
Abstract
Background:
Arthroscopic superior capsular reconstruction (SCR) has been introduced as a successful alternative to latissimus dorsi tendon transfer (LDTT) for irreparable posterosuperior rotator cuff tears.
Purpose:
To compare minimum 5-year clinical outcomes of SCR and LDTT for the treatment of irreparable posterosuperior rotator cuff tears in patients with minimal evidence of arthritis and intact or reparable subscapularis tears.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent SCR or LDTT and had undergone surgery ≥5 years earlier were included. The SCR technique used a dermal allograft customized to the defect. Surgical, demographic, and subjective data were collected prospectively and reviewed retrospectively. Patient-reported outcome (PRO) scores utilized were the American Shoulder and Elbow Surgeons (ASES), Single Assessment Numeric Evaluation (SANE), the short version of the Disabilities of the Arm, Shoulder and Hand score (QuickDASH), 12-Item Short Form Health Survey Physical Component Summary (SF-12 PCS), and patient satisfaction. Further surgical procedures were documented, and treatment that progressed to reverse total shoulder arthroplasty (RTSA) or revision rotator cuff surgery was considered a failure. Kaplan-Meier survivorship analysis was performed.
Results:
Thirty patients (n = 20 men; n = 10 women) with a mean follow-up of 6.3 years (range, 5-10.5 years) were included. A total of 13 patients underwent SCR and 17 patients underwent LDTT. The mean age of the SCR group was 56 years (range, 41.2-63.9 years), and the mean age of the LDTT group was 49 years (range, 34.7-57 years) (P = .006). One patient in the SCR group and 2 patients in the LDTT group progressed to RTSA. Two additional (11.8%) patients in the LDTT group had further surgery—1 had arthroscopic cuff repair and 1 had hardware removal with biopsies. The SCR group demonstrated significantly better ASES (94.1 ± 6.3 vs 72.3 ± 16.4; P = .001), SANE (85.6 ± 8 vs 48.7 ± 19.4; P = .001), QuickDASH (8.8 ± 8.7 vs 24.3 ± 16.5; P = .012), and SF-12 PCS (56.1 ± 2.3 vs 46.5 ± 6; P = .001) PROs at the final follow-up. There was no significant difference between groups in median satisfaction (SCR, 9; LDTT, 8 [P = .379]). At 5 years, survivorship rates were 91.7% and 81.3% for the SCR and LDTT groups, respectively (P = .421).
Conclusion:
At the final follow-up, SCR yielded superior PROs compared with LDTT for the treatment of massive, irreparable posterosuperior rotator cuff tears despite similar patient satisfaction and survivorship between procedures.
Keywords
Massive irreparable rotator cuff tears negatively affect activities of daily living and require treatment to reestablish adequate shoulder biomechanics and reduce pain. This represents a challenging clinical scenario, especially in younger patients. 2 DeOrio and Cofield 7 defined a massive rotator cuff tear as an injury that is >5 cm in diameter. Alternatively, it has also been defined as a rotator cuff tear involving ≥2 tendons. 10 Progression of rotator cuff deficiency may lead to superior humeral head migration and articulation with the coracoacromial arch, resulting in pain and loss of shoulder function. Patients can experience the loss of active shoulder function due to the disruption of the normal glenohumeral joint force-coupling mechanism that centralizes the humeral head during shoulder elevation. 6 While these disabling functional limitations, in addition to the potential for advancement to rotator cuff arthropathy, 3,40 result in the need for surgical intervention, a consensus does not exist on the optimal treatment strategy for massive irreparable rotator cuff tears. 37
Latissimus dorsi tendon transfer (LDTT) and superior capsular reconstruction (SCR) are 2 surgical options that have been developed for the treatment of irreparable rotator cuff tears. 15 These treatment options aim to delay or prevent the need for reverse total shoulder arthroplasty (RTSA). Gerber et al 9,13 originally described LDTT in 1988 as a technique for posterosuperior cuff insufficiency, in which it restores the kinematics of the shoulder by rebalancing the soft tissue tension of the shoulder. The biomechanical effects of LDTT provide a tenodesis effect to create humeral head depression, as well as provide increased active external rotation through the transfer vector with dynamic muscle activation. 17,31 This theoretically creates a fulcrum for the deltoid to provide active abduction of the shoulder. 9,11,13 Since its conception, long-term durable results have been demonstrated. 12
Arthroscopic SCR, originally described by Mihata et al, 26 is a newer technique that allows reestablishment of the superior stabilizing forces by employing a graft that spans between the greater tuberosity and the superior glenoid. This procedure aims to restore the superior glenohumeral joint capsule to reconstitute the glenohumeral force couple mechanism. 20 The graft functions as an interpositional static depressor to maintain centralization of the humeral head during range of motion, which allows force transmission between the remaining intact rotator cuff muscles. 28 In the United States, a dermal allograft is commonly used rather than fascia lata autograft as originally described to avoid donor-site morbidity. 23 Encouraging early results have been shown in the literature. 5,21,22,33
While LDTT has been established longer and therefore has a longer-term follow-up, SCR has recently grown in popularity, potentially because of the techniques’ less invasive approach, decreased donor-site morbidity, and complication profile. The purpose of this study was to compare minimum 5-year clinical outcomes of SCR and LDTT for the treatment of irreparable posterosuperior rotator cuff tears in patients with minimal evidence of arthritis and intact or reparable subscapularis tears. The hypothesis was that both treatments would produce similar, significant improvements in restoring shoulder function and subjective outcomes.
Methods
This study was an institutional review board–approved retrospective review of prospectively collected data. Patients were eligible for inclusion if they were aged 18 to 85 years at the time of follow-up and underwent SCR or LDTT for the treatment of an irreparable posterosuperior rotator cuff tear between October 2005 and January 2016 by the senior surgeon (P.J.M.). Indications for SCR and LDTT were identical and included patients who had retracted full-thickness tears of the supraspinatus and infraspinatus tendons that were technically irreparable, which was defined as the inability to restore the tendons to their anatomic footprints by any method when the arm was in full adduction. Additionally, all patients had to have an intact or reparable subscapularis tendon. The majority of LDTT procedures occurred before the development of SCR with dermal allograft, after which SCR was the predominant procedure performed. Patients were excluded if they had previously refused to participate in research, died in the follow-up period, lived outside the country without contact information, or had LDTT performed in conjunction with an arthroplasty procedure. Demographic (age, sex, prior surgical procedures, workers’ compensation cases, time from injury to surgery, preoperative arthropathy, and functional level) and surgical factors, along with complications and further surgical procedures, were analyzed between the 2 groups.
SCR Surgical Technique
The surgical technique for SCR has been described previously. 1,8,34 The irreparability of the torn supra- and infraspinatus tendons was confirmed during diagnostic arthroscopy. If the proximal long head of the biceps tendon was present, a subpectoral biceps tenodesis was performed with an interference screw. The greater tuberosity and the superior glenoid were prepared with a motorized rasp. An arthroscopic measuring device was then used to determine the necessary graft size in the anteroposterior and mediolateral directions. The necessary graft dimensions were measured using standard techniques, and a 3 mm–thick human acellular dermal allograft was sized accordingly. It incorporated 7 to 8 mm of coverage medially over the superior glenoid and 15 to 18 mm laterally over the greater tuberosity to cover the anatomic footprint. An initial superior glenoid anchor was inserted at the 12-o’clock position and the graft was shuttled into the joint into the appropriate position and secured. Glenoid fixation was then completed with 2 additional anchors, which were placed at the 10-o’clock and 2-o’clock positions. Next, lateral fixation of the graft was performed with the humerus in 30° to 40° of abduction with a crossing knotless, tape-bridging transosseous equivalent reconstruction using 4 to 6 anchors. The graft was also secured laterally to the infraspinatus or teres minor and subscapularis using margin convergence–to–bone sutures from the posterior and anterior medial row anchors, respectively. The rotator interval was not closed medially. Finally, margin convergence was performed in a side-to-side fashion between the graft and the remaining infraspinatus.
LDTT Surgical Techniques
The surgical technique for LDTT has been previously described. 36 The irreparability of the torn supra- and infraspinatus tendons was confirmed during diagnostic arthroscopy. A curvilinear incision was made posteriorly and laterally after the lateral border of the latissimus dorsi muscle belly, and the tendon was harvested at the humeral insertion site after adequate exposure. The neurovascular pedicle of the latissimus dorsi muscle belly was identified and protected. Achilles tendon allograft augmentation of the latissimus dorsi was performed if the tendon’s natural length was too short to provide an optimal length-tension relationship by reaching the anterior aspect of the greater tuberosity. The intraoperatively measured gap between the latissimus dorsi tendon and greater tuberosity, which was commonly 10 to 15 cm, largely determined the length of the graft to achieve the ideal length-tension relationship. A soft tissue tunnel anteroinferior to the deltoid and posterior to the teres minor was created and dilated. The arm was then placed into 30° of abduction, 30° of forward flexion, and 30° of external rotation. The augmented latissimus dorsi tendon was then shuttled through the soft tissue tunnel and placed on the lateral aspect of the greater tuberosity to create an external rotation moment arm, thereby restoring the function of the posterosuperior rotator cuff. Finally, 6 to 8 anchors were used to fix the allograft in a linked double-row construct.
Postoperative Rehabilitation
Patients who underwent SCR were strictly immobilized in an abduction pillow for 6 weeks. Patients then began full passive and active-assisted range of motion as tolerated. At 10 to 12 weeks postoperatively, a full active range of motion and the beginning of strengthening were allowed. Return to full activity and recreational activities without restriction were allowed 3 months postoperatively. 35
Patients who underwent LDTT were also immobilized in an abduction pillow for 6 weeks. Patients then began full passive and active-assisted range of motion as tolerated. A biofeedback program was initiated, teaching the patient how to activate the latissimus dorsi muscle for forward flexion and external shoulder rotation. The muscular strength phase was generally introduced at 10 to 12 weeks postoperatively. After 3 months, the focus turned to building strength and progressing endurance with daily activities as well as work and recreational activities.
Patient-Reported Outcome Assessments
Patient-reported outcome (PRO) scores were collected and compared preoperatively and at the final follow-up. If patients did not have minimum 5-year outcomes data in our institutional database, they were contacted regarding elective participation in the study. Patients who agreed to participate in the study were sent questionnaires via email after giving their informed consent. No questionnaires were administered via telephone. PROs collected included the American Shoulder and Elbow Surgeons (ASES) (100 = best score), Single Assessment Numeric Evaluation (SANE) (100 = best score), short version of the Disabilities of the Arm, Shoulder and Hand (QuickDASH) (0 = best score), and 12-Item Short Form Health Survey Physical Component Summary (SF-12 PCS) (higher scores correspond with better health) scores. Patients were also asked specific questions regarding pain and functional use of their arm preoperatively and postoperatively. Patient satisfaction with surgical outcomes using a scale of 1 to 10—with 1 representing a very unsatisfied response and 10 a very satisfied response—was collected at the final follow-up.
Statistical Analysis
Univariate analyses were performed using an independent t test for normally distributed variables. Mann-Whitney or Fisher exact tests were performed for data that were not normally distributed or for bivariate comparisons. The Wilcoxon signed-rank test was used to detect differences between pre- and postoperative variables. The chi-square test was used for bivariate data. Kaplan-Meier survivorship analysis was performed, with failure defined as progression to RTSA or revision rotator cuff surgery. Statistical analyses were performed using SPSS Version 11.0 (SPSS). The threshold for significance was set at P < .05.
Results
A total of 30 patients—13 patients underwent SCR reconstruction and 17 patients underwent LDTT for irreparable posterosuperior rotator cuff tears between October 2005 and January 2016 by the senior surgeon (P.J.M.)—were identified and included in the analysis. The study included 20 men and 10 women. Patient characteristics for each group are demonstrated in Table 1. The age at surgery was significantly higher in the SCR group compared with the LDTT group (56 vs 49 years; P = .006). The LDTT group had a significantly higher proportion of workers’ compensation cases (58.8% vs 7.7%; P = .007) and a higher incidence of prior rotator cuff repairs (100% vs 69.2%; P = .026) compared with the SCR group. Preoperative Hamada grade was higher in the LDTT group (median = 2; interquartile range, 1-3) compared with the SCR group (median = 1; first quartile = 1; third quartile = 3) (P = .032). No significant differences were found in preoperative external rotation (P = .108) or forward elevation (P = .225) between the 2 groups. There were no partial- or full-thickness subscapularis tears that required repair in either the SCR or the LDTT groups. There were no differences in preoperative PROs between the SCR and LDTT groups.
Characteristics of the SCR and LDTT Groups (N = 24 Shoulders) a
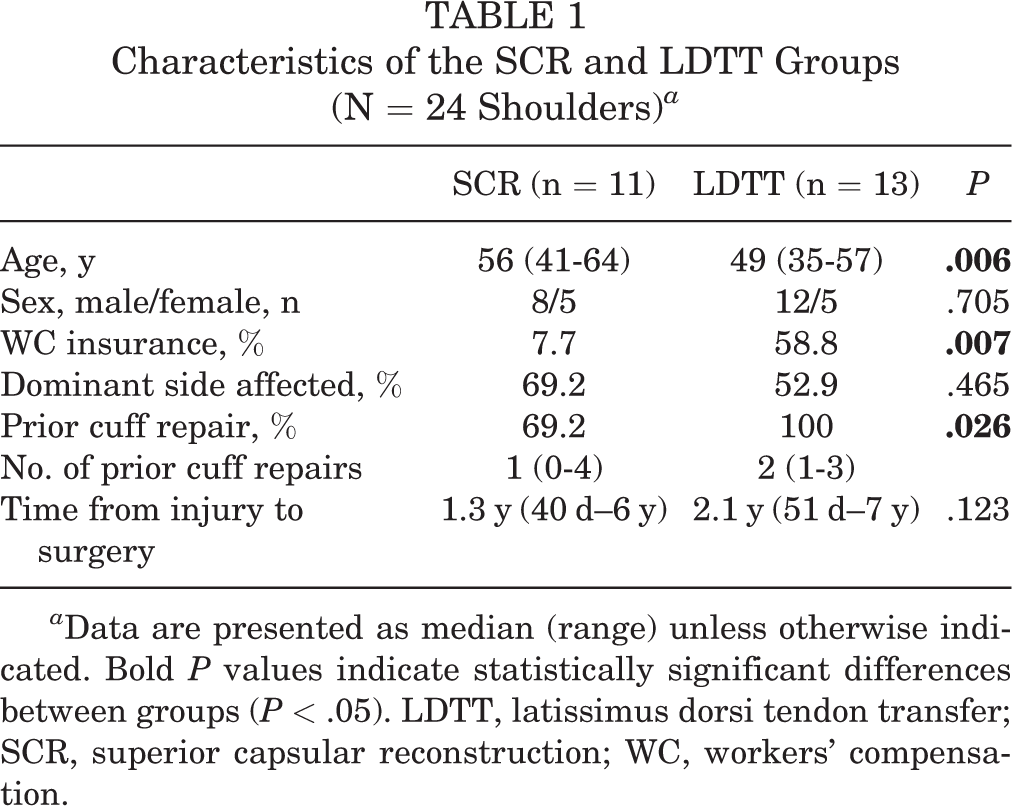
a Data are presented as median (range) unless otherwise indicated. Bold P values indicate statistically significant differences between groups (P < .05). LDTT, latissimus dorsi tendon transfer; SCR, superior capsular reconstruction; WC, workers’ compensation.
One patient treated with SCR (7.7%) progressed to RTSA at 2.5 years due to structural failure of the graft, while 2 patients treated with LDTT (11.8%) progressed to RTSA at 1 and 1.5 years due to persistent pain and functional limitations, respectively. Surgical failure occurred in 1 patient (7.7%) in the SCR group at 2 months postoperatively due to a graft tear on magnetic resonance imaging and because the patient was unsatisfied with his surgical outcomes and refused to complete further shoulder questionnaires. Two additional patients (11.8%) in the LDTT group had further surgery at approximately 1 year after surgery—1 patient had revision arthroscopic rotator cuff repair and 1 patient had hardware removal with biopsies and cultures (all negative) to rule out infection as the cause of persistent pain.
In the remaining patients, a final follow-up was obtained in 22 of 24 patients (91.7%; 11/11 SCR and 11/13 LDTT) at a mean follow-up of 6.3 years (range, 5-10.5 years) (Figure 1). The SCR group demonstrated significant improvements in all PROs at the final follow-up compared with preoperative scores, while the LDTT group only demonstrated significant improvements in the ASES, ASES function, and SF-12 PCS scores (Table 2). The LDTT cohort did experience modest preoperative to postoperative improvements in ASES pain, SANE, and QuickDASH scores, but did not reach statistical significance (Table 2). The LDTT cohort did not maintain significant improvement when asked specific questions about shoulder pain and function (Table 3). At a minimum 5-year follow-up, the SCR group had significantly better PROs compared with the LDTT group (Table 4). There were no statistically significant differences in final median satisfaction with surgical outcomes between each group (SCR, 9; LDTT, 8 [P = .379]).
At 5 years, Kaplan-Meier survivorship analysis demonstrated a survivorship rate of 91.7% for the SCR group and 81.3% for the LDTT group (P = .421), respectively. A decreasing trend in survivorship was observed by extending the LDTT group to a 6-year follow-up that resulted in 73% survivorship. At the final follow-up, 5 of all 17 (29%) patients who underwent LDTT reported either being unable to work or having filed for long-term disability because of their shoulder.

Flow diagram. LDTT, latissimus dorsi tendon transfer; MRI, magnetic resonance imaging; RCR, rotator cuff repair; RCT, rotator cuff tear; RTSA, reverse total shoulder arthroplasty; SCR, superior capsular reconstruction.
Pre- to Postoperative Comparison of PROs for SCR and LDTT a

a Data are presented as mean ± SD. Bold P values indicate statistically significant differences between pre- and postoperative values (P < .05). ASES, American Shoulder and Elbow Surgeons; LDTT, latissimus dorsi tendon transfer; Postop, postoperative; Preop, preoperative; PRO, patient-reported outcome; QuickDASH, short version of the Disabilities of the Arm, Shoulder and Hand; SANE, Single Assessment Numeric Evaluation; SCR, superior capsular reconstruction; SF-12 PCS, 12-Item Short Form Health Survey Physical Component Summary.
Pre- to Postoperative Comparison of Specific Shoulder Pain and Function Questions for SCR and LDTT a

a Bold P values indicate statistically significant differences between pre- and postoperative values (P < .05). ADL, activities of daily living; LDTT, latissimus dorsi tendon transfer; Postop, postoperative; Preop, preoperative; SCR, superior capsular reconstruction.
b Significant improvements pre- to postoperatively—none = 0; mild = 1; moderate = 2; severe = 3.
c Unable = 0; very difficult = 1; somewhat difficult = 2; normal = 3.
d To waist = 0; chest = 1; neck = 2; head = 3; overhead = 4.
e No difficulty = 1; slight difficulty = 2; moderate difficulty = 3; severe difficulty = 4; unable = 5.
Comparison of SCR Versus LDTT PROs at Minimum 5 Years a

a Data are presented as mean ± SD unless otherwise indicated. Bold P values indicate statistically significant differences between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; LDTT, latissimus dorsi tendon transfer; PRO, patient-reported outcome; QuickDASH, short version of the Disabilities of the Arm, Shoulder and Hand; SANE, Single Assessment Numeric Evaluation; SCR, superior capsular reconstruction; SF-12 PCS, 12-Item Short Form Health Survey Physical Component Summary.
Discussion
The principal findings of the present study were that SCR produced significantly improved PROs for the treatment of irreparable posterosuperior rotator cuff tears at a minimum follow-up of 5 years, while LDTT produced only modest increases in most PROs and continued functional limitations. Further, patients treated with SCR reported superior outcomes at the final follow-up compared with those treated with LDTT. Both patient populations experienced similar rates of progression to RTSA, and there were no significant differences in final satisfaction with surgical outcomes between groups. While there are several studies in the current literature documenting outcomes of SCR or LDTT, this study provides comparative outcomes of prospectively collected data with a minimum follow-up of 5 years.
LDTT is a well-established surgical procedure for irreparable posterosuperior rotator cuff tears, providing a vascularized tendon transfer to act as a humeral head depressor and dynamically improve function by restoring external rotation. In 1988, Gerber et al 13 presented good clinical results with improvement in age-adapted Constant scores (CS) in 16 patients with a 33-month follow-up. More recently described techniques for LDTT include arthroscopic assistance (aLDTT), as utilized in some of the patients in the present study, which potentially minimizes the trauma to the overlying deltoid muscle. 14,16,19,29,38 Waltenspul et al 39 recently reported midterm (mean follow-up, 3.5 years) outcomes on 27 shoulders after aLDTT, demonstrating significant improvements in Subjective Shoulder Value, CS, pain scores, and functional outcomes. The mean CS at the final follow-up was 67, which is comparable with the LDTT cohort’s total ASES score of 72.3 in the present study. The authors also reported that 13% of LDTTs failed as patients progressed to an RTSA, which is again similar to the failure rate of 11.8% reported in the present study. Despite these promising results, unsatisfactory outcomes have been demonstrated when LDTT is performed in the revision setting. 24,30 In a retrospective analysis of 22 patients undergoing LDTT in the setting of prior failed rotator cuff repair, Muench et al 30 reported a postoperative ASES score of 55.8 and a clinical failure rate of 41% at a mean follow-up of 3.4 years. Importantly, all LDTT procedures in our series were performed in the revision setting and 59% were workers’ compensation cases. Further, while the LDTT cohort in our study had a lower failure rate and a higher collective ASES score after a mean follow-up of 7.0 years, the clinical outcomes of LDTT were again demonstrated to be unsatisfactory when performed in patients with prior failed rotator cuff repairs.
Outcomes of LDTT augmented with the Achilles tendon allograft were previously reported at a minimum of 2 years by Pogorzelski et al 36 and were comparable with those of the patients who had undergone LDTT in the present series. Several factors may have contributed to subdued improvement in PROs in our series. In the LDTT group, 59% of patients had a workers’ compensation claim and all patients had ≥1 prior rotator cuff repair, both of which are known risk factors for inferior outcomes. 16,24,39 Additionally, the mean follow-up was 7.0 years in the present study, potentially allowing for outcome deterioration as demonstrated by Gerber et al 12 in their 10-year LDTT outcome study.
SCR is a more recently developed technique initially described by Ishihara et al 18 Mihata et al 27,28 in an attempt to restore the biomechanical role of the superior capsule to improve shoulder function in patients with irreparable massive rotator cuff tears. Reconstruction of the superior capsule demonstrated restoration of shoulder biomechanical stability, providing a functional fulcrum for range of motion, and resulted in the decreased superior translation of the humeral head, decreased subacromial contact pressures, and decreased glenohumeral joint forces. 20,28 Previous short-term SCR outcomes utilizing an acellular dermal allograft published by Lacheta et al 21,22 and Ciccotti et al 4 illustrated excellent outcomes with significant improvements in ASES, SANE, and QuickDASH scores while maintaining a 100% return to sports rate. Mihata et al 25 recently published 5-year clinical outcomes after SCR and found continued significant improvements in ASES (63.3 points) and Japanese Orthopaedic Association (39.9 points) scores, active elevation (66°), and acromiohumeral distance (4.7 mm) at 5 years. Despite reporting a greater change in the ASES score, the total ASES score (93.2) at the final follow-up is comparable with the score of 94.1 seen in the present study. The rates of return to physical work and return to sports were 92% and 100%, respectively. While patients without graft tears showed no progression of rotator cuff arthropathy, the 3 patients with graft tears demonstrated severe glenohumeral arthritis at the final follow-up.
Öztürk et al 32 recently completed a randomized prospective trial of SCR versus LDTT with a minimum 2-year follow-up for massive irreparable rotator cuff tears in a group of 42 patients. Both groups displayed significantly improved results in the ASES, Western Ontario Rotator Cuff, CS, and visual analog scale scores at the final follow-up (P < .001). The SCR group yielded significantly higher final ASES (81.7 vs 72.1; P = .007) and CS (81.1 vs 73.9; P = .008) scores compared with patients treated with LDTT. 32 This partially aligns with the present study’s findings of superior ASES (94.1 vs 72.3; P = .001), SANE (85.6 vs 48.7; P = .001), QuickDASH (8.8 vs 24.3; P = .012), and SF-12 PCS (56.1 vs 46.5; P = .001) scores in the SCR group compared with patients treated with LDTT. However, while ASES, SANE, and QuickDASH scores in the LDTT group improved in the present study, the only shoulder-specific outcomes to significantly improve were the ASES and ASES function scores.
Interestingly, the present study illustrated that despite significantly higher PROs within the SCR group, there was no significant difference in median patient satisfaction (SCR, 9; LDTT, 8; P = .379). Additionally, Kaplan-Meier analysis showed improved survivorship rates of 91.7% for the SCR group versus 81.3% for the LDTT group at 5 years (P = .421). However, despite promising patient satisfaction rates and reasonable survivorship in the LDTT cohort, nearly 30% of patients reported being unable to return to work. This finding, in conjunction with the superior PROs in the SCR cohort, may indicate that the SCR is a superior treatment option for young active patients with massive irreparable rotator cuff tears, as the SCR more effectively improves pain and function while reducing disability. Further, the sustained improvement through a minimum 5-year follow-up, as demonstrated by the present study and the study by Mihata et al, 25 supports the use of SCR as a means of delaying progression to RTSA in a young, active population.
Limitations
This study had several limitations. There was a limited number of patients available for both the SCR and the LDTT groups, which decreases the robustness of the statistical analysis. However, this also reflects one of the strengths of this study, as the opportunity to evaluate the comparative midterm outcomes between these 2 groups from a single surgeon is uncommon. In concordance, as the outcomes of this study represent the results of a single high-volume shoulder surgeon, they may not be generalizable. Furthermore, as this was not a randomized series, there were demographic differences between the SCR and LDTT groups, with the LDTT group’s being younger, having a higher proportion of workers’ compensation cases, and having a higher incidence of prior rotator cuff surgeries as previously noted. This could introduce bias when comparing groups and would be important to consider when preoperatively counseling patients on appropriate treatment recommendations.
Conclusion
At the final follow-up, SCR yielded superior PROs compared with LDTT for the treatment of massive, irreparable posterosuperior rotator cuff tears despite similar patient satisfaction and survivorship between procedures.
Footnotes
Final revision submitted January 24, 2023; accepted February 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was partially funded directly by a private grant from Paul and Lee Schmidt. This research was supported by the Steadman Philippon Research Institute (SPRI), which is a 501(c)(3) nonprofit institution supported financially by private donations and corporate support. The SPRI exercises special care to identify any financial interests or relationships related to the research conducted. During the past calendar year, the SPRI has received grant funding or in-kind donations from Arthrex, DJO, MLB, Ossur, Siemens, Smith & Nephew, and XTRE. S.L. has received grant support from Arthrex and education payments from Arthrex and Smith & Nephew. P.J.M. has received research support from Arthrex, Ossur, Siemens, and Smith & Nephew; consulting fees from Arthrex; and royalties from Arthrex, MedBridge, and Springer; and has stock/stock options in VuMedi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Vail Health Hospital (ref No. 2021-006).