to the first group (ET), and 2 doses of PRP were applied to the second group (PRP) in addition to the same program. Home exercises were taught to both groups by an experienced physical therapist (Y.Ş.). The exercises were performed for 8 weeks, ≥5 times a week, and 3 sets daily, with 8 to 10 repetitions of each movement. An exercise diary was prepared so that all participants could follow their protocol.
Patients were called by the physical therapist by telephone to inquire about their exercise practices and answer questions about the ET. Patients were followed up to keep regular records in the exercise diary. Weekly call were made during the 8 weeks of ET.
ET Protocol
Wand Exercise
Wand exercises were applied to increase the normal ROM of the joint. Exercises were performed in the directions of shoulder flexion, abduction, and internal-external rotation. The patient used objects such as a round stick, walking stick, and towel as aids during the exercise.
Shoulder Flexion Exercise
The patient held a long stick with both hands at shoulder width and tried to raise one arm upward with the help of the healthy arm.
Shoulder Abduction Exercise
The patient tried to lift the stick sideways and upward by holding the upper end of a long stick with one arm and the lower end with the other arm.
Shoulder External Rotation Exercise
The patient's elbows were in 90° of flexion, and the arm was adjacent to the trunk. Holding the stick, the stick was moved outward without moving the arm from the body.
Shoulder Internal Rotation Exercise
The patient's elbows were in 90° of flexion, and the arm was adjacent to the trunk. Holding the stick, the stick was moved inward without moving the arm from the body.
Pendulum (Codman) Exercise
These exercises were performed by turning the arm back and forth, to the sides, clockwise, and counterclockwise, with the waist flexed at 90°, while resting on the contralateral/uninjured hand.
Capsule Stretching
Auto stretching was applied to the posterior capsule, pectoralis minor, and upper trapezial muscles. The stretching intensity was within the pain limit, the stretching time was 30 seconds, repeated 3 times, and the resting time between stretches was 30 seconds.
Isometric Shoulder Exercise
Isometric exercises were given in the direction of shoulder extension, abduction, and internal-external rotation. The patient was asked to maintain the muscle contraction created without movement in the relevant muscle groups in the appropriate directions for 5 to 10 seconds without holding one's breath against the resistance. A total of 8 to 10 repetitions were performed for movements in all directions.
PRP Protocol
Ten milliliters of venous blood was collected from each patient using a syringe containing 2.5 mL of anticoagulant citrate dextrose solution. The collected blood was transferred to the PRP tube and centrifuged at 3000 rpm for 8 minutes, and the 5- to 6-mL PRP remaining at the top of the tube and the entire buffer coat was collected with a spinal needle without air contact. Leukocyte-rich PRP was applied to the subacromial space, which is compatible with the posterior arthroscopy portal (inferior to the acromial posterolateral bone prominence, targeting the subacromial space from the endpoint of the posterior fibers of the deltoid muscle). No buffering or activating agents were used for PRP. PRP was applied before the first session and again 4 weeks later. Exercises were started 3 days after the PRP application. All patients who underwent PRP were informed by the physician (N.Z.) of the possible complications of the injection, and routine secondary controls were not performed after the injection. Self-limiting minor complications such as pain at the injection site, localized swelling, and increased temperature were noted in 3 patients. No major complications occurred.
Statistical Analysis
The statistical program SPSS Version 21.0 (IBM Corp) was used to analyze the data. Frequency, mean, standard deviation, and percentage values were analyzed and evaluated within the scope of descriptive statistics. Before the statistical analysis, the compatibility of the data with the normal distribution was evaluated with the Kolmogorov-Smirnov test. Chi-square analysis was used to compare categorical variables from the demographic characteristics of the groups, and the Mann-Whitney U test was used to compare continuous variables. Intragroup changes before and after treatment were evaluated using the Wilcoxon signed-rank test. Changes between groups were evaluated with the Mann-Whitney U test. P < .05 was considered statistically significant in all analyses.
Sample Size
The sample size was calculated based on VAS, as we primarily aimed to improve the pain scores of our patients and then increase their shoulder function and improve their QoL. The number of our volunteers was calculated with the G*Power (Universität Düsseldorf) sample size calculator. In a 95% CI, when the values of the first group were taken as (mean ± SD) 7.3 ± 0.6 and the values of the second group as 6.9 ± 0.5 using the initial and final pain scores according to the VAS, to determine the 80% power and .05 significance level, we found that ≥25 volunteers should be included in each group. 33
Results
There were initially 67 patients (67 shoulders) enrolled in the study. Five patients did not meet the inclusion criteria and 6 were lost to follow-up (Figure 1). This left 56 (16 male, 40 female) patients with a mean age of 46.82 ± 10.33 years who participated in the study. Patients were randomized into 2 groups of 28, each with a unilateral shoulder. No differences were observed between the groups in terms of sex, age, and disease duration before treatment (Table 1). There was no statistically significant difference between the groups in terms of pretreatment pain (VAS), functionality (CMS), and QoL (SF-36) measurements and evaluations (P > .05).
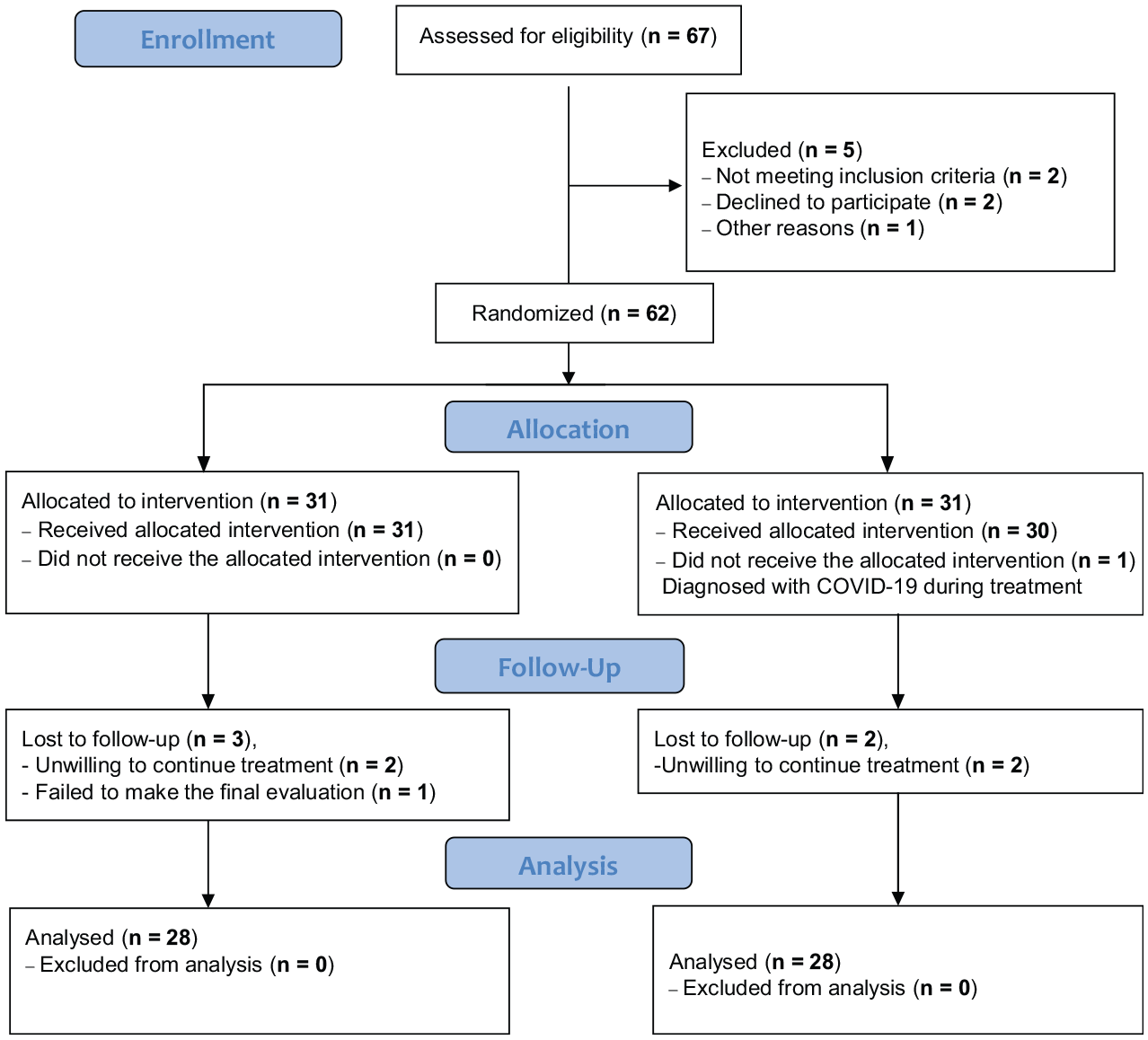
CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Characteristics of Participants a

Data are presented as mean ± SD unless otherwise indicated. ET, exercise therapy; PRP, platelet-rich plasma.
Mann-Whitney U test; P < .05.
The comparisons between the groups in terms of VAS subparameters before and after treatment showed that there was a statistically significant difference in favor of the PRP group in VAS rest and VAS night scores (P < .05), and there was no significant difference in VAS activity (P > .05) (Table 2). There was no difference in the CMS and SF-36 evaluations of the groups before and after treatment. Flexion and abduction muscle strength and abduction range were in favor of the PRP group when the groups were compared in terms of joint ROM and muscle strength before and after treatment. However, there was no difference in terms of internal rotation range and strength, external rotation range and strength, and flexion range. There was a significant difference in all parameters evaluated in both groups in intragroup changes before and after treatment (P < .05). Between-group comparisons are shown in Table 3.
Treatment Comparison in Terms of Pain Scores a

Data are presented as mean ± SD. ET, exercise therapy; PRP, platelet-rich plasma; VAS, visual analog scale. Bold characters indicate statistically significant values.
Mann-Whitney U test; P < .05.
Wilcoxon signed-rank test; P < .05.
Comparison in Terms of Quality of Life, Muscle Strength, Range of Motion, and Shoulder Function Scores a

Data are presented as mean ± SD. Bold characters indicate statistically significant values. CMS, Constant-Murley Score; E, energy; ERD, emotional role difficulty; ET, exercise therapy; GH, general health; MH, mental health; P, pain; PF, physical function; PRD, physical role difficulty; PRP, platelet-rich plasma; SAMS, shoulder abductor muscle strength; SAROM, shoulder abduction range of motion; SERMS, shoulder external rotation muscle strength; SERROM, shoulder external rotation range of motion; SF, social functioning; SF-36, 36-Item Short Form Health Survey; SFMS, shoulder flexor muscle strength; SFROM, shoulder flexion range of motion; SIRMS, shoulder internal rotator muscle strength; SIRROM, shoulder internal rotation range of motion.
Mann-Whitney U test; P < .05.
While minor complications such as mild local temperature increase, moderate swelling, and tenderness were reported in 3 PRP group participants (10.7% of participants and 5.35% of PRP applications), local or systemic major complications such as fever and weakness, septic arthritis, or hemarthrosis were not observed. Minor complications consisting of localized swelling and increased temperature complaints were resolved by pausing the exercise program for a few days and applying an ice pack.
Discussion
The major finding of our study showed that both isolated ET and PRP application in addition to ET were effective methods in the treatment of SIS in terms of pain, function, and QoL (P < .05). Additionally, combining ET with 2 additional doses of PRP was significantly superior in reducing resting pain and night pain (VAS rest, P = .001; VAS night, P = .004), as well as in increasing abduction and forward flexion (shoulder abductor muscle strength, P = .046; shoulder flexor muscle strength, P = .001) muscle strength and degree of abduction (shoulder abduction ROM; P = .041). Another important emphasis of our study is that it offered an alternative protocol by showing that PRP treatment and exercise treatments can be combined effectively and safely.
Supporting the current literature, ET is an effective method in the nonoperative treatment of SIS in terms of reducing pain as well as increasing functionality and QoL.12,18,21,34,36 The benefits of PRP in patients with SIS have also been shown in the literature.13,23,25,27,32,33 NSAIDs, physical therapy, ET, elastic therapeutic tape, manual therapy, ultrasound therapy, and subacromial CS injections are some of the nonoperative treatment options. § In the absence of concomitant major pathologies, 70% to 90% of patient complaints can be treated with 3 to 6 months of conservative multimodal treatments.10,11,21,36 PRP can provide good pain relief and functional results as well as a positive effect on the QoL in people presenting with common shoulder diseases.5,42,43 There are conflicting studies in the literature on the effectiveness of PRP applications in patients diagnosed with SIS.4,5,25,27,33,35 Therefore, we applied ET with proven efficacy in SIS to patients in both groups.21,22,31,36 We compared the groups at 6 months to evaluate the effects of 2 sessions of PRP application. Whether or not PRP applications are added, ET is effective on pain, ROM, muscle strength, and QoL. However, PRP application is significantly superior, especially in rest and night pain, which is one of the first reasons for patients to apply it. In addition, although PRP is not superior to isolated ET on QoL, it is advantageous in increasing both flexion and abduction strength and abduction ROM.
A recent systematic review and meta-analysis study assessing optimal treatment of SIS emphasized that physical therapy combined with subacromial CS injection should be the primary treatment but recommended acromioplasty in cases where conservative treatment does not benefit. 21 It is an important systematic review that recommends combining physical therapy and injection, similar to the protocol we suggested in our study. Differently, we showed the effectiveness of PRP application instead of CS injection. Although CS injection is included in our treatment portfolio as an inexpensive and effective treatment option, it is associated with various complications. These are mainly tendon damage, nerve atrophy, hypopigmentation, hyperglycemia, and blood pressure irregularity, which can be observed in the weeks after the application.6,37,44 Systemic adverse effects are very rare and mostly associated with prolonged and high-dose steroid administration. 41 PRP applications have the effect of protecting tenocytes against senescence caused by CSs. 42 The biggest disadvantage of PRP is the cost, which varies depending on the coverage of the country's health system and the individual's insurance. 9 Infection, bleeding, swelling, and soft tissue damage are common side effects of all injection applications.41,42,44 A total of 56 blind subacromial injections were made to 28 patients in the PRP group, 2 times each. Minor complications were reported in 10.7% of the patients and 5.36% of the applications, but no major complications were observed. Local soft tissue swelling and mild temperature increase were reported by 3 patients after injection. Self-limiting complaints were resolved by interrupting the exercise program for 2 to 3 days and applying ice packs.
Apart from these differences, PRP also varies according to its leukocyte content. Pure platelet, leukocyte-rich, and poor PRP types have been defined, and various studies have reported the superiority or indifference of one of them.11,24 We applied leukocyte-rich PRP to all participants.
A systematic review 31 published in 2015 recommended conservative treatment as the first choice in the treatment of early-stage symptomatic SIS, both because of its low cost and because of the absence of complications associated with surgery. 14
In a study with a similar concept that compared CS and PRP treatments applied to patients with SIS, PRP was recommended because it is safer even though their efficacy is similar. 6 Unlike our study, patients who received a single dose of PRP were compared with those who received a single dose of CS. Although CS seemed to be more effective at 1 and 3 months, the results were similar at 6 months. The important problem in the studies related to PRP is the lack of an application standard, which is mentioned in the Strengths and Limitations section. 7
Multiple and single PRP injections have been performed in various studies. For instance, Nejati et al 25 administered 2 PRP injections 1 month apart, Rha et al 29 made 2 PRP injections 4 weeks apart, and Saurav et al 32 and Say et al 33 administered a single injection of PRP. The volumes of PRP injected in the studies also ranged from 2 to 6 mL. The heterogeneity of PRP products has been emphasized. 15 Feltri et al 15 reported differences regarding the number of applications, application interval, applied product volume, use, and types of activating agents. Variables such as the preferred local anesthetic (LA) type, amount, and application portal can also be counted. 32
In the meta-analysis study 5 comparing PRP treatment with various treatments (ET, CS injection, etc) in the conservative treatment of SIS, it is stated that PRP treatment is maximally effective in 6 to 7 months, and our study also supports the current literature in terms of comparing the results at 6 months and emphasizing the superiority of PRP injection. 5
It has been shown that the administration of 3 consecutive doses of PRP to patients with SIS has positive effects not only on pain and functionality but also on daily activities. 35 Our protocol consisted of 2 doses of PRP, at the beginning (day 0) and middle (day 28) of ET. Blind randomized controlled studies with large series may answer the ideal application number and interval. In addition, patients’ compliance with and documentation of ET should be emphasized for the effectiveness, monitoring, and comparison of treatment.
In a study comparing the early term pain and functional scores of CS injection and PRP application in patients with SIS, CS injection was found to be more effective. 33 In the related article, 1 session of PRP produced from 30 mL of blood was applied, and as we mentioned, it is difficult to compare the applications using different amounts, different numbers, and different amounts of LA with each other.
CS and LA injection is an effective therapy for the treatment of symptomatic subacromial pathologies, such as impingement, tendinitis, and bursitis. 17 The injection can substantially reduce pain and increase ROM. A rotator cuff tear should be suspected if there is no improvement after injection. 40 Despite its possible local and systemic side effects, CS and LA application should be included in the clinician’s conservative treatment portfolio as an effective and inexpensive method. It should be carefully preferred in elderly patients with degenerative shoulder pathologies, especially in patients with hypertension and diabetes.17,33,44
Another practitioner-dependent difference seen in subacromial injection applications is the amount of LA administered. A systematic review comparing low- and high-volume LA applications combined with CS therapy in patients with SIS reported that high volumes were associated with lower risk of function, pain, and complications. 37
A study comparing PRP injection and ET in patients with SIS emphasized the superiority of ET on functionality and shoulder ROM, although both treatments had similar effectiveness on pain relief. 25 Unlike our study, although there are commonalities in terms of ET applied to 1 group and PRP protocol applied to the other group, we applied ET, which is a cost-effective, noninvasive initial treatment, to both groups and questioned the possible additional effects of PRP. Our study showed the effectiveness of ET and the additional benefits of PRP application, especially on pain, in support of Nejati et al. 25 Since we compared QoL, functionality, and pain parameters, we did not perform a control magnetic resonance imaging that would create additional costs.
Strengths and Limitations
The strengths of the study are that the sample consists of a relatively large number of homogeneous participants, adequate treatment was accomplished by applying a standard ET with proven effectiveness to both groups, and the possible benefits were investigated with high accuracy by adding PRP treatment to 1 group.
Our study also had several limitations. ETs were performed without the supervision of a trained provider, and variable program compliance is one limitation. Other limitations include blind injections without imaging, short follow-up periods, lack of a standard for PRP application procedures, and lack of isolated PRP application groups. The heterogeneity of PRP products arises from the reasons stated: the possible variations in the application tube and anticoagulant solutions, the time of application, the variations in the number of applications and the interval, the amount of plasma applied, the application portals, the LA agent used, and the differences in the amount made it challenging to compare with the studies in the literature. Since only the PRP group was injected, the blinding of the patients may have been compromised, which may have affected their subjective evaluations. In addition, although it is a subjective scale, the main complaint of the patients at clinical presentation was pain, so the power analysis was performed on the VAS. Therefore, although we report statistical significance in comparisons of VAS subparameters, it was not possible to report significant changes for QoL and CMS subscales with this sample.
Conclusion
Our study showed that both isolated ET and additional PRP application to ET are effective methods in SIS treatment regarding pain, function, and QoL. Combining ET with PRP was superior in reducing pain and improving abduction degree and strength. Future studies with larger sample sizes and the basic science of PRP are needed to help with our understanding.
Footnotes
Acknowledgements
The authors acknowledge Associate Professor Altuğ Duramaz for his critical review of this work.
Correction (October 2024):
Article updated to remove a duplicate paragraph from the section ‘Inclusion and Exclusion Criteria.’
Final revision submitted December 22, 2023; accepted February 23, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Biruni University (reference No. 2015-KAEK-59-22-04).