
Abstract
Background:
Lower limb muscle strength symmetry has been suggested as an essential criterion for the safe return to sports after anterior cruciate ligament (ACL) reconstruction. Limited evidence is available regarding the most effective intervention to achieve symmetry after reconstruction with contralateral bone–patellar tendon–bone (BPTB) graft.
Purpose:
To verify whether unilateral isotonic resistance exercise is more effective than bilateral exercise for obtaining postoperative functional and muscular strength symmetry between the donor limb and reconstructed limb for patients who received BPTB graft.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 88 patients were randomly divided into a control group (n = 44) and an intervention group (n = 44). All participants performed an 8-week exercise program starting at the beginning of the fourth postoperative month and were evaluated before and after the program. The control group performed bilateral exercises, and the intervention group performed unilateral exercises for the donor limb only (the limb with the greatest disability). The primary outcome was muscle strength (peak torque and hamstrings to quadriceps [H:Q] ratio), and the secondary outcomes were range of motion (ROM; goniometry), KT-1000 arthrometer side-to-side difference in anteroposterior knee laxity, and objective (single-leg hop test) and subjective (Lysholm score) functionality.
Results:
Both groups improved significantly from before to after the exercise program. The improvements were significantly greater in the intervention group regarding peak torque, H:Q ratio, flexion ROM, single-leg hop test, and Lysholm score in the donor limb (P < .001 for all), and the improvements were significantly greater in the control group regarding peak torque and single-leg hop test in the reconstructed limb (P < .001 for both). Comparison between the groups showed significantly increased symmetry regarding peak torque, H:Q ratio, and single-leg hop test in the intervention group compared with the control group (P < .001), with large effect sizes (>0.80) except for the H:Q ratio.
Conclusion:
Although postoperative, bilateral, isotonic resistance exercise provided better strength gains to the reconstructed limb, unilateral exercise was more effective in obtaining functional and muscle strength between-limb symmetry in patients who underwent ACL reconstruction with contralateral BPTB graft.
Registration:
Brazilian Registry of Clinical Trials (number RBR-22rnjh).
Anterior cruciate ligament (ACL) injuries have been the subject of study since the ninth century. 24 The direct costs estimated for surgical and rehabilitative procedures reach $3 billion per year. 32 ACL injury is a severe injury that can cause a series of physical, psychological, and economic sequelae for the patient. 3 In sports, ACL injury can mean a premature decrease in performance or even the end of a career. 26
Few studies have assessed the progression of resistance exercise in the postoperative period of ACL reconstruction. In general, the literature has been limited to understanding the ideal time to introduce resistance exercise, 5,18,28,49 measuring the loads generated during movements, comparing open and closed kinetic chain exercises, 14,25,40 and analyzing the progression of sensorimotor training (neuromuscular training). 41
Previous studies 6,30,36 demonstrated the clinical results of short- and medium-term recovery of patients who underwent ACL reconstruction with a contralateral bone–patellar tendon–bone (BPTB) graft and were rehabilitated under the same conditions as described by Shelbourne and Klotz. 45 The patients were satisfied with their function, but the isokinetic evaluation at multiple time points showed the presence of significant differences in muscle performance between each lower limb, of which the donor limb, (ie, the healthy limb), was shown to be more deficient. 6,30,36 Symmetry of muscle strength is thought to be an essential criterion for a safe return to sports. 21 However, limited evidence is available regarding the most effective interventions to achieve symmetry. To the best of our knowledge, no randomized controlled trial has identified the best strategy for the progression of resistance exercise for obtaining limb symmetry (range of motion [ROM], joint stability, muscle strength, and functionality) for patients who undergo ACL reconstruction with contralateral BPTB graft. Answering this question will contribute to the establishment of a better approach for these patients, reducing treatment time and minimizing muscle imbalance when they resume their activities. Finding an effective way to obtain symmetry is not only relevant but a necessity for professionals and patients. 4,29,50
The aim of the present study was to evaluate the effectiveness of unilateral isotonic resistance exercise when compared with its bilateral counterpart for obtaining the highest level of symmetry in functional and muscle strength variables between the donor limb and the ACL-reconstructed limb starting from the fourth month of rehabilitation in patients who received contralateral BPTB graft. Our hypothesis was that the use of unilateral isotonic resistance exercise in the donor limb would be more effective than the bilateral form for obtaining the highest level of functional and muscular strength symmetry between the donor limb and the reconstructed limb.
Methods
Our institution approved the protocol for this randomized, parallel, prospective, single-blinded controlled trial, and all participants were volunteers and signed an informed consent form. The method used was registered on the Brazilian Registry of Clinical Trials platform (number RBR-22rnjh).
Patients
Patients were recruited at the Orthopedic Hospital and Specialized Medicine/FIFA Medical Centre of Excellence between 2018 and 2019. The present study was performed with patients who underwent ACL reconstruction surgery with a contralateral BPTB graft. Patients of both sexes and varying occupations, who had practiced physical activity regularly (at least 3 times per week), had experienced an acute, traumatic ACL injury, and had received the same treatment—based on the knee symmetry model described by Biggs et al 9 —were included in the study. The exclusion criteria were patients younger than 18 and older than 55 years (according to the age group with the highest prevalence of ACL injuries in Brazil 31 ), professional athletes, patients who had undergone revision surgery, patients with a history of injuries and/or lower limb surgery, patients who had developed arthrofibrosis in the early postoperative period (according to the classification established by Shelbourne et al 43 ), patients who had heart disease, pregnant women, and nursing mothers.
Sample Size Calculation
The sample size was based on the main objective of verifying whether there was a difference between the treatment groups in the progression of peak torque symmetry from before the exercise program (preintervention) to after (postintervention). Therefore, the following parameters were considered: significance level α = 5% (bilateral), power of the 1– β test = 80%, and the expected relatively “moderate” difference in the change (from pre- to postintervention) of peak torque symmetry between groups, known as effect size (≍0.60). As established by Cohen, 13 the minimum number of patients in each group was 44, totaling 88 patients equally divided into the control group (n = 44) and the intervention group (n = 44).
Initial Monitoring of Patients
The medical team referred patients with an ACL injury to the study while they were still in the preoperative phase, after they had been diagnosed, and the treatment under study had been defined as the primary option.
Preoperative rehabilitation aimed to control the inflammatory process, restore ROM, improve muscle performance and sensorimotor capacity, obtain a symmetrical gait cycle, and encourage effective adherence to treatment and intervention, so that patients could fully dedicate themselves to the different phases of recovery, thus achieving the expected results. The preoperative phase was concluded when the patients had no acute inflammatory signs, with restored ROM and muscle trophism (considering ≤1-cm difference in thigh circumference between the limbs) 36 and good neuromuscular control, were walking normally, and were fully motivated. The mean preoperative rehabilitation time was 4 weeks.
The postoperative phase began at the hospital during the hospitalization period. The main objectives of this phase were to control pain and hemarthrosis, restore ROM, start weightbearing as tolerated, introduce bike training, and start muscle strengthening exercises (initially in closed kinetic chain) along with sensorimotor progression. The limbs were differentiated in terms of objectives. In the donor limb, the aim was to stimulate the regeneration and development of the donor area, so that muscle performance could be restored. For the reconstructed limb, special emphasis was given to controlling hemarthrosis, reestablishing ROM, and stimulating graft maturation. 9
Surgical Procedure
All surgeries were performed by the same medical team. The procedures were based on previous studies. 30,44,45 All approaches were performed using the anatomic technique, via the medial portal, simultaneously in both knees (receptor and donor). A tourniquet was also used on both knees.
Regarding the donor procedure, an incision was initially made in the medial paratendon with divulsion in planes. From the opening of the paratendon, markings were made on the patellar ligament 10 mm wide and on the patella and tibia 20 mm in length, and bone plugs 10 mm in depth were removed. After removal of the graft, the donor area was closed with No. 1.0 Vicryl suture, including sheath and tendon. The bone graft was then placed in the patellar defect (from the tibial tunnel of the recipient knee).
Arthroscopic portals were made in the recipient knee, followed by synovectomy with cleaning of the tibial and femoral footprint, following the pattern of arthroscopic surgery. The knee was then positioned on the surgical table at 120° of flexion. Using the medial portal, the surgeon made the femoral tunnel, located approximately between the anteromedial and posterolateral bands, a little more medial, trying to reproduce the anteromedial band. The surgeon created the tibial tunnel with the patient’s knee off the table and flexed to 90°, using a tibial guide. The tibial footprint is located in the medial region of the tibial plateau, with reference to the posterior edge of the anterior horn of the lateral meniscus. After the tunnels were measured, the graft was introduced with the patient’s knee flexed at 45° to 90° and was fixed to the femur with a CL BTB Endobutton (Smith & Nephew) and to the tibia with a bioabsorbable screw (Smith & Nephew) with the knee flexed at 0° to 20°. Finally, an intra-articular suction drain was placed, portals were sutured with No. 4-0 nylon thread, and the donor knee incision was sutured.
Randomization
This was a 2-parallel-group, randomized clinical trial with a 1:1 intervention allocation. The randomization of the patients was performed by a statistical researcher using the Random Allocation Software (Version 2.0, Mahmood Saghaei). The allocation groups were placed in 100 (to account for dropout) opaque, nontranslucent, numbered envelopes that were opened at the time the patients arrived for the beginning of the intervention; thus, these patients received envelopes that were opened when they showed up for the continuation of rehabilitation.
Intervention Group
Patients in the intervention group underwent an 8-week program of unilateral resistance exercises (only for the donor limb) (Figure 1), starting at the beginning of postoperative month 4, immediately after the preintervention evaluation. Patients in the control group underwent an 8-week program according to the conventional method of bilateral exercises where patients are exercising both lower limbs at the same time (Figure 2) (Video Supplement 1).
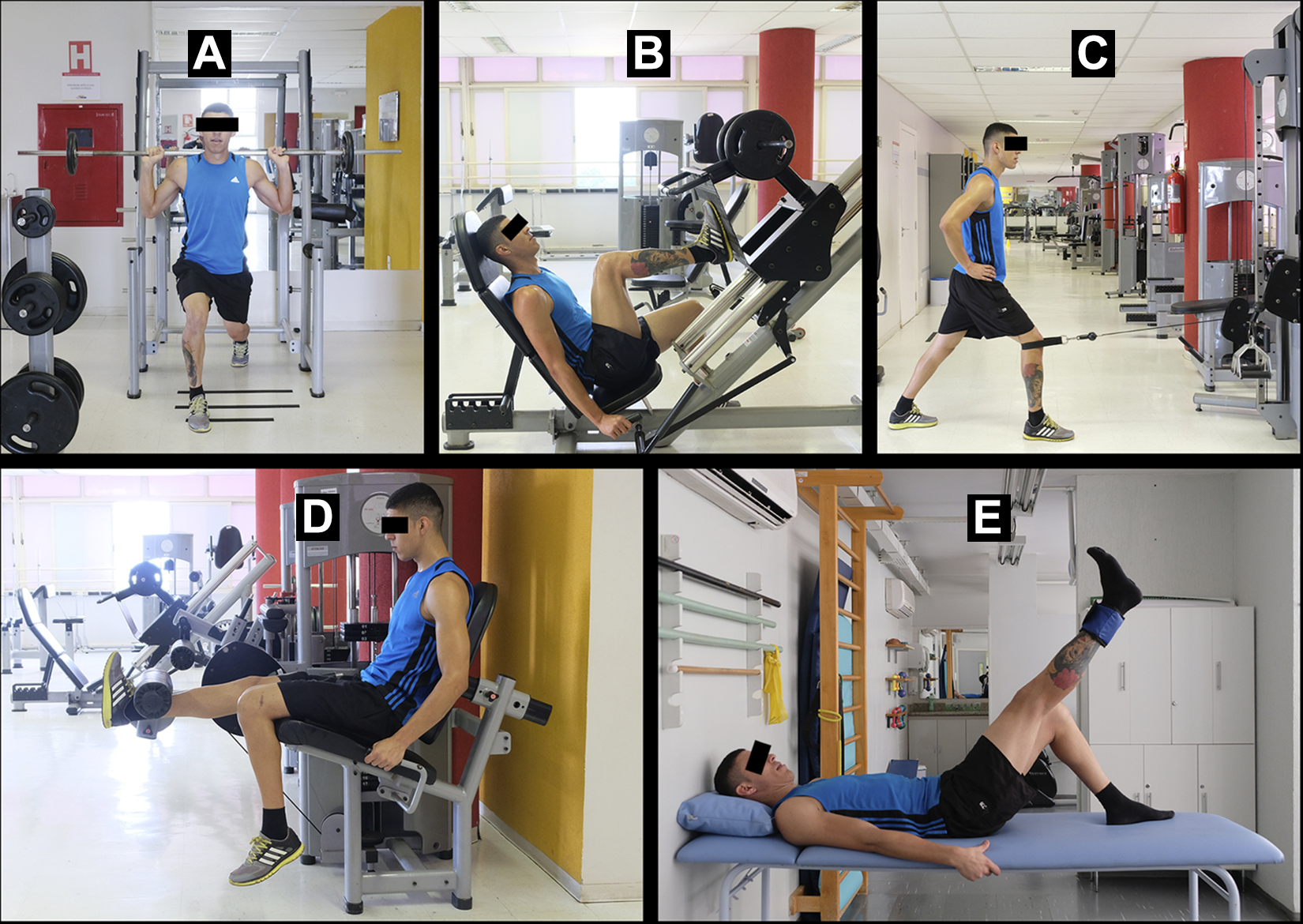
Sequence of exercises performed by the intervention group: (A) lunge, (B) leg press, (C) terminal extension, (D) leg extension machine, and (E) straight leg raise.
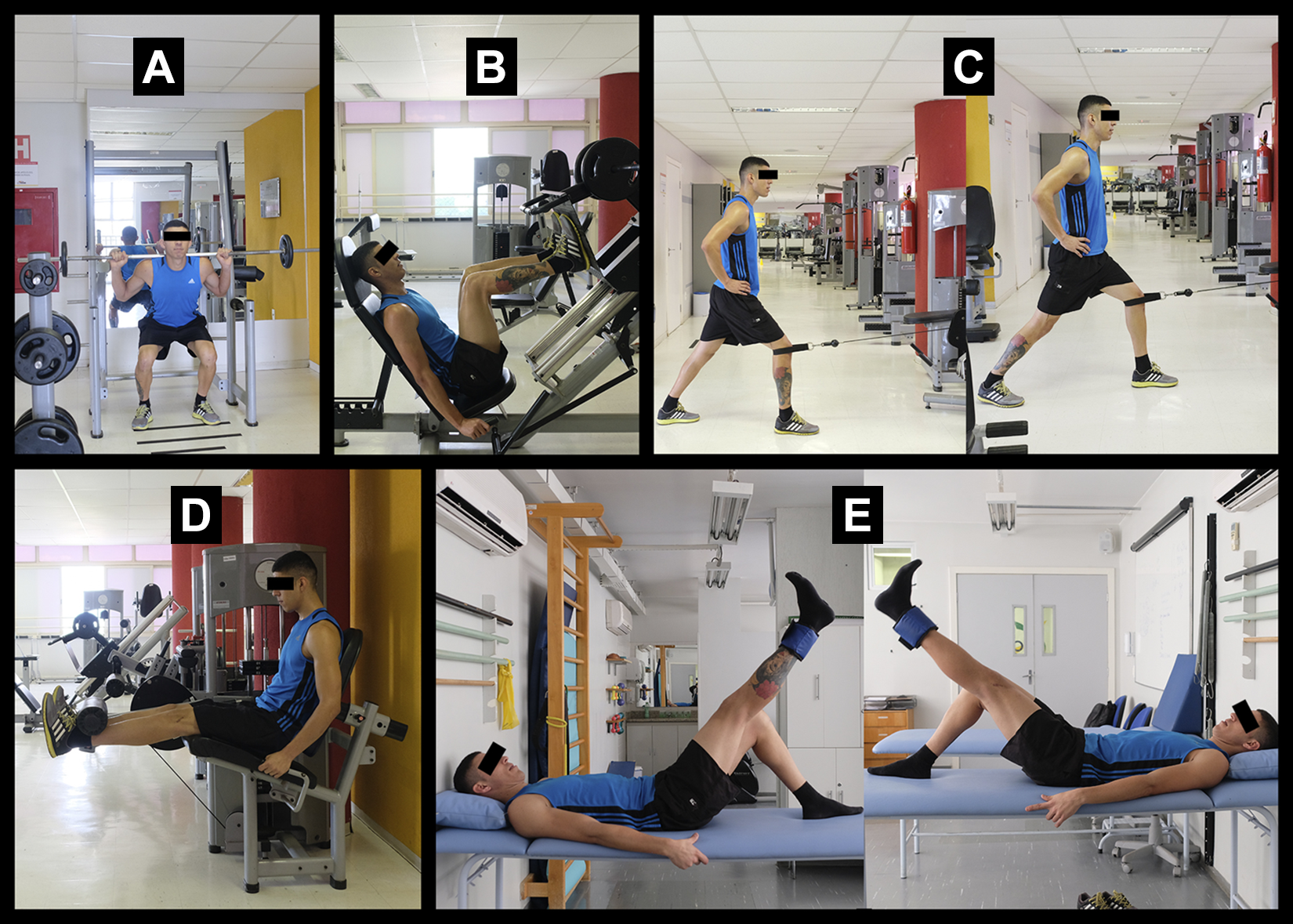
Sequence of exercises performed by the control group: (A) squat, (B) leg press, (C) terminal extension, (D) leg extension machine, and (E) straight leg raise.
A minimum of 2 treatment sessions per week were performed, representing a minimum interval of 48 hours between sessions. The exercise sequence included stimuli through closed kinetic chain as well as open kinetic chain movements. These sessions were performed based on the complexity of the motor movement and on the number of joints involved.
For both groups, the exercise sequence was preceded by a 15-minute warm-up on the bike. The sequence is described below and was adopted for all the prescriptions of resistance exercises in the course of the patient follow-up period. 1 During the intervention period, patients were recommended to perform only the proposed activities. The sequence of exercises for the intervention group were lunge (with the donor limb in front), leg press, terminal extension, leg extension machine, and straight leg raise. The exercises for the controls were similar but used both limbs (squatting, leg press, terminal extension [knee extension with low pulley], leg extension machine, and straight leg raise).
The sessions consisted of 3 sets of 12 repetitions for each exercise, with each repetition performed within 2 seconds in both the concentric and eccentric phases. The program progression was performed through load adjustment, with increments from 2% to 10% for the following session in which the individual was able to perform all the repetitions in all sets of a given exercise. 1
The initial workload was defined according to the repetition test proposed by Kraemer and Fleck, 27 which makes it possible to identify the appropriate overload for the specificity of the resistance exercise program without subjecting the locomotor apparatus to maximum contraction stress. The interval between the sets was 1 minute, whereas the interval between the exercises was 3 minutes. All resistance exercise sessions were preceded by a 5-minute warm-up period on an exercise bike with an intensity of 60% of the maximum heart rate reserve (monitored by an Onyx Nonin digital finger pulse oximeter; Nonin Medical Inc) estimated from the maximum heart rate predicted by age, as follows: {[(220– Age)– Resting Heart Rate] × 0.6} + Resting Heart Rate. 1 At the end of each session, stretching was performed for quadriceps, hamstrings, and triceps surae in three 30-second sets. 17
Outcome Measures
All the patients were evaluated before (4 months after surgery) and after the 8-week exercise program (Video Supplement 2). The primary outcome was muscle strength (peak torque and hamstrings to quadriceps [H:Q] ratio), and the secondary outcomes were ROM, side-to-side difference in anteroposterior knee laxity, and objective and subjective functionality. The procedures were performed by a blinded independent evaluator not involved in the study and with no employment relationship with the institutions. The evaluator was a physical therapist with a background in functional and sports trauma and orthopaedic physiotherapy and experienced in the application of the criteria used. He was unaware of any information related to the objectives of the study, diagnosis of patients, and distribution of the sample. The physical therapist was previously trained to use the assessment tools.
Initially, identification and anamnesis were performed, including the recording of weight and height. Next, the physical examination was performed by measuring ROM, anteroposterior knee laxity, knee extensor and flexor muscle strength, and knee function. ROM was measured using goniometry, considering the flexion and hyperextension movements. Joint stability was assessed objectively using a KT-1000 arthrometer (MEDmetric). Muscle strength was assessed using the Biodex Multi-Joint System 4 Pro isokinetic dynamometer (Biodex Medical Systems). 10 The patients performed 5 maximum concentric repetitions of knee extension and flexion at a speed of 60 deg/s. The last step was the assessment of functional capacity, performed objectively through the single-leg hop test and subjectively using the Lysholm score, an instrument translated into Portuguese and validated with measurement and reliability properties. 39 Table 1 presents all of the primary (peak torque and H:Q ratio) and secondary outcomes assessed, as well as the assessment methods.
Evaluation Criteria to Analyze the Primary and Secondary Outcomes

Data Analysis
The descriptive data analysis is presented to provide an overview of the participants based on their general characteristics: identification and anamnesis data. Such data are presented as median ± standard deviation for continuous data and as frequency and percentage for categorical data. Numerical data were compared using the Mann-Whitney U test, whereas categorical data were compared using the chi-square or Fisher exact test.
The normality and homogeneity of data were analyzed using the Shapiro-Wilk and Levene tests, respectively. Data showing a normal distribution were compared using the t test for independent samples. For the remaining variables, the nonparametric Mann-Whitney U test was used. For intra- and intergroup comparison of variables that showed normal distribution, a mixed-model analysis of variance (repeated measures and 2 factors) was used. For the remaining variables, the nonparametric Mann-Whitney U test was used (the pre-to-post difference in both groups was verified, and an intergroup comparison of this difference was made). The effect size was interpreted as follows: 0.00-0.49 (small effect), 0.50-0.79 (medium effect), and >0.80 (large effect). 15 The level of symmetry between the limbs was calculated based on the difference between the donor and reconstructed limbs. All statistical analyses were conducted using IBM SPSS Version 20.0 for Windows.
Results
The study sample consisted of 97 patients assigned to the intervention and control groups. During development of the activities, 9 patients did not complete their participation in the study: 2 because of pain in the donor area (control group), 4 because of withdrawal (3 from the intervention group and 1 from control group), and 3 for not complying with the proposed procedures (2 from the intervention group and 1 from the control group). The final study sample consisted of 88 patients (44 each in the control and intervention groups) (Figure 3).

CONSORT (Consolidated Standards of Reporting Trials) 34 flowchart of the randomized controlled trial showing the phases covered by the 2 study groups.
The general baseline characteristics of the study cohort are shown in Table 2. In total, 59 men (67%) and 29 women (33%) participated. Male patients were predominant in both groups: The intervention group consisted of 28 men and 16 women, whereas the control group consisted of 31 men and 13 women. Table 3 shows a comparison between the groups before the intervention. A significant difference between groups was found for flexion ROM in the donor limb (P = .03).
Comparison of Baseline Characteristics Between the Groups a
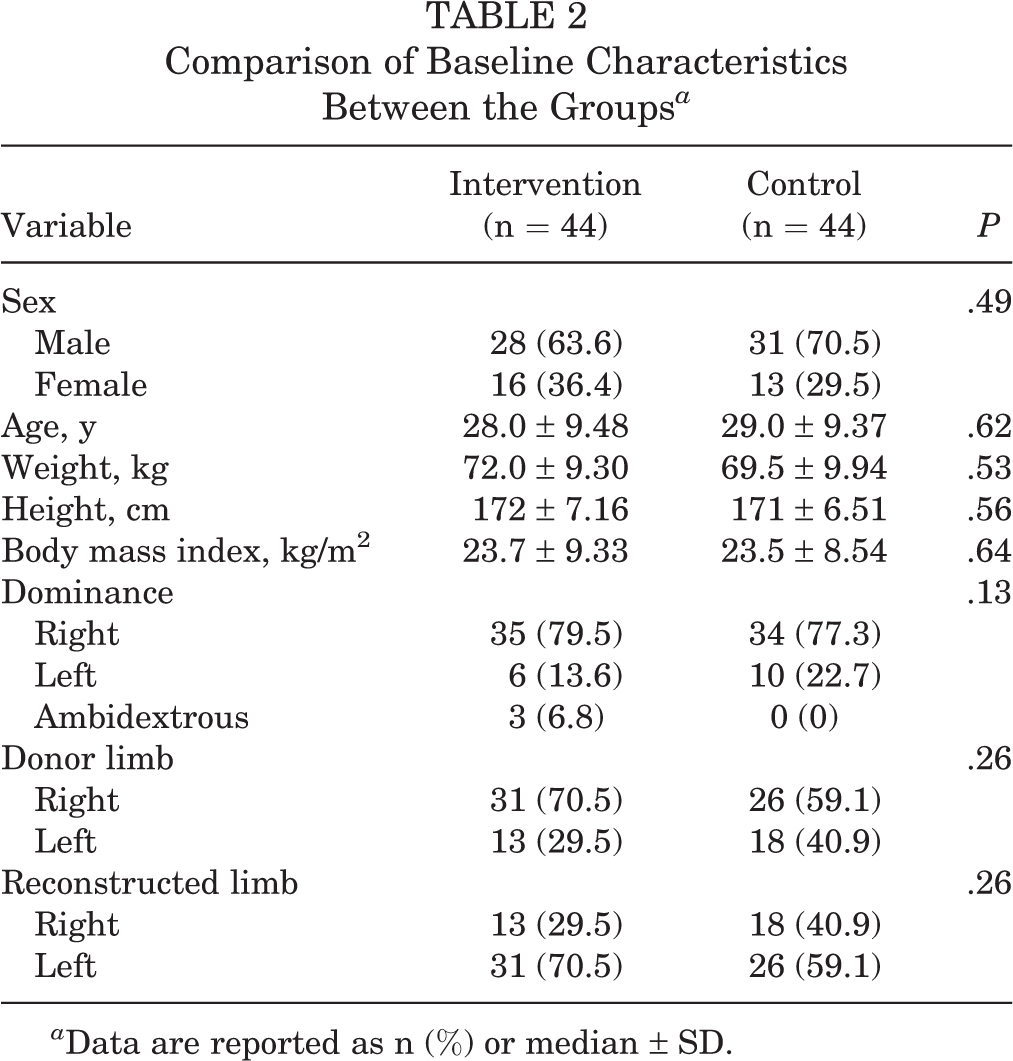
a Data are reported as n (%) or median ± SD.
Comparison Between Groups at the Preintervention Stage Concerning the Study Outcomes a

a Data are reported as median ± SD. Bolded P value indicates statistically significant difference (P < .05). ACL, anterior cruciate ligament–reconstructed limb; DL, donor limb; H:Q, hamstrings to quadriceps; SLHT, single-leg hop test; SSD, side-to-side difference.
Assessment of Primary and Secondary Outcomes Between Groups
After the intervention, significant differences were found between groups (Table 4). Flexion ROM, single-leg hop test performance, H:Q ratio, peak torque in the donor limb, and Lysholm score were better in the intervention group compared with the control group (P < .001 for all). The single-leg hop test and peak torque in the reconstructed limb were better in the control group compared with the intervention group (P < .001 for both). Large effect sizes (>0.80) were seen in the pre- to postintervention change for peak torque (donor and reconstructed limbs) and single-leg hop test values (donor limb).
Intra- and Intergroup Comparison of the Study Outcomes a

a Data are expressed as median ± SD. Bolded P values indicate statistically significant difference (P < .05). ACL, anterior cruciate ligament–reconstructed limb; DL, donor limb; H:Q, hamstrings to quadriceps; SLHT, single-leg hop test.
b Dashes indicate not applicable.
c 0.00-0.49 (small effect); 0.50-0.79 (medium effect); >0.80 (large effect).
Effectiveness of Unilateral Versus Bilateral Resistance Exercise in the Symmetry of Muscle Strength After ACL Reconstruction
Table 5 shows a comparison between groups for the level of symmetry between the donor and reconstructed limbs concerning the objective functionality and muscle strength criteria. Significant differences were found for all variables, with increased symmetry in the intervention group compared with the control group (P < .001 for all). Except for the H:Q ratio, the effect sizes were large (>0.80).
Comparison of Intralimb Symmetry (Donor–Reconstructed Limb) Between Groups a

a Data are expressed as median ± SD. Bolded P values indicate statistically significant difference (P < .05). H:Q, hamstrings to quadriceps.
Discussion
The aim of the current study was to evaluate the effectiveness of unilateral isotonic resistance exercise compared with its bilateral counterpart for obtaining the highest level of symmetry after ACL reconstruction with contralateral patellar ligament graft. Our results confirmed the initial hypothesis. The present study demonstrated, for the first time, the obtainment of a higher symmetry between limbs through unilateral exercise compared with bilateral exercises according to functional and muscle performance variables in patients undergoing contralateral BPTB graft.
Rehabilitation after ACL injury is widely studied, and several protocols are described in the literature. 16,20,44,46 The decreases in sensorimotor capacity and muscle performance are 2 of the main complications verified after ACL reconstruction. 41 Levels of quadriceps strength asymmetry are associated with biomechanical alterations in functional tests and are considered risk factors for the development of osteoarthritis and injury recurrences. 38 Effective strategies to achieve symmetry through resistance exercise are still a subject of controversy and little scientific study. 18,28,49 Our results showed the superiority of unilateral exercise compared with bilateral exercise. The main hypotheses that indicate the inferiority of bilateral training are related to mechanical and/or neural mechanisms, such as antagonist coactivation, reduced stimulation of motor units and/or type II fibers, the differentiated neural recruitment due to the cross effect in the extrapyramidal system, fiber differences in the limbs, and the predominance of using one limb to the detriment of the other, resulting in less force production. 11,37
In contrast, the unilateral exercises, despite achieving better symmetry, resulted in a delay of strength recovery in the ACL-reconstructed leg, given that the protocol used in our investigation focuses on muscle development, mainly in the donor limb.
Previous studies in patients undergoing ACL reconstruction with contralateral limb graft harvest showed similar results. Gonzalo-Skok et al 19 analyzed basketball players who were randomly assigned to perform unilateral or bilateral training over the course of 6 weeks. The authors found that both programs improved physical fitness tests. However, only the unilateral group experienced a reduction in asymmetry between the limbs and demonstrated better results in actions that required the application of unilateral force. In the same year, to compare the neuromuscular adaptations of unilateral and bilateral training for knee extensor muscles, Botton et al 12 submitted 43 healthy young women to a 12-week resistance exercise program. The isometric muscle strength test demonstrated a significant increase in the unilateral group compared with the bilateral group, which could also be observed in the muscles’ electrical activity. The authors concluded that if training aims to optimize the gain of force produced for each lower limb separately, unilateral training should be recommended.
Regarding knee injury, Welling et al 51 compared the results of a progressive strength training program for amateur soccer players after ACL reconstruction versus the results for healthy individuals (also amateur soccer players), investigating the quadriceps and hamstrings strength recovery. The intervention group consisted of 38 players, whereas the control group (healthy individuals) had 30 players, matched by age. The training program included unilateral and bilateral exercises in open kinetic chain (extension and flexor chair) and closed kinetic chain (squat, deadlift, split squats, step-ups, and good mornings). Quadriceps and hamstrings muscle strength was measured 3 times during rehabilitation using a limb symmetry index >90% as a discharge criterion. The results showed that the intervention group did not have significant differences between the limbs 7 months after the ACL reconstruction compared with the dominant limb of the control group. Also, 65.8% of patients reached a limb symmetry index of >90% at 10 months after surgery.
Moreover, analysis of the patients’ final condition showed significant changes in the muscle H:Q ratio, with more symmetry in the unilateral group compared with the bilateral group. The use of unilateral exercises in the donor limb (intervention group) provided a greater gain in quadriceps muscle strength compared with the use of bilateral exercises (control group): Increased in strength in the reconstructed limb promoted higher asymmetry. In patients with ACL injuries, an increase in H:Q ratio is normal for 2 reasons: (1) increased hamstrings reflex activity due to the instability caused by ligament loss 48 and (2) quadriceps weakness, which is typical in this type of patient, both before and after surgery. 35,38 Such analysis (H:Q ratio) is an outcome widely used in rehabilitation programs to ensure functional ability of the knee and its muscle balance. 42 The H:Q ratio has been demonstrated to be protective for graft rupture (ie, the higher the ratio, the lower the risk). 42 This is likely because the hamstrings are agonists to the ACL and should be in good balance with the quadriceps (antagonists of the ACL). Thus, our results demonstrate the importance of the unilateral protocol in ACL rehabilitation. We found no differences regarding ligamentous laxity between the analyzed groups.
Limitations
Our study has some limitations. We are aware of other widely used surgical techniques that directly affect decision-making regarding the most effective method of implementing resistance exercise from the preoperative period until discharge. Also, we do not know how the patients will progress until the end of the first year, which is a critical period for the occurrence of new injuries and/or complications. Furthermore, the wide age range of the study volunteers should be considered, as the goals and course of postoperative rehabilitation are very different based on age. This study applies only to patients receiving contralateral BPTB graft and is probably not suitable for other graft options. Finally, future studies should investigate the possible role of single-leg exercises for both legs.
Aside from these limitations, our study is the first randomized controlled trial to find the best strategy (unilateral or bilateral) for using resistance exercise to achieve symmetry between the lower limbs. We reported data following the CONSORT (Consolidated Standards of Reporting Trials) recommendations, 34 we described the interventions following the recommendations of the Template for Intervention Description and Replication, 21,22 and we described the intervention exercises according to the recommendations of the Consensus on Exercise Reporting Template. 47
In clinical terms, the main point of this study was to confirm the use of unilateral exercise as an effective alternative for the recovery of symmetry in patients who have undergone ACL reconstruction. This is the main implication of the results, allowing professionals to start the rehabilitation protocol early and ensure a favorable outcome. However, it is still not known which strategy—unilateral, bilateral, or unilateral performed with both legs—is the best option for rehabilitation. Moreover, new strategies must be developed to enhance the benefits of unilateral exercise in this group. The current literature contains promising alternatives, such isoinertial exercise, 8 the use of vascular occlusion methods, 7,23 and the improvement of sensorimotor exercises. 33 These are essential topics for further investigation.
Conclusion
Although bilateral isotonic resistance exercise provided better strength gains to the ACL-reconstructed limb, the unilateral protocol obtained the highest level of functional and muscle strength symmetry between the donor limb and ACL-reconstructed limb in the postoperative phase of patients who underwent ACL reconstruction with contralateral BPTB graft.
A Video Supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671221088830.
Footnotes
Final revision submitted December 6, 2021; accepted December 15, 2021.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Universidade Federal de São Paulo (ref No. 60929).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.