
Abstract
Background:
Platelet-rich plasma (PRP) and patch augmentation (PA) are 2 adjuncts that are used in the context of rotator cuff repair (RCR) to strengthen the repair construct and promote healing.
Purpose:
To systematically review the literature to compare the clinical efficacy of RCR with PA versus RCR with PRP.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
A systematic review was performed by searching the PubMed, Cochrane Library, and Embase databases to identify Level 1 and 2 studies that compared the clinical efficacy of RCR alone with RCR with PRP or RCR with PA. The search phrase used was as follows: rotator cuff repair AND (patch OR augmentation OR bioinductive OR implant OR PRP OR platelet-rich plasma OR platelet-rich plasma). Patients were assessed based on the visual analog scale for pain, the Constant-Murley score, the American Shoulder and Elbow score, the University of California Los Angeles shoulder score, range of motion (ROM), and retear rates.
Results:
A total of 27 studies (Level 1 or 2) met the inclusion criteria, including 342 patients undergoing RCR with PA (mean age, 60 years) and 547 patients undergoing RCR with PRP (mean age, 58.1 years). The mean follow-up was 20.6 months in the PA group and 22.2 months in the PRP group. Among all patient-reported outcomes and ROM measures, there were no significant differences in weighted improvements between the 2 groups from pre- to postoperatively. However, patients undergoing RCR with PRP (13.1%) demonstrated significantly lower retear rates at the latest follow-up when compared with patients undergoing RCR with PA (18.4%) (P = .04).
Conclusion:
Patients undergoing RCR with PRP may experience lower retear rates when compared with patients undergoing RCR with PA. Patients in both groups can be expected to experience similar improvements in both patient-reported and functional outcomes, although further randomized studies are needed to directly compare these 2 groups.
Rotator cuff tears are a common shoulder injury resulting in pain, weakness, and shoulder dysfunction, with a prevalence rate of around 20% in the population.36,50,72 In the United States, rotator cuff repair (RCR) is one of the most common orthopaedic surgeries, with approximately 200,000 to 250,000 RCRs performed annually, with an increasing frequency among patients aged 50 to 64 years.20,47,73 RCR has been shown to significantly improve functional outcomes and patient satisfaction and is the standard of care for surgical repair of the rotator cuff.35,47,68 However, retear rates have varied greatly, ranging between 9% and 94%.17,22,25,27,30,38,39,43,65 In recent years, multiple adjuncts to RCR have been used in an attempt to improve outcomes and lower retear rates, with patch augmentation (PA) and platelet-rich plasma (PRP) being 2 of the most popular adjuncts.
PA during RCR has been increasing in popularity, particularly for large and massive tears. 5 A patch can be made of various biological degradable and nondegradable materials and is placed over the repaired rotator cuff tendon as a mechanical support to enhance the repair construct. 45 Depending on the materials utilized, PA can promote vascularization and cellular growth, encouraging tendon-to-bone healing, as it infiltrates tissue cells at the repair site.1,13,16,24 The increasing popularity of PA during RCR is supported by multiple studies demonstrating lower retear rates and improved clinical outcomes in patients undergoing RCR with PA versus RCR alone.10,23,53 Similarly, PRP is another biological option used to enhance tendon healing for RCR as an autologous derivative of whole blood rich with growth factors.2,46,63 Previous studies have also found RCR with PRP augmentation to demonstrate improved clinical outcomes and lower retear rates when compared with RCR alone.40,42,64,67 However, to our knowledge, the superiority of PA versus PRP in the setting of RCR has not been studied. This study aimed to systematically review the literature to compare the efficacy and safety of RCR with PA and RCR with biological augmentation of PRP. The authors hypothesized that there would be no difference in outcomes and retear rates among patients undergoing RCR with PA versus patients undergoing RCR with PRP.
Methods
This systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using a PRISMA checklist. Two independent reviewers (J.W.B. and J.J.L.) searched the PubMed, Embase, and Cochrane Library databases up to June 7, 2024. The electronic search strategy used was as follows: rotator cuff repair AND (“patch” OR “augmentation” OR “bioinductive” OR “implant” OR “PRP” OR “platelet-rich plasma” OR “platelet-rich plasma”). A total of 597 studies were reviewed by title and/or abstract to determine study eligibility based on the inclusion criteria. In cases of disagreement, a third reviewer (E.C.M.) made the final decision. The inclusion and exclusion criteria followed the participants, interventions, comparators, outcomes, and study design strategy. Studies selected for inclusion met the following criteria: (1) participants: patients undergoing arthroscopic RCR; (2) intervention: PA or PRP augmentation; (3) comparator: no augmentation; (4) outcomes: clinical efficacy and adverse events; (5) study design: Level 1 and 2 randomized controlled trials (RCTs) that were published in English. The exclusion criteria included Level 3 to 5 studies that did not meet the aforementioned inclusion criteria and studies that did not have a minimum of 1-year follow-up. A total of 27 studies were determined to meet the inclusion criteria (Figure 1). Data extraction from each study was performed independently and then reviewed by a second author (J.W.B.). There was no need for funding or a third party to obtain any of the collected data. Risk of bias was assessed according to the Cochrane Collaboration risk of bias tool, 29 which incorporates an assessment of randomization, blinding, completeness of outcomes data, selection of outcomes reported, and other sources of bias.

A PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Reporting Outcomes
Outcomes assessed included patient-reported outcomes (PROs). PROs included the visual analog scale (VAS) for pain, the Constant-Murley (CM) score, 21 the American Shoulder and Elbow Surgeons (ASES) score, 58 and the University of California Los Angeles (UCLA) shoulder score. 3 Additional outcomes assessed included ROM and rotator cuff retear rates. Twelve studies used the VAS, in which all scores were standardized to a 100-point scale (PA: 4 studies4,11,32,37; PRP: 8 studies34,44,54,57,60,74 -76). Twenty studies used the CM score (PA: 9 studies4,6,9,10,11,37,41,61,66; PRP: 11 studies12,26,28,34,44,54,56,57,74 -76). Fourteen studies used the ASES score (PA: 7 studies7,9,11,37,41,61,66; PRP: 7 studies26,34,54,57,59,60,70). Eleven studies reported results of the UCLA shoulder score (PA: 3 studies6,10,37; PRP: 8 studies34,44,54,56,57,62,70,74). Seven studies reported on range of motion (ROM), specifically in external rotation (PA: 3 studies9,32,37; PRP: 4 studies34,57,75,76). A total of 25 studies reported on rotator cuff retear rates (PA: 10 studies6,9 -11,31,32,37,41,61,66; PRP: 15 studies ‡ ).
Study Methodology Assessment
The Modified Coleman Methodology Score (MCMS) 18 was used to evaluate study methodology quality. The MCMS has a scaled potential score ranging from 0 to 100. Scores ranging from 85 to 100 are excellent, 70 to 84 are good, 55 to 69 are fair, and <55 are poor. The primary outcomes assessed by the MCMS are study size and type, follow-up time, attrition rates, number of interventions per group, and proper description of study methodology.
Statistical Analysis
A weighted mean was calculated for numerical demographic characteristics (age, follow-up, and sex) and the percent improvement of PROs separated by augmentation type. Weighted means are necessary to accurately capture study data, accounting for each study’s variability in size; therefore, unweighted means would present skewed values. In the cases where standard deviations were not provided,9,11,62,76 a quarter of the mean was used as the standard deviation, as previously described.
71
Chi-square tests were used to calculate statistical significance for rotator cuff retear rate data between the groups. To compare the postoperative percent improvements between groups for PROs and ROM, a 2-sample weighted t test was used from the weights package in R (CRAN).
55
Weights were calculated as
Results
A total of 27 studies met the inclusion and exclusion criteria (Figure 1), including a total of 889 patients (PA = 342 patients; PRP = 547 patients). The mean patient age at the time of repair was 60 and 58.1 years in the PA and PRP groups, respectively, and the mean follow-up time was 20.6 months in the PA group and 22.2 months in the PRP group (Table 1). The percentage of male patients was 53.8% and 47.6% in the PA and PRP groups, respectively.
Studies Included a
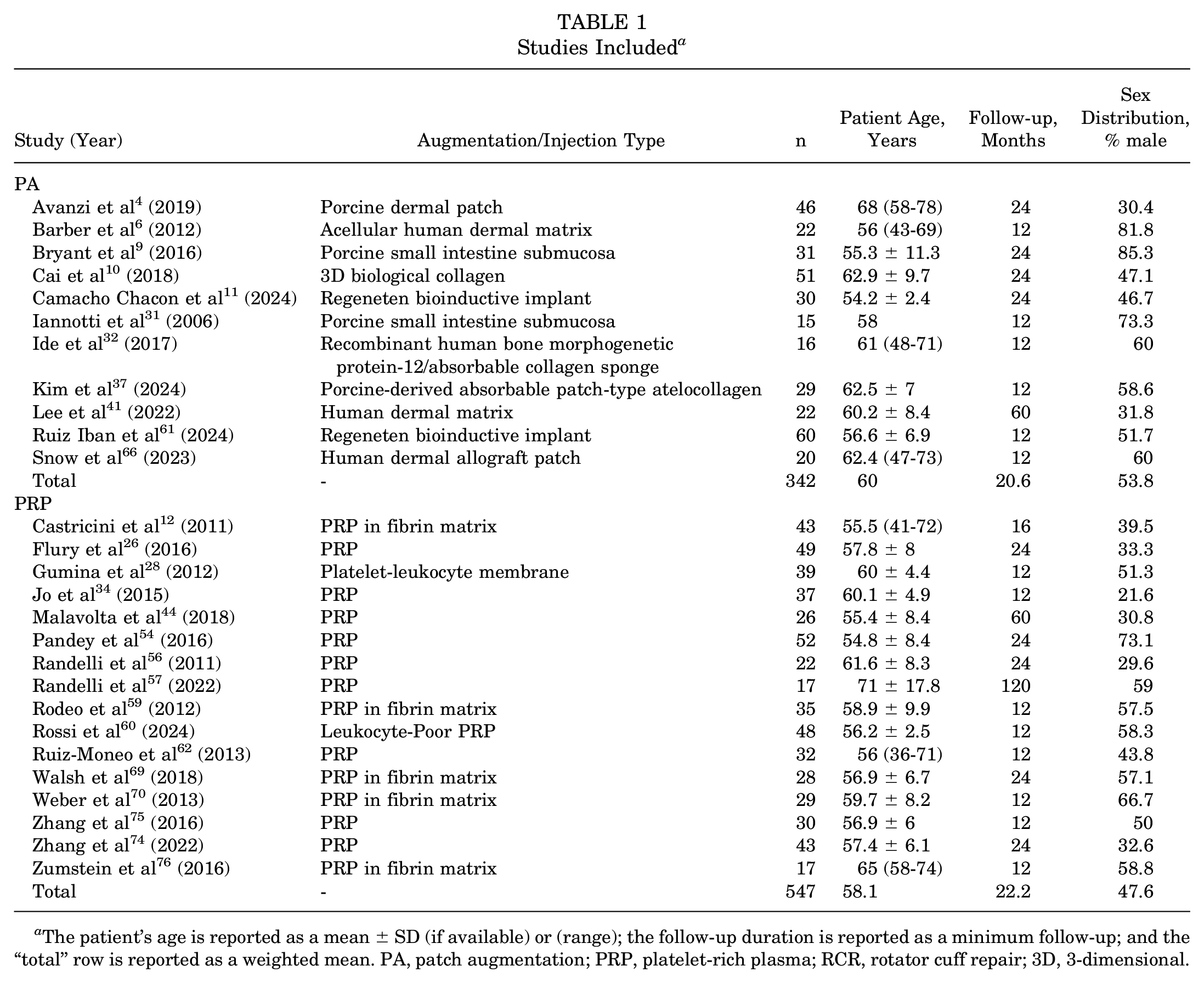
The patient’s age is reported as a mean ± SD (if available) or (range); the follow-up duration is reported as a minimum follow-up; and the “total” row is reported as a weighted mean. PA, patch augmentation; PRP, platelet-rich plasma; RCR, rotator cuff repair; 3D, 3-dimensional.
PRP Preparation and Administration Method
Fourteen studies (87.5%) described details of PRP preparation. § Specific machines or processing kits used for PRP preparation were highly variable but were reported as a centrifugation system or a plateletpheresis system in all studies. In 13 studies (81.3%), blood was drawn from the peripheral antecubital vein, and the spin details of the centrifugation to isolate the red blood cells from the upper plasma layer were described. ‖ In 8 studies (50%), the supernatant layer was transferred to a new centrifuge tube for a second centrifugation to separate the platelet-poor plasma layer from the PRP layer,12,56,57,59,60,69,74,75 of which 7 studies reported these second spin details.12,56,57,60,69,74,75 In 12 studies ¶ (75%), the PRP was then activated by adding calcium chloride12,44,54,56,57,59,62,69,74,75 or calcium gluconate28,34 before injection, while 1 study 26 reported no activation. In 6 studies (37.5%), platelet concentration was between 1.7 and 7.7 times baseline values.28,34,44,54,56,57 Ten studies (62.5%) did not report on the final injected platelet concentration.12,26,56,57,59,62,69,70,75,76 All studies utilized RCR with PRP administered PRP intraoperatively only, meaning no studies included patients who also received additional injections postoperatively.
Tear Type
Five studies included patients with small or medium rotator cuff tears.4,11,12,44,60 Three studies included patients with small to large tears.57,59,62 Two studies included patients with small to massive tears.26,56 One study included patients with medium tears only. 54 Ten studies included patients with medium or large tears.9,10,28,32,34,37,61,66,69,74 One study included patients with medium to massive tears. 75 Two studies included patients with large tears only.6,41 One study included patients with large or massive tears. 31 One study included patients with massive tears only. 76 One study did not report the tear size inclusion criteria but reported the tear size mean of its PRP group to be 1.77 cm, characterizing it as a medium tear 70 (Table 2).
Tear Size Included a
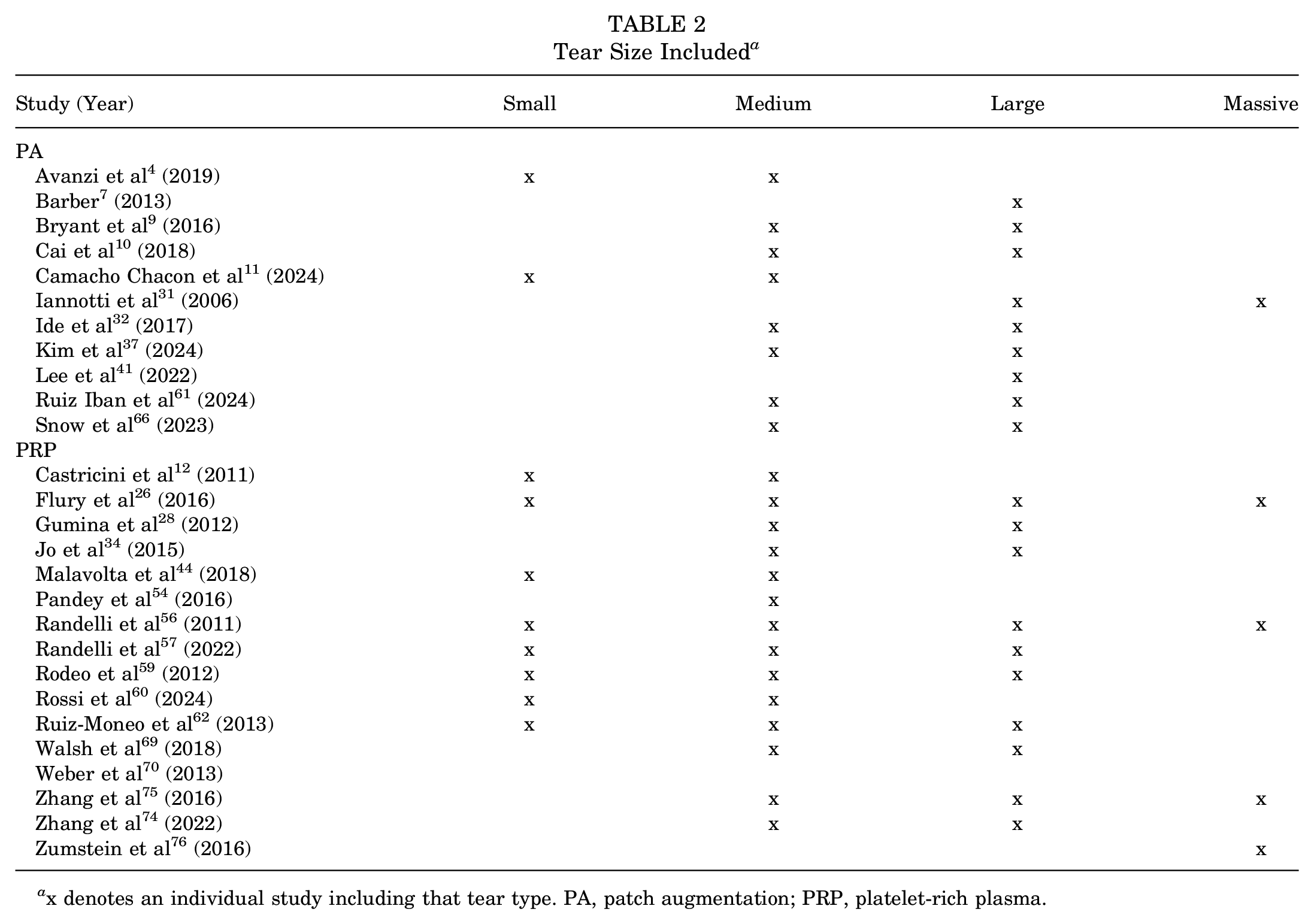
x denotes an individual study including that tear type. PA, patch augmentation; PRP, platelet-rich plasma.
Modified Coleman Methodology Score
Table 3 shows the MCMS scores from the 27 included studies. A total of 20 studies # received excellent scores, and 7 studies4,12,31,32,59,66,70 received good scores.
Modified Coleman Methodology Scores a
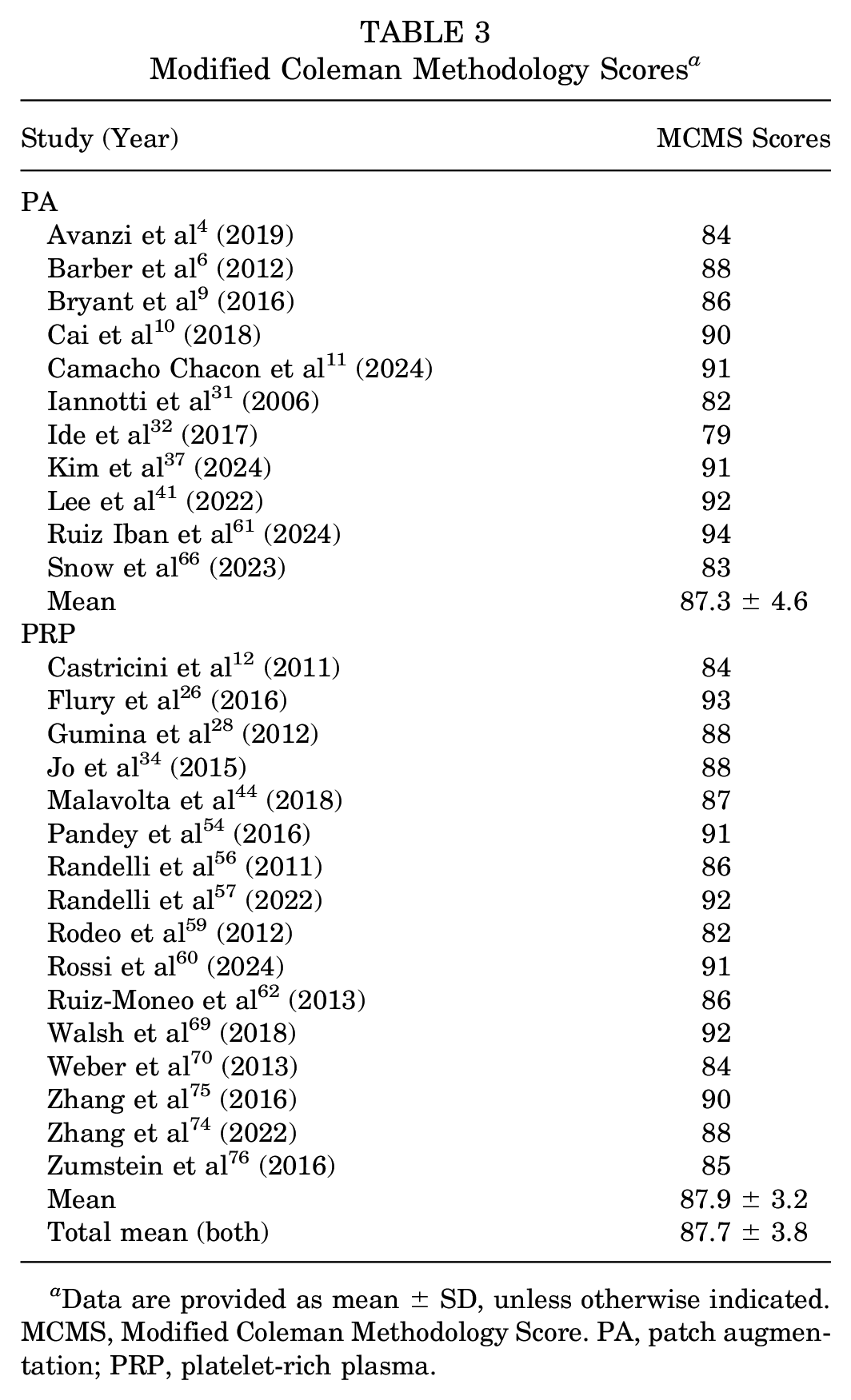
Data are provided as mean ± SD, unless otherwise indicated. MCMS, Modified Coleman Methodology Score. PA, patch augmentation; PRP, platelet-rich plasma.
Methodologic Quality Assessment
The results of the methodologic quality assessment of included studies using the Cochrane Collaboration risk of bias tool are presented in Figure 2. Sequence generation was adequately reported by all studies (low risk of bias). In all studies, concealment of allocation from the investigators was not possible because of the nature of the intervention (high risk of bias). All studies were deemed to be at low risk for detection bias because of the blinding of the outcome assessor, except in 3 studies in which the outcome assessor was not blinded (high risk of bias).41,75,76 Patients in most studies were blinded to their intervention group (low risk of bias), except in 9 studies in which patients were aware of their treatment group (high risk of bias).6,10,12,28,31,32,34,75,76 Seven studies reported a minor loss of follow-up between 10% and 20% without proper explanation (unclear risk of bias), while no other studies reported significant loss of follow-up (low risk of bias).4,41,56,57,59,69,74

Risk of bias graph. Risk of bias is presented as a percentage across all included studies (green, low risk; yellow, unclear; red, high risk).
Patient-Reported Outcomes
Twelve studies used the VAS, in which all scores were standardized to a 100-point scale (PA: 4 studies4,11,32,37; PRP: 8 studies34,44,54,57,60,74 -76) (Table 4). Of the 4 studies utilizing RCR with PA, 3 studies (75%) reported P values on pre- to postoperative scores.4,11,37 All 3 studies found patients receiving RCR with PA to report significantly less pain from preoperative to the latest follow-up. Of the 8 studies utilizing RCR with PRP augmentation, 6 studies (75%) reported P values on pre- to postoperative scores.44,54,60,74 -76 All 6 studies found that patients receiving RCR with PRP reported significantly less pain from preoperative to the latest follow-up. There was no significant difference between groups when comparing the percent weighted improvement from pre- to postoperatively (P = .75).
VAS Scores for Pain Severity a
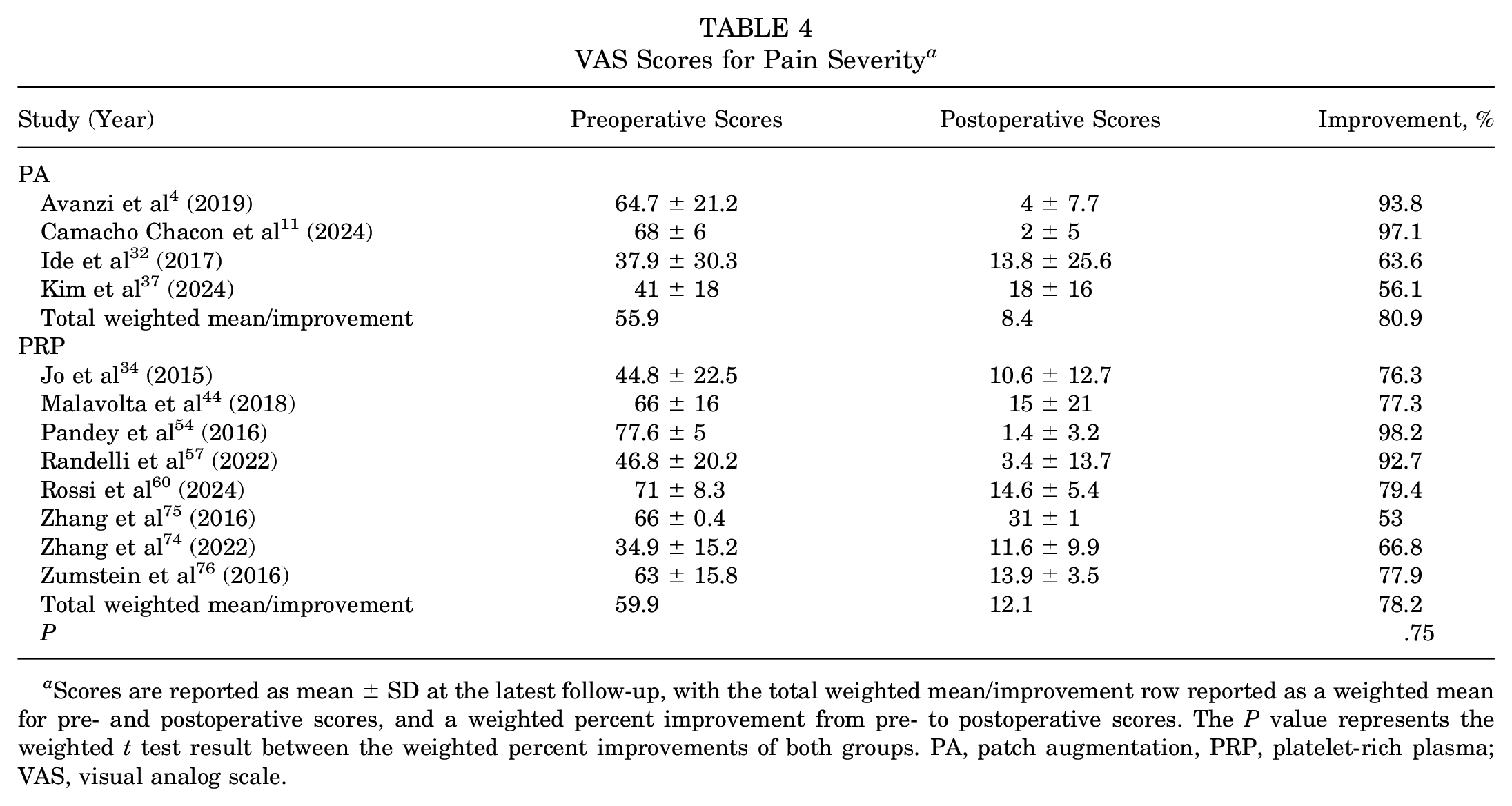
Scores are reported as mean ± SD at the latest follow-up, with the total weighted mean/improvement row reported as a weighted mean for pre- and postoperative scores, and a weighted percent improvement from pre- to postoperative scores. The P value represents the weighted t test result between the weighted percent improvements of both groups. PA, patch augmentation, PRP, platelet-rich plasma; VAS, visual analog scale.
Twenty studies used the CM score (PA: 9 studies4,6,9,10,11,37,41,61,66; PRP: 11 studies 12,26,28,34,44,54,56,57,74 -76) (Table 5). Of the 9 studies utilizing RCR with PA, 6 studies (66.7%) reported P values on pre- to postoperative scores.4,10,11,37,41,61 All 6 studies found that patients receiving RCR with PA improved significantly from preoperative to the latest follow-up. Of the 11 studies utilizing RCR with PRP, 9 studies (81.8%) reported P values on pre- to postoperative scores.12,26,34,44,54,56,74 -76 All 9 studies found that patients receiving RCR with PRP improved significantly from preoperative to the latest follow-up. One study 61 did not report postoperative CM scores, and 1 study 11 did not report mean pre- and postoperative CM scores but instead median scores; therefore, the percent improvement was not calculated for these studies and was not accounted for in the total weighted improvement calculation. There was no significant difference between groups when comparing the percent weighted improvement from pre- to postoperatively (P = .98).
Constant-Murley Scores a

Scores are reported as mean ± SD at the latest follow-up, with the total weighted mean/improvement row reported as a weighted mean for pre- and postoperative scores, and a weighted percent improvement from pre- to postoperative scores. The P value represents the weighted t test result between the weighted percent improvements of both groups. NR, not reported; PA, patch augmentation; PRP, platelet-rich plasma.
Fourteen studies used the ASES score (PA: 7 studies6,9,11,37,41,61,66; PRP: 7 studies 26,34,54,57,59,60,70) (Table 6). Of the 7 studies utilizing RCR with PA, 4 studies (57.1%) reported P values on pre- to postoperative scores.11,37,41,61 All 4 studies found that patients receiving RCR with PA reported better ASES scores from preoperatively to the latest follow-up. Of the 7 studies utilizing RCR with PRP, 4 studies (57.1%) reported P values on pre- to postoperative scores.26,34,54,60 All 4 studies found that patients receiving RCR with PRP reported better ASES scores from preoperative to the latest follow-up. In total, 2 studies57,70 did not report preoperative ASES scores, 1 study 61 did not report postoperative ASES scores, and 1 study 11 did not report mean pre- and postoperative ASES scores but instead reported median scores; therefore, the percent improvement was not calculated for these studies and was not accounted for in the total weighted improvement calculation. There was no significant difference between groups when comparing the percent weighted improvement from pre- to postoperatively (P = .26).
American Shoulder and Elbow Surgeons Scores a

Scores are reported as mean ± SD at the latest follow-up, with the total weighted mean/improvement row reported as a weighted mean for pre- and postoperative scores, and a weighted percent improvement from pre- to postoperative scores. The P value represents the weighted t test result between the weighted percent improvements of both groups. NR, not reported; PA, patch augmentation; PRP, platelet-rich plasma.
Eleven studies reported results of the UCLA shoulder score (PA: 3 studies6,10,37; PRP: 8 studies34,44,54,56,57,62,70,74) (Table 7). Of the 3 studies utilizing RCR with PA, 2 studies (66.7%) reported P values on pre- to postoperative scores.10,37 Both studies found that patients receiving RCR with PA reported better UCLA shoulder scores from preoperative to the latest follow-up. Of the 8 studies utilizing RCR with PRP, 4 studies34,44,54,74 (50%) reported P values on pre- to postoperative scores. All 4 studies found patients receiving RCR with PRP to report better UCLA shoulder scores from preoperative to the latest follow-up. One study did not report preoperative UCLA shoulder scores; therefore, the percent improvement was not calculated and was not accounted for in the total weighted improvement calculation. 70 There was no significant difference between groups when comparing the percent weighted improvement from pre- to postoperatively (P = .78).
University of California Los Angeles Shoulder Scores a

Scores are reported as mean ± SD at the latest follow-up, with the total weighted mean/improvement row reported as a weighted mean for pre- and postoperative scores, and a weighted percent improvement from pre- to postoperative scores. The P value represents the weighted t test result between the weighted percent improvements of both groups. NR, not reported; PA, patch augmentation; PRP, platelet-rich plasma.
Seven studies reported ROM, specifically in external rotation (PA: 3 studies9,32,37; PRP: 4 studies34,57,75,76) (Table 8). Of the 3 studies utilizing RCR with PA, 1 study (33.3%) reported P values on pre- to postoperative ROM. 37 This study found that patients receiving RCR with PA reported improved external rotation from preoperative to the latest follow-up. Of the 4 studies utilizing RCR with PRP, 3 studies34,75,76 (75%) reported P values on pre- to postoperative ROM, 275,76 of which found that patients receiving RCR with PRP reported improved external rotation from preoperative to the latest follow-up. One study 57 did not report preoperative external rotation ROM; therefore, the percent improvement was not calculated and was not accounted for in the total weighted improvement calculation. There was no significant difference between groups when comparing the percent weighted improvement from pre- to postoperatively (P = .20).
External Rotation Assessment a

Scores are reported as mean ± SD at the latest follow-up, with the total weighted mean/improvement row reported as a weighted mean for pre- and postoperative scores, and a weighted percent improvement from pre- to postoperative scores. The P value represents the weighted t test result between the weighted percent improvements of both groups. NR, not reported; PA, patch augmentation; PRP, platelet-rich plasma.
Rotator Cuff Retear Rates
A total of 25 studies reported rotator cuff retear rates (PA: 10 studies6,9 -11,31,32,37,41,61,66; PRP: 15 studies ** ) (Table 9). Overall, 18.4% of patients undergoing RCR with PA experienced rotator cuff retear compared with 13.1% of patients undergoing RCR with PRP (P = .04).
Rotator Cuff Retear Rates a

Retears are reported as the number of retears/total number of patients (%). PA, patch augmentation; PRP, platelet-rich plasma.
Discussion
Despite the highly positive long-term clinical outcomes of patients undergoing RCR, there has been an increasing popularity of utilizing novel augments and materials to promote healing and lower the failure rate of the repair. As a result, PA and PRP have garnered interest as RCR augmentation options with their inherent biological potential to promote healing. Both augmentation techniques have demonstrated improved clinical outcomes and lower retear rates when compared with RCR without augmentation. However, the superiority of one adjunct over the other has not been adequately investigated. There are no studies to date that directly compare the clinical outcomes and retear rates of patients undergoing RCR with PA with those undergoing RCR with PRP. Therefore, with similar improvements found in studies evaluating these augmentations in the setting of RCR separately, the authors hypothesized that there would be no difference in outcomes between patients undergoing RCR with PA versus patients undergoing RCR with PRP.
The present systematic review is, to our knowledge, the first review to compare clinical and PROs in patients undergoing RCR with PA versus patients undergoing RCR with PRP. The results of this systematic review suggest that patients undergoing RCR with PRP can be expected to experience lower retear rates when compared with patients undergoing RCR with PA. These results may in part be explained by the introduction of concentrated platelet alpha-granules that possess and release growth factors, stimulating healing within the repair site.7,15,19,49 The biologically active components of PRP are thought to contribute to the healing of damaged blood vessels by revascularizing and helping form new connective tissue, thereby regenerating torn tendon tissue. 49 In RCR with PRP, the repair site is actively supported in its healing process. In the context of PA, patches may act as more of a mechanical or structural supporter and provide fewer biological healing properties when compared with PRP. In addition, the more autologous nature of PRP may be advantageous in that it serves as more of an individualized healing agent rather than a general patch made synthetically or derived from animal tissue. Consequently, PRP may have several important biological advantages over patches that should be considered when approaching RCR patients who may need additional augmentation.
However, it is important to note the limitations surrounding the clinical use of PRP in RCR, despite the observed benefits. The Food and Drug Administration categorizes PRP as an autologous blood product and approves of the equipment utilized to produce PRP, thereby making it easier to implement clinically. Along with the lack of regulatory obstacles before clinical application, this ease of utilization resulted in a notable surge in the use of PRP as a treatment for musculoskeletal pathologies. However, the PRP injection procedures themselves are still considered investigational and are currently not approved and covered by most insurance carriers, thus requiring expensive personal payments by the patients, who can reach up to thousands of dollars. Therefore, understanding the significant cost most patients will have to pay out-of-pocket when utilizing PRP as an augmentation to RCR is important for both the physician and the patient to consider, despite the findings of the current systematic review favoring RCR with PRP. Another important consideration regarding PRP use in RCR is the knowledge of the variability in PRP protocols and composition because of its lack of standardization, which results in a heterogeneity of the PRP utilized as an augmentation during RCR that may result in differing outcomes.
Occasionally, clinical outcomes do not correlate as expected with tendon appearance on imaging, especially with larger tears. 16 It has been observed that some patients who experience retears or failure of the repair still experience improved ROM and function.14,27,33,48 These functional outcomes, however, have been shown to deteriorate over time, and patients with an unhealed rotator cuff after repair eventually experience worse outcomes compared with patients whose tendons heal completely after repair.8,51,52 Therefore, it is important to maximize tendon healing potential to maximize function and minimize pain for patients undergoing RCR with PRP or PA.
In all the PROs and ROM measures analyzed in this systematic review, there was no superiority of one group over another in any instance. When evaluating each group independently, both treatment groups demonstrated excellent improvements from pre- to postoperatively, and to a similar degree. Out of the 26 cases where studies with RCR with PRP patients reported on pre- to postoperative scores, 25 (96.2%) found patients to significantly improve from preoperative to the latest follow-up. Similarly, all 16 (100%) with RCR with PA patients found that patients improved significantly from preoperative to the latest follow-up. These results confirm the beneficial properties of both augmentation options compared with RCR alone. However, future randomized studies are needed to directly compare RCR with PRP and RCR with PA to determine whether one treatment type is superior to another.
The strengths of this study include a comprehensive systematic review of Level 1 and Level 2 studies performed by 2 independent reviewers. The limitations of this study should also be noted. Among the 27 studies included, only 15 were Level I evidence. There were no studies directly comparing clinical outcomes of RCR with PA and RCR with PRP; therefore, a meta-analysis of the literature could not be performed. The studies differed regarding surgical techniques, follow-up periods, rehabilitation protocols, and grade of tears for included patients. Because of the high variability in the tear type included among studies, a subanalysis categorizing results by tear type could not be performed. In addition, there was high variability in the composition and preparation of PRP, as well as patch type, which similarly prevented a subanalysis on this topic from being performed. Follow-up times were also variable between study groups. Overall, the heterogeneous nature of these studies serves as a confounding factor in the comparison of these 2 treatment groups.
Conclusion
Patients undergoing RCR with PRP may experience lower retear rates when compared with patients undergoing RCR with PA. Patients in both groups can be expected to experience similar improvements in both patient-reported and functional outcomes, although further randomized studies are needed to directly compare these 2 groups.
Footnotes
Final revision submitted January 29, 2025; accepted April 17, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.M. has received publishing royalties and financial or material support from Elsevier; has received research support from Arthrex, Breg, Ossur, and Smith & Nephew; has received speaking fees from Vericel; and has received royalties and consulting fees from Zimmer. R.M.F. has received consulting fees from Allosource, Arthex, and JRF; has received speaking fees from Allosource, Arthrex, JRF, and Ossur; has received research support from Arthrex and Smith & Nephew; and has received publishing royalties and financial or material support from Elsevier. J.T.B. has received research support from Biomet and Stryker; has received other financial or material support from Mitek, Smith & Nephew, and Stryker; has received intellectual property (IP) royalties from Shukla Medical; is an unpaid consultant for Shukla Medical; and has received consulting fees from DJ Orthopaedics and Smith & Nephew. A.J.S. is a paid consultant for DJ Orthopaedics. E.C.M. has received research support from Arthrex, Breg, DJ Orthopaedics, Mitek, Ossur, and Smith & Nephew; IP royalties from Biomet and Zimmer; consulting fees from Biomet and Bioventus; publishing royalties and financial or material support from Elsevier; and speaking fees from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.