
Abstract
Background:
Massive and irreparable rotator cuff tears (MIRCTs) pose unique challenges, and clinicians have explored a variety of surgical approaches to manage them. However, the optimal treatment strategies for MIRCT remain widely debated.
Purpose:
To investigate the biomechanical effects of 2 superior fulcrum reconstruction (SFR) techniques—using either 2 halved autologous peroneus longus tendons (SFR-H) in a sutured bridge configuration or a single entire autologous peroneus longus tendon (SFR-E) in an “X” configuration—on MIRCT in a static biomechanical setup. This study explores the biomechanical implications of these methods, aiming to address MIRCTs affecting the entire supraspinatus tendon and 50% of the infraspinatus tendon.
Study Design:
Controlled laboratory study.
Methods:
Eight cadaveric shoulders were subjected to biomechanical testing under 4 different conditions: Intact, MIRCT, SFR-E, and SFR-H. These tests were conducted at 0°, 30°, and 60° of glenohumeral abduction. The parameters measured included the rotational range of motion, superior translation of the humeral head, and subacromial contact pressure. Statistical analysis was performed using repeated-measures analysis of variance with Tukey post hoc tests, with significance set at P < .05.
Results:
The MIRCT condition led to a significant increase in the superior translation of the humeral head at all tested abduction angles (P < .05 for all). By contrast, SFR-E significantly reduced this translation across all angles (P < .05 for all), while SFR-H effectively reduced it at 0° and 30° (P < .05 for both). After MIRCT, subacromial contact pressure significantly increased at all tested abduction angles compared with the Intact state (P < .05 for all). Following SFR-E, significant pressure reductions were observed at 0° and 30° abduction angles (P < .05 for both). Similarly, SFR-H led to significant pressure reductions at all abduction angles (P < .05 for all).
Conclusion:
Compared with MIRCT, both SFR-H and SFR-E techniques significantly reduce superior translation of the humeral head and subacromial contact pressure, without limiting the range of motion of the humerus. In cadaveric biomechanical experiments, the use of peroneus longus tendon for SFR via bone tunnels has been proven to be a reliable method. Additionally, peroneus longus tendon is a viable source for autografting.
Clinical Relevance:
The results of this study are significant for patients suffering from MIRCTs, as they demonstrate that both surgical techniques may be used to treat these tears, potentially improving shoulder function and alleviating associated symptoms. The success of the cadaveric experiments lays the groundwork for further clinical trials.
Keywords
Massive irreparable rotator cuff tears (MIRCTs) present a significant challenge in treatment, primarily due to factors such as the large size of the tendon tear, tendon retraction, muscle atrophy, and fatty infiltration.2,17,21,42,53,54 These tears can lead to superior translation of the humeral head, reducing the acromiohumeral distance and resulting in shoulder dysfunction characterized by restricted abduction and elevation.10,11,15,17,20,66 This upward shift can increase subacromial pressure, potentially causing impingement.15,51 Therefore, preventing superior translation of the humeral head is essential for maintaining shoulder function.
Galatz et al 19 reported surgical failure rates of up to 94%, highlighting the ongoing uncertainty in determining the optimal treatment for MIRCTs. Current treatment options include partial cuff repair, 23 bridging techniques, 30 subacromial balloon spacer (SBS), 62 reverse total shoulder arthroplasty (RTSA), 64 and superior capsular reconstruction (SCR). 48 However, the retear rate after partial repair of MIRCTs is as high as 48.9%. 8 Bridging techniques 69 and SBS 22 show promising short-term outcomes, but their long-term effects remain uncertain, and RTSA 63 is generally considered a last resort.
The SCR technique is noted for its effectiveness in reducing pain and enhancing function, as well as yielding positive results on imaging, thus validating its clinical value.35,44,45 However, the technique's complexity calls for simpler, more reliable surgical methods to improve outcomes and minimize risks. Variability in results and the lack of long-term efficacy data highlight the necessity for refined surgical strategies.14,70 Issues such as graft deterioration over time and potential complications are concerning,16,27 spurring interest in alternative graft materials. The long head of the biceps 24 tendon (LHBT) and hamstring allograft 3 have been proposed for the treatment of MIRCT, showing promising results. However, these options are limited by poor tendon quality, limited availability, and smaller tendon-to-bone healing surface area.3,7,65
Biomechanical experiments 55 have demonstrated that applying a tension of 24 N effectively restores the original alignment between the humeral head and scapula. Therefore, as long as the graft’s size, width, and strength are appropriate, it can meet the biomechanical requirements. This principle applies to various tendon types, including dermal allografts, Achilles tendon allografts, or hamstring tendons. The peroneus longus tendon is increasingly recognized as a good choice for tendon grafts and is valued for its robustness and adequate width,31,38,71 suggesting potential for broader application in similar surgical procedures. Additionally, the peroneus longus tendon, with an ultimate tensile strength surpassing 4000 N, 61 is more than capable of withstanding such forces.
For some current treatment methods, tendon fixation to the bone surface using anchors raises concerns regarding the effectiveness of tendon-to-bone healing. Additionally, the use of numerous anchors and sutures not only increases surgical complexity and cost but also may have unpredictable long-term effects.13,26 Compared with surface contact with anchors, bone tunnels offer a greater contact area, which can enhance tendon-to-bone healing. Bone tunnel fixation methods have demonstrated favorable outcomes in both animal experiments and biomechanical studies.34,41,72 Additionally, the suture bridge technique provides superior biomechanical properties.57,58
In 2023, Li et al 37 developed an innovative method named superior fulcrum reconstruction (SFR) for MIRCT, utilizing the autologous peroneus longus tendon to perform bridge fixation via the intramedullary canal. This technique contrasts with traditional fixation methods by employing bone tunnels instead of anchors, potentially improving tendon-to-bone healing due to the increased contact area. Although the SFR method laid the groundwork for investigating its biomechanical properties, a comprehensive biomechanical evaluation of these constructs has yet to be performed. As an extension of the SFR technique, we propose an “X”-shaped repair using one entire peroneus longus tendon to further improve shoulder stability. This modification aims to enhance the biomechanical strength of the repair and provide better resistance against superior humeral head migration.
Our study aimed to compare the biomechanical outcomes in a static biomechanical investigation of 2 variations of SFR: bridge coverage using 2 halved autologous peroneus longus tendons (SFR-H) and X-type repair using 1 entire autologous peroneus longus tendon (SFR-E). The study focused on MIRCTs involving the entire supraspinatus tendon and the superior half of the infraspinatus. We hypothesized that both SFR-E and SFR-H would effectively reduce superior translation of the humeral head and subacromial contact pressure in the context of MIRCT, without compromising the humeral rotational range of motion (ROM).
Methods
This study, focusing on basic science research involving cadaveric specimens, did not require institutional review board approval.
Specimen Preparation and Mounting
The research utilized 8 cadaveric shoulder specimens (mean ± SD age, 62 ± 5.4 years [range, 56-71 years]; 5 male, 3 female). Before biomechanical testing, the specimens were thawed overnight. Each was inspected for rotator cuff integrity and found suitable for dissection. During preparation, only the capsule, coracoacromial ligament, and tendinous insertions of the following muscles to the humerus were preserved: supraspinatus, infraspinatus, subscapularis, teres minor, deltoid, latissimus dorsi, and pectoralis major. K.W. conducted all dissections to minimize variability.
For biomechanical testing, an intramedullary rod was inserted into the humerus to facilitate movement control in various directions (Figure 1). Rotation was monitored using a posture sensor (Weite Intelligent Technology Co., Ltd) attached to the rod. The humerus was securely mounted on a custom-designed scapular board at a 20° forward tilt using 3 screws.46,52 The muscles of the rotator cuff, along with the deltoid, latissimus dorsi, and pectoralis major, were affixed to the humerus using HEALIX Suture Anchors (DePuy Mitek) employing a Krackow suture technique. Suture distribution was as follows: 2 sutures each for the supraspinatus, subscapularis, pectoralis major, and latissimus dorsi; 1 each for the infraspinatus and teres minor; and 3 for the deltoid. Each suture was connected to a robust fishing line (Mermaid, Inc). Tension was consistently applied through an adjustable pulley system, with the direction of force vectors designed to simulate muscle loads and force couples that closely resembled those in human anatomy.

Photograph of the shoulder secured to the custom testing system.
Measurements
The study evaluated the biomechanical behavior of shoulder specimens at 3 different angles—0°, 30°, and 60°—to simulate a variety of daily activities. This involved setting the muscle load based on the physical characteristics of the shoulder specimen and previous muscle activity data. Each muscle was assigned a specific weight to establish distinct loading scenarios. Under balanced conditions, the following weights were used: supraspinatus and subscapularis at 10 N each, infraspinatus and teres minor at 5 N each, deltoid at 40 N, and both pectoralis major and latissimus dorsi at 20 N. By contrast, the unbalanced condition increased the deltoid’s load to 80 N while completely removing the weights from the pectoralis major and latissimus dorsi to investigate changes in the position of the humeral head.12,43 The study’s outcomes included measurements of the humeral rotation ROM, superior translation of the humeral head, and subacromial contact pressure. The ROM was assessed in a balanced condition by applying a torque of 2.2 N·m to determine the maximal internal and external rotation of the humerus at shoulder abduction angles of 0°, 30°, and 60°. The total ROM was calculated as the sum of these maximal internal and external rotation angles at each position. Assessments were conducted under 4 conditions: intact rotator cuff (Intact), simulated MIRCT, and after reconstruction with SFR-E and SFR-H. A posture sensor attached to the intramedullary rod (Sertuo) measured the internal and external rotation with an accuracy of 0.1°. At 60° abduction, external rotation was defined as 90° when the bicipital groove aligned with the anterolateral edge of the acromion. Superior humeral head translation was assessed by comparing the position of the humeral head relative to the acromion in unbalanced and balanced states, with the shoulder externally rotated by 30°. We used a calibrated monocular camera to record the humeral head and acromial position, determining the actual millimeter value corresponding to each pixel with an accuracy of 0.001 mm. By tracking the movement of target points marked on the humeral head and acromion, and multiplying the pixel displacement by the actual distance per pixel, we calculated the upward translation of the humeral head. Last, subacromial contact pressure was recorded under unbalanced conditions using a Tekscan pressure sensor (model 6900; Tekscan) with a saturation pressure of 1100 psi, positioned in the subacromial space during a 30° external rotation of the humerus.
Conditions
Each specimen underwent testing under 4 distinct conditions: (1) having an intact rotator cuff, (2) simulating MIRCT by excising the entire supraspinatus footprint and the superior half of the infraspinatus footprint, (3) SFR-E, and (4) SFR-H (Figure 2). Each test was replicated twice to ensure consistency and reliability of results. Utilizing the same specimen for all tests allowed for effective control of variables, clearly delineating the differential outcomes associated with each rotator cuff state.
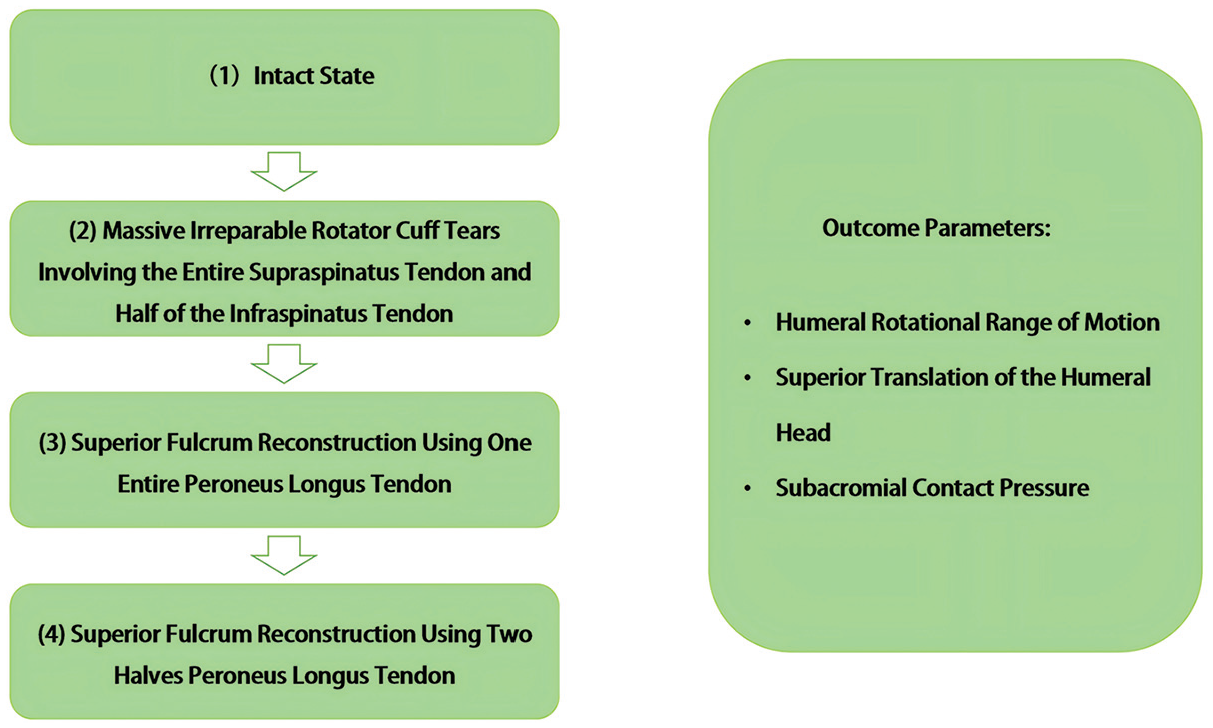
The 4 testing conditions utilized in the study. Each test was replicated twice.
Massive Irreparable Rotator Cuff Tear
Initial testing involved specimens with intact rotator cuffs. For MIRCT simulations, the greater tuberosity of the humerus was meticulously incised, methodically removing the superior capsule, supraspinatus, and half of the infraspinatus muscle. This was carried out by starting anteriorly and progressing posteriorly, moving from the lateral to the medial aspect, until the level of the glenoid was reached (Figure 3).

(A) Photograph of the specimen after defect creation, simulating a posterosuperior rotator cuff tear by excising the entire supraspinatus footprint and superior half of the infraspinatus footprint. (B) Photograph of the shoulders following superior fulcrum reconstruction using 1 entire peroneus longus tendon. (C) Photograph of the shoulders following superior fulcrum reconstruction using 2 halves of the peroneus longus tendon.
Superior Fulcrum Reconstruction
For condition 3, a section of the mid-to-distal peroneus longus tendon was harvested and trimmed, yielding a tendon with a diameter of approximately 4 to 5 mm and a length of approximately 13 to 15 cm. Each end of the tendon was secured using HEALIX Suture Anchors, ensuring optimal tension. A bone tunnel measuring 4.5 mm in diameter was drilled on the glenoid side, extending from the 10:30 position to the 1:30 position to accommodate the graft, which allowed for sufficient movement at both ends (Figure 4).

Schematic representation. (A) Bone tunnel on the glenoid side and the humeral side. (B) Superior fulcrum reconstruction using 1 entire peroneus longus tendon. (C)
On the humeral side, two 4.5 mm–diameter bone tunnels in the humeral head were prepared: one at the anterolateral edge and another 5 mm laterally from the posterolateral edge of the supraspinatus footprint. The graft’s ends were crossed over the humeral head, threaded through these tunnels, and then secured with Orthocord anchor sutures. During this process, the humerus was maintained at 30° of abduction and in neutral rotation, ensuring the graft was firmly anchored.
For condition 4, another processed peroneus longus tendon was used. The tendon was longitudinally divided, yielding 2 halves with 4 separate ends. Each half of the peroneus longus tendon had a diameter of approximately 2 to 3 mm. Each end uses anchor sutures for enhanced traction. These halves were then threaded through the previously prepared glenoid tunnel. The ends of one half toward a single humeral tunnel were routed, while the ends of the other half were directed to the opposite tunnel, creating a crisscross pattern across the humeral head. Finally, each end was pulled through its designated humeral tunnel and sutured securely, ensuring the graft was firmly positioned.
In conditions 3 and 4, the peroneus longus tendon was anchored at a 45° angle of shoulder abduction. 48
Statistical Analysis
Each experiment was repeated twice to gather data, and the mean of these replicates was calculated for each subject or sample point. First, the data were tested for normality using the D’Agostino-Pearson omnibus test to ensure that the assumptions for analysis of variance (ANOVA) were met. All groups passed the normality test (P > .05). Subsequently, a repeated-measures ANOVA was performed to assess differences among the 4 groups. Post hoc analysis was conducted using Tukey test to determine which specific group means were significantly different from each other. The threshold for statistical significance was set at P < .05. All statistical analyses were performed using GraphPad Prism software.
Results
Humeral Rotational ROM
The data revealed that the mean total rotational ROM—defined as the sum of internal and external rotation angles measured at shoulder abduction angles of 0°, 30°, and 60°—significantly increased after MIRCT (P < .001 for all). This may be attributed to the sudden loss of stability following the excision of the supraspinatus and superior infraspinatus tendons, resulting in increased joint laxity and, as a consequence, a greater ROM. Following the SFR-H and SFR-E procedures, the rotational ROM decreased across all abduction angles compared with the post-MIRCT condition. Significant differences were observed for SFR-H at 30° abduction (P = .01) and for both SFR-E (P = .01) and SFR-H (P = .02) at 60° abduction (Table 1).
Total Humeral Rotational Range of Motion for Each Condition and Abduction Angle a

Data are presented as mean ± SD. Dashes indicate not applicable.
Superior Humeral Head Translation
Following MIRCT, a marked increase in the superior translation of the humeral head was observed at glenohumeral abduction angles of 0°, 30°, and 60° (P < .001 for all). Compared with the Intact condition, the mean values also increased notably (Figure 5). Conversely, SFR-E significantly reduced superior translation at each abduction angle compared with MIRCT (P < .001 for all), while SFR-H showed notable reductions at 0° and 30° abduction (P < .001 for both). Although the superior translation was reduced with both SFR techniques compared with MIRCT, it remained greater than that of the Intact state. In certain conditions, particularly for SFR-H (with a 1- to 2-mm statistically significant improvement), the clinical relevance of this change remains uncertain.
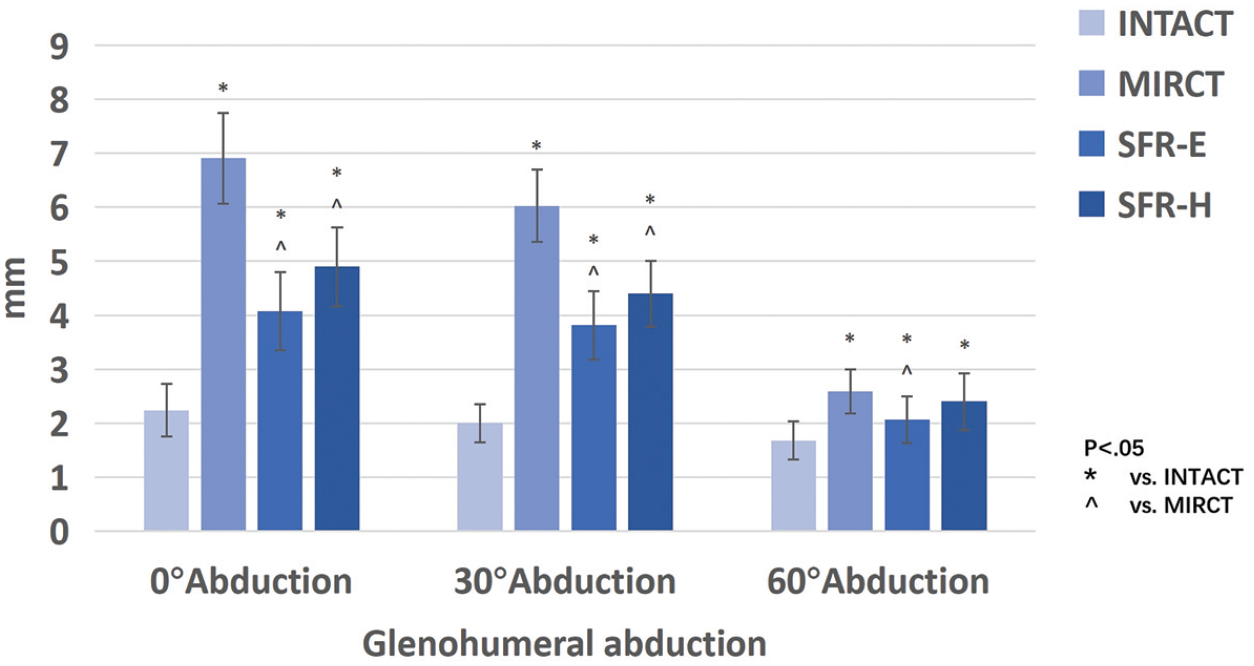
Superior humeral head translation (mm) was recorded for each testing condition and glenohumeral abduction angle. MIRCT, massive and irreparable rotator cuff tear; SFR-E, superior fulcrum reconstruction using 1 entire peroneus longus tendon; SFR-H, superior fulcrum reconstruction using 2 halves of the peroneus longus tendon.
Subacromial Contact Pressure
Post-MIRCT, significant increases were observed in subacromial contact pressure at 0°, 30°, and 60° of glenohumeral abduction compared with the Intact state (P < .005 for all) (Figure 6). Following the implementation of SFR-E, significant reductions in subacromial contact pressure were observed at 0° and 30° abduction angles (P < .001 for both), but not at 60° abduction (P = .07). Similarly, SFR-H led to significant pressure reductions at all abduction angles (0°, P < .001; 30°, P < .001; 60°, P = .02). However, the pressures did not revert to those observed in the Intact state, with SFR-E achieving a slightly more substantial reduction compared with SFR-H.

Subacromial contact pressure (MPa) was recorded for each testing condition and glenohumeral abduction angle. MIRCT, massive and irreparable rotator cuff tear; SFR-E, superior fulcrum reconstruction using 1 entire peroneus longus tendon; SFR-H, superior fulcrum reconstruction using 2 halves of the peroneus longus tendon.
Discussion
The most important finding of this study was that, in biomechanical testing, both SFR repair techniques significantly reduced the superior translation of the humeral head and subacromial contact pressure when compared with MIRCT, without significantly limiting the total ROM.
If the ROM after repair significantly improves to the Intact level, it could potentially lead to joint stiffness. However, in this study, although there was a reduction in ROM after SFR-H or SFR-E repair compared with MIRCTs, it did not reach the Intact level. Some shoulder scoring systems, such as those from the University of California, Los Angeles, and the Japanese Orthopaedic Association, consider a 17% reduction in elevation as an excellent postoperative outcome.18,29,48 In this study, the reduction in ROM after SFR-H or SFR-E was much lower than 17%, suggesting that it is unlikely to result in joint stiffness.
From a biomechanical perspective, MIRCT leads to increased humeral head translation due to the pull of the deltoid muscle.5,27,33 Both dynamic and static biomechanical studies have demonstrated that this condition significantly reduces the shoulder abduction angle compared with the Intact state.3,4,49,50 Increased translation of the humeral head can also impair its ability to rotate beneath the acromion; however, our study observed an increase in humeral rotational ROM. This could be due to the acute loss of stability when the supraspinatus and superior infraspinatus tendons are excised, leading to increased joint laxity and consequently greater ROM. However, after repair with both SFR techniques, ROM did not decrease significantly. Previous biomechanical studies25,43,47,65 have indicated that grafts fixed with anteroposterior side-to-side suturing may result in a significant reduction in ROM. The reason ROM did not significantly decrease after our repair might be due to the use of the bridgelike structure and X-shaped fixation methods, which did not involve anteroposterior side-to-side suturing.
The increase in superior translation of the humeral head following MIRCT was consistent with previous research (Table 2). Post-SFR, the techniques SFR-H and SFR-E significantly reduced humeral head translation across most angles, except for a nonsignificant reduction by SFR-H at 60° abduction. However, the decrease in translation after SFR-H or SFR-E repair was minimal. If only superior translation is considered, its clinical relevance may be questioned. However, it is worth noting that the subacromial pressures—except for the SFR-E at 60° abduction—were much lower than those observed in the MIRCT condition, almost reaching the Intact level. This suggests that the SFR technique may provide a spacing effect comparable with the Intact condition. Additionally, the graft fixation methods used in this study (bridgelike and X-shaped) restored force couples and the fulcrum, which could be expected to improve overall shoulder function and potentially increase ROM. Moreover, although this study did not measure the abduction angle before and after surgery, after performing the 2 SFR procedures, a reduction in humeral head superior translation was observed in most cases. We speculate that this could potentially improve glenohumeral joint abduction. Of course, this requires further validation in future studies.
Summary of Recent Biomechanical Studies for Treatment of Rotator Cuff Tear a

Data are presented as mean ± SD. AHDAT, acellular human dermal allograft tuberoplasty; BR, biceps rerouting; BRSS, biceps rerouting with side-to-side repair; DA, human dermal allograft; DA AP, human dermal allograft with anteroposterior suturing; DA P, human dermal allograft with posterior suturing; FL, fascia lata; IST, irreparable supraspinatus tear; LDT, latissimus dorsi tendon; LHBT, long head of the biceps tendon; LIRCT, large irreparable rotator cuff tear; MIRPS RCT, massively retracted irreparable posterosuperior rotator cuff tear; MRCT, massive rotator cuff tear; N/A, not available; PR, partial repair; PT, patellar tendon; PT-SCR, patellar tendon allograft–superior capsular reconstruction; SCR, superior capsular reconstruction; STT, semitendinosus tendon.
Statistically significant difference compared with Intact condition (P < .05).
Statistically significant difference compared with rotator cuff tear (P < .05).
When approaching MIRCT, RTSA is a more established treatment option. However, there is an increasing demand for non–joint replacement treatments, particularly in young and active patients without severe signs of osteoarthritis. Choosing the appropriate treatment method is a challenging issue. Kishan et al 32 reported good early and midterm outcomes for patients with MIRCT treated with subacromial balloon spacer interposition. However, the in vivo degradation of subacromial balloon spacers raises concerns. Wong et al 69 reported good early results with bridging allograft reconstruction for chronic, massive rotator cuff tears, but long-term outcomes remain unknown. The conventional use of fascia lata and human dermal grafts in SCR surgery raises concerns regarding potential donor-site morbidity, graft reactions, and the minimal required graft size. Additionally, this technique demands a high level of surgical skill and is prone to complications related to suture management, making it difficult to perform and challenging to promote.
An alternative approach involves using the LHBT to restore the shoulder joint’s force couple in the treatment of MIRCT. 40 This technique is relatively simple and has shown satisfactory clinical outcomes. However, it places high demands on the integrity and stability of the LHBT itself. A subset of MIRCT patients may have poor LHBT quality, and not all patients are suitable candidates for this procedure. Additionally, the LHBT can be a source of shoulder pain,6,67 which further complicates its use in this context.
When using hamstring allografts 3 for SCR, only 1 anchor is placed on the glenoid, resulting in a limited contact area between the hamstring allograft and the superior surface of the scapula. This raises concerns about tendon-to-bone healing potential. Furthermore, the single anchor must bear significant concentrated stress and load, which increases the risk of loosening or failure due to repetitive pull forces during shoulder movement.
In this study, graft placement utilized bone tunnels for fixation, a method proven to deliver favorable outcomes in both animal trials and biomechanical research.34,41,72 This technique improves the tendon-bone interface, establishing a stronger foundation for tendon integration with the bone. We utilized bone tunnels to create a repair similar to the suture bridge technique, which possesses superior biomechanical properties.57,58 Compared with techniques that require multiple anchors and sutures, using bone tunnels significantly saves surgical time and reduces complexity. Furthermore, in contrast to anchor fixation, which results in a very small tendon-to-bone contact area and higher stress, the use of bone tunnels in repair forms a structure similar to a tension band. This allows for early mobilization without the risk of anchor failure. Additionally, the tension band–like structure promotes further tendon-bone contact, aiding in postoperative rehabilitation.
Rotator cuff tears lead to the loss of force couple, which provides a stable fulcrum for shoulder movement. Such loss of stability causes the humeral head to migrate superiorly, resulting in shear forces and a significant loss of elevation and/or rotational function.1,59 These techniques aid in fulcrum reconstruction. Although, like SCR, this technique cannot provide active contraction force, the suture bridge–like fixation through bone tunnels offers good initial fixation strength and limits superior migration during shoulder movement. This helps control pain and optimize function. Thus, in combination with a preserved force couple, the described technique could restore this fulcrum, enhancing the ROM compared with traditional SCR methods.
Peroneus longus tendon is a robust and substantial option for anterior cruciate ligament reconstruction, consistently yielding favorable outcomes for patients.39,68 Positive postoperative results have been observed when utilizing this tendon for reconstruction. 60
These methods simplify the surgery, require less technical skill, and are cost-effective by using only anchor nail wire for autograft fixation, thereby reducing the need for additional materials.
Limitations
This study has some limitations. First, graft healing and remodeling were not considered in this biomechanical study, as only time-zero effects were examined. Second, the study utilized a static biomechanical model without accounting for dynamic muscle movements and therefore cannot fully simulate human shoulder kinematics. Additionally, our model was limited to specific types of rotator cuff tear and did not include other common variants. Moreover, the ROM was not measured using 3-dimensional cameras, which would have allowed for a more precise and dynamic evaluation. Furthermore, cadavers from older donors may not reflect the tissue quality of younger patients who are typical SFR candidates. Finally, the study did not compare this method to other repair techniques.
Conclusion
Compared with MIRCT, both SFR-H and SFR-E techniques significantly reduce superior translation of the humeral head and subacromial contact pressure, without limiting the ROM of the humerus. In cadaveric biomechanical experiments, the use of peroneus longus tendon for SFR via bone tunnels has been proven to be a reliable method. Additionally, peroneus longus tendon is a viable source for autografting.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all the individuals who have offered their invaluable support and assistance throughout the course of this study.
Final revision submitted November 20, 2024; accepted January 2, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Anhui Provincial Key Research and Development Plan (No. 202104j07020057). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.