
Abstract
Background:
In recurrent patellar instability, medial patellofemoral ligament reconstruction (MPFLR), with or without concomitant bony procedures, has become the treatment of choice to stabilize the patellofemoral joint. In the setting of recurrent patellar instability after primary MPFLR, revision MPFLR can be considered. Numerous potential risk factors for failure of isolated primary MPFLR have been evaluated with mixed findings.
Purpose/Hypothesis:
The purpose of this study was to compare anatomic and demographic patient characteristics between patients undergoing primary and revision MPFLR. It was hypothesized that patients undergoing revision MPFLR will demonstrate a higher prevalence of anatomic risk factors and J-tracking and will demonstrate more articular cartilage damage than patients undergoing primary MPFLR.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective chart review was performed to identify patients who underwent primary MPFLR between 2009 and 2021 and revision MPFLR between 2009 and 2023. Patients were categorized into 2 groups based on whether they underwent primary or revision MPFLR. Demographic (age, sex, and body mass index [BMI]), anatomic characteristics (patellar height, trochlear morphology, and tibial tubercle–trochlear groove distance), physical examination findings (presence or absence of a J-sign), and intraoperative findings (articular cartilage damage of the patellofemoral joint) were compared between these groups.
Results:
A total of 164 patients who underwent MPFLR within this period, including 26 revision and 138 primary procedures, were evaluated. No difference in patient age, sex, or any measure of patellar height was noted between the 2 groups. The revision MPFLR group was noted to have a higher BMI (29.9 kg/m2 vs 27.2 kg/m2; P = .036), a higher mean sulcus angle (145° vs 140°; P = .007), more frequent presence of a crossing sign (77% versus 18%; P < .001), and were more likely to have a J-sign (42% vs 22%; P = .048) than the primary MPFLR group. Intraoperatively, the revision MPFLR group had a higher prevalence of articular cartilage damage (81% versus 37%; P < .0001) than the primary MPFLR group.
Conclusion:
Patients undergoing revision MPFLR had more prior patellar dislocations, higher BMI, and more trochlear dysplasia (increased sulcus angle and more frequent crossing sign) than those undergoing primary MPFLR. The revision group was also more likely to have a J-sign on clinical examination and patellar articular cartilage damage at the time of arthroscopy.
Keywords
Recurrent patellar instability can lead to an increase in disability and reduction in mobility and activity levels for patients.5,19,24 These injuries most commonly occur in younger, more active patient populations. The initial treatment for most first-time traumatic dislocations without osteochondral injury remains nonoperative management with bracing, physical therapy, and strength training. 17 However, in the case of recurrent lateral patellar instability, surgical treatment is recommended. The medial patellofemoral ligament (MPFL) is nonfunctional in the setting of recurrent patellar instability, and its reconstruction (MPFLR) has become the standard surgical treatment of patellar instability with recurrence risk noted to be <5%. 26
Those patients who experience recurrent patellar instability after primary MPFLR are commonly treated with revision MPFLR, often in conjunction with other procedures. Outcomes of revision MPFLR have been variable, and much research has focused on the optimization of the primary surgery. 23 Many studies have utilized a cohort methodology to evaluate factors that may contribute to the risk of failure and the need for revision surgery. These factors have included patient demographics (age, sex, and body mass index [BMI]),12,28 anatomic factors (patellar height, trochlear morphology, and the tibial tubercle–trochlear groove [TT-TG] distance) 21 physical examination findings (the presence of a J-sign),25,33 and intraoperative findings (patellofemoral articular cartilage status). 10
Previous work has shown that anatomic factors including patella alta, trochlear dysplasia, presence of a preoperative J-sign, and femoral tunnel placement are associated with failure of MPFLR.15,18,25,33 Very few studies in general have evaluated risk factors for failure of MPFLRs that were performed in conjunction with bony procedures. One such study did show that younger age and trochlear dysplasia were associated with increased risk of failure of combined MPFLR and tibial tubercle osteotomy. 29
Most of the studies that evaluate the effect of anatomic and other factors on outcomes of MFPLR utilize patient-reported outcome (PRO) scores as outcome measures. In a review by Cregar et al, 7 8 studies evaluated the effects of anatomic and social factors on postoperative PROs. These studies found that trochlear dysplasia, patellar tilt, and femoral tunnel placement were the factors most frequently identified as affecting postoperative outcomes.8,12-15,20,30,31 However, these studies did not correlate any of the included factors with failure risk of MPFLR.
Another potential methodology for identifying risk factors for failure of primary MPFLR is to compare characteristics of patients undergoing primary MPFLR with those undergoing revision MPFLR. In this study, we hypothesize that patients undergoing revision MPFLR will demonstrate a higher prevalence of anatomic risk factors and higher prevalence of J-tracking and will demonstrate more articular cartilage damage than patients undergoing primary MPFLR. We aim to identify whether these factors, as well as any additional factors, are associated with the need for revision MPFLR.
Methods
Study Design and Inclusion Criteria
The presented study is an institutional review board–approved cross-sectional study of patients undergoing MPFLR surgery by 1 of 4 sports medicine fellowship–trained orthopaedic surgeons from a single academic institution (including C.C.K., D.F.C., R.A.M.). All patients aged >13 years who underwent primary MPFLR between January 1, 2009, and December 31, 2021, and all patients who underwent revision MPFLR between January 1, 2009, and May 31, 2023, were eligible for inclusion in the study. A longer data collection period was utilized for patients undergoing revision surgery given the decreased frequency of this procedure. Patients were included in the study group if preoperative plain films and magnetic resonance imaging (MRI) were available in the medical records system. Procedures were classified as primary MPFLR if they were the first MPFLR performed in the index knee. Procedures were classified as revision MPFLR if the patient had undergone prior MPFLR in the index knee. Patients were included in both groups regardless of whether the MPFLR was performed in isolation or in conjunction with other procedures.
Data Collection
Patient demographics including age, sex, BMI, number of dislocations, and age at first dislocation were collected. Physical examination data, including the presence of a J-sign, were collected from medical records. Intraoperative findings, including the presence of patellofemoral articular cartilage damage and the performance of concomitant procedures, were obtained from operative reports. All surgical data for the revision group are from the revision surgery, and no primary surgical data are included for this cohort. Articular cartilage damage at the time of diagnostic arthroscopy was quantified using the International Cartilage Regeneration & Joint Preservation Society (ICRS) grading system. 4 Anatomic metrics were obtained from preoperative MRI and radiographs, including the Caton Deschamps index, 6 TT-TG distance, 27 trochlear sulcus angle, 1 crossing sign, supratrochlear spur sign, degree of patellofemoral compartment osteoarthritis (Iwano classification), 16 patellar tilt, and patellotrochlear index. 3
Statistical Analysis
Patient demographics and anatomic characteristics were compared between the 2 groups using Fisher exact tests for categorical variables and t tests or Mann-Whitney U tests for continuous variables depending on normality. All statistical analysis was performed using IBM SPSS software (Version 29.0.1.0) and Microsoft Excel.
Results
A total of 223 patients were identified who underwent MPFLR during the study period, including 30 revision patients and 193 primary MPFL patients. Of these, 164 had both preoperative radiographs and MRI that could be viewed, including 26 revision patients (87%) and 138 primary MPFL patients (72%), who comprised the final study group (Table 1).
Demographics a

BMI, body mass index. Bold values indicate p < 0.05.
Demographics
The 164 patients in the cohort included 62 male and 102 female patients with a mean age of 24.2 years and a mean BMI of 27.7 kg/m2. The mean age at initial dislocation was 17 years, and patients had suffered a median of 6.3 patellar dislocations before the index procedure. The median number of prior patellar dislocations was lower in the primary MPFLR group (2 dislocations) than in the revision MPFLR group (7 dislocations) (P = .0007). The revision MPFLR group also demonstrated elevated mean BMI (29.9 kg/m2) compared with the primary group (27.2 kg/m2) (P = .036), but no differences in age at surgery, sex, or age at initial patellar dislocation were noted between the 2 groups (Table 1).
Physical Examination and Intraoperative Data
Overall, a J-sign was noted in 42 patients (26%) and articular cartilage damage of ICRS grade ≥2 was noted in 72 patients (44%). There was a higher prevalence of a J-sign on preoperative examination in the revision group (42%) than in the primary group (22%) (P = .048). Articular cartilage damage of grade ≥2 was noted in more patients in the revision group (81%) than in the primary group (37%) (P < .0001) (Table 2).
Physical Examination and Intraoperative Findings a
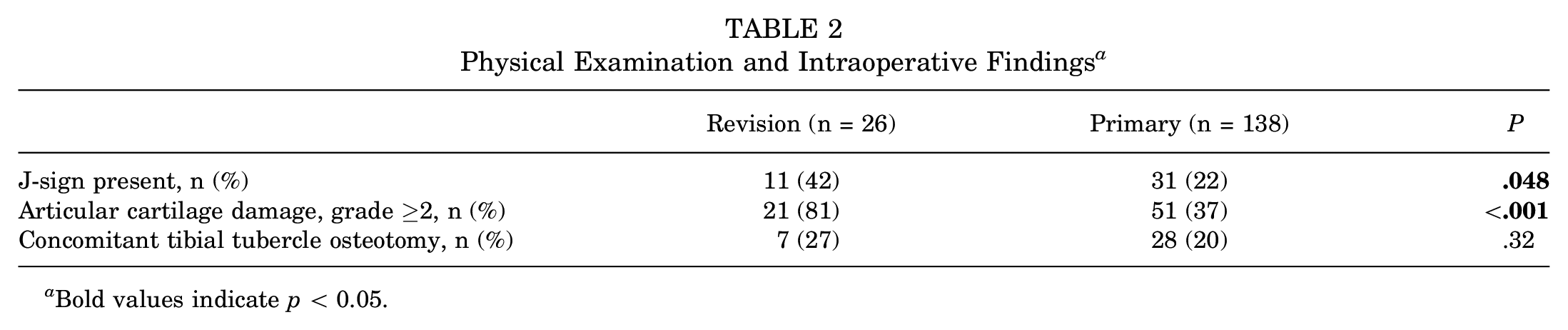
Bold values indicate p < 0.05.
Anatomic Data
Overall, the mean Caton Deschamps index was 1.14, and the mean patellotrochlear index was 0.48. The mean TT-TG distance was 17.4 mm. A supratrochlear spur was noted in 9.8% of patients and a crossing sign was present in 27% of patients. The mean sulcus angle was 141°. The revision group was noted to have a higher prevalence of trochlear dysplasia, including more frequent presence of a crossing sign (77% versus 18%; P < .0001) and a higher sulcus angle (145° vs 140°; P = .008). There were no significant differences between groups in any measure of patellar height (Table 3).
Imaging Findings a

Data are presented as mean ± SD or n (%).CD, Caton Deschamps; TT-TG, tibial tubercle–trochlear groove. Bold values indicate p < 0.05.
Discussion
The most important findings of this study are that elevated BMI, trochlear dysplasia (as defined by higher trochlear sulcus angles and more prevalent crossing signs), a J-sign, and patellofemoral articular cartilage damage are more common in patients undergoing revision MPFLR than primary MPFLR. Patients undergoing revision procedures also had a higher number of prior patellar dislocations.
It is not surprising that patients undergoing revision surgery have suffered more previous dislocations, as this group may be more symptomatic and more likely to undergo revision surgery. Previous work has demonstrated that patients with a history of >2 prior patellar dislocations who undergo isolated primary MPFLR demonstrate poorer outcomes than those who have suffered ≤2 prior dislocations, potentially putting such patients at high risk of revision surgery. 22 The effect of BMI on outcomes after MPFLR has been evaluated previously, but previous work has been limited. Sherman et al 28 reported that MPFLR was safe and effective in obese patients with improvements in most PRO measures; however, at the final follow-up visit they had lower quality-of-life and activity scores compared with the patients with a BMI <30. Gibbs et al 9 reported similar results, showing that BMI did not affect complication rates or have poorer PROs at 5-year follow-up. Both of these previous studies focused on PROs and not on the effect of BMI on chances of needing a revision reconstruction. The clinical relevance of the 2.7-kg/m2 difference in BMI noted in this study is unknown.
There are limited data evaluating the effect of potential risk factors on failure risk after MPFLR. One of the reasons for this paucity is that many MPFL cohort studies utilize PROs as their primary endpoint and are underpowered to identify predictors of failure of MPFL surgery requiring revision. Studies looking at tibial tubercle osteotomy in combination with bony procedures are more prone to this sample size limitation, as these procedures are less common. Two previous studies have looked at predictors of PROs after these combined procedures and noted female sex to be a risk factor for poorer results.2,29 However, limited studies identify risk factors for needing revision MPFLR.
The anatomic factors that were noted more frequently in the revision group were the presence of trochlear dysplasia as determined by their trochlear sulcus angle on MRI and crossing sign on plain films. Interestingly, no difference in any patellar height measurements or TT-TG distance was noted between the groups. The explanation for these findings is not clear and the associations are likely multifactorial. One could contend that these findings suggest that patella alta and tibial tubercle lateralization play less of a role in the failure of previous surgery than has been previously thought, as they are not more prevalent in the revision cohort than the primary cohort. Alternatively, these findings could be taken to suggest that patella alta and tubercle lateralization were appropriately addressed when needed at the time of primary MPFLR in most cases, mitigating the prevalence of patella alta and tubercle lateralization in the revision cohort. In contrast, trochlear dysplasia was noted to be much more prevalent in the revision group, which one could interpret as possible undertreatment of trochlear dysplasia in the case of primary surgery.
A clear and unambiguous finding of this study was the elevated presence of a J-sign in the revision cohort. While the drivers of a J-sign have not been clearly articulated, it likely results from some combination of trochlear dysplasia, patella alta, and/or an elevated TT-TG distance.11,32 Previous work has demonstrated a clear association with a J-sign and failure of isolated MPFLR, making it unsurprising that J-signs are common in patients undergoing revision surgery.25,33 The reason for the higher prevalence of articular cartilage damage in the revision group is also likely multifactorial. These patients have had more patellar dislocations, undergone more previous surgery, and have more trochlear dysplasia, increasing their risk of chondral damage. Further, previous work has demonstrated that articular cartilage damage is associated with poorer outcomes of MPFLR, potentially putting these patients at higher risk of undergoing revision surgery. 10
Limitations
The most important limitation of this study to bear in mind is that this is simply a cross-sectional study comparing 2 separate groups of patients---one undergoing primary and one undergoing revision MPFLR. The differences between the groups cannot be directly inferred to be factors that predict failure of primary MPFL surgery. This study identifies factors that are more prevalent in the revision group. The reasons for these differences cannot be provided by this study. In this way, the study should really be seen as hypothesis generating and not as providing definitive answers. A strength of this study is the fact that all patients undergoing MPFLR (revision or primary) during these periods are utilized, including those who underwent bony procedures either before or during the index procedure. The result of this selection process is data that are more broadly applicable to all patellofemoral instability surgery patients than a study limited to those undergoing isolated soft tissue procedures.
Conclusion
Patients undergoing revision MPFLR had more previous patellar dislocations, higher BMI, and more trochlear dysplasia (increased sulcus angle and more frequent crossing sign) than those undergoing primary MPFLR. The revision group was also more likely to have a J-sign on clinical examination and patellar articular cartilage damage at the time of arthroscopy.
Footnotes
Final revision submitted January 16, 2025; accepted March 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.C.K. has received consulting fees and travel and lodging payments from Arthrex Inc. D.C.F. has received consulting fees from Medical Device Business Services Inc, Linvatec Corp, Smith & Nephew, Vericel, and DePuy Synthes; nonconsulting fees from Smith & Nephew; speaking fees from Vericel; and travel and lodging payments from Linvatec, Smith & Nephew, and Medical Device Business Services Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ohio State Biomedical institutional review board (No. 2015H0446).