
Abstract
Background:
The diameter of 4-strand semitendinosus and gracilis (ST/G) autograft varies between 6 and 8 mm in most Asian patients. Recent studies showed higher failure rates for ST/G anterior cruciate ligament (ACL) reconstructions (ACLRs) performed with graft diameters <8 mm. The 8-strand ST/G ACL graft preparation technique has been reported to achieve diameters of up to 9.5 to 11.5 mm.
Hypotheses:
(1) The diameter of the ACL graft would be >8 mm in all cases (100%) by using the 8-strand graft preparation technique and (2) the ACLR with 8-strand ST/G autograft would show satisfactory functional scores, excellent knee stability with good graft signal, and promising graft healing status.
Study Design:
Case series; Level of evidence, 4.
Methods:
From January 2020 to January 2022, 67 consecutive patients who underwent primary ACLR with unilateral 8-strand ST/G autograft were prospectively enrolled. Clinical outcomes were assessed using functional scores (Lysholm, Tegner, and International Knee Documentation Committee [IKDC] objective grade) and physical examination results (pivot-shift test and manual maximum KT-1000 side-to-side difference [SSD]). Radiologically, intra-articular ACL graft signal intensity (grade 1, good; grade 2, moderate; grade 3, poor) and anterior subluxation of the lateral compartment (ASLC) and medial compartment (ASMC) in extension relative to the femoral condyles were evaluated on magnetic resonance imaging (MRI) scans. Additionally, second-look arthroscopic evaluations were used to assess the synovial coverage (A, normal [>75%]; B, nearly normal [50%-75%]; C, abnormal [25%-50%]; and D, severely abnormal [<25%]) of the ACL graft.
Results:
Ultimately, 50 patients were enrolled and completed the minimum 2-year follow-up tasks. The mean graft diameter for the 8-strand graft configuration was 9.3 mm (range, 8.5-10.5 mm). At final follow-up, all of the following showed significant improvements (pre- vs postoperatively): mean Lysholm score (52.7 vs 93.2; P < .001), median Tegner Activity Scale (5 vs 8; P < .001), IKDC objective grading results (27 grade C and 23 grade D vs 48 grade A and 2 grade B; P < 0.05), pivot-shift tests (27 grade 1+ and 23 grade 2+ vs 48 grade 0 and 2 grade 1; P < .001) and manual maximal KT-1000 SSD (6.7 vs 1.0 mm; P < .001). Additionally, 46 (92%) patients showed grade 1, 3 (6%) showed grade 2, and only 1 (2%) showed grade 3 graft intensity on MRI scans. The synovial coverage of the grafted tendon was observed as grade A in 46 (92%) and grade B in 4 (8%) patients during the second-look arthroscopic exploration. However, there were no significant differences observed in the mean ASLC and ASMC in extension, respectively, before (5.9 vs 4.1 mm; P = .10) and after (4.8 mm vs 3.5 mm; P = .34) surgery.
Conclusion:
The 8-strand graft configuration technique proposed in this study ensured that the diameter of the ST/G ACL autograft reached ≥8 mm. Additionally, this technique demonstrated promising clinical scores, knee stability, and graft maturity in ACLR patients at 2-year minimum follow-up in this cohort.
Anterior cruciate ligament (ACL) reconstruction (ACLR) using semitendinosus and gracilis (ST/G) hamstring tendon autograft is a popular technique. The biomechanical study of Hamner et al 8 demonstrating that equally tensioned doubled ST/G autografts were stronger and stiffer than the gold standard bone–patellar tendon–bone autograft was the foundation for establishing 4-strand ST/G autograft configuration as the standard method for preparing ACL grafts. However, the diameter of the 4-strand ST/G autograft varies between 6 and 8 mm in most Asian populations. 27
Recent clinical outcome studies demonstrating higher failure and revision rates for ST/G autograft ACLRs with graft diameters <8 mm have led to interest in developing graft preparation techniques that can potentially increase the diameter of hamstring tendon ACL autografts.5,7,8 Previous studies have shown that in the 5-strand ST/G graft configuration, 75% of grafts have a diameter >8 mm, compared with approximately 28% in the 4-strand ST/G graft configuration. 15 The 5-strand ST/G graft preparation technique lies in the ability to triple the ST tendon. It has been reported that the mean increase in the diameter of the 5-strand versus the traditional 4-strand hamstring tendon ACL graft was 1.4 mm. 13 However, the unequally tensioned tripled ST tendon might not necessarily increase the ultimate load to failure and stiffness of the 5-strand hamstring tendon grafts. 8 A quick and easy 8-strand ACL graft preparation technique (combination of 4-strand ST and 4-strand G) to achieve graft diameters of up to 10 to 13 mm was recently suggested by Gudas et al, 7 which might improve the ultimate load to failure of the ACL graft and, meanwhile, increase the coverage of the native ACL attachment site. Until now, few studies have investigated the clinical efficacy of such an ACLR technique.
The purpose of this study was therefore to report the minimum 2-year clinical, radiological, and second-look arthroscopic outcomes of ACLR with 8-strand ST/G autograft configuration. The hypotheses of this study would be as follows: (1) the diameter of the ACL graft would be >8 mm in all cases (100%) by using the 8-strand graft preparation technique; and (2) the ACLR with 8-strand ST/G autograft would show satisfactory functional scores, excellent knee stability with good graft signal and promising graft healing status.
Methods
Study Design
This was a prospective study. This study received approval from our institutional review board. Informed consent was obtained from all participants in this study. From January 2020 to January 2022, patients who had noncontact ACL injuries and underwent primary anatomic single-bundle ACLR at our institution were prospectively enrolled. The included patients underwent ACLR with a unilateral 8-strand ST/G graft preparation technique. The contralateral side had to be intact to evaluate the side-to-side difference (SSD) during physical examinations. Patients excluded from the study met ≥1 of the following criteria on the injured side: major concomitant procedure (eg, multiligament reconstructions, high tibial osteotomy, and/or anterolateral extra-articular tenodesis), history of knee surgery, generalized joint laxity (>5 of 9 on the Beighton score) or significant local hyperextension (>10°) of the knee joint, lack of available preoperative or postoperative magnetic resonance imaging (MRI) scans, and lack of minimum 2-year follow-up data. Patients who underwent partial meniscectomy, meniscal repair, or cartilage microfracture were not excluded from this study. The patient enrollment process is shown in Figure 1.
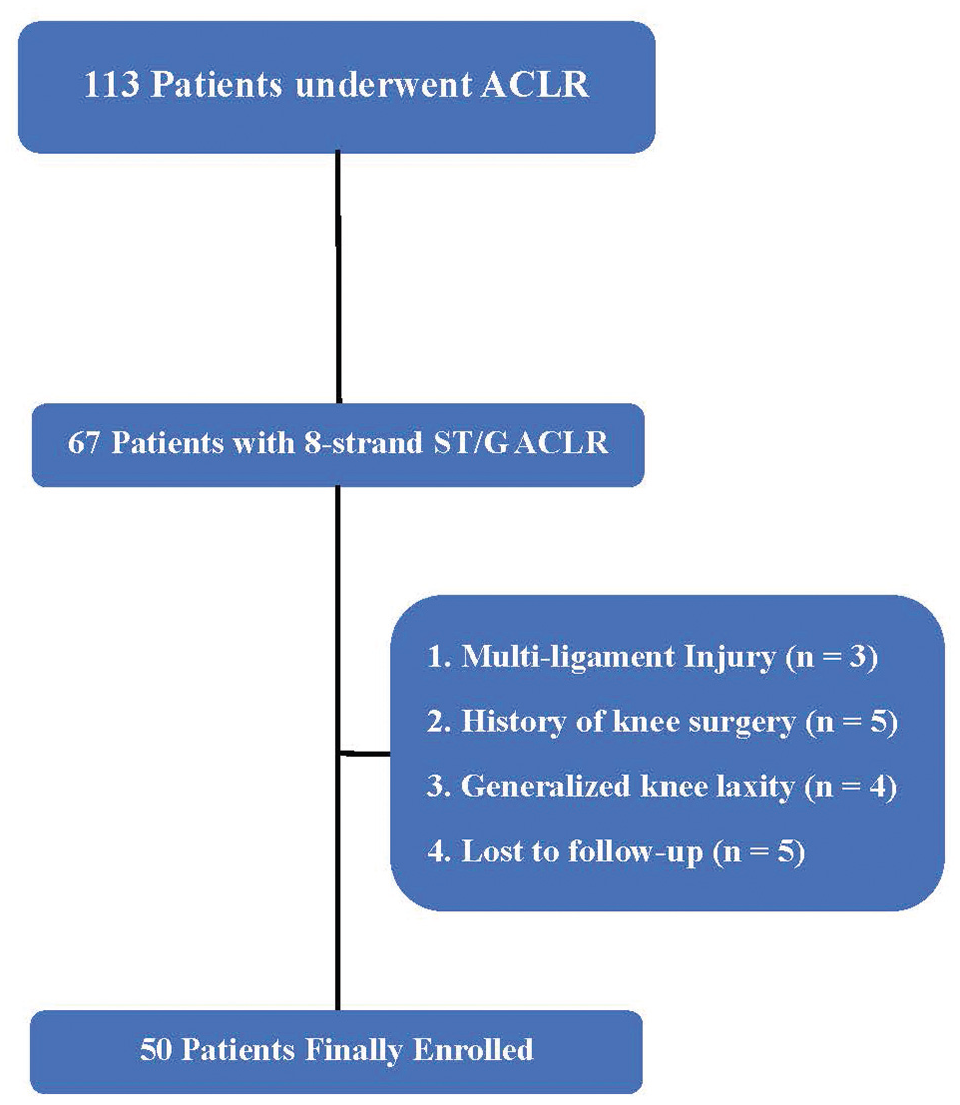
Flowchart of the patient enrollment process. ACLR, anterior cruciate ligament reconstruction; ST/G, semitendinosus and gracilis.
Surgical Technique
All procedures were performed by a single senior surgeon (H.Z.) using an 8-strand ST/G autograft configuration. The minimal graft length for the 8-strand ST/G technique was 24 cm and ≥6.0 cm after folding: 15 mm in the femoral bone socket, about 30 mm intra-articularly, and 15 mm in the tibial canal (Figure 2). ST/G full-length tendons were harvested using standard technique and trimmed to ≥24 cm in length. Each tendon graft was doubled and sutured at the ends with 2-0 FiberWire sutures (Arthrex). Then both tendons were passed through the suture loop of the Tightrope RT system (Arthrex) and bent, achieving an 8-strand graft (combination of 4-strand ST and 4-strand G) (Figure 3). If the length of the G tendon was <24 cm, the 6-strand ST/G technique was used (combination of 4-strand ST and 2-strand G).
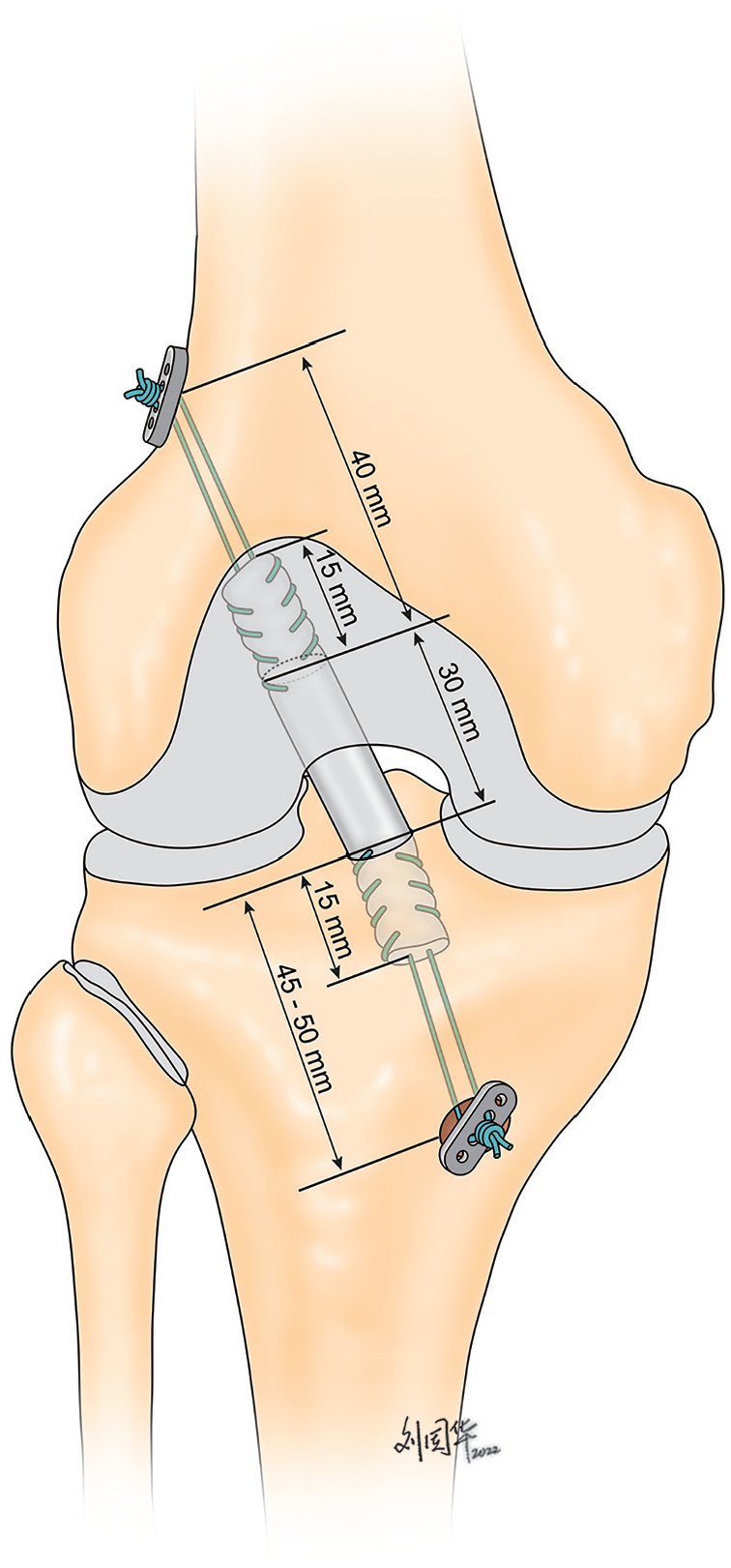
Diagram of the anatomic anterior cruciate ligament reconstruction using 8-strand semitendinosus and gracilis graft configuration.

(A) The diameter of semitendinosus and gracilis (ST/G) autograft is only 7.5 mm by using the 4-strand configuration technique. (B) Each tendon graft was doubled and sutured at the ends with 2-0 FiberWire sutures. (C) The diameter of the ST/G autograft increased to 9.0 mm by using the 8-strand configuration technique.
Standard anterolateral and anteromedial portals were used for arthroscopy and an accessory anteromedial portal for instrumentation. Debridement, meniscal surgery, and preparation of the intercondylar notch were performed before ACLR. The femoral tunnel was drilled at the anatomic anteromedial bundle position by using the inside-out technique through the accessory anteromedial portal with the knee in 120° of flexion. A full 4.5-mm bone canal was formed with a specialized drill. Then, a femoral socket was reamed, gradually increasing the diameter of the drill until it became equal to the 8-strand graft. A socket length of 15 mm was recommended. Sutures were passed through the femoral tunnel. Then a full tibial tunnel was drilled using an outside-in approach using a tibial aimer set at 55° to obtain a long enough bone tunnel calibrated with the length and width of the 8-strand graft. The length of the tunnel from 45 to 50 mm was recommended. Sutures were retrieved through the tibial tunnel, and the 8-strand graft was loaded. The graft was pulled outside in and tracked with the arthroscope as it moved through the joint space to the femoral socket. Tensioning threads of the Tightrope RT system were used to strain the fixation loops and fix the autograft into the femoral socket. The tibial side of the 8-strand autograft was fixed with a suspensory fixation device using the Tightrope ABS button (Arthrex) while the knee was in 20° of flexion. Additional knots were tied over the button. Supplementary tibial fixation was performed by tying the sutures around a bicortical screw. Possible impingement of the ACL graft to the intercondylar notch was then checked. A notchplasty was performed if needed.
Postoperative Rehabilitation
A hinged knee brace was used from the first 4 weeks. The brace was unlocked to allow a passive range of motion from 0° to 90°, with emphasis on early passive extension stretching. Partial weightbearing was not allowed until 4 weeks after surgery. Full weightbearing was started at 6 weeks postoperatively. Patients were allowed to return to preinjury level of sports at 9 to 12 months after surgery.
Data Collection
Patient characteristics, physical examination results, clinical scores, MRI evaluations, intraoperative findings, and second-look arthroscopic outcomes were recorded and analyzed individually. All data were collected by 2 observers (D.W. and T.Z.).
Patient Data
Age, sex, posterior tibial slope (PTS), and time from injury to surgery were recorded for all patients. PTS was measured by 2 knee fellowship-trained orthopaedic surgeons (T.Z. and Y.C.) using a picture archiving and communication system workstation (GE Healthcare). In this study, PTS was measured using the method described by Julliard et al, 11 which was the angle between the tangent line of the medial tibial plateau and the line perpendicular to the mechanical axis of the tibia (Figure 4). This method was considered suitable, as the full length of the tibia was shown. The mean value of PTS was calculated from the results of the 2 observers.

The posterior tibial slope (PTS) is measured on whole-leg radiograph, which is the angle formed by the tangent line to the medial tibial plateau and the line perpendicular to the mechanical axis of the tibia (the line connecting the middle point of tibial plateau and the center of the talus). For this patient, the PTS was 18°.
Physical Examination Results
All physical examinations were performed preoperatively and ≥2 years after surgery with the patient under anesthesia. The physical examinations included the pivot-shift test and the KT-1000 arthrometer. The pivot-shift test was graded as negative, 1+ (glide), 2+ (clunk), and 3+ (locking). The KT-1000 arthrometer was performed using the maximal manual forces and recorded as the SSD. All physical examinations were performed by the senior author (H.Z.).
Intraoperative Findings
The diameter of the ST/G ACL graft was recorded as 4-strand and then 8-strand, respectively. The presence of concomitant meniscal tears was verified during ACLR.
Clinical Scores
The standardized Lysholm subjective score, the Tegner Activity Scale, and International Knee Documentation Committee (IKDC) objective grading system were used preoperatively and ≥2 years after surgery. For the IKDC objective grading system, patients were given an overall grade of A (normal), B (nearly normal), C (abnormal), or D (severely abnormal). All clinical scores were collected and recorded by the senior surgeon (H.Z.).
MRI Evaluations
MRI was performed using a 1.5-T superconducting magnet (Signa; GE Medical Systems) using a standardized institutional protocol. The MRI protocols included coronal, sagittal, and axial sequences. Each sequence included the T1 and T2 weighted phases (echo time, 25-30 ms; repetition time, 4000-6000 ms; and slice thickness, 3.5 mm with no gap). Examinations were performed with the patient in the supine position and with a pillow under the entire lower leg and ankle, supporting the leg in extension and with neutral rotation. The quadriceps muscle was relaxed, and no anesthesia was used in any patient. The extremity was secured in a commercial extremity coil (8-channel knee coil; Medrad) to ensure a consistent extremity position for all patients. In this study, all patients received MRI scans preoperatively and at 2-year minimum follow-up visit.
Anterior tibial subluxation (ATS) in extension was measured on MRI scans. Electronic measurements were performed by 2 observers (D.W. and Y.C.) to determine the anterior subluxation of the lateral compartment (ASLC) and medial compartment (ASMC) in extension relative to a posterior femoral condylar reference line on sagittal MRI scans using the method described by Song et al. 21 The amount of ASLC and ASMC in extension was measured on the preoperative and postoperative MRI scans (Figure 5). To determine the interobserver and intraobserver reliability of the measurement, intraclass correlation coefficients (ICCs) were calculated by randomly selecting 10 preoperative MRI scans from the included patients.18,25 The 2 observers separately measured the amount of ASLC and ASMC. In addition, 1 independent observer (D.W.) performed all the above MRI measurements on each selected patient twice 2 weeks apart. The interobserver and intraobserver ICCs were as follows, respectively: 0.92 and 0.96 for the ASLC measurement and 0.93 and 0.95 for the ASMC measurement.

The preoperative magnetic resonance imaging scans of the same patient illustrate the excessive anterior tibial subluxation in extension. (A) For anterior tibial subluxation of the lateral compartment (ASLC) in extension, the first line was drawn tangent to the tibial plateau (a); the circle represented a best-fit circle over the posterior lateral femoral condyle at the subchondral bone. The posterior reference line (c) was drawn from the posterior margin perpendicular to the tibial plateau (a). An additional line perpendicular to line a represented the posterior tibial plane (b). The distance between these lines (b and c) demonstrated ASLC in extension. For this patient, the amount of ASLC in extension was 7.8 mm. (B) The amount of anterior tibial subluxation of the medial compartment (ASMC) in extension for this patient was 4.6 mm.
In addition, signal intensity of the intra-articular portion of the ACL graft was analyzed on postoperative MRI scans using the method described by Howell et al. 9 Grade 1 (good), low graft signal that had a homogeneous low-intensity signal indistinguishable from that of the posterior cruciate ligament or patellar tendon; grade 2 (moderate), high-intensity signal within 50% of the whole graft; and grade 3 (poor), high-intensity signal >50% of the whole graft (Figure 6).
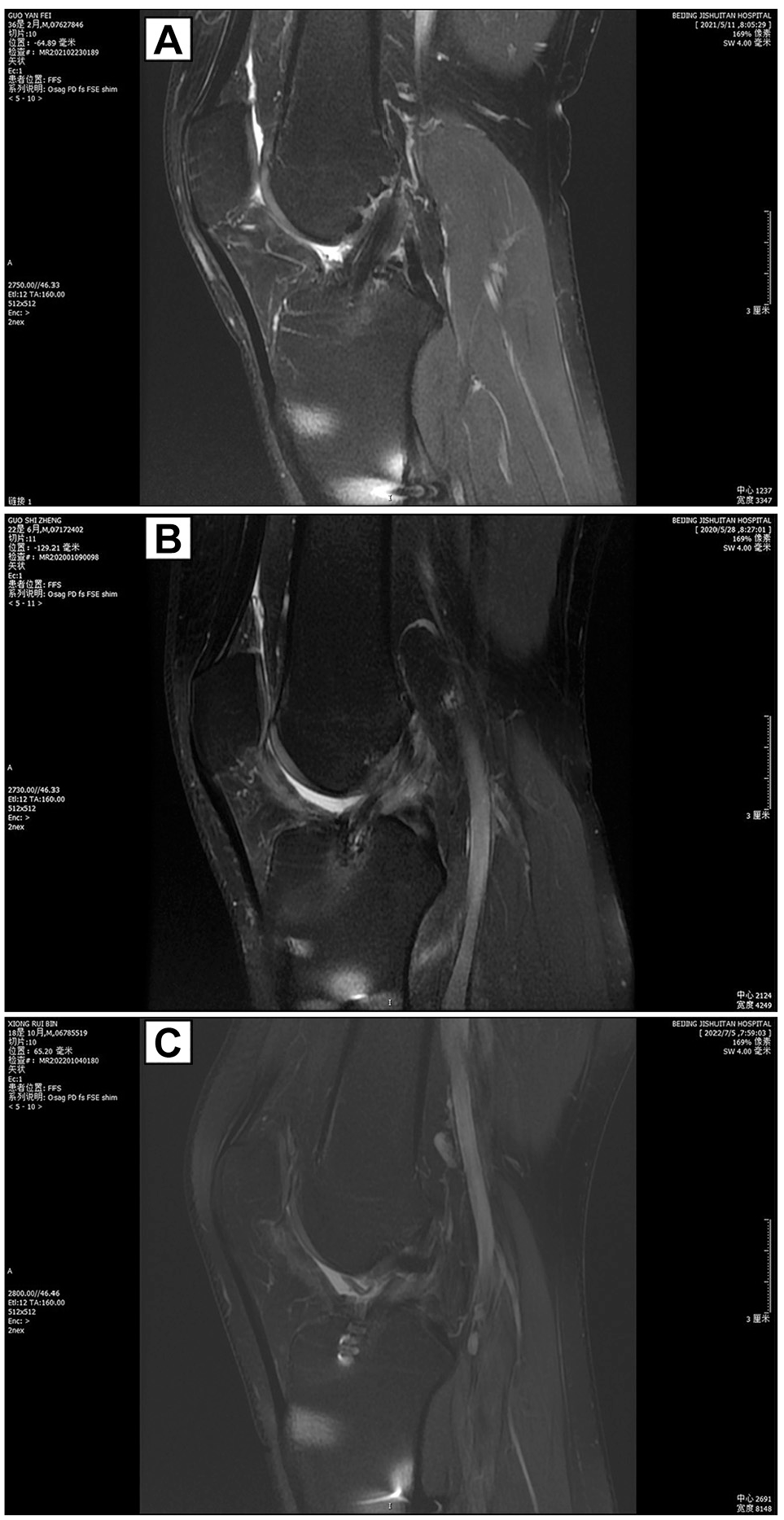
Case presentations of graft signal intensity, which showed (A) grade 1 signal, (B) grade 2 signal, and (C) grade 3 signal.
Second-Look Arthroscopic Findings
For patients who wanted to remove the cortical fixation device and agreed to undergo second-look arthroscopic surgery, the synovial coverage of the ACL graft was assessed. The extent of synovial coverage was graded as 4 types: A, normal (>75%); B, nearly normal (50%-75%); C, abnormal (25%-50%); and D, severely abnormal (<25%). 22 Moreover, the presence of graft roof impingement (GRI) during knee passive motion was recorded based on the findings reported by Watanabe and Howell 26 : (1) fractured or guillotined bundles at the tibial insertion or (2) cyclops lesion.
Statistical Analysis
Descriptive statistics were calculated for patient characteristics, physical examination results, clinical scores, intraoperative findings, MRI evaluations, and second-look arthroscopic findings. Comparisons between the preoperative and postoperative status were performed. Continuous variables were analyzed by the paired t test or Wilcoxon signed-rank test according to the assumption of normality and homoscedasticity. Categorical variables were analyzed by Pearson chi-square test or Fisher exact test. All statistical analyses were performed using SPSS software (Version 26.0; IBM). The significance level was set at .05. For priori power analysis, the sample size was based on the Lysholm score, where a 10-point improvement would be significant, and the expected standard deviation in the Lysholm score was 15 points; thus, for a power of .80 and α = .05, a sample size of ≥36 was required.
Results
Patient Data
There were 50 patients ultimately enrolled in this study. The mean age at the time of surgery was 28.2 ± 7.2 years. All patients completed the minimum 2-year follow-up tasks. The patient group included 40 men and 10 women, with the right side involved in 23 patients and the left side in 27 patients. The mean time from injury to surgery was 12 months (range, 0.5-120 months). The mean follow-up time was 2.4 years (range, 2-3 years).
Intraoperative Findings
There were 27 (54.0%) and 28 (56.0%) patients combined with lateral and medial meniscal injuries, respectively. The mean graft diameter for the 4-strand ST/G autograft was 7.3 ± 0.4 mm (range, 6.5-8.5 mm), which increased to 9.3 ± 0.5 mm (range, 8.5-10.5 mm) by using the 8-strand graft preparation technique.
Clinical Scores
The mean Lysholm score increased from 52.7 (range, 46-58) preoperatively to 93.2 (range, 86-100) postoperatively (P < .001). The median Tegner Activity Scale increased from 5 (range, 4-6) preoperatively to 8 (range, 7-9) postoperatively (P < .001). All (100%) patients returned to the same preinjury activity level at the minimum 2-year follow-up visit. Specifically, 36 (72.0%) patients returned to competitive athletics sports, 10 (20.0%) patients returned to competitive sports (basketball or football), and the remaining 4 (8.0%) patients returned to recreational sports (tennis, volleyball, jogging). The objective IKDC grading system was graded C in 27 (54.0%) patients and graded D in 23 (46.0%) patients preoperatively, whereas it was graded A in 48 (96.0%) patients and graded B in 2 (4.0%) patients at the final follow-up visit (P < .001) (Table 1).
Pre- and Postoperative Comparisons of Clinical Outcomes (N = 50) a

Data are presented as mean ± SD, median (range), or n (%). ASLC, anterior subluxation of the lateral compartment; ASMC, anterior subluxation of the medial compartment; IKDC, International Knee Documentation Committee; SSD, side-to-side difference.
Physical Examination Results
Preoperatively, none of the patients had any fixed flexion deformity or genu recurvatum. Postoperatively, all patients returned to their preinjury full range of motion of the knee joint. The mean KT-1000 SSD was 6.7 mm (range, 4 to 8 mm) preoperatively and significantly decreased to 1.0 mm (range, –1 to 3 mm) at the final follow-up visit (P < .001). Preoperatively, 27 (54.0%) patients had grade 0/grade 1 pivot-shift test results and 23 (46.0%) had grade 2 pivot-shift test results. At the final follow-up visit, 48 (96.0%) patients had a grade 0 pivot-shift test result and only 2 (4.0%) patients showed a grade 1 pivot-shift test result (P < .001) (Table 1).
MRI Evaluations
The preoperative mean ASLC and ASMC in extension were 5.9 mm (range, 2-9 mm) and 4.1 mm (range, 1-7 mm), respectively. At the final follow-up visit, the mean ASLC and ASMC in extension were 4.8 mm (range, 0-7 mm) and 3.5 mm (range, 0-6 mm), respectively. There were no significant changes observed in both variables compared with the preoperative status (P > .05) (Table 1). In terms of ACL graft signal intensity, 46 (92.0%) cases showed grade 1, 3 (6.0%) cases showed grade 2, and only 1 (2.0%) patient showed grade 3 signal. There were 4 (8.0%) patients who showed grade 2 or 3 graft signal intensity on the final MRI scans. Among them, 2 patients showed grade 1 and the other 2 showed a grade 0 pivot-shift test result. The mean time from injury to surgery of these 4 patients was 40 months (range, 8-84 months), and all showed chronic ACL injury. Moreover, the mean PTS of these 4 patients was 18.5° (range, 17.0°-20.3°), which all showed steep PTS values.
Second-Look Arthroscopic Findings
For patients who wanted to remove the cortical fixation device and agreed to undergo second-look arthroscopic surgery, the synovial coverage of the ACL graft was assessed. The ACL grafted tendons all showed intact during the second-look arthroscopic exploration. The survival rate of the graft was 100%. Moreover, 2 (4.0%) patients had combined cyclops lesions and 2 (4.0%) patients had fractured or guillotined bundles, which underwent intercondylar notchplasty during the exploration. In addition, there were 46 (92.0%) patients who showed grade A and 4 (8.0%) patients who showed grade B synovial coverage of the ACL grafted tendon.
Discussion
The most important findings of this study were as follows: (1) the 8-strand graft configuration technique proposed in this study ensures that the diameter of the ST/G ACL autograft reaches ≥8 mm; (2) this technique demonstrated promising clinical scores, knee stability and graft maturity in ACLR patients at 2-year minimum follow-up in this cohort.
Conte et al 5 summarized and analyzed data from 913 patients in 2014 and found that the autogenous 4-strand hamstring tendon graft reconstruction can effectively reduce failure rates when the diameter of the ACL graft exceeds 8 mm (odds ratio [OR], 6.8; P = .008). Recently, Itoh et al 10 conducted a systematic review which indicated that within the range of 7 to 9 mm, for every 0.5-mm increase in the diameter of the 4-strand ACL graft, the risk of ACLR failure decreased. Biomechanical tests also showed a strong correlation between the mechanical strength of the autogenous ST tendon graft and its size. Boniello et al 1 discovered that the mean failure load was 2359 N for a 4-strand graft diameter of 6 mm, 3263N for 7 mm, and 3908N for 8 mm. It can be assumed that increasing the diameter helps to enhance the ultimate load to failure of the ACL graft, thus reducing the risk of graft failure after reconstruction. It should be noted that the diameter of the autogenous 4-strand hamstring tendon graft is significantly correlated with an individual’s height.4,6,16 Therefore, it is challenging to obtain 4-strand grafts with a diameter exceeding 8 mm from female or petite patients. Additionally, the Asian population generally has a shorter stature, making it difficult to achieve 4-strand graft diameters and ultimate load to failure of the graft equivalent to those of the Caucasian population using the same graft preparation techniques. 4 A study has reported that the mean diameter of 4-strand ST/G grafts in Chinese patients is 7.4 mm. 27 Given this, the proposal of graft configuration techniques targeting this patient population is of vital importance for reducing the failure rate of ACLR.
Previous studies have shown that the 4-strand ST/G graft configuration technique cannot guarantee satisfactory graft diameters from female or petite patients. 5 Subsequent research has indicated that this technique can only ensure that 28% of graft diameters exceed 8 mm. 13 The 5-strand autogenous tendon graft configuration, combining tripled ST tendons with doubled G tendons, has been utilized to further increase the overall graft diameter.3,12-14 Lodhia et al 15 were the first to use the 5-strand ST/G tendon grafts for ACLR. They reported that compared with the 4-strand graft configuration, the 5-strand graft preparation technique achieves better knee joint stability. 15 Krishna et al 13 demonstrated that the 5-strand graft configuration technique ensured that 75% of patients had graft diameters >8 mm, which was crucial for reducing graft failure rates after reconstruction. Clinical experience suggests that transitioning from a 4-strand to a 5-strand graft configuration generally increases the graft diameter by 1 mm. 15 However, biomechanical studies have shown no significant differences between the 2 configurations in terms of mean failure load, stress relaxation, stiffness, and graft displacement.2,24 Many clinical studies have also demonstrated no significant statistical differences between the 2 graft configurations in terms of patient-reported outcomes (Lysholm knee score, IKDC Subjective Knee Score, 36-Item Short Form Health Survey, and Tegner Activity Scale), objective tests (KT-2000 measurements, Lachman test, pivot-shift test, and hop test), and graft rerupture rates.12,15
Gudas et al 7 have reported a detailed technique for preparing (>10 mm) ACL grafts (combination of 4-strand ST + 4-strand G) using autogenous ST/G tendons. This technique, utilizing an 8-strand graft configuration with both tendons, effectively increases the graft diameter while enhancing fixation strength and maximizing coverage of the anatomic ACL attachment area. When the 4-strand hamstring tendon diameter is <8 mm in female patients, this technique can achieve a final graft diameter of 11 mm. Currently, there is limited clinical research on the 8-strand graft configuration. In this study, data from patients who underwent ACLR with the 8-strand graft configuration at our center over 3 years were summarized, and a follow-up observation of ≥2 years was conducted. The analysis suggested that this technique ensures that all graft diameters exceed 8 mm; significantly improves postoperative clinical scores, knee joint stability, and graft signal intensity; and effectively controls graft failure rates. The key point of the 8-strand graft preparation technique is to quadruple both the ST and the G tendon; therefore, the length of the tendons should be >24 cm to ensure that the length of the 8-strand graft is >6 cm. However, sometimes the length of the G tendon is shorter than 20 cm. In this situation, the 6-strand technique is recommended (4-strand ST and 2-strand G).
The currently recognized appropriate threshold for graft diameter is 8 mm.15,17,19,20 Snaebjörnsson et al 20 conducted a registry study involving 18,425 patients to explore the correlation between graft diameter and graft failure rates. The study revealed that compared with larger diameter autografts, patients with 4-strand hamstring autografts ≤8 mm in diameter had a significantly increased risk of ACL retear by 25% (OR, 1.25; 95% CI, 1.01-1.57). Furthermore, for every 1-mm increase in graft diameter, the likelihood of ACL revision within 2 years after reconstruction decreased by 0.84 times. Larger autografts contain more collagen, thereby increasing their tensile strength, which may at least theoretically explain this association. 20 This study included a total of 50 patients who underwent ACLR with an 8-strand ST/G configuration, with a mean graft diameter of 9.3 mm. All graft diameters were ≥8 mm, with a maximum diameter of 10.5 mm. It is worth noting that oversized grafts may also carry the risk of graft impingement. 23 In this study, 4 patients experienced graft roof impingement (GRI), with 3 having a graft diameter of 10 mm and 1 patient with a graft diameter of 9.5 mm. However, it cannot be definitively concluded whether GRI is correlated with excessively large graft diameter because the notchplasty is performed.
This study also found that although the 8-strand graft configuration effectively reduced the postoperative ACL graft failure rate and revision rate, simply increasing the graft diameter did not effectively control the ATS at 2-year minimum follow-up. Clinical data have shown that an excessive preoperative ATS increase is associated with poorer clinical outcomes after anatomic ACLR, 22 but no clinical data indicate that increased postoperative ATS leads to graft failure. In this study, the mean preoperative ASLC and ASMC were 5.9 mm and 4.1 mm, respectively. Song et al 22 found that excessive (>10 mm) preoperative ATS in extension after ACL injury was associated with inferior knee stability after anatomic ACLR. This threshold is significantly higher than the ATS value observed in this study, which may explain why there was no improvement in this variable.
Limitations
This study has several limitations. First, it lacks a control group, which to some extent weakens the generalizability of the results. However, the study strictly adhered to the inclusion criteria and examined data only from patients who underwent the isolated 8-strand ST/G anatomic ACLR, providing data support for investigating the clinical application of the 8-strand graft preparation technique. Second, exclusion of high-risk patients, such as patients with general laxity and high-demand female athletes, also limits the generalizability of the results. For such those patients with high risk of reinjury, the additional anterolateral tenodesis should be performed during our clinical practice. Furthermore, the study included patients from a single center, which introduces selection bias and limits the extrapolation of the research findings.
Conclusion
The 8-strand graft configuration technique proposed in this study ensures that the diameter of the ST/G ACL autograft reaches ≥8 mm. Additionally, this technique demonstrated promising clinical scores, knee stability, and graft maturity in ACLR patients at 2-year minimum follow-up in this cohort. This may provide an easy path for graft preparation if the 4-strand ST/G graft diameter is <8 mm.
Footnotes
Final revision submitted March 29, 2025; accepted April 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (82002288), National Natural Science Foundation of China (82172514), Beijing Natural Science Foundation (7254374), and Beijing Hospitals Authority Youth Programme (QML20230402). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from Beijing Jishuitan Hospital, Capital Medical University.
Data Accessibility Statement
Data yielded in our study will be made available by the authors to any qualified researchers.