
Abstract
Background:
Some patients still experience mild residual rotational laxity of the knee after anterior cruciate ligament reconstruction (ACLR). The clinical symptoms of this residual rotational laxity are controversial, and methods for evaluating the symptoms have become a focus of academic interest in recent years. It is unclear whether there is a correlation between mild residual rotational laxity after ACLR and performance.
Purpose:
To investigate the influence of residual mild rotational laxity after ACLR on subjective outcomes, performance, psychological readiness, and return to sports (RTS).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 81 patients who underwent ACLR at our sports medicine center were observed for >2 years. The follow-up included KT-2000 measurements, the pivot shift test (PST), subjective outcome scores (Lysholm, International Knee Documentation Committee Subjective Knee [IKDC], Knee injury and Osteoarthritis Outcome Score [KOOS], ACL-Return to Sport after Injury Score [ACL-RSI], Tegner score, and Marx score), and performance evaluations, such as isokinetic testing at 60 deg/sec, hop tests, and Y-balance tests (YBT). Patients were grouped based on the results of the last PST follow-up on the operated knee. The stable group (SG) consisted of 42 patients with negative PST results, while the mild rotational laxity group (MIG) comprised 39 patients with PST grade 1. Statistical analysis was conducted to compare patient characteristics, subjective outcome scores, and performance between the 2 groups.
Results:
Significant differences were observed between the 2 groups in the single-leg hop test, the triple hop test, and the cross-over hop limb symmetry index, respectively (P = .013; P = .017; P = .046). In addition, the SG had significantly higher ACL-RSI scores than the MIG (69.54 ± 21.34 vs 53.60 ± 21.66; P = .006); and postoperative Tegner scores were significantly higher in the SG compared with the MIG (5.81±1.70 vs 4.95 ± 1.93; P = .036). No significant differences were observed in Lysholm, IKDC, KOOS score, postoperative Marx, or KT-2000 side-to-side difference scores, and no significant differences were found in isokinetic testing at 60 deg/sec, hamstring-to-quadriceps ratio, or YBT results between the 2 groups.
Conclusion:
Residual mild rotational laxity in the knee after ACLR leads to poorer performance in hop tests and a lower level of activity, and poor psychological readiness. Furthermore, in short- to medium-term follow-up after ACLR, regardless of knee rotational laxity, the return to preinjury activity rate remains low, with the majority not meeting the safe RTS criteria.
Keywords
The anterior cruciate ligament (ACL) is a significant anatomic structure in the knee that restricts anterior tibial translation and internal rotation of the tibia, commonly subject to sports-related injuries. 25 ACL injury leads to anterior-posterior and rotational instability of the knee, resulting in aberrant movement patterns. 28 Anterior cruciate ligament reconstruction (ACLR) serves as the primary intervention to restore knee stability and functionality after ACL injury, facilitating patients’ return to sports (RTS). 8 Despite ACLR, approximately 3% to 22% of patients still experience residual mild rotational laxity in the knee postoperatively. 13 The association between this residual instability and subjective outcome scores and performance remains uncertain, contributing to the controversy surrounding its clinical significance.17,31 A subset of studies suggested that knee stability does not correlate with subjective outcome scores,20,30 nor does it correlate with performance.16,23 However, others have suggested that mild knee laxity heightens the risk of revision and significantly affects subjective outcomes.17,24 Consequently, the evaluation of residual mild rotational laxity after ACLR has garnered substantial academic attention in recent years.
Assessment of knee rotational laxity typically involves physical examination. The pivot shift test (PST), first described by Galway and MacIntosh, 6 is a specific assessment of rotational instability observed in ACL-injured knees and is now widely utilized in postoperative ACLR assessment. Furthermore, the patient's Lysholm score, the International Knee Documentation Committee Subjective Knee (IKDC) score, the Knee injury and Osteoarthritis Outcome Score (KOOS), the Tegner score, and the Marx score are commonly employed to evaluate the efficacy of ACLR. Among these, the Tegner score reflects the patient’s preinjury activity level and postoperative recovery, with a comparison made to ascertain whether the patient has returned to the preoperative level. 27 Webster et al 30 developed the ACL-Return to Sport after Injury Score (ACL-RSI), recognized as a reliable indicator for assessing postoperative psychological readiness. 26 According to the latest Panther guidelines 22 of 2020, performance evaluation constitutes an integral aspect of assessing postoperative function, encompassing lower extremity muscle strength, hop tests, and Y-balance tests (YBT). Therefore, the principal aim of this study was to investigate whether residual mild rotational laxity after ACLR influences subjective outcomes and performance in short- and medium-term follow-ups. Furthermore, the study aimed to compare the disparities in subjective outcome scores and performance between patients exhibiting grade 1 and negative PST, thereby providing valuable insights for clinical treatment.
Methods
Participants
This study was conducted between November 2022 and December 2023 to observe patients who were seeking medical care at our hospital during July 2008 and December 2021 and underwent their first ACLR. Sex, age at surgery, body mass index (BMI), affected side, time from injury to surgery, meniscal injury, and follow-up time were recorded for the enrolled patients. The inclusion criteria were as follows: (1) primary single-bundle ACLR; (2) no combined posterior cruciate ligament injury; (3) the use of autologous hamstring tendon graft for ACLR; (4) ACLR performed using the anterior medial approach femoral tunnel localization technique; (5) epiphyseal closure; (6) ≥2 years of follow-up; (7) ability to be contacted and participate in the postoperative offline follow-up; and (8) no history of other surgeries affecting the knee function. The exclusion criteria were as follows: (1) ACL revision between the initial postoperative period and the follow-up period; (2) posterior cruciate ligament injury between the initial postoperative period and the follow-up period; (3) generalized ligamentous laxity; (4) other surgeries affecting the knee function between the initial postoperative date and the follow-up date; (5) a PST of ≥2 grade; (6) inability to complete all the required examinations or evaluations at the postoperative follow-up visit.
A total of 81 patients completed all required evaluations for the follow-up—including clinical examinations using the KT-2000, PST, Lysholm, IKDC, KOOS, ACL-RSI, Tegner, and Marx scores for subjective outcome scores; and the isokinetic muscle strength test at 60 deg/sec in the affected knee, hop tests, and YBTs for performance evaluations—and were included in the study (Figure 1).

Flowchart of participants. ACLR, anterior cruciate ligament reconstruction; PTS, pivot shift test.
Questionnaires regarding sports participation were completed at 2 time points: preoperatively and at the postoperative follow-up. A clinical examination was performed at the last follow-up to complete the subjective outcome scores, as well as the performance tests. The study was approved by the Regional Ethics Committee (202210), and consent for the study was obtained from all included patients.
Clinical Examination
Pivot Shift Test
Each patient was examined separately by 2 specialists (J.Z. and F.G.) in the field of sports medicine. These 2 surgeons were independent examiners with no previous involvement in patient care. The absence or presence of specific criteria during flexion of the affected knee at the follow-up was classified according to the grading method proposed by Jakob et al. 14 Patients with consistent grade 1 PST results were included in the mild rotational instability group (MIG), while those with grade 0 PST results were included in the stable group (SG). In cases of disagreement between examiners, the PST under anesthesia was performed. Ultimately, 5 patients were excluded from the study because they had grade 2 PST results under anesthesia.
KT-2000
We used the KT-2000 arthrometer (Medmeric) at 133 N (30 Lb) force for assessment, and the knee was flexed between 20° and 25°. The results were expressed as the side-to-side difference (SSD) between the affected side and the healthy side measurements.
Lower Extremity Muscle Strength
The patient’s peak knee extensor and flexor moments were assessed using the American Biodex system 4 isokinetic muscle strength testing system (Figure 2). This system is primarily employed to evaluate the capacity of knee flexor and extensor muscle groups to generate maximum muscle force at low-speed dynamics. Patients underwent comprehensive warm-up sessions under the guidance of professional testers (J.S. and Y.Z.) to conduct the knee joint isokinetic muscle strength test with adaptive training, ensuring full adaptation before the formal assessment. The patient assumed a seated position on the testing chair, with the torso and the test leg secured by safety belts, aligning the direction of the test knee joint with that of the power arm. The range of motion for the knee was individualized for each patient, and the angular velocity of knee flexion and extension movements was standardized at 60 deg/sec for the assessment, commencing with testing the healthy side, followed by the affected side. To facilitate analysis, the limb symmetry index (LSI) was utilized to express the ratio of peak moments of the extensor and flexor muscle groups on the affected side relative to those on the healthy side (hamstring-to-quadriceps ratio [H/Q]).

Schematic diagram of isokinetic muscle strength testing.
Hop Test
Three functional tests were chosen: (1) the single-leg hop test; (2) the single-leg triple hop test; and (3) the single-leg cross-over hop test (Figure 3). Before each test, the examiner (J.S. and Y.Z.) explained and demonstrated the procedures to the participants to acquaint them with the testing protocol and movements. Participants practiced each movement on both legs before the official assessment to familiarize themselves with the procedures. A successful attempt was defined as the participant maintaining the jump for at least 2 seconds after landing. Each test was repeated 3 times, and the distance achieved was recorded, with a precision of 1 cm. If the distance achieved on the third attempt was greater than previous attempts, a fourth attempt was conducted, and if the fourth attempt exceeded all previous distances, it was included in the data analysis. Test failure was defined as any instance where the participant’s contralateral lower or upper limb made contact with the ground, loss of balance occurred, or an additional jump was made upon initial landing. The time interval between attempts of the same test was 30 seconds, while the time interval between different test items was 2 minutes.
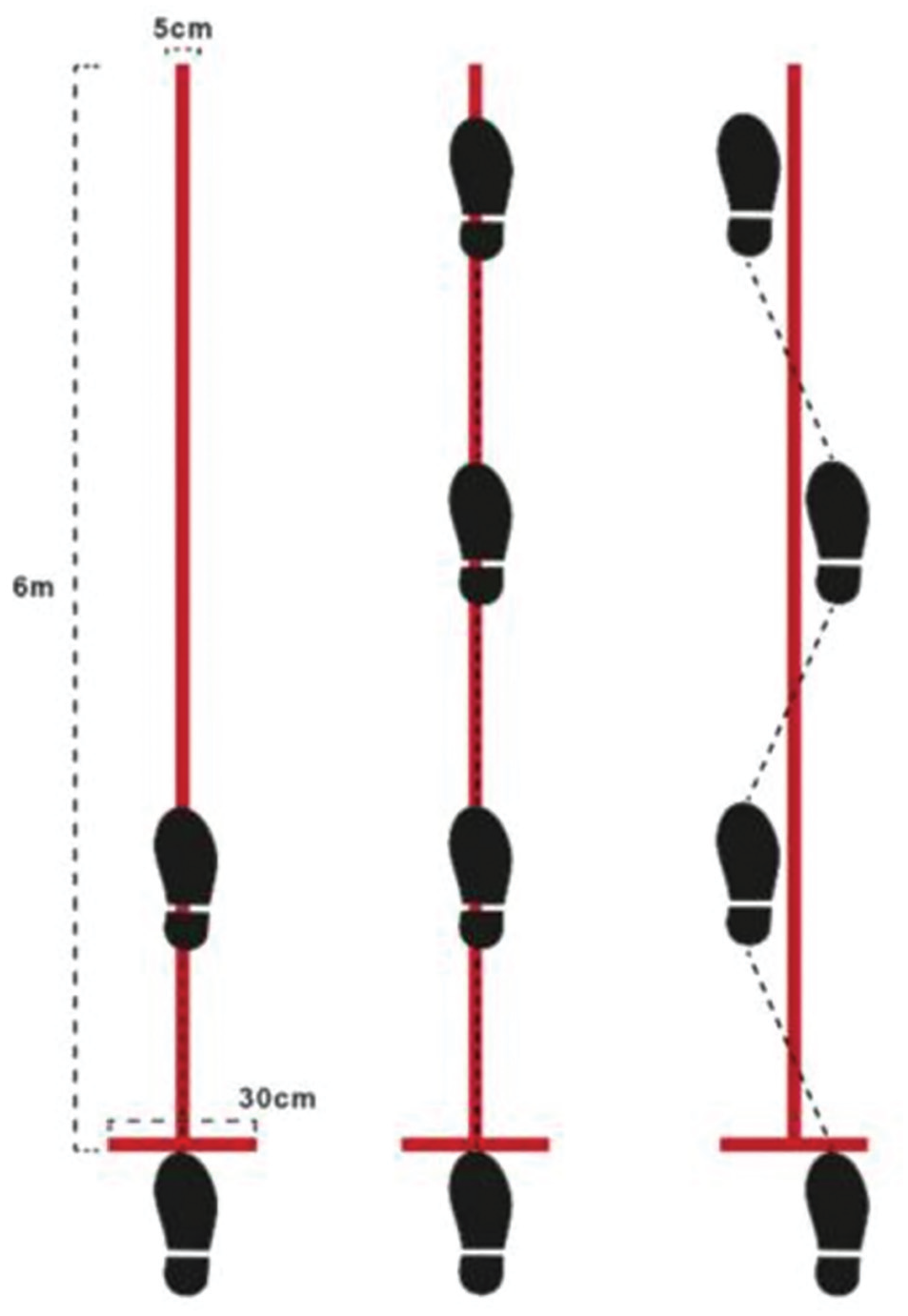
Schematic diagram of the hop test. 11
Y-Balance Test
The YBT exercise kit (The Functional Movement Screen) was positioned on a level testing surface. The angle formed between the anterior lateral tube of the YBT kit and the posterior medial and posterior lateral tubes was set at 135°, while the angle between the posterior medial and posterior lateral tubes was set at 90°. The central area encompassed by all 3 directions constituted the support leg standing area.
Participants stood barefoot on a force platform equipped with the YBT kit, positioning 1 leg with the big toe aligned behind the center horizontal line and directly facing the subject, while the hands were crossed (Figure 4). The other leg sequentially extended in the anterior, posterolateral, and posteromedial (PM) directions, with the distance of each extension recorded in centimeters (cm). After 3 extensions in each direction, the direction of extension was rotated.

Schematic diagram of YBT.
Before the formal test, participants engaged in corresponding warm-up activities. They practiced each directional extension 3 times to acquaint themselves with the movements. The formal assessment commenced after a 5-minute rest period. If a participant failed to extend in any direction during all 3 attempts, the distance was recorded as 0 cm. Testers were prohibited from utilizing the block as a support for the forward-extended leg. Failures were defined as instances of balance loss while standing on 1 leg, significant movement of the standing foot, the extended foot making contact with the ground for support, or failure of the extended leg to return to its initial position. These instances were not included in the data analysis.
Safe Return to Sports
Meredith et al 22 defined RTS as a return to the type, intensity, frequency, and quality of performance as before the injury; thus, in this study, RTS was judged according to whether the postoperative Tegner athletic ability evaluation score and the Marx Activity Rating Scale reached the preinjury level. It has been found 10 that when certain criteria are met, the knee reinjury rate when patients return to sports is reduced by 84%, suggesting that the criteria for RTS safely should include postoperative time, subjective outcome scores, objective assessment of knee function, and psychological readiness assessment. Therefore, the following safe RTS criteria were determined in this study in conjunction with related studies1,3,5,32: (1) postoperative time ≥9 months; (2) lower extremity maximal muscle strength LSI ≥85%; (3) ACL-RSI >65; (4) jump test LSI ≥85%; (5) Y-balance LSI ≥85%; and (6) Tegner score restored to the preinjury level. Anyone who did not fulfill any of the above was considered to have failed to return to sport safely.
Statistical Analysis
SPSS 26.0 (SPSS Inc) statistical software was used to analyze the data. Continuous variables were expressed as means ± standard deviations, and categorical variables were expressed as numbers or percentages. All continuous variables were judged for normality using the Kolmogorov-Smirnov test, and combined with probability-probability and quantile-quantile plots. If the variables were normally distributed, they were compared between groups using an independent samples t test. All noncontinuous variables were compared between groups using the chi-square test. P < .05 was considered statistically significant.
Results
Patient Characteristics
Table 1 summarizes patient characteristics of the 2 groups. Based on the results of the PST performed by 2 surgeons specialized in sports medicine at a senior level, 81 patients were included, with a mean age of 31.47 ± 8.35 years (range, 14-48 years), and a mean follow-up of 4.19 ± 2.48 years, including 57 male (70%) and 24 female patients (30%). A total of 42 patients (52%) had negative PST results (SG), while 46 patients (48%) had positive PST results (MIG). No significant differences were found between the 2 groups in terms of sex, age at surgery, BMI, time from injury to surgery, affected side, and meniscal injury.
Patient Characteristics a

Data are presented as mean ± SD or n (%). BMI, body mass index; MIG, mild rotational laxity group; SG, stable group.
Anteroposterior Laxity of the Knees
The results of the KT-2000 joint kinematics are shown in Table 2. The results showed that the KT-2000 SSD on the healthy side and the affected side of the SG were smaller than that of the MIG; nonetheless, the difference was not statistically significant.
Comparison of the Difference in the Anteroposterior Laxity of the Knees Between the 2 Groups a
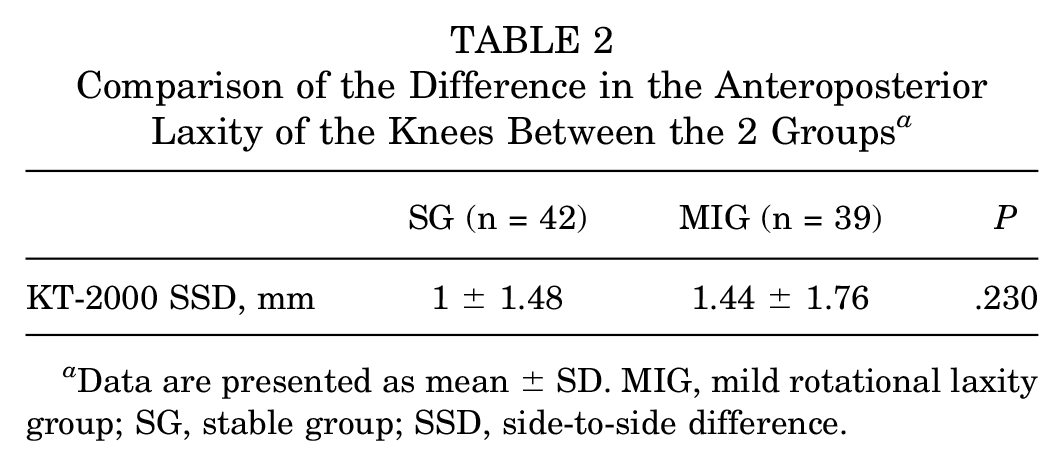
Data are presented as mean ± SD. MIG, mild rotational laxity group; SG, stable group; SSD, side-to-side difference.
Outcomes
No significant difference was observed in the Lysholm, Marx, IKDC, KOOS, and Marx scores between the 2 groups. However, the ACL-RSI score and the Tegner motor level were significantly higher in the SG than in the MIG (69.54 ± 21.34 vs 56.70 ± 19.51; P = .006; 5.81 ± 1.70 vs 4.95 ± 1.93; P = .036) (Table 3).
Comparison of Subjective Scores Between the 2 Groups a

Data are presented as mean ± SD. ACL, anterior cruciate ligament; ACL-RSI, ACL-Return to Sport after Injury Score; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MIG, mild rotational laxity group; Postop, postoperative; SG, stable group.
Performance
A significant difference was observed between the 2 groups in terms of LSI in the jump test, with the SG having a higher LSI in the single-leg hop, triple hop, and cross-over hop test scores than the MIG (78.51 ± 29.62 vs 59.34 ± 37.61 [P = .013]; 83 ± 27.70 vs 65.04 ± 37.22 [P = .017]; 84.24 ± 27.39 vs 68.73 ± 39.69 [P = .046]), with no significant differences in any other aspects of performance (Table 4).
Comparison of the Performance Between the 2 Groups a

Data are presented as mean ± SD. A, anterior; H/Q, hamstring-to-quadriceps; LSI, limb symmetry index; MIG, mild rotational laxity group; PL, posterior lateral; PM, posteromedial; SG, stable group; YBT, Y-balance test.
Return to Sports
In this study, the overall RTS rate was 37% (30/81). The RTS rate was 38.1% (16/42) in the SG and 35.9% (14/39) in the MIG. The safe RTS rate was 7.1% (3/42) in the SG, compared with 2.6% (1/39) in the MIG (Table 5). Among those patients who returned to sports, approximately 18.8% (3/16) in the SG met the criteria for a safe RTS, compared to just 7.1% (1/14) in the MIG. However, the difference was not statistically significant between the 2 groups.
Comparison of RTS Between the 2 Groups a

Data are presented as %. MIG, mild rotational laxity group; RTS, return to sports; SG, stable group;
Discussion
In this study, patients exhibiting negative PST demonstrated significantly enhanced levels of postoperative physical activity compared with the MIG. Furthermore, all metrics evaluating performance in the single-leg hop, triple hop, and cross-over hop tasks exhibited statistically significant elevations in patients with negative PST, as opposed to those with grade 1 PST. Moreover, the SG yielded significantly higher scores on the ACL-RSI scale compared with the MIG, indicating that knee laxity after ACLR may exert a substantial influence on knee function during the short and medium terms, as well as on the recovery process aimed at resuming athletic activities.
Hop tests are generally used to assess the neuromuscular control of the knee, which is poor in ACLR knees during jump landings. 7 Among the 3 jump tests, the single-leg jump test is more sensitive for assessing return to motion after ACLR, 12 and the results of the triple and cross-over hop tests are strongly correlated with the recovery of muscle strength of the quadriceps and hamstrings in the lower extremity; nonetheless, the association with the rotational laxity of the knee is not clear. 2 In this study, no significant difference was observed in the 60 deg/sec isometric muscle strength test between the 2 groups, and the H/Q ratio was similar on the affected side (0.59 vs 0.56; P > .05), whereas the LSI of the hop test in the SG was significantly higher than that of the MIG, which suggests that knee stabilization during dynamic activities affects the function of neuromuscular control, and this functional deficit may result in excessive damage to ligaments, excessive loading on such structures as the joint capsule, and ultimately increasing the risk of ACL reinjury. 32 In other words, this hop test could be used to make a tentative judgment about laxity and objectively evaluate the efficacy of ACLR and the safety of RTS. In previous studies, Jonsson et al 15 found that the difference between the single-leg hop test results of patients with negative PST results and those of patients with positive PST results was not statistically significant at 5 to 9 years of follow-up. Sundemo et al 29 found that the single-leg hop test results of patients with negative PST were better than those of patients with positive PST results at the 2-year postoperative follow-up after ACLR; nevertheless, the difference in findings was not significant, whereas a significant difference was observed at 16 years.
The ACL-RSI scale has been recognized as a reliable and valid tool for evaluating RTS in recent years. In the present study, the ACL-RSI scores of the SG were significantly higher than those of the MIG (69.54 ± 21.34 vs 53.60 ± 21.67; P = .001). According to the Albano 1 standard for ACL-RSI scores in RTS, 54.8% of the SG met the standard, compared with just 35.9% of the MIG. This result suggests that the rotational laxity of the knee after ACLR may influence the psychological status during RTS. Faleide et al 4 showed that the degree of laxity of the knee could be predicted by the ACL-RSI scores, and the psychological scores of the lax knee scores were lower. McPherson et al 21 hypothesized that this was due to the fear of reinjury caused by the inherent instability of the knee, which lowered the psychological score. In contrast, Webster et al 30 found no association between the degree of anteroposterior laxity of the knee and ACL-RSI scores in a 1-way correlation analysis. However, this may be because the patients included in the study were all athletes or sportsmen with high basal muscle strength, which compensated to a certain extent for the mechanical laxity of the knee through plyometric and neuromuscular feedback, thus creating this difference. Thus, the results of this study may not apply to the general population. Psychological monitoring is often overlooked in rehabilitation. This study shows that the ACL-RSI score is associated with knee rotational laxity postoperation, emphasizing the need to address psychological readiness during rehabilitation.
The ultimate goal of testing on performance is also to assess the safety of patients to RTS. RTS is characterized by achieving the preinjury level of sports participation as defined by the same type, frequency, intensity, and quality of performance as before injury in the Panther Consensus. 22 Grindem et al 10 found that even when patients returned to sports after ACLR, they still had a high risk of reinjury, while when certain criteria were met, the rate of knee reinjury when patients returned to sports was reduced by 84%. In this study, the RTS rate in the SG was 38.1% (16/42), of which 18.8% (3/16) met the safe RTS criteria, while the RTS rate in the MIG was 35.9% (14/39), of which 7.1% (1/14) met the safe RTS criteria; however, none of the differences between the groups were statistically significant. The rate of meeting safe RTS criteria was approximately 3 times higher in the SG than in the MIG, and even though the difference between the groups was not significant, the authors concluded that the role of rotational laxity of the knee on safe RTS still could not be ignored. The results of this study showed that patients in the SG had significantly higher postoperative Tegner scores than those in the MIG, and that patients with stable knees had a high level of athletic ability, suggesting that return to preinjury levels may be easier with a stable knee. Zhou et al 32 showed that patients who did not meet the safe return criteria postoperatively had greater lateral tibial translation distances and more pronounced external tibial rotational angles. This seems to indicate that the restoration of knee rotational laxity after ACLR is important for safe RTS.
In addition, the present study found that the percentage of patients who met the criteria for RTS safely was low, regardless of knee stabilization. A study by Sheean et al 27 showed that even if postoperative patients were able to RTS, there was a higher likelihood of reinjury due to functional deficits or insufficient recovery. The results of this study showed a significant decrease in the Marx scores of all postoperative patients, suggesting that the reconstructive surgery affected the patients’ lives and exercise habits, and most of the patients exercised less frequently. The results of the study by Longstaffe et al 19 showed that the RTS rate after ACLR in professional soccer players was 69.8%, which was significantly higher than the RTS rate in the results of the present study. This is mainly due to the difference in the study population. Lindanger et al18,19 also suggested that postoperative rehabilitation is one of the most important factors influencing RTS participation, and rehabilitation under the supervision of a professional rehabilitation therapist is more effective than self-rehabilitation or no rehabilitation at all. 9 However, the goal of professional athletes after surgery is to RTS as soon as possible as well as to regain their original level of competition, and they usually have more comprehensive medical care, receive continuous and individualized rehabilitation and fitness-specific training, et cetera. These are the reasons why the rate of athletes’ RTS is higher than that of the general population in the present study; nonetheless, there are few reports on whether athletes who RTS meet the criteria of safe RTS, and it needs to be explored in greater depth. The results suggest that clinicians should further strengthen patient education, guide patients to set correct rehabilitation goals, and fully inform patients about the importance of postoperative rehabilitation for functional recovery and RTS to encourage them to adhere to rehabilitation training for a safe RTS.
There are certain strengths of this study. Most current reports on knee laxity after ACLR focus on short-term follow-ups and anteroposterior laxity. This study, however, examines the effect of rotational laxity on RTS with a longer follow-up of 2 to 15 years, incorporating PST results. In addition, the present study was more specific about RTS, not only using questionnaires, but also taking into account the objective performance of various aspects of sports, including lower extremity muscle strength tests, hop tests, and YBTs.
Limitations
There are some limitations to this study. First, the PST is a subjective assessment, and there may be bias or inaccurate results due to the patient's muscle tension during the test. However, in this study, the tests were initially conducted without anesthesia by 2 sports medicine experts separately. If the results were inconsistent, further testing was performed under anesthesia to minimize this potential error as much as possible. In addition, our population was not composed of athletes, and that likely could have affected observations of activity levels. Moreover, we have set stricter criteria for assessment of “safe RTS,” thus, comparison to other studies with different criteria may not be valid.
Meanwhile, this was a study with a short-to-medium-term follow-up, and a long-term follow-up will also be conducted.
Conclusion
Mild rotational laxity of the knee after ACLR results in poorer performance in single-leg hop, triple hop, and cross-over hop tests as well as lower-level athletic ability. Patients with stabilized knees had higher ACL-RSI scores than unstable patients, and the stabilized group scored at the return-to-exercise standard while the unstable group did not. In addition, the rotational stability of the knee significantly affected patients’ postoperative exercise levels, with rotational instability of the knee showing lower levels of exercise. In the general population, RTS rates were lower in the short- to medium-term after ACLR, regardless of rotational stability, with most patients failing to meet safe RTS criteria.
Footnotes
Final revision submitted February 10, 2025; accepted March 17, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Regional Ethics Committee (202210), National Institute of Sports Medicine.