
Abstract
Background:
While the relationship between obesity and adverse outcomes after anterior cruciate ligament (ACL) reconstruction has been studied, the relationship remains unclear due to conflicting reports from the existing literature.
Purpose/Hypothesis:
The purpose was to assess the correlation of obesity with 90-day complications, readmissions, and 5-year retearing rates after ACL reconstruction using a large national cohort of patients. It was hypothesized that obesity would be associated with increased odds of adverse outcomes after ACL reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The PearlDiver Mariner M165Ortho patient claims database (2010-2022) was used to identify patients who underwent ACL reconstruction. Obese (body mass index, ≥30 kg/m2) and nonobese patients were matched 1:1 based on age, sex, and comorbidity burden (Elixhauser Comorbidity Index). Outcomes included 90-day adverse events and readmission, which were assessed by univariate and multivariate analyses. Five-year rates of ipsilateral ACL retearing and contralateral ACL tearing were also assessed and compared with log-rank tests.
Results:
A total of 172,673 patients were identified, with obesity noted in 28,047 (16.2%). After matching the obese and nonobese cohorts, there were no differences in age, sex, or ECI between the 2 cohorts (P > .05 for all). Multivariate analysis showed that obesity was independently associated with increased odds of any adverse event (OR, 3.08; P < .001), serious adverse events (OR, 2.19; P < .001), and readmissions (OR, 6.40; P < .001). Specific complications linked to obesity included higher odds of the following, in decreasing odds ratio order: pneumonia (OR, 5.98), urinary tract infections (OR, 4.51), pulmonary embolism (OR, 3.97), sepsis (OR, 3.71), wound dehiscence (OR, 3.34), acute kidney injury (OR, 3.02), deep vein thrombosis (OR, 2.18), and surgical site infection (OR, 2.03) (P < .001 for all correlations). Over 5 years, there were no significant differences in the rates of ipsilateral or contralateral ACL tears between obese and nonobese patients (P = .5 and P = .6, respectively).
Conclusion:
In a large cohort of patients, obesity was found to be associated with significantly increased odds of 90-day complications and readmissions after ACL reconstruction. Nonetheless, obesity was not correlated with 5-year rates of ipsilateral ACL retearing or contralateral ACL tearing after ACL reconstruction.
Anterior cruciate ligament (ACL) reconstruction is a common procedure aimed at restoring knee stability and function, particularly in active individuals. 31 Despite advancements in surgical techniques and patient management, there remains a risk of postoperative complications, readmissions, and retearing, on either the same side due to graft failure or the opposite side, especially with high-activity sports.13,27,32,37,40,42 Understanding the patient-related factors that contribute to these adverse outcomes is essential for optimizing patient care.
Obesity, characterized by a body mass index (BMI) of 30 kg/m2 or higher, has emerged as a risk factor for inferior outcomes across a variety of surgical fields.1,5,16,25,47 The metabolic and systemic effects of obesity, including chronic inflammation, impaired immune function, and delayed wound healing, may increase the risk of medical complications and hinder recovery.15,19,21,33,35 Furthermore, in the context of ACL reconstruction, elevated BMI may impose additional mechanical stress on the knee joint and native or grafted ACL.4,7,34,37
Several studies have indicated that obesity contributes to an increased risk of primary ACL tears3,6 as well as a higher severity of the injury. 4 However, few studies have investigated postoperative outcomes after ACL reconstruction in obese patients, and their findings have been mixed. Some studies showed no differences in ACL reconstruction outcomes between individuals with and without obesity,8,14,22,46 while others have found worse outcomes for patients with obesity compared to those without.9,12,36,38,41,45
Given the limited and conflicting literature, this study analyzed a national database to examine complications, readmissions within 90 days postoperatively, and the incidence of retearing over a 5-year period after ACL reconstruction. By providing robust, large-scale data on how obesity correlates these outcomes, this research aims to inform clinical decision-making, highlight the need for potential modifications in perioperative care, and ultimately improve the management and prognosis of obese patients undergoing ACL reconstruction.
Methods
Study Cohorts
The current study used the 2010 to 2022 M165Ortho PearlDiver Mariner patient claims database (PearlDiver Technologies). This national administrative data set is widely used in orthopaedic research.2,18,24,43,44 Our institutional review board has deemed PearlDiver studies exempt from review because all data are de-identified and presented in aggregate form.
Patients who underwent primary ACL reconstruction were identified using Current Procedural Terminology code 29888. Patients were excluded if they were <18 years of age; had concurrent neoplasms, trauma, or infections; or had <90 days of follow-up. Patients were also excluded if they underwent same-day posterior cruciate ligament, medial collateral ligament, or lateral collateral ligament reconstruction, as well as any other same-day knee procedures.
Patients with obesity were identified using the International Classification of Diseases (ICD) Revision 9 and 10, diagnosis codes for BMI, with obesity defined based on a BMI threshold ≥30 kg/m2. A 1:1 matching process was implemented between the obese and nonobese groups, considering age, sex, and the Elixhauser Comorbidity Index (ECI).
Adverse Events and Outcome Metrics
Using ICD-9 and ICD-10 coding, we identified 90-day adverse events, with occurrences monitored both independently and as aggregate groups. This approach is consistent with previous literature studying adverse events after orthopaedic procedures in PearlDiver.11,23,28,30
An aggregated serious adverse event was recorded if any of the following occurred: surgical site infection, sepsis, deep vein thrombosis, or pulmonary embolism. An aggregated minor adverse event was recorded if any of the following occurred: acute kidney injury, pneumonia, urinary tract infection, wound dehiscence, hematoma, or transfusion.
Additionally, readmissions, identified through the PearlDiver “ADMISSION” function, were tracked for 90 days after surgery.
Five-year outcome metrics included retearing rates of ipsilateral and contralateral ACL. Laterality was determined by identifying ACL tear diagnoses using ICD-9 and ICD-10 codes within 1 year before surgery. If a diagnostic code for an ACL tear was present for one side but absent for the other within 1 year before ACL reconstruction, it was assumed that the ACL reconstruction was performed on the side with the documented tear. ICD-9 and ICD-10 codes for ACL tears were monitored over a 5-year period after surgery to identify tears occurring on the same side (ipsilateral) or the opposite side (contralateral) of the knee that was initially operated on. Notably, patients with ICD-9 codes lacking laterality were excluded from the current analysis.
Statistical Analysis
The demographics of patients who underwent ACL reconstruction were compared between obese and nonobese patients. Differences in the categorical variable sex distribution were assessed using chi-square tests, while differences in numeric variables such as age and ECI were assessed using t tests. Such comparisons were made before and after 1:1 matching.
Adverse events were compared between the obese and nonobese groups using univariate t tests. Multivariate analysis was then performed, controlling for age, ECI, and sex.
Significance in both univariate and multivariate analyses was adjusted for multiple comparisons using the Bonferroni correction, with significance defined as a P value <.003.
Ipsilateral ACL retearing and contralateral ACL tearing within 5 years after surgery were compared between obese and nonobese patients using Kaplan-Meier survival analysis. Results were compared using the log-rank test.
All statistical analyses were performed using PearlDiver's RSuite software (PearlDiver Technologies). Figures were created using GraphPad Prism Version 10 (GraphPad Software).
Results
Study Cohorts
A total of 172,673 patients who underwent ACL reconstruction were identified, and obesity was identified in 28,047 (16.2%) (Table 1). Nonobese patients were younger, with a mean age of 30.1 ± 13.7 years compared with 36.5 ± 11.5 years for obese patients (P < .001). The sex distribution showed that a higher proportion of females were among the obese patients (60.5%) compared with nonobese patients (49.2%), while males comprised 39.5% of the obese group and 50.8% of the nonobese group (P < .001). The ECI indicated that obese patients had a greater burden of comorbidities, with a mean ECI of 4.1 ± 3.0 compared with 1.3 ± 1.6 for nonobese patients (P < .001).
Demographics of Patients Who Underwent ACLR Organized by Obesity Status a

Data are presented as n (%) or mean ± SD unless otherwise indicated. Bold P values indicate statistical significance. ACL, anterior cruciate ligament reconstruction; ECI, Elixhauser Comorbidity Index.
Once matched, both groups included 23,990 patients, with identical means and distributions for key variables. The mean age was 36.1 ± 11.6 years for both groups, and the sex distribution was balanced, with 57.3% females and 42.7% males in each group. Additionally, the ECI was equal between groups, with a mean of 3.7 ± 2.3, demonstrating the effectiveness of the matching strategy in balancing demographic and clinical characteristics, facilitating an accurate comparison of outcomes between nonobese and obese patients after ACL reconstruction.
Adverse Events
Adverse outcomes and univariate analyses are shown in Table 2. Obese patients had significantly higher rates of any adverse events after ACL reconstruction compared with nonobese patients (10.5% vs 3.8%; P < .001). Serious adverse events were also more frequent in the obese group (1.9% vs 0.7%; P < .001), with increased occurrences of pulmonary embolism (0.3% vs 0.06%; P < .001), sepsis (0.3% vs 0.08%; P < .001), and deep vein thrombosis (0.9% vs 0.4%; P < .001). Minor adverse events occurred more often among obese patients (6.9% vs 1.8%; P < .001), with increased rates of pneumonia (1.9% vs 0.3%), urinary tract infections (4.1% vs 1.0%), wound dehiscence (0.8% vs 0.2%), and acute kidney injury (0.7% vs 0.2%). Readmission rates were higher for obese patients (5.0% vs 0.8%; P < .001).
Univariate and Multivariate Analyses Comparing Adverse Events Between Obese and Nonobese Patient Groups After ACLR a
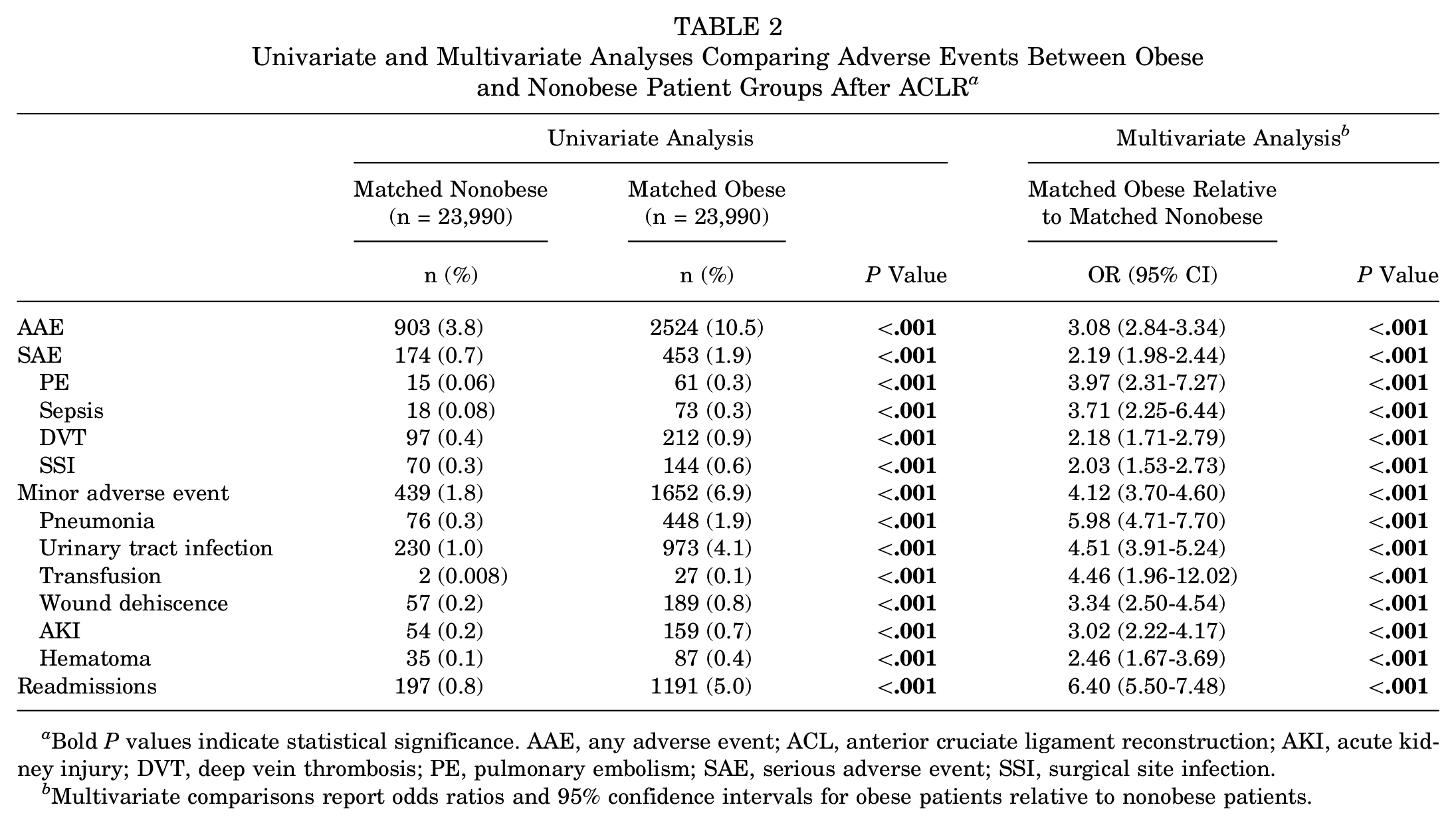
Bold P values indicate statistical significance. AAE, any adverse event; ACL, anterior cruciate ligament reconstruction; AKI, acute kidney injury; DVT, deep vein thrombosis; PE, pulmonary embolism; SAE, serious adverse event; SSI, surgical site infection.
Multivariate comparisons report odds ratios and 95% confidence intervals for obese patients relative to nonobese patients.
Multivariate analysis results are shown in Table 2 and Figure 1. Obesity was associated with an increased odds of adverse events (OR, 3.08; P < .001), serious adverse event (OR, 2.19; P < .001) and minor adverse event (OR, 4.12; P < .001). Specific adverse events linked to obesity included higher odds of the following, in decreasing odds ratio order, pneumonia (OR, 5.98), urinary tract infections (OR, 4.51), transfusion (OR, 4.46), pulmonary embolism (OR, 3.97), sepsis (OR, 3.71), wound dehiscence (OR, 3.34), acute kidney injury (OR, 3.02), hematoma (OR, 2.46), deep vein thrombosis (OR, 2.18), and surgical site infection (OR, 2.03) (P < .001 for all correlations). Readmission risk was significantly higher in obese patients (OR, 6.40; P < .001).

Forest plot of the multivariate comparison of adverse events in obese versus nonobese patients, controlling for age, sex, and Elixhauser Comorbidity Index. Odds ratios and 95% confidence intervals are reported for each outcome. AAE, any adverse event; AKI, acute kidney injury; DVT, deep vein thrombosis; MAE, minor adverse event; PE, pulmonary embolism; SAE, serious adverse event; SSI, surgical site infection; UTI, urinary tract infection.
Subsequent Ipsilateral ACL Retearing and Contralateral ACL Tearing
Kaplan-Meier survival curves for both ipsilateral (P = .5) and contralateral (P = .6) tearing are shown in Figures 2 and 3. These revealed no significant differences between the 2 groups, indicating that obesity did not have a notable effect on the rate of occurrence of tears in either knee over the follow-up period of 5 years.
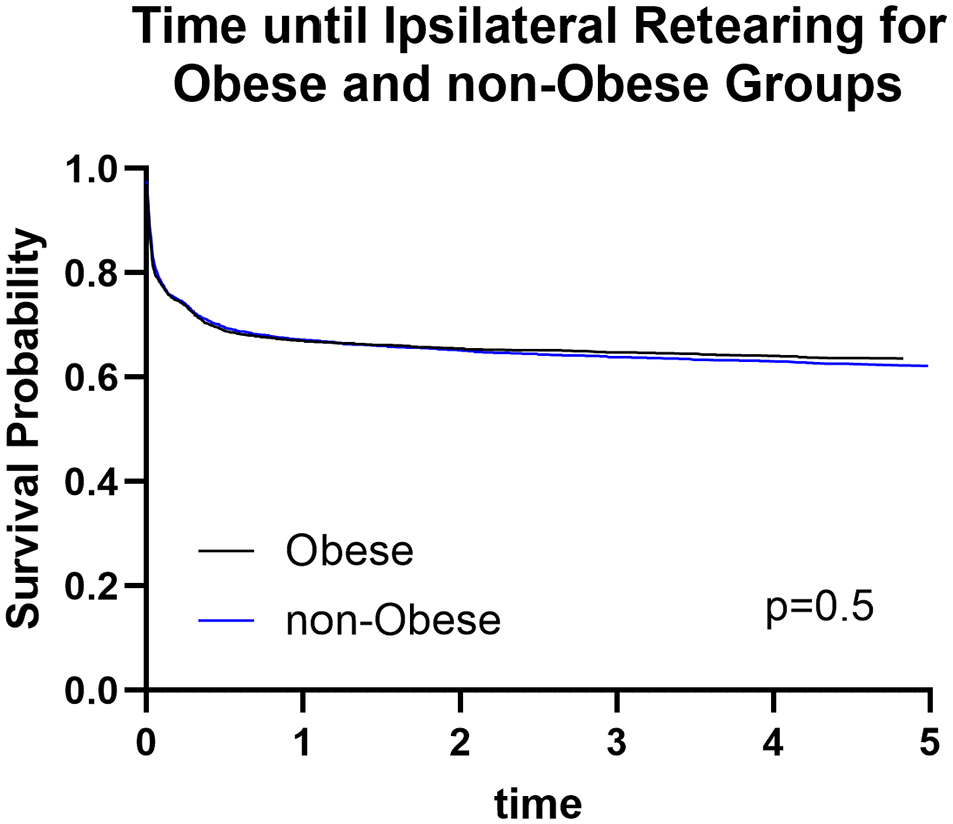
Kaplan-Meier survival curves for postoperative ipsilateral anterior cruciate ligament tear rates between obese and nonobese patients. There was no significant difference as shown by log-rank test (P = .5).

Kaplan-Meier survival curves for postoperative contralateral anterior cruciate ligament tear rates between obese and nonobese patients. There was no significant difference as shown by log-rank test (P = .6).
Discussion
The current study provides valuable insights into the correlation of obesity with adverse postoperative outcomes after ACL reconstruction, but not differences in 5-year ACL retears or contralateral tears, using large national patient cohorts.
Obesity was found to be significantly associated with an increased odds of multiple aggregated and individual adverse perioperative outcomes after ACL repair. This finding is consistent with previous studies that identified obesity as a risk factor for complications after ACL reconstruction, such as meniscal tears, 38 longer operative times,8,9,41 surgical site infections, 44 and subsequent arthritis. 12 However, it contrasts with other research that found no correlation between obesity and postoperative complications14,46 or revisions.8,22
Specifically, obese patients were more likely to experience a range of complications, including sepsis, surgical site infections, pneumonia, and urinary tract infections. This is consistent with previous studies that have reported similar outcomes after total joint arthroplasty 47 and supports the well-documented suppressive effect of obesity on immune function.17,29 Additionally, obese patients had higher odds of wound dehiscence, which aligns with existing literature that highlights the negative effect of obesity on the skin and wound healing. 15 Obesity was also independently associated with an increased risk of pulmonary embolism and deep vein thrombosis, aligning with previous studies linking obesity to a higher risk of thromboembolic disease. 39 Furthermore, the incidence of acute kidney injury was higher in the obese group, which is consistent with findings in patients undergoing various orthopaedic, colon, and thoracic surgeries.10,20,26
Obesity was also found to be independently associated with an approximately 6-fold increased odds of 90-day readmissions. This finding underscores the importance of closely monitoring obese patients in the early postoperative period to mitigate this from occurring. Our results align with previous work by Cooper et al, 9 which demonstrated that obesity is associated with a higher likelihood of 30-day readmissions after ACL reconstruction. These consistent findings further support the need for tailored perioperative care strategies for obese patients undergoing ACL surgery.
Interestingly, the 5-year outcomes related to ipsilateral and contralateral ACL tears did not show significant differences between obese and nonobese patients. This contrasts with the increased early complication rates, suggesting that while obesity may influence short-term postoperative recovery, it does not appear to have a substantial effect on the long-term risk of graft failure or contralateral knee injury within the 5-year follow-up period. This finding is valuable, as it implies that while obesity is a factor in immediate postoperative complications, it does not appear to affect the durability of the ACL graft or the incidence of tears in the opposite knee. These results are consistent with work done by Byun et al, 8 which also showed no significant association between obesity and postoperative revision surgeries.
Limitations
The current study does have limitations. The retrospective design limits causal inference, and reliance on administrative coding may lead to inaccuracies in the classification of obesity and adverse events. Additionally, the data set lacks detailed clinical information on patients and their outcomes, which could influence the observed correlations. Finally, when examining retearing after surgery by reviewing diagnostic codes over a 5-year period, inaccurate timing of coding for the tear might influence the results.
Conclusion
Our study highlights the elevated risk of adverse events and readmissions in obese patients undergoing ACL reconstruction, which may inform clinical decision-making and the need for tailored perioperative care strategies for this population. However, the lack of an association with long-term graft survival and contralateral injury suggests that while obesity affects postoperative complications, it may not influence the long-term surgical outcomes to the same extent. Future research should explore additional factors that may contribute to these findings and investigate potential interventions to mitigate the risks associated with obesity in ACL reconstruction.
Footnotes
Final revision submitted February 15, 2025; accepted March 17, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.