
Abstract
Background:
The number of ulnar collateral ligament (UCL) surgical procedures in professional baseball players continues to increase.
Hypothesis:
Performance, injury history, physical characteristics, pitching velocity, elbow torque, and amount of pitching are associated with the risk of a UCL injury resulting in surgery.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
All 30 Major League Baseball (MLB) clubs were contacted for recruitment at Spring Training and the Fall Instructional League in 2015, 2016, and 2017. Pitchers were eligible if they were from the most recent draft and were healthy. Participants completed a questionnaire, a physical examination, magnetic resonance imaging (MRI), and biomechanical testing. The questionnaire included date of birth, previous elbow surgery, and self-reported fastball velocity. The physical examination included measurements of height, weight, and passive range of motion in both shoulders. Elbow MRI assessed for abnormalities of the UCL. During biomechanical testing, fastball velocity was measured, and elbow varus torque was calculated. Pitching volume and injuries resulting in UCL surgery were monitored until the end of 2019. Continuous variables were compared between pitchers with and without UCL surgery using the Student t test. For binary risk factors, significant differences in proportions were determined with the chi-square test. Cox proportional hazards regression was used to model hazard ratios for the associations between risk factor variables and time to injury. An alpha level of .05 was used for all tests.
Results:
Overall, 31 of 305 participants required UCL surgery during the follow-up period. Elbow varus torque was significantly higher for pitchers with a subsequent injury requiring UCL surgery (100.8 ± 18.1 N·m) compared with pitchers without such an injury (94.3 ± 16.1 N·m). The risk of UCL surgery increased 26% for every 10-N·m increase in elbow varus torque. No statistically significant association was found between UCL surgery and body size, history of surgery, fastball velocity, percentage of games pitched as a starter, or UCL abnormalities on MRI, although the 2 pitchers with a full-thickness UCL tear on MRI subsequently underwent UCL surgery.
Conclusion:
High elbow varus torque was associated with a greater risk of UCL surgery. With motion capture technology and biomechanists now part of MLB organizations, teams can analyze and improve the biomechanics of their pitchers to reduce elbow varus torque and the injury risk.
The number of ulnar collateral ligament (UCL) injuries in professional baseball players continues to increase.8,19 While clinical outcomes after UCL surgery in professional baseball players are generally positive,19,24 these procedures necessitate a significant amount of time off for recovery and hinder a player's ability to contribute to his team's success during the recovery process. As such, there has been a significant push to try to decrease the number of UCL injuries in this population. To decrease the number of UCL injuries, modifiable risk factors significantly associated with a UCL injury must be identified.
Numerous studies have investigated risk factors related to a UCL injury in professional baseball. Pitch volume, pitch type, ball velocity, and elbow torque have been identified as risk factors.3,10,14,20,27-30,41,46 Decreased shoulder passive range of motion has also been associated with UCL injuries in professional pitchers.42,51 However, most of these studies have utilized a retrospective design, limiting the strength of their injury prediction and prevention. Furthermore, most of these studies have focused on a single type of risk factor, despite the recognition that no single factor is believed to be the primary contributor to UCL injuries. More research is needed that examines the multifactorial mechanisms that can contribute to the UCL injury risk.
The purpose of this study was to investigate multiple potential risk factors for a UCL injury in professional baseball pitchers using a prospective longitudinal design. It was hypothesized that excessive pitching volume, fastball velocity, and elbow varus torque would increase the risk of UCL injuries. It was also hypothesized that previous elbow surgery, previous shoulder surgery, and insufficient passive range of motion in the throwing elbow or shoulder would increase the risk of UCL injuries.
Methods
After obtaining institutional review board approval from Johns Hopkins University, we contacted all 30 Major League Baseball (MLB) clubs in January 2015. The study purpose and procedures were explained, and all teams were invited to participate. Dates were then scheduled in March 2015 for each participating team at its Spring Training complex for player enrollment and initial data collection. All pitchers on these teams who were drafted in 2014 were invited to participate in the study.
Each pitcher who agreed to participate completed an informed consent process, followed by filling out a pitching and medical history questionnaire at the time of enrollment (ie, baseline). On the questionnaire, the pitcher self-reported his average fastball velocity, previous injuries, and previous surgery. Participants underwent a physical examination conducted by their team's medical staff, which included measurements of height, weight, and passive range of motion in both their throwing and nonthrowing upper extremities. Body mass index was calculated from the player's height and weight. Shoulder and elbow passive range of motion were measured by athletic trainers using goniometers and agreed-upon standardized methods.52,53 There were 4 variables calculated by comparing passive range of motion in the 2 shoulders. Shoulder flexion deficit was flexion of the nonthrowing shoulder minus flexion of the throwing shoulder. Increased external rotation was external rotation of the throwing shoulder minus external rotation of the nonthrowing shoulder. Internal rotation deficit was internal rotation of the nonthrowing shoulder minus internal rotation of the throwing shoulder. Total rotation deficit was internal rotation deficit minus increased external rotation. Additionally, 3 variables were calculated by comparing passive range of motion in the 2 elbows. Elbow flexion deficit was flexion of the nonthrowing elbow minus flexion of the throwing elbow. Elbow extension deficit was extension of the throwing elbow minus extension of the nonthrowing elbow. Total deficit was elbow flexion deficit plus elbow extension deficit. We relied on the teams and their athletic trainers for the collection of range of motion measurements; unfortunately, there were some organizations that did not consistently or successfully collect range of motion data for the study.
We also asked each participant and his team for the player to undergo magnetic resonance imaging (MRI) of the throwing elbow. Some teams told us that their players would not be permitted to participate in the MRI portion of the study. Furthermore, some players on teams agreeing to allow MRI decided that they did not want to participate in this portion of the study. All MRI scans were systematically evaluated, using previously described methods, 18 by 2 orthopaedic surgeons (P.N.C. and B.J.E.) with experience caring for professional baseball players. These surgeons were blinded to the identity and injury history of the players. Elbow MRI scans were examined for the presence of previous UCL reconstruction or repair, previous ulnar nerve transposition, and previous open reduction and internal fixation of the medial epicondyle. The UCL was evaluated for the presence of a tear; whether the tear was partial or full thickness; and whether the tear was located proximally, distally, or at the midsubstance.
A pitcher was considered to have undergone previous elbow surgery if he so indicated on his medical history form, signs of previous surgery were observed on elbow MRI, and/or previous elbow surgery was identified via an Internet search by an investigator of this study (R.F.). The same process was used to determine previous shoulder surgery.
Pitching biomechanical data were also collected at baseline. Biomechanical testing was performed similarly to the methods used in Spring Training 2014 for a previous study. 24 Namely, a 10-camera motion capture system (Motion Analysis) was set up at a designated pitching mound at each participating team's training facility. Each participant wore only his tight sliding pants, baseball socks, spikes, and baseball cap during testing, and 38 reflective markers were attached to his clothing and skin. Markers were attached bilaterally at the clavicle, acromion process, medial epicondyle of the humerus, lateral epicondyle of the humerus, forearm, medial wrist, lateral wrist, anterior superior iliac spine, posterior superior iliac spine, greater trochanter, medial knee, lateral knee, medial malleolus, lateral malleolus, and third toe. In addition, markers were attached at C7; the third metacarpophalangeal joint of the throwing hand; and the front, top, left, and right aspects of the cap. To add asymmetry to assist tracking the body segments, markers were attached to the throwing-side scapula and the heel of the front (nonthrowing-side) foot. After all markers were secured, the pitcher warmed up as he desired, typically with dynamic stretching, followed by flat-ground long toss with another study participant and then warm-up pitches from the mound to a catcher under the supervision of a pitching coach. Once the pitcher indicated that he was ready, he threw 10 full-effort fastballs from the mound to the catcher for data capture. For each trial, the catcher had the target in the middle of the strike zone. The motion capture system tracked the 38 reflective markers at 240 Hz while ball velocity was measured with a radar gun (Figure 1).

Biomechanical testing.
Pitching kinematics and kinetics were determined as previously described.13,20,22,23,25,46,54 Joint center motion of the wrist, elbow, shoulder, and hip were calculated from reflective marker position data. Kinematics of the upper trunk, upper arm, and forearm were then computed from these position data. Inertial properties of the forearm and upper arm were calculated based on the participant's height and weight. Elbow varus torque was computed via inverse dynamics utilizing kinematic data and segment inertial properties. The baseball was considered to be a 0.142-kg point mass in the hand until the moment of ball release. Normalized elbow varus torque was calculated as elbow varus torque divided by body weight and divided by height.
All 30 MLB clubs were contacted again in July 2015, January 2016, July 2016, January 2017, and July 2017 to ask for their participation in subsequent data collection in their upcoming Fall Instructional League or Spring Training. At each of these time points, the process described above for informed consent, history taking, physical examination, MRI, and biomechanical testing was conducted on the organization's pitchers from the most recent draft.
We retained data from each participant from his initial Spring Training or Fall Instructional League; access to the data was not provided to the participants or their teams. The investigators and the teams provided no feedback or intervention to the participants based on their collected data.
The initial design of the study was to follow the performance and injury history of each participant for 5 years. However, because of the unexpected COVID-19 pandemic and the shutdown of baseball in 2020, the study design was modified to follow each participant through the end of 2019. Games pitched, innings pitched, and games started in professional baseball during the follow-up period were provided by MLB.
The outcome in this study was the time to a UCL injury. The date of the injury that required UCL surgery was obtained from MLB's Health and Injury Tracking System. 39 Surgery included UCL reconstruction, UCL repair, and hybrid procedures that were primary or revision cases, but only the first surgical procedure during the follow-up period was considered. Follow-up time was calculated from the date of study entry to the date of the UCL injury or last follow-up time point (dropped out of professional baseball or study end).
Time-to-event analysis was conducted to estimate the probability of remaining injury free and to identify risk factors associated with the time to injury. A Kaplan-Meier curve was plotted to visualize injury-free probability against follow-up time. 11 Cox proportional hazards regression was used to model hazard ratios for the associations between risk factor variables and time to injury. The hazard ratio is a measure of the relative risk of an event occurring between 2 participants whose values of a continuous risk factor differ by 1 unit or whose values of a binary risk factor differ by its presence or absence. A hazard ratio >1 indicates that a variable is positively associated with the UCL injury risk; as values increase, the event hazard increases, and the time to event decreases. 6 Before modeling, descriptive statistics were compared between pitchers with and without UCL surgery during the follow-up period. For all continuous risk factor variables, significant differences in means were determined with the Student t test. For all binary risk factor variables, significant differences in proportions were determined with the chi-square test. Regression analysis was performed in 2 steps. In the first step, univariate regression was conducted individually for all risk factor variables to gauge their strength, independent of other factors. In the second step, multivariate regression adjusted for multiple risk factors simultaneously. The correlation coefficient and variance inflation factor (VIF) were used to detect multicollinearity in the second step; a VIF <5.0 was considered sufficient to ensure no issues of multicollinearity for regression inference. 49 An alpha level of .05 was used for significance for each test.
Results
Tables 1 to 3 show descriptive statistics comparing pitchers who did and did not undergo UCL surgery during the follow-up period and are separated into (1) pitching, medical history, and physical characteristics; (2) biomechanical measurements; and (3) performance at follow-up.
Pitching, Medical History, and Physical Characteristics a

MRI, magnetic resonance imaging; UCL, ulnar collateral ligament.
These included ligaments with any scarring, a heterogeneous signal, partial tears, complete tears, or calcification within the ligament.
Significant at alpha = .05.
Measurements From Initial Biomechanical Testing a

Data are presented as mean ± SD. UCL, ulnar collateral ligament.
Significant at alpha = .05.
Performance at Follow-up a

Data are presented as mean ± SD. UCL, ulnar collateral ligament.
In Table 1, the only significant difference was in full-thickness UCL tears; 2 pitchers had a full-thickness UCL tear noted on MRI, and both pitchers subsequently underwent UCL surgery. There was a trend regarding pitching handedness in which 87% of the injured pitchers and 69% of the noninjured pitchers were right-handed, but this trend was not statistically significant (P = .063) and could simply be the result of more right-handed pitchers (71%) in the study. Some of the variables in Table 1 had high missingness, for reasons discussed in the Methods section; of the 305 participants who were enrolled and provided consent, passive range of motion variables were obtained for 134 pitchers, and MRI variables were obtained for 153 pitchers.
In Table 2, elbow varus torque was significantly greater in the injured pitchers (100.8 ± 18.1 N·m) than in the noninjured pitchers (94.3 ± 16.1 N·m). Although 266 pitchers participated in biomechanical testing, unfortunately, one team instructed its pitchers to pitch at reduced effort during testing one season; biomechanical data for these pitchers were discarded, resulting in full-effort biomechanical data for 248 pitchers.
Table 3 compares average innings pitched per game and percentage of games started during the follow-up period. On average, noninjured and injured players pitched the same number of innings per game. Although injured pitchers started more games, on average, the difference was not statistically significant.
Overall, 31 of 305 pitchers underwent UCL surgery during the follow-up period. Figure 2 shows the Kaplan-Meier curve and risk table for the study population. Each pitcher entered the study and became “at risk” at follow-up time 0. By the end of the first follow-up year, 10 pitchers underwent UCL surgery, and 41 pitchers dropped out of professional baseball, leaving 254 remaining healthy pitchers. The probability of remaining injury free until the end of the fourth follow-up year was 85% (95% CI, 80%-91%). Alternatively, the cumulative incidence of UCL injuries at follow-up time 4, based on the inverse of the Kaplan-Meier curve, was 15% (95% CI, 9.5%-21%). As the longest follow-up time was about 4.5 years, the probability of being injury free at follow-up time 5 could not be calculated.
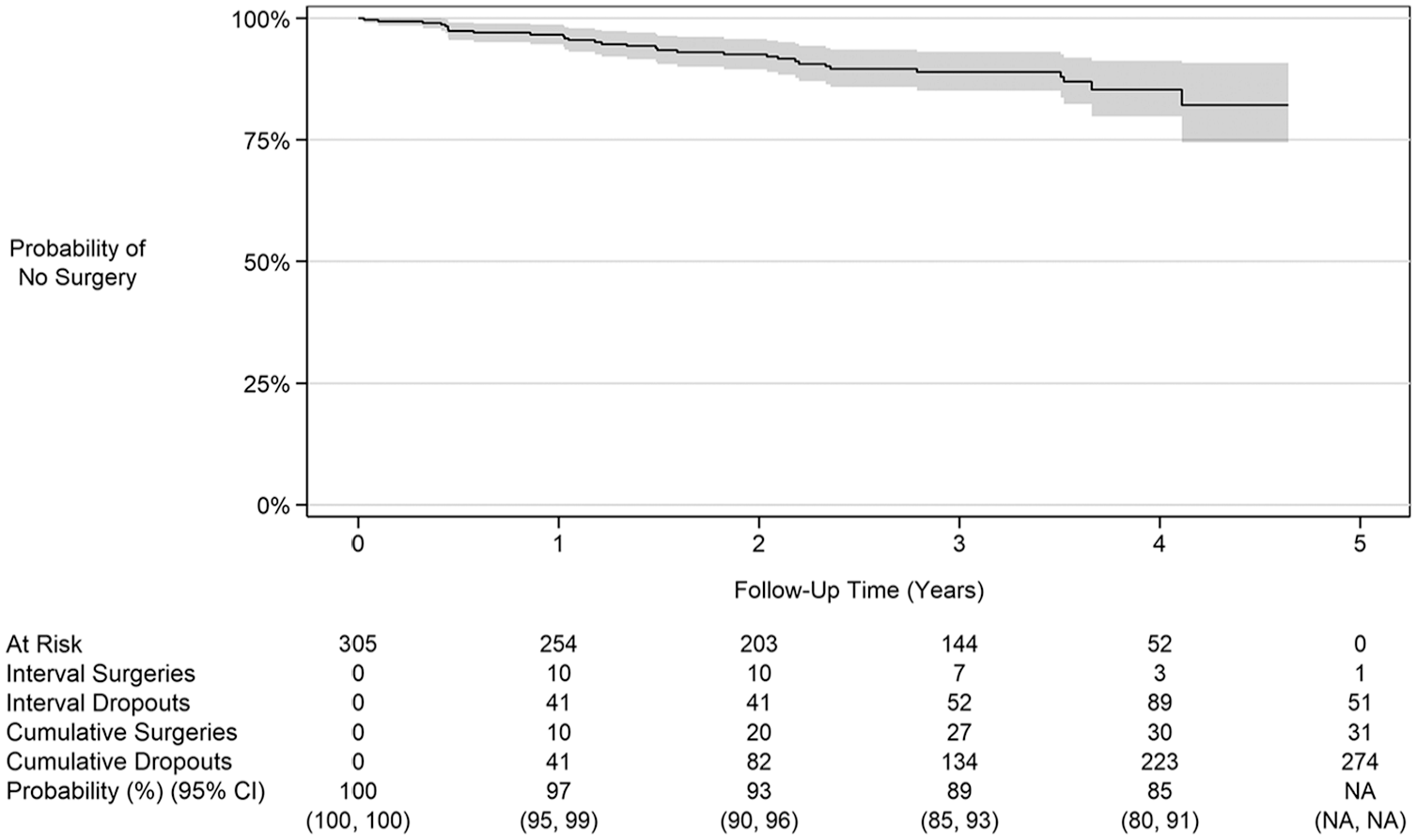
Kaplan-Meier curve.
Univariate Cox proportional hazards regression revealed a significant correlation (P < .05) for elbow varus torque (Table 4). Because of the small number of left-handed pitchers in the UCL surgery group (n = 4) and the level of missingness and low counts in the range of motion and MRI data (with no noninjured pitchers having a full-thickness UCL tear on MRI and only 2 injured pitchers who did), these variables were not considered in any regression analyses. Thus, the only meaningful finding was a hazard ratio of 1.02 (95% CI, 1.00-1.05) for elbow varus torque. The hazard ratio can be interpreted as a 2% increase in the risk of a UCL injury between 2 pitchers whose torque values differ by 1 N·m. Given the relatively large range of torque values (60.5-161.8 N·m), it is reasonable to interpret a >1-unit difference. For example, for a 10-N·m difference, the hazard ratio was 1.26 (95% CI, 1.01-1.56), which signifies a 26% increase in the risk of a UCL injury.
Univariate and Multivariate Regression Results

Significant at alpha = .05.
Although elbow varus torque was the only meaningful finding from univariate regression analysis, a multivariate model (Table 4) was constructed to determine if elbow varus torque remained significant after adjusting for other factors. Variables with the same or higher level of completeness as elbow varus torque (n = 248) were considered to preserve the sample size. Because of multicollinearity indicated by large VIF values in intermediate models, weight, body mass index, normalized elbow varus torque, and percentage of games started were removed. In the final adjusted model for 248 pitchers, elbow varus torque remained a significant risk factor with an unchanged hazard ratio of 1.02 (95% CI, 1.00-1.05).
Discussion
As hypothesized, elbow varus torque was a significant risk factor for a serious elbow injury requiring UCL surgery. This is an important and timely finding. Since the seminal article proposing the relationship between elbow varus torque in pitching and UCL injuries 3 decades ago, 23 dozens of biomechanical studies have implied or explicitly stated that increased elbow varus torque correlates with an increased risk of UCL injuries.2,7,13,15,17,26,28,34,46,47 However, only one previous study has investigated this relationship. Anz et al 3 analyzed pitching biomechanics for 23 professional pitchers and prospectively followed them for 3 seasons. That study showed significantly higher (P = .013) elbow varus torque in the 9 injured pitchers (91.6 ± 23.0 N·m) than in the 14 noninjured pitchers (74.7 ± 22.4 N·m). This is consistent with the findings from the pitchers who completed biomechanical testing in the current study, as elbow varus torque was significantly higher (P = .049) in our 28 injured pitchers (100.8 ± 18.1 N·m) than in our 220 noninjured pitchers (94.3 ± 16.1 N·m) (Table 2).
Identifying the critical relationship between elbow varus torque and UCL surgery is particularly timely because in the past decade, biomechanical analysis has evolved from a specialized method used by select professional pitchers and organizations to a principal component in pitchers’ health and success throughout MLB. With the growing importance of biomechanics in the sport, the American Baseball Biomechanics Society (www.BaseballBiomechanics.org) was founded in 2020. The introduction of markerless motion capture technology has empowered MLB and all 30 MLB organizations to collect pitching biomechanical data during games and practices.21,48 Although there are inherent complications in comparing data from markerless motion capture to marker-based motion capture, both modalities provide consistent pitching data.25,29 A number of markerless motion capture companies have provided services during the last few years in MLB and Minor League Baseball. The 2 most prevalent motion capture companies in professional baseball (Hawk-Eye and KinaTrax) are now both owned by the same parent company (Sony), with the intention of broadening the reach and value of biomechanics in professional baseball (www.sony.net/corporate/information/news/202410/24-1016E/). Inertial measurement unit technology is also now used in professional and amateur baseball, providing another modality to quantify and monitor elbow varus torque during pitching and throwing.5,9,16,32,35,37,38,43,50
Many previous studies have reported elbow pitching torque in absolute values (typically in N·m),2,3,17,20,23,24,47 while in recent years, many other studies have reported unitless, normalized elbow pitching torque.13,17,34,46 The decision on whether to scale varus torque is based on the issue of whether UCL strength is related to body size. Beason et al 4 examined cadaveric elbow specimens from 20 young men and found no correlations between UCL failure torque and UCL stiffness with body weight and height. The implications from that study are that biomechanical studies should not normalize elbow varus torque by weight and height. The results of the current study support this conclusion, as UCL injuries were associated with elbow varus torque (in N·m) but not with normalized elbow varus torque. Thus, pitchers and their coaches should strive to reduce elbow varus torque. A recent article illustrated key kinematic parameters associated with elbow varus torque and other variables. 15 Among the modifiable mechanical factors associated with elbow kinetics were front foot position and angle at landing, shoulder external rotation at foot contact, maximum shoulder external rotation, and proper sequencing of the kinematic chain of events. Shoulder abduction and trunk tilt were also associated with elbow stress.
While elbow varus torque data are not widely available to the public, pitch velocities are displayed on scoreboards at professional games and also recorded and provided for analyses. A recent study published by MLB surveyed more than 200 experts.1,31 The consensus was that the continuously increasing pitch velocity during recent years and the focus on pitching with maximal effort in professional baseball are primary contributors to rising UCL injury rates.1,31 Biomechanical studies have shown a strong correlation between fastball velocity and elbow varus torque within an individual pitcher.33,44,46 However, the correlation between fastball velocity and elbow varus torque across multiple pitchers is very weak.33,36,40,44,46 Thus, the biomechanical literature suggests that on its own, fastball velocity is not a strong indicator of elbow varus torque associated with UCL injuries. This is consistent with the results of the current study, showing no difference in fastball velocity (during biomechanical testing or self-reported fastball velocity) between the injured and noninjured pitchers. Keller et al 27 also found no difference in preinjury fastball velocity for MLB pitchers who sustained a UCL injury compared with that for a matched control group. In contrast, systematic reviews and meta-analyses of MLB pitchers concluded that fastball velocity was a UCL injury risk factor in professional baseball.28,42 Thus, pitchers should vary the velocity and effort of their pitches instead of throwing all pitches with maximum effort. In addition to reducing cumulative elbow torque (and the UCL injury risk), varying the effort may be effective in throwing off the timing of opposing batters.
The hypothesis that a previous injury or previous surgery increases the risk of injuries during the follow-up period was not supported by the data. The current study found no statistically significant association between UCL abnormalities on initial MRI and UCL injuries during the follow-up period. The current study also found no association between previous elbow or shoulder surgery and injuries during the follow-up period. This supports the findings of a previous 8-year prospective study of elbow injuries in 296 professional pitchers, which showed no association (P = .70) between previous elbow injuries and elbow injuries during the follow-up period. 51 A 10-year prospective study of 407 Minor League Baseball pitchers found a trend of previous arm injuries in their prediction model of arm injuries, but this trend was not statistically significant (P = .07). 45 It should be noted that initial MRI for 2 pitchers in the current study showed a full-thickness UCL tear, and both of these pitchers underwent UCL surgery during the follow-up period.
This study also found no difference in passive range of motion between the injured and noninjured pitchers. In contrast, a prospective study by Wilk et al 51 found that deficits in total rotation and flexion of the shoulder were significant risk factors for an elbow injury. While that study included a similar sample size of professional pitchers (n = 296) to the current study, they prospectively followed their participants for a longer time (8 years) and had a broader definition of an elbow injury (placement on the disabled list). Consequently, their study included a greater number of injured pitchers (n = 38) than the current study, providing more power for statistical analysis. The objective of the current study was not simply to identify factors leading to time on the injured list but to determine the risk factors specifically for a UCL injury requiring surgery.
The current study found no association between height and the risk of injuries. This supports previous research of professional pitchers, which found no relationship between height and the risk of UCL injuries.10,12,14 The current study also found no association between weight and the risk of injuries. However, 2 previous studies reported greater weight for the injured group than for the noninjured group.10,12
It is difficult to classify a professional pitcher as a pure starter or reliever, as pitching role may be fluid, especially during a pitcher's early career. No difference was found between injured and noninjured groups in the percentage of games as a starting pitcher. Pitching volume, expressed as average innings pitched per game, was also not a risk factor for injuries. More detailed performance data, such as average and maximum fastball velocities by season, were not available for this study but may have allowed for better workload comparisons between injured and noninjured groups.
Because of the COVID-19 pandemic, MLB shortened the 2020 season from 162 games to 60 games per team and canceled all Minor League Baseball games. As such, the amount of pitching was not normal. The number of UCL surgical procedures in professional baseball (MLB and Minor League Baseball) in 2020 and 2021 were unusual as well (Figure 3). Less pitching in 2020, combined with the pandemic-related restricted availability of surgery, led to a low number of surgical procedures that year. Players pitching a lot more in 2021 than in 2020, as well as the availability of surgery, led to an unusually high number of surgical procedures. Thus, the decision to modify the prospective study design in progress was not desirable but was necessary.
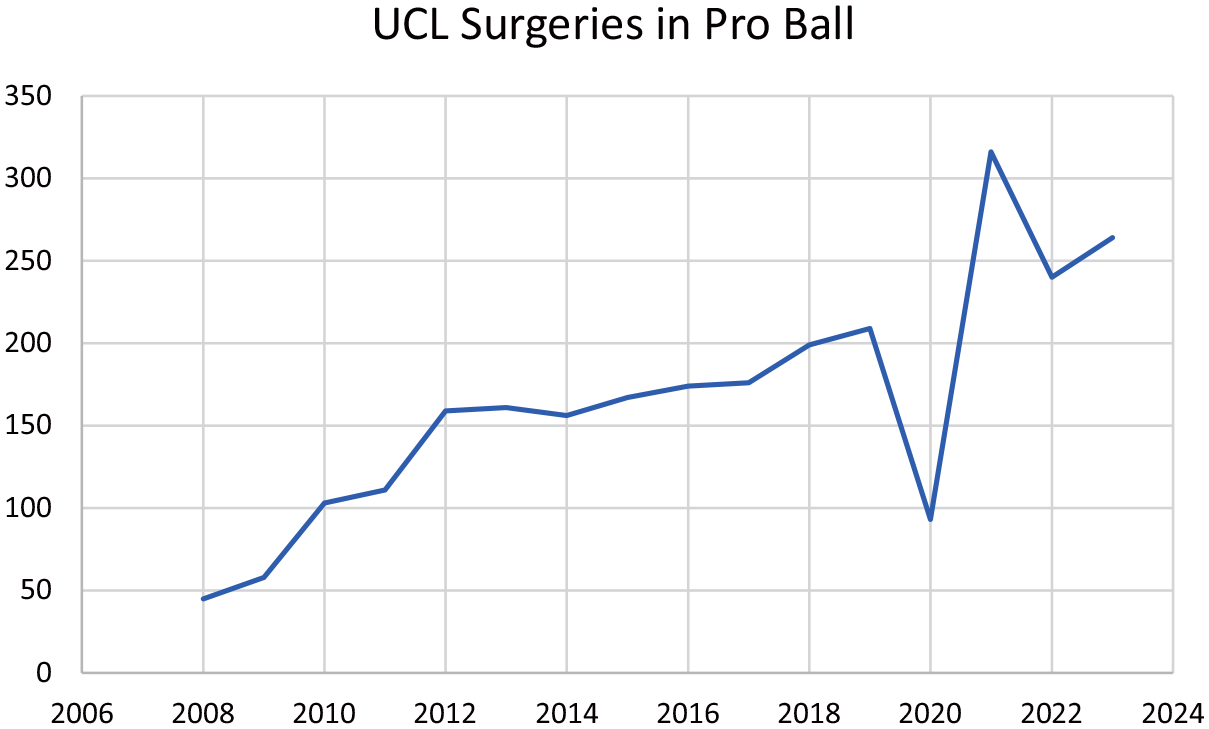
Number of ulnar collateral ligament (UCL) surgical procedures in professional baseball (Major League Baseball and Minor League Baseball) each calendar year during a 15-year span.
As with most studies of this size, this study had underlying limitations that should be noted. Notably, medical history, physical examination, and biomechanical data were obtained only at the beginning of the study and not monitored continuously throughout each pitcher's follow-up period. Metrics such as body weight, passive range of motion, fastball velocity, elbow varus torque (via biomechanical testing), and UCL integrity (via MRI) likely changed throughout the follow-up period for many of the pitchers. While players may have evolved during the follow-up period, initial measurements described baseline characteristics and differences for the large sample of study participants. Furthermore, pitchers were evaluated only at the beginning of their professional baseball careers. Ideally, future research should include measurements of potential risk factors throughout the career of professional pitchers. Fastball velocities during Spring Training and the Fall Instructional League were less than self-reported velocities during competition. This is a historical pattern in biomechanical studies of baseball pitching. Because all participants in the current study were assessed in similar Spring Training and Fall Instructional League bullpen settings, it is reasonable to assume that torque differences between injured and noninjured pitchers in these settings reflect differences between these groups in competition. Another limitation was the relatively low number of participants in the injured group (n = 31). Considering that Figure 3 shows only 925 UCL surgical procedures during the 5-year follow-up period of this study (2015-2019) among the thousands of athletes who pitched in Minor League Baseball and MLB during this time frame, the 10% incidence rate (31/305) of procedures in the current study seems reasonable. A power analysis was conducted as part of the study design. However, as mentioned, because of the COVID-19 pandemic and its effect on professional baseball, the study ended with data collection in 2019, earlier than the full 5 prospective years for all enrolled pitchers, which impacted the sample size. As a result, the study may have lacked sufficient statistical power to detect differences. In addition, some measurements were not collected for all participants; thus, finding statistically significant differences for such variables was even more challenging. Finally, only fastball biomechanics was quantified in this study. Future research analyzing associations between pitching biomechanics of other pitch types and injuries is warranted.
Conclusion
Elbow varus torque was significantly higher for pitchers with subsequent UCL surgery compared with pitchers without subsequent UCL surgery. The risk of UCL surgery increased 26% for each 10-N·m increase in elbow varus torque. No association was found between UCL surgery and body size, history of surgery, fastball velocity, percentage of games pitched as a starter, and UCL abnormalities on MRI, although the 2 pitchers with a full-thickness UCL tear on MRI subsequently underwent UCL surgery. To limit the risk of UCL surgery, pitchers should avoid pitching biomechanics that produce excessive elbow varus torque. With motion capture technology and biomechanists now part of MLB organizations, teams can analyze and improve the biomechanics of their pitchers to reduce elbow varus torque.
Footnotes
Acknowledgements
The authors thank the numerous athletic trainers, physicians, biomechanists, players, and front office personnel who participated and helped make this project work.
Final revision submitted April 15, 2025; accepted April 25, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by Major League Baseball (MLB). C.W., K.M.P.P., and F.C.C. have received salary support through a Johns Hopkins University–MLB contract. G.S.F. is a paid consultant for MLB. P.N.C. has received consulting fees from DePuy, Responsive Arthroscopy, and Exactech; is a paid speaker for DePuy and Exactech; has received intellectual property royalties from DePuy, Exactech, and Responsive Arthroscopy; and has equity in Titin KM Biomedical. B.J.E. has received consulting fees from Arthrex and DePuy and research support from Arthrex, DePuy, Linvatec, Smith & Nephew, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Johns Hopkins University.