
Abstract
Purpose:
To compare the healing and clinical outcomes of anterior cruciate ligament (ACL) reconstruction between patients with or without intraoperative administration of adipose-derived regenerative stem cells (ADRC).
Methods:
Between 2013 and 2014, the outcomes of 20 soccer players undergoing ACL reconstruction using bone–patellar tendon–bone autograft infiltrated with ADRC at the end of the procedure were compared to a historical, matched cohort of 19 soccer players undergoing the same procedure without ADRC. Outcomes were obtained at baseline, and 6 and 12 months postop for IKDC (International Knee Documentation Committee), Lysholm, and Lequesne, and at 2, 4, 6, and 12 months postop for VAS (visual analogue scale) for pain and graft maturation to evaluate the ligamentization process (magnetic resonance imaging (MRI)-based).
Results:
Both groups significantly improved the IKDC (p < 0.001 in both groups), Lysholm (p < 0.001 in both groups), Lequesne index (p < 0.001 in both groups), VAS for pain (p = 0.002 for the ADRC and p < 0.001 for the control group), and MRI scores (p < 0.001 in both groups) in the 12 months postop compared to baseline scores. However, there were no significant differences in the improvement of the outcomes between groups across time (p > 0.05). All patients returned to sports after surgery, but 8 (40%) patients in the ADRC and 13 (68.4%) patients in the control group had lower Tegner activity score at 12 months postop.
Conclusions:
Patients receiving ADRC at the time of ACL reconstruction significantly improved knee function and healing/maturation of the graft at 12 months. However, this improvement was not statistically significant compared to a control group undergoing ACL reconstruction alone.
Keywords
Introduction
Anterior cruciate ligament (ACL) tear is the most common serious knee injury in soccer. 1 The gold standard for treatment of ACL injuries is arthroscopic-assisted reconstruction. 2 Despite the outcomes of ACL reconstruction are generally very good, this injury implies shorter career duration, lower performance after injury, and long recovery period before the player is cleared to return to play. 3 –5 Therefore, strategies aimed to increase or accelerate healing are paramount, particularly in high-level soccer.
Biologic therapies aimed to improve or accelerate the healing process after ACL reconstruction are growth factors, biomaterials, stem cells, gene therapy, autologous tissue, biophysical/environmental, and pharmaceuticals. 6 –8 Of these, platelet-rich plasma (PRP) is the most commonly employed. 6 –8 The use of PRP during ACL reconstruction has demonstrated a positive influence in the tissue healing process both at the tendon portion of the graft and at the donor site. 9 –11
Cell-based therapies in ACL reconstruction have been tried. 12,13 The two main sources of stem cells are the bone marrow and adipose tissue. Adipose tissue has been identified as an abundant and accessible source of stem cells and other regenerative cells (referred to as adipose-derived regenerative stem cells or ADRC). 14,15 Studies have demonstrated that ADRC and bone marrow-derived mesenchymal stem cells have pro-angiogenic, antiapoptotic, and immunomodulatory properties. 16 –19 However, the number of clinical studies using stem cells in ACL reconstruction is very limited, 6 and the only available study have used bone marrow-derived mesenchymal stem cells. 20 Therefore, investigating the clinical applications of ADRC in ACL reconstruction is clearly needed.
The purpose of this study was to compare the healing and clinical outcomes of ACL reconstruction between patients with or without intraoperative administration of ADRC. It was hypothesized that ADRC would improve the healing and clinical outcomes of ACL reconstruction when using bone–patellar tendon–bone (BTB) autograft.
Material and methods
Procedures
An open-label, single-arm study was conducted to evaluate the efficacy of ADRC administration to improve the healing and clinical/functional outcomes of ACL reconstruction using BTB autografts. Between June 2013 and June 2014, 20 soccer players with ACL tear treated with reconstruction using BTB autograft with additional ADRC intraoperative administration were enrolled in the study (experimental group). Patients were included if they (1) were aged 18 years or older, (2) had primary acute ACL tear, and (3) consented to participate in this study. A historical, matched cohort was obtained from same-level soccer players/athletes undergoing ACL reconstruction using the same technique without ADRC administration (control group). 11,21 The outcomes were obtained at baseline and at several postoperative periods and compared between both groups (see “Outcome measurements” section). Patients from both groups had been operated at the same Institution by the same surgical team, through the same surgical technique, and following the same rehabilitation protocol. This study received approval by the Agencia Española del Medicamento y Productos Sanitarios and by the Ethical Committee for Clinical Research at our Institution.
Patients
There were 20 soccer players and 19 soccer players/athletes from other sports in the experimental and control groups, respectively. The mean (standard deviation (SD); range) age was 24.7 (4.7; 18–40) years in the experimental group and 31.1 (8.4; 19–48) years in the control group (p = 0.005). The mean (SD) weight was 77.9 (10.5) kg in the experimental group and 78.6 (11.8) kg in the control group (p = 0.8). The mean (SD) height was 1.7 (0.07) m in the experimental group and 1.7 (0.06) m in the control group (p = 0.2). The mean (SD) body mass index was 24.7 (3) in the experimental group and 25.6 (3.9) in the control group (p = 0.4). The median (range) preoperative Tegner activity scale was 9 (9–10) and 7 (4–8) in the experimental and control groups, respectively (p < 0.001). The time interval between injury and surgery was 15 days to 1 year.
Surgical technique
The surgical technique employed in this study is the monofascicular anatomic ACL reconstruction using the BTB autograft. 22 The graft was taken from the central third of the patellar tendon of the injured knee, with bone plugs measuring 25 mm long × 9 mm wide × 6 mm thick. A tibial tunnel guide was used to create the tibial ACL attachment site at an angle of 55°. A 9-mm-diameter femoral tunnel was made at the anatomic attachment site (in the middle of the two bundles) of the ACL to the femur through the anteromedial portal. Biocomposite interference screws (Biosure, Smith & Nephew, Warsaw, Indiana, USA) were used for the femoral attachment in all cases. For the tibial site fixation, the same biocomposite interference screws were used. In cases where the bone plug ended up outside the tibial tunnel after the femoral fixation, two number 8 staples were used for the femoral site fixation.
ADRC protocol
The ADRC extraction, preparation, and administration protocol used in this study followed the Celution® System (Cytori Therapeutics, San Diego, California, USA) guidelines. Liposuction was performed in the abdomen or inner side of the thigh to obtain a sample of 360 ml of fat (or as close as possible), as per Celution® System recommendations. The lipoaspirate was introduced into an automated cell processing system (Celution® System). Cell numbers and viability were assessed using an automated cell counter (NucleoCounter®, Chemometec, Copenhagen, Denmark). The ADRC product is a diluted cell suspension which contains >95% of the total cell concentration of nonnucleated cells (red blood cells) and about 1–5% of nucleated cells. The nucleated cells are present in the following concentrations: CD31+/CD34+ (>2%); CD34+/CD31−/CD45− (>10%); CD45+/CD31−/CD34− (>15%). The combination of these phenotypes represents more than 90% of the nucleated cells in the ADRC product. Once the ACL reconstruction was finalized, the BTB graft was infiltrated with 5 mL of the prepared ADRC solution under direct dry-arthroscopy visualization before skin closure (Figure 1).

Intraoperative picture demonstrating the intra-ACL graft infiltration of ADRC. ADRC: adipose-derived regenerative stem cells; ACL: anterior cruciate ligament.
Outcome measurements
The outcomes evaluated in this study included knee pain, function, and imaging studies. Knee pain was evaluated at 2, 4, 6, and 12 months after surgery through the visual analogue scale (VAS). The Lequesne index, 23 the Tegner activity scale, 24 the Lysholm knee scoring system, 25 and the International Knee Documentation Committee (IKDC) subjective evaluation form 26 were obtained at baseline and at 6 and 12 months after surgery in both groups.
Magnetic resonance imaging (MRI) of the knee was obtained at 2, 4, 6, and 12 months after surgery to evaluate remodeling of the ACL graft. An experienced musculoskeletal radiologist evaluated the signal intensity of the graft, which was broken down into four remodeling stages 27 : grade I, diffuse, increased T2 signal intensity of the graft with no area of normal ligament; grade II, <50% of ligament volume with a normal-appearing ligament signal intensity; grade III, >50% of normal ligament signal mixed with portions of the graft yielding increased signal intensity; and grade IV, 100% and homogeneously hypointense signal (indistinguishable from the posterior cruciate ligament and patellar ligament).
Rehabilitation protocol
The rehabilitation protocol was the same in both groups. All patients were placed in an immobilizing cast splint for 1 week, performing isometric exercises and allowing the patients to perform partial weight-bearing using crutches. Patients began range of motion exercises at 1 week, and full weight-bearing and elliptical exercise machine between 4 and 6 weeks after surgery (at 6 weeks, crutches were definitely discontinued). Patients were permitted to begin running at 3 months and then progress as tolerated.
Statistical analysis
Descriptive statistics were used to summarize the parameters evaluated in the present study. Mean and median were used as central tendency statistics, and SD and range were used as measures of dispersion. Demographic and baseline Tegner characteristics between groups were compared using an independent T-test and χ 2, respectively. Baseline to 12-month postoperative between-group differences for IKDC, Lysholm, Lequesne, and VAS for pain were compared using an independent T-test as well. A 2 × 3 (group by time) mixed-design repeated measures analysis of variance (ANOVA) was conducted to compare the IKDC, Lysholm, Lequesne, and VAS for pain. A Bonferroni’s post hoc analysis was conducted in the presence or absence of significant group by time interaction. A mixed ordinal logistic regression analysis was conducted to compare Tegner activity scale and MRI outcomes between groups across all time periods. The Wilcoxon signed-rank test and Mann–Whitney U test were also used for inter- and intragroup comparisons of categorical data. The χ 2, T- test, and ANOVA analyses were carried out using SPSS v.21 (SPSS Inc., Chicago, Illinois, USA), whereas the mixed ordinal logistic regression, the Wilcoxon signed-rank test, and the Mann–Whitney U test were conducted using the R project (The R Foundation, Vienna, Austria). 28 The α level was set at 0.05.
Results
The mean (SD) amount obtained from the aspiration of the adipose tissue was 119.8 ± 49.0 ml. Mean (SD) viable nucleated cells were 3.99 × 106 ± 2.77 × 106 cells/ml. Overall, mean (SD) cell viability was 87 ± 0.1%. The mean (SD) total dose of ADRC was 18.5 × 106 ± 13 × 106.
Table 1 shows the comparison of IKDC, Lysholm, and Lequesne score between both groups across all time periods. The mean (SD) difference between the baseline and the 12-month postoperative evaluation was IKDC 39.9 (19.5) for the ADRC group and 28.1 (13.5) for the control group (p = 0.03); Lysholm 28.4 (19.1) for the ADRC group and 21 (8.4) for the control group (p = 0.12); and Lequesne 5.6 (5.3) for the ADRC group and 4.5 (2.9) for the control group (p = 0.45). Table 2 shows the comparison of VAS for pain between both groups across all time periods. The mean (SD) difference between the baseline and the 12-month postoperative evaluation was 1.4 (1.2) for the ADRC group and 1.8 (1.6) for the control group (p = 0.37).
Comparison of IKDC, Lysholm, and Lequesne scores between both groups across all time periods.

ADRC: adipose-derived regenerative stem cells; G: main effect of group; G × T: group by time interaction; IKDC: International Knee Documentation Committee; m: months; postop: postoperative; preop: preoperative; SD: standard deviation; T: main effect of time.
a Significantly different from preop (p < 0.001).
b Significantly different from preop (p < 0.001) and 6 m postop (p = 0.003).
c Significantly different from preop (p < 0.001) and 6 m postop (p = 0.002).
d Significantly different from preop (p < 0.001).
e Significantly different from preop (p < 0.001).
f Significantly different from preop (p = 0.002).
g Significantly different from preop (p < 0.001) and 6 m postop (p = 0.001).
Comparison of VAS for pain scores between both groups across all time periods.
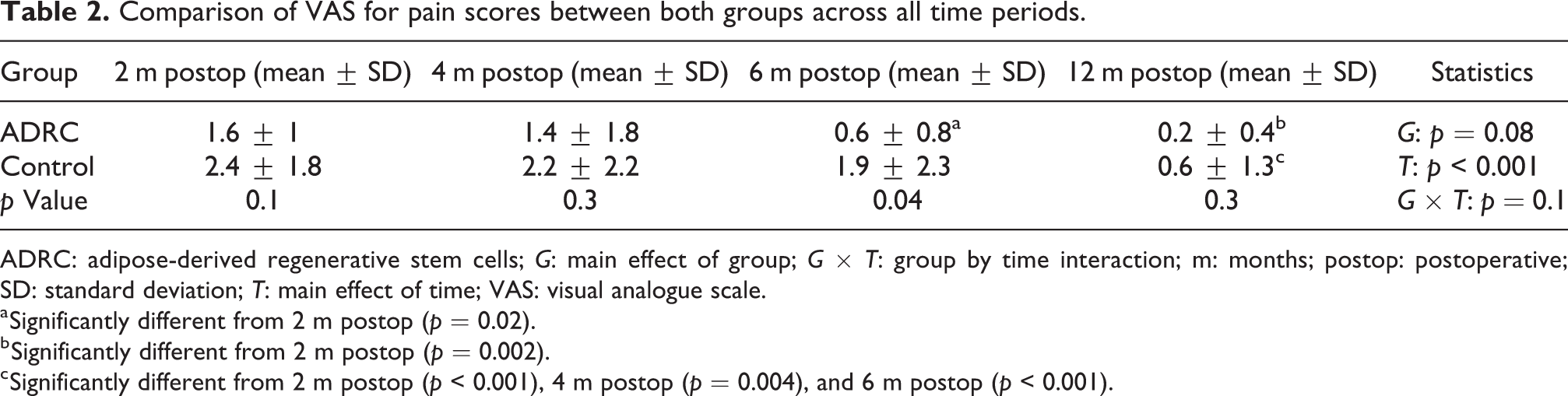
ADRC: adipose-derived regenerative stem cells; G: main effect of group; G × T: group by time interaction; m: months; postop: postoperative; SD: standard deviation; T: main effect of time; VAS: visual analogue scale.
a Significantly different from 2 m postop (p = 0.02).
b Significantly different from 2 m postop (p = 0.002).
c Significantly different from 2 m postop (p < 0.001), 4 m postop (p = 0.004), and 6 m postop (p < 0.001).
Figure 2 shows the differences in the Tegner activity scale between both groups across all time periods. The Tegner activity scale was significantly lower in the control group at all time periods (including baseline) compared to the ADRC group (p < 0.001) (Figure 2). There were no significant baseline to 12-month postop differences in the ADRC group (p > 0.05), whereas the 12-month postop Tegner activity scale score was significantly lower compared to the baseline in the control group (p = 0.006) (Figure 2). In addition, when considering the evolution of this score across all time periods, we found statistically significant differences between-groups (p ≤ 0.001). In the ADRC, 12 (60%) patients had equal and 8 (40%) patients had lower Tegner activity score in the 12 months postop compared to the baseline period. In the control group, 6 (31.6%) patients had equal and 13 (68.4%) patients had lower Tegner activity score in the 12 months postop compared to the baseline period.

Boxplot showing the Tegner activity scale in the ADRC and the control groups across the three time periods. *p ≤ 0.05; **p ≤ 0.01; ***p ≤ 0.001. †Significant between-group differences for each paired time periods (p ≤ 0.001). ADRC: adipose-derived regenerative stem cells; m: months; NS: non-significant; Pre: preoperative.
Figure 3 shows the comparison of the MRI score between both groups across all time periods. The 12 months postop MRI score was higher compared to the 2 months postop period in all patients from both groups. Both groups experienced a significant improvement in the 12 months compared to 2 months postoperative period (p ≤ 0.001). In fact, all within-group time comparisons were statistically significant in both groups (Figure 3). Patient in the control group had an overall worse improvement of 12 months compared to 2 months postoperative MRI scores, although this difference was not statistically significant (p = 0.4).

Boxplot showing the MRI score in the ADRC and the control groups across the four time periods. *p ≤ 0.05; **p ≤ 0.01; ***p ≤ 0.001. †Comparison of between-group differences for each paired time periods (p > 0.05). ADRC: adipose-derived regenerative stem cells; m: months; MRI: magnetic resonance imaging; NS: non-significant.
There were no major complications from the lipoaspirate or ACL surgery. One (5%) patient (from the ADRC) ruptured his ACL graft at 10 months after surgery playing soccer. The overall reinjury rate in this study was 2.5%.
Discussion
The principal finding of this study was that while patients receiving intraoperative administration of ADRC after ACL reconstruction significantly improved all the outcomes (pain scores, knee function, activity level, and MRI-based graft maturation) 12 months after surgery, this improvement was not significantly different compared to patients receiving ACL reconstruction without ADRC. Therefore, the use of intraoperative administration of ADRC is not justified to improve the healing or accelerate the functional recovery after ACL reconstruction. To the best of our knowledge, this is the first clinical study applying ADRC in ACL reconstruction.
Previous research using ADRC in ACL reconstruction has mainly involved animal studies. 29 –31 Teuschl et al. compared the degradation and regeneration potential (ligamentization) of ACL reconstruction with degradable silk fiber-based scaffold with or without ADRC in sheep. 29 Despite the authors observed better histological characteristics 6 months after surgery in the cell-seeded scaffold, there were no significant between-group differences in silk fiber degradation and tissue regeneration at 12 months. Kosaka et al. compared the tendon–bone healing (histologic and biomechanical study) in rabbits undergoing ACL reconstruction (using hamstring tendons) with or without the administration of ADRC. 30 The authors found an earlier formation of Sharpey-like fibers, greater ultimate failure load at 2 weeks, and greater stiffness at 6 weeks in the ADRC group, but biomechanical differences were no longer present at 8 and 12 weeks after surgery. Zhang et al. evaluated the effects of runx2-overexpressing (a powerful osteo-inductive factor) ADRC on the tendon-to-bone healing after ACL reconstruction in rabbits. 31 The authors observed that the runx2-overexpressing ADRC group had better histological characteristics and higher tendon pullout strength at 8 weeks after surgery compared to the control groups. However, it is unknown if these differences are maintained over time. Therefore, it seems that ADRC has provided an earlier graft healing and better biomechanical characteristics but that these differences could not be maintained over time. These studies have obvious methodological and outcome-related differences compared to our study, but we could not demonstrate that the ADRC group had earlier graft healing and maturation, or clearly greater clinical and functional outcomes.
Silva et al. have reported the only clinical study to date applying stem cells in ACL reconstruction. 20 The authors investigated whether the intraoperative, intra-graft, and intra-tunnel bone marrow-derived stem cells administration accelerated tendon-to-bone healing evaluated with MRI after ACL reconstruction using hamstring tendons. At 3 months after surgery, no differences in the signal-to-noise ratio of the interzone on MRI could be observed between patients with or without administration of bone marrow-derived stem cells. Interestingly, two patients (one in each group) underwent second-look arthroscopy and biopsies were obtained, which demonstrated no apparent differences in vascularity, and cellular and collagen content. 20 Again, there are obvious methodological differences between the study by Silva et al. and the present study, including the type of stem cells used, type of graft employed for ACL reconstruction, or the outcomes evaluated. Similarly, no significant between-group differences could be observed at any time point or across all time periods for MRI-based graft healing and maturation between patients receiving or not the ADRC in the present study. Both groups had similar improvement in the graft healing and maturation.
The automated cell processing system for obtaining the ADRC carried out in the present study (Celution® System) was chosen because of its reliability, reproducibility, and acceptance in the cell therapy community. The volume of fat that could be harvested from the patients in this study, who were in general elite athletes and had low body fat, was lower than that specified in the company’s protocol. The processing system was readjusted to work with a lower quantity of fat. This change did not alter the quality of the cells obtained. With the current methods and sample size, no clear clinical and functional difference could be demonstrated between both groups across time. Despite certain between-group differences (Tables 1 and 2), overall it cannot be considered that the ADRC clearly elicited better outcomes compared to the control group. With regard to graft healing and maturation, both groups showed a similar pattern: the maturation process started at 2 months after surgery, was greater between 4 and 6 months, and was completed at 12 months after surgery. The Tegner activity scale is the only outcome that demonstrated relevant between-group differences (Figure 2). However, the preoperative activity level was significantly different between groups, which not only entails potentially different physical characteristics but also likely different life motivations. This may explain why after surgery the patients in the control may be less motivated to reach the pre-injury activity level.
The present study has some limitations. First, this was not a randomized controlled trial, which entails a higher risk of selection bias. However, both groups were highly homogeneous in terms of the employed surgical technique, rehabilitation protocol, and patient characteristics (except for the baseline activity level). Second, the sample size was small. Third, MRI evaluations were only conducted by one non-blinded radiologist, which may imply a high risk of biased evaluations and prevents to calculation of interobserver reliability of the MRI readings of graft healing and maturation. In addition, gadolinium-enhanced MRI (helpful at considering graft healing and maturation) was only obtained for the ADRC group, so no comparison with the control group could be possible for this imaging technique. However, the present study is the first to date to investigate the use of ADRC after ACL reconstruction, providing both imaging and clinical/functional outcomes.
Further research
The use of stem cells to enhance healing and accelerate the recovery after ACL reconstruction is still in the beginnings. There is very little research conducted to date, and robust conclusions about its efficacy cannot still be elaborated. It might be possible that the inclusion of groups with larger sample size changes the main conclusions, particularly if we take into account that the outcomes of ACL reconstruction alone (control group) are, in general, excellent. This makes difficult to find significant differences between groups.
Conclusions
While patients receiving intraoperative administration of ADRC after ACL reconstruction significantly improved all the outcomes (pain scores, knee function, activity level, and MRI-based graft maturation) 12 months after surgery, this improvement was not significantly different compared to patients receiving ACL reconstruction without ADRC. Therefore, the use of intraoperative administration of ADRC is not justified to improve the healing or accelerate the functional recovery after ACL reconstruction at this point.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.