
Abstract
Background:
Although previous reports have stated that the addition of a fibrin clot to an allograft can effectively inhibit femoral bone tunnel enlargement (BTE) after anterior cruciate ligament reconstruction (ACLR), no relevant study has quantitatively evaluated the chronological changes in the cross-sectional area (CSA) of the bone tunnel on 3-dimensional computed tomography (3D-CT) images in double-bundle ACLR (DB-ACLR) with hamstring tendon autografts.
Purpose:
To evaluate whether adding a fibrin clot to a hamstring autograft would reduce postoperative femoral BTE by means of 3D-CT image analysis.
Study Design:
Cohort study; Level of evidence, 3.
Method:
A total of 21 patients with fibrin clot who underwent anatomic DB-ACLR using hamstring tendon autografts and 24 control patients without fibrin clot were included in the study. In preparing the graft, a fibrin clot was placed between the 2 strands of the graft end to be inserted into the femoral bone tunnel. The CSAs of the anteromedial (AM) and posterolateral (PL) femoral bone tunnels at the intra-articular aperture, 5 mm and 10 mm from the tunnel aperture, were measured on 3D-CT images at 1 week and 1 year postoperatively, and the difference between the 2 time points was defined as the BTE.
Results:
In the autograft group with fibrin clot, a significantly smaller BTE ratio was observed in the AM tunnel 5 mm (P = .003; with fibrin clot: 29.3% ± 58.1%; autograft alone: 58.8% ± 57.8%) and 10 mm (P < .001; with fibrin clot: –8.0% ± 43.7%; autograft alone: 42.3% ± 39.7%) from the intra-articular tunnel aperture and in the PL tunnel at all levels (P = .048, P < .001, and P < .001; with fibrin clot: 49.1% ± 89.3%, 7.9% ± 28.4%, and −5.1% ± 25.6%; autograft alone: 89.8% ± 57.0%, 28.9% ± 26.8%, and 51.4% ± 38.6%, respectively) compared with controls who received only autograft.
Conclusion:
Adding a fibrin clot to the autograft of an anatomic DB-ACLR was associated with a decreased BTE at 1 year. This effect was more evident in the PL tunnel and the midportion of the AM tunnel.
Keywords
Anterior cruciate ligament reconstruction (ACLR) using an autogenous tendon graft is a widely performed procedure for active patients with anterior cruciate ligament (ACL) insufficiency after injury. There have been a number of studies investigating factors that may influence surgical outcomes.27,39 Among such factors, bone tunnel enlargement (BTE) after ACLR is considered a postoperative problem that may be associated with poor healing at the graft-bone interface and difficulty in performing revision surgery due to bone loss at the anatomic tunnel position. 37 BTE is caused by biological and/or mechanical factors. 10 Biological factors reportedly associated with BTE include immune or inflammatory responses to the grafts known as “synovial bathing effect” that trigger a cytokine-induced osteolytic response, a peri-implant inflammation response, and cell necrosis due to the presence of ethylene oxide which is associated with the implant.6,10,11,13 With regard to mechanical factors, it has been reported that graft micromotion, referred to as the “bungee cord effect” or “windshield wiper effect”; bone tunnel malposition; and aggressive rehabilitation protocols can affect graft-bone healing and lead to BTE.4,12,33
Fibrin clots can function as a scaffold, providing structural support and supplying platelet-derived growth factors.2,24 In our practice, intraoperative preparation and insertion of fibrin clots in the repaired site have been utilized as an augmentation to enhance tissue healing in meniscal or cartilage repair procedures.22,25 In addition, favorable results have been published for the use of fibrin clot in ACLR with an animal model. 9 In a recent clinical study, it was reported that in ACLR with a single-bundle allograft, the fibrin clot prevents BTE from being measured on plain radiographs. 31 However, few studies have investigated the effect of fibrin clots in anatomic double-bundle ACLR (DB-ACLR) based on accurate assessment of BTE by 3-dimensional (3D) reconstructed computed tomography (CT) images.
The aim of this study was to evaluate, using 3D-CT imaging analysis, whether the addition of a fibrin clot to an autograft hamstring graft reduces postoperative BTE. It was hypothesized that in anatomic DB-ACLR, using an autograft implanted with a fibrin clot would reduce femoral BTE compared with an autograft alone.
Methods
Study Design and Patient Selection
The study is a retrospective comparative study. Its protocol was approved by the Ethics Review Board at our institution (No. 4095), and informed consent was obtained from all patients for inclusion in an institutional database.
A consecutive series of patients who underwent primary anatomic DB-ACLR with autogenous hamstring grafts from April 2017 to March 2022 were included in this study. All patients who received ACLR either with or without fibrin clot underwent CT imaging 1 week and 1 year after surgery. Exclusion criteria were concomitant ligament reconstruction or bone surgery, lack of CT imaging data at the 2 postoperative time points (1 week and 1 year), and loss to follow-up before 1 year. ACLR with fibrin clot application has been performed at our institution since it was first introduced in April 2019. This study compared the results of ACLR with fibrin clot implantation after April 2019 to historical control participants who underwent ACLR without fibrin clot before April 2019.
Surgical Procedure
All patients underwent surgery using the same ACLR technique 18 by 3 senior knee surgeons (T.I., R.K., and S.O.). Only the semitendinosus tendon was harvested in all cases and prepared into 2 double-stranded tendon grafts, one for the anteromedial (AM) bundle and one for the posterolateral (PL) bundle. At the same time, the fibrin clot was prepared using a previously reported technique. 1 At the start of the procedure, 25 mL of venous blood was drawn from the dorsum of the patient’s foot and collected in a sterile beaker. The blood was stirred with a glass rod for about 10 minutes until a clot formed (Figure 1A). The clot attached to the glass rod was then wiped off using a clean dry surgical gauze and squeezed until hard (Figure 1B). After longitudinally splitting it into 2, each clot was placed between the strands at the folded end of the graft for both the AM and PL grafts, which were inserted into the femoral bone tunnel (Figure 1C). In this study, fibrin clot insertion into the graft was conducted only on the femoral side, because the incidence of BTE has been generally higher on the femoral side in comparison with the tibial side.5,16,21

Method of autograft preparation with fibrin clot. (A) About 25 mL of venous blood was obtained and poured into a sterile beaker. The blood was stirred with a glass rod to create a fibrin clot. (B) The clot attached to the glass rod was wiped off and squeezed with gauze to harden it. The prepared clot was divided longitudinally into 2 pieces, and each piece was placed between the folded ends of the graft, which was inserted into the femoral tunnel. A circumferential suture was placed around the femoral and intra-articular portions of the graft to secure the clot and stabilize the limbs of the graft. (C) Final appearance of the graft augmented with fibrin clot.
For ACLR, both femoral and tibial bone tunnels were drilled using the outside-in technique, with diameters corresponding to the size of each graft. The femoral AM and PL tunnels were positioned posterior to the lateral intercondylar ridge, and the tibial AM and PL tunnel locations were determined using the residual footprint and anterior horn of the lateral meniscus as landmarks. Endobutton CL (Smith & Nephew Endoscopy) was used for graft fixation on the femoral side, and 2-post method fixation with a screw post (6.5-mm cancellous screw; Arthrex) was used on the tibial side. When fixing the graft to the tibia, first, the AM bundle graft was fixed to the post screw at 20° of knee flexion while maximum tension was manually applied after checking for changes in graft length through a range of motion. Then, the PL bundle graft was similarly placed at 0° of knee flexion.
CT Measurement for Assessment of BTE
All patients who received ACLR with or without fibrin clot underwent CT scans 1 week and 1 year after surgery following our standard protocol for assessments of bone tunnel location and geometry. A 256-slice multidetector CT scanner (SOMATOM Definition Edge; Siemens) was used with a slice thickness of 0.7 mm. The size of the bone tunnel was calculated by measuring the cross-sectional area (CSA) using 3D-CT image analysis software with the region of interest method (ZioCube imaging software; Ziosoft Inc). CSA measurements on CT images were conducted at the following 3 levels for both the AM and PL tunnels: at the tunnel aperture and 5 mm and 10 mm from the tunnel aperture, along the axis of the bone tunnel. First, the plane of the intra-articular tunnel aperture was established on the 3D-CT image, and the CSA of the bone tunnel was measured on that plane (Figure 2A). Inside the bone tunnel, the CSA was measured on a plane perpendicular to the axis of the bone tunnel (Figure 2B). The CSA was measured at 1 week and 1 year after surgery, and the relative change in CSA between the 2 time points (BTE ratio) was calculated using the following formula:

Measurement method of the cross-sectional area (CSA) of the femoral tunnel on 3-dimensional reconstructed computed tomography images. Regions of interest for the CSA measurement were established at the following 3 levels: (A) at the tunnel aperture and (B) at 5 and 10 mm from the aperture, along the bone tunnel axis. (C) A case showing coalition of the bone tunnel at the aperture.
Cases with tunnel coalition at 1 week and/or 1 year were excluded from CSA measurements at that level (Figure 2C).
Statistical Analysis
To ensure the accuracy of the statistical analysis, the methods used were reviewed by a qualified statistician (T.T.), and their recommendations were incorporated. Data are presented as mean ± standard deviation. Statistical analysis was performed using JMP Pro Version 16.0.0 (SAS Institute Inc), and a P value <.05 was considered statistically significant. The Shapiro-Wilk test was used to check the normality of the distribution of continuous variables. For the comparison of continuous variables (age, body mass index, Tegner activity score, CSA, and BTE ratio) between the autograft-only group and the autograft with fibrin clot group, an unpaired t test was used for normally distributed variables and a Mann-Whitney U test for nonnormally distributed variables. A chi-square test was used to compare categorical variables (operated side, sex, and comorbidities) between the 2 groups. The intraclass correlation coefficient (ICC) was used to assess the reliability of intra- and interobserver CSA measurements. All measurements were taken by 2 different orthopaedic surgeons (N.S. and S.O.). One of the observers (N.S.) measured all parameters twice, with a minimum interval of 2 weeks between the 2 measurements. A priori power analysis was conducted to determine the sample size required to detect the difference in BTE ratio between the 2 groups based on the values in the literature by Surer et al, 31 who investigated BTE after single-bundle ACLR. Consequently, it was shown that a power of 0.8 would require 21 patients in each group.
Results
Patient Population
Considering the results of the power calculation, 63 patients who underwent anatomic DB-ACLR during the study period were initially included in the study. The initial patient population consisted of 26 patients who underwent anatomic DB-ACLR with only a hamstring tendon autograft between April 2017 and March 2019 and 37 patients who underwent anatomic DB-ACLR with an autogenous hamstring graft with fibrin clot implantation between April 2019 and March 2022. During the process of data acquisition for the study, 5 patients in the autograft-alone group were excluded for a lack of CT imaging data at the 2 time points (4 males and 1 female, with 3 right-side cases and 2 left-side cases). In the fibrin clot group, there were 37 eligible patients. Thirteen patients (6 males and 7 females, with 6 right-side cases and 7 left-side cases) were excluded from the subsequent study analysis. Therefore, 21 patients who underwent anatomic DB-ACLR autogenous hamstring graft alone (autograft-alone group) and 24 patients who underwent anatomic DB-ACLR autogenous hamstring graft with fibrin clot (fibrin clot group) formed the basis of this study. The patient selection process is shown in Figure 3. The mean time periods from surgery to the 1-year CT examination were 12.2 ± 0.37 months and 12.1 ± 0.40 months in the fibrin clot and autograft-alone groups, respectively.

Flowchart showing selection of the study population. ACL, anterior cruciate ligament.
Patient demographics of the 2 groups can be found in Table 1. There were baseline differences between groups in sex and operated side. Concomitant meniscal surgery was performed in 14 knees with medial meniscal injuries, 4 knees with lateral meniscal injuries, and 5 knees with bilateral meniscal injuries. None of the included cases were treated with concomitant ligament reconstruction, osteotomy, or osteochondral grafting.
Demographic Information of All Included Patients a
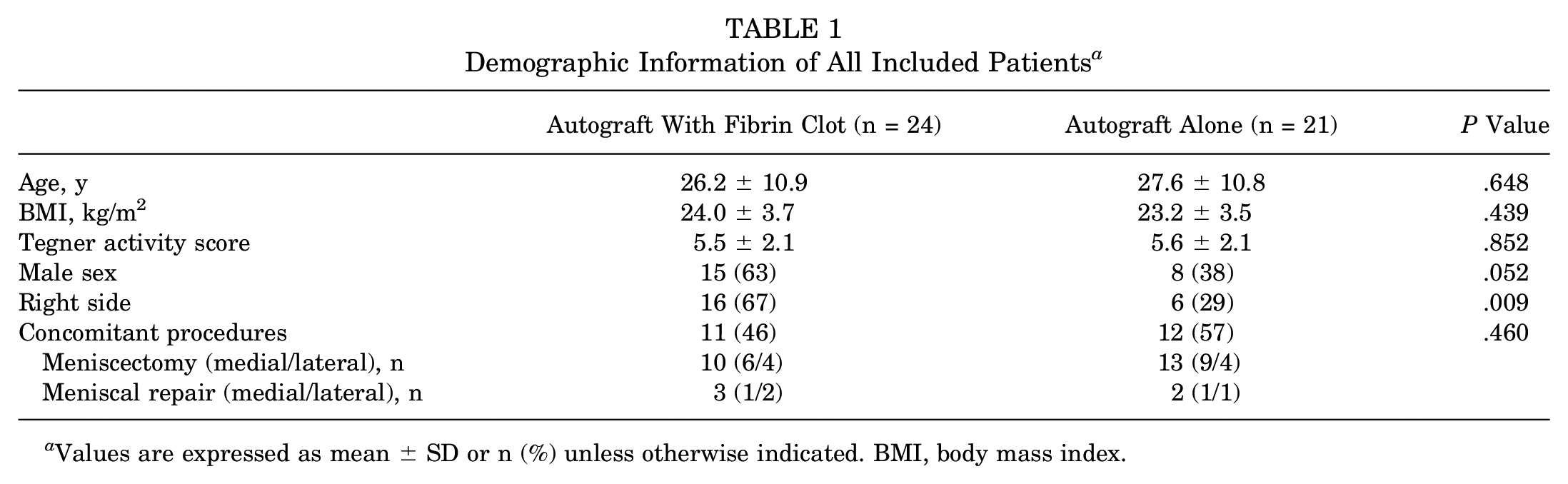
Values are expressed as mean ± SD or n (%) unless otherwise indicated. BMI, body mass index.
CT Measurement of Tunnel CSA
To assess the reliability of the CT measurements, 1 observer (N.S.) repeated the tunnel CSA measurements at intervals of at least 2 weeks, and 2 observers (N.S. and S.O.) independently measured all cases. The intra- and interobserver reliability of the CT measurements was then evaluated by ICCs. Reliability assessments showed that both intra- and interobserver reliability were >0.9 for all CSA measurements (intraobserver reliability, 0.969; interobserver reliability, 0.960). Based on the high reliability confirmed by the reliability analysis, this study used the mean value derived from the 2 investigators’ assessments in the analysis.
Based on confirmation of normal distribution for each of the continuous variables, unpaired t tests were performed for the Tegner activity score, postoperative CSAs at the AM and PL tunnel apertures, and BTE ratio at the AM tunnel aperture. As for other continuous variables with nonnormal distribution, the Mann-Whitney U test was performed for the comparative analysis. Tunnel coalition was not observed in any cases 1 week postoperatively, while coalition was identified in 14 cases at 1 year after surgery: 8 cases in the fibrin clot group and 6 cases in the autograft-only group. All of these were found only at the bone tunnel aperture. These cases were excluded from the CSA measurements, leaving 16 cases in the fibrin clot group and 15 cases in the autograft-only group for tunnel aperture BTE analysis.
Although CSA measurements taken 1 week after surgery showed no significant differences between the 2 groups at all levels (Table 2), CSA measurements taken 1 year postoperatively showed significant intergroup differences at all 3 levels, with significantly smaller values measured in the fibrin clot group (Table 3).
Bone Tunnel CSA (mm2) on 3D-CT Images Measured 1 Week Postoperatively a

Values are expressed as mean ± SD. AM, anteromedial; CSA, cross-sectional area; PL, posterolateral; 3D-CT, 3-dimensional computed tomography.
Bone Tunnel CSA (mm2) on 3D-CT Images Measured 1 Year Postoperatively a

Values are expressed as mean ± SD. Bold P values indicate statical significance. Cases with tunnel aperture coalition were excluded from the analysis. Therefore, the mean cross-sectional area (CSA) values at the bone tunnel aperture were derived from 16 cases (fibrin clot group) and 15 cases (autograft-alone group). AM, anteromedial; PL, posterolateral; 3D-CT, 3-dimensional computed tomography.
With regard to the change from 1 week to 1 year postoperatively, the relative postoperative increase in CSA (BTE ratio) at the PL tunnel aperture was significantly less in the fibrin clot group than in the autograft-only group (P = .048) (Table 4), but there were no significant differences between groups in the AM tunnel aperture. At the 5-mm level in the bone tunnel, the BTE values calculated for the fibrin clot group were significantly smaller than those in the autograft-alone group in both the AM and PL tunnels (AM tunnel: P = .003; PL tunnel: P < .001). The difference between the 2 groups was more evident at the 10-mm level, showing highly significant differences between the groups (AM tunnel: P < .001; PL tunnel: P < .001). In terms of the difference in male-to-female ratio, there were no significant sex differences in demographic profiles (Table 5), while significant differences in the BTE ratio were observed, with females showing a larger postoperative increase in tunnel diameter compared with males (Table 6).
BTE Ratio (Relative Change in CSA Between 1 Week and 1 Year After ACLR) for the 2 Groups at the 3 Levels for Measurement a

Values are expressed as mean ± SD. A P value is presented for each comparative analysis. Bold P values indicate statical significance. ACLR, anterior cruciate ligament reconstruction; AM, anteromedial; BTE, bone tunnel enlargement; CSA, cross-sectional area; PL, posterolateral.
Demographic Information Separated by Sex a

Values are expressed as mean ± SD or n (%). BMI, body mass index.
BTE Ratio (Relative Change in CSA Between 1 Week and 1 Year After ACLR) Separated by Sex at the 3 Levels for Measurement a

Values are expressed as mean ± SD. A P value is presented for each comparative analysis. Bold P values indicate statical significance. ACLR, anterior cruciate ligament reconstruction; AM, anteromedial; BTE, bone tunnel enlargement; CSA, cross-sectional area; PL, posterolateral.
Discussion
The principal finding of this study is that placing a fibrin clot onto the graft in anatomic DB-ACLR was associated with a reduction in femoral BTE. The effect of fibrin clot application was more evident in the midportion of the bone tunnel rather than the intra-articular tunnel aperture. These findings correspond to the results of the study reported by Surer et al, 31 which showed that use of a fibrin clot in single-bundle allograft ACLR is effective in preventing BTE. They used plain radiographs to make radiological measurements, whereas we used reconstructed 3D-CT images to make our measurements, which allowed for a more rigorous evaluation than the study by Surer.
BTE has been reported as post-ACLR phenomenon. It is not clear whether postoperative BTE affects clinical outcomes, but the enlarged tunnel aperture associated with BTE can significantly complicate graft placement and fixation in revision ACLR. 35 In addition, this phenomenon may theoretically impair the healing between the graft and bone tunnel wall.19,30 To date, there are limited means available to achieve optimal healing at the graft-bone interface. The results of this study suggest that the application of a fibrin clot may prevent BTE.
BTE can be caused by various factors, mainly classified as biological and mechanical factors. 10 Considering the biological effects of fibrin clotting, one advantage is that it contains and delivers a variety of platelet-derived growth factors (PDGF, VEGF, TGF-β, etc) and cytokines. The gradual release of these beneficial factors has been shown to promote tissue healing and integration. 20 The thickness of the fibrin clot layer attached to the graft tendon is approximately 1 mm. However, this layer can effectively fill the graft-bone interface and serve as a passage for cell migration and growth factor delivery, potentially enhancing biological activity. 38 Hensler et al 9 confirmed the effectiveness of fibrin clot application in promoting graft healing in DB-ACLR in a caprine animal model by showing that adding fibrin clot to the graft induced faster tissue maturation. The use of a fibrin clot may have enabled quicker and more secure fixation in a shorter period of time, which may have contributed to the prevention of BTE.
From a mechanical perspective, fibrin clotting has a structural support capacity as a scaffold. It can be hypothesized that the application of the fibrin clot in this study may have inhibited the influx of synovial fluid into the graft-bone interface and physically filled the space between the graft and the bone tunnel wall, thereby reducing micromotion at the interface. Synovial fluid contains a variety of inflammatory cytokines, including TNF-α, IL-1β, IL-6, and nitric oxide, which may inhibit bone formation and increase osteoclast activity. 36 Hayward et al 8 reported the results of a clinical study showing increased release of proinflammatory cytokines that may inhibit graft-bone fusion in the early phase after ACLR. Masuda et al 17 reported the effectiveness of residual tissue preservation in reducing the femoral AM tunnel enlargement after anatomic DB-ACLR. They speculated that the preserved residual tissue covered the tunnel aperture and inhibited the influx of synovial fluid into the bone tunnel. Fibrin clots filling the space at the graft-bone interface may account for another mechanism to prevent BTE in this study.
With regard to the prevention of BTE through improved reconstructive techniques, some reports suggest that fixing the graft close to the tunnel can reduce the movement of the graft in the bone tunnel and eliminate the so-called windshield wiper effect that may contribute to BTE.26,28,32 When a free tendon graft is used in ACLR, the graft is usually fixed outside of the bone tunnel (suspension type fixation), resulting in significant graft-bone movement. In contrast, bone–patellar tendon–bone grafts can be fixed near the tunnel aperture if secured with interference screws (aperture fixation). However, it has been reported that BTE is more prominent in ACLR with hamstring tendon grafts than with bone–patellar tendon–bone grafts.3,5,14,34 The use of soft tissue interference screws in hamstring graft ACLR can reduce graft movement and inhibit synovial fluid influx, but there are concerns about initial BTE due to the space occupied by the screw, possible graft damage during screw insertion, and foreign body reaction to the screw material.7,23 Thus, the fibrin clot augmentation may alleviate these concerns and preserve the advantages over the use of an interference screw in prevention of BTE.
In this study, a significant inhibitory effect was observed in both bone tunnels, particularly at approximately 10 mm from the tunnel aperture, where the fibrin clot was expected to meet the graft-bone interface. There was no significant difference detected at the AM tunnel aperture, but a significant difference was observed at the PL tunnel aperture. The reason for this may be that the PL tunnel is inherently known to have a greater BTE than the AM tunnel.15,29 Therefore, the inhibitory effect may have been more evident in the PL tunnel due to its tendency for BTE.
Limitations
There are some limitations in this study. First, the physiological function of the fibrin clot and other factors associated with BTE were not evaluated. Second, clinical outcomes were not compared between groups, and the clinical efficacy of fibrin clot application could not be confirmed. Third, a postoperative rehabilitation protocol was not standardized across the study participants because of the inclusion of cases with concomitant meniscal surgery. Fourth, in this study, measurement of the bone tunnel dimension was conducted only for CSA; thus, the relationship with diameter and length of the bone tunnel could not be investigated. Fifth, there was a nearly significant difference in sex distribution (P = .052) with female predominance in the autograft-alone group, which may have influenced the extent of BTE due to sex differences in properties of the bone. This issue may have induced a bias in the data analysis. Comparison of the 2 groups matched for age and sex would have led to fairer analysis. Sixth, analysis at the bone tunnel aperture 1 year postoperatively may have lowered statistical power compared with other portions due to the exclusion of cases with tunnel coalition.
Conclusion
Adding the fibrin clot to the autograft in anatomic DB-ACLR reduced the BTE at 1 year after surgery. This effect was more evident in the PL tunnel and midportion of the AM tunnel.
Footnotes
Final revision submitted January 8, 2025; accepted February 11, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hyogo Medical University (4095).