
Abstract
Background:
Reconstruction of the medial patellofemoral ligament (MPFL) has become a popular surgical procedure to address patellofemoral instability. As a consequence of the growing number of MPFL reconstructions performed, a higher rate of failures and revision procedures has been seen.
Purpose:
To perform a failure analysis in patients with patellar redislocation after primary isolated MPFL reconstruction.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients undergoing revision surgery for reinstability after primary isolated MPFL reconstruction were included. Clinical notes were reviewed to collect demographic data, information on the primary surgery, and the mechanism of patellar redislocation (traumatic vs nontraumatic). Preoperative imaging was analyzed regarding femoral tunnel position and the prevalence of anatomic risk factors (ARFs) associated with patellofemoral instability: trochlear dysplasia (types B through D), patella alta (Caton-Deschamps index >1.2, patellotrochlear index <0.28), lateralization of the tibial tuberosity (tibial tuberosity–trochlear groove distance >20 mm, tibial tuberosity–posterior cruciate ligament [TT-PCL] distance >24 mm), valgus malalignment (mechanical valgus axis >5°), and torsional deformity (internal femoral torsion >25°, external tibial torsion >35°). The prevalence of ARF was compared between patients with traumatic and nontraumatic redislocations and between patients with anatomic and nonanatomic femoral tunnel position.
Results:
A total of 26 patients (69% female) with a mean age of 25 ± 7 years were included. The cause of redislocation was traumatic in 31% and nontraumatic in 69%. Position of the femoral tunnel was considered nonanatomic in 50% of patients. Trochlear dysplasia was the most common ARF with a prevalence of 50%, followed by elevated TT-PCL distance (36%) and valgus malalignment (35%). The median number of ARFs per patient was 3 (range, 0-6), and 65% of patients had 2 or more ARFs. Patients with nontraumatic redislocations showed significantly more ARFs per patient, and the presence of 2 or more ARFs was significantly more common in this group. No significant difference was observed between patients with anatomic versus nonanatomic femoral tunnel position.
Conclusion:
Multiple anatomic risk factors and femoral tunnel malposition are commonly observed in patients with reinstability after primary MPFL reconstruction. Before revision surgery, a focused clinical examination and adequate imaging including radiographs, magnetic resonance imaging (MRI), standing full-leg radiographs, and torsional measurement with computed tomography or MRI are recommended to assess all relevant anatomic parameters to understand an individual patient’s risk profile. During revision surgery, care must be taken to ensure anatomic placement of the femoral tunnel through use of anatomic and/or radiographic landmarks.
Patellofemoral stability is a complex interaction between dynamic muscle action, passive soft tissue restraints, the surface geometry of the patella and trochlea, and limb alignment. 38,71 Therefore, patellofemoral instability is commonly seen as a multifactorial problem.
The medial patellofemoral ligament (MPFL) is the main passive soft tissue restraint against lateral patellar translation during the first 30° of flexion, providing 50% to 60% of the total restraining force. 18,71 MPFL insufficiency is found in most patients with recurrent patellar dislocation. 58 Therefore, reconstruction of the MPFL has become a popular surgical procedure to address patellofemoral instability with good clinical results and a low redislocation rate. 36,66 However, as a consequence of the increasing number of MPFL reconstructions performed, a higher rate of failures and revision procedures has been seen. 29,59 The main reasons for failed MPFL reconstruction are technical errors and disregard for additional risk factors. 13,56,59,73 With regard to technical errors, femoral tunnel positioning is especially critical because a nonanatomically placed tunnel can cause excessive strain on the graft, leading to stretching and insufficiency of the reconstructed MPFL. 11,37,77,78
Multiple anatomic risk factors (ARFs) predisposing to first-time patellar dislocation and recurrence after first-time dislocation have been described, including trochlear dysplasia, patella alta, lateralization of the tibial tuberosity, valgus malalignment, and torsional deformity. 1 –4,14,17,22,75 In the presence of 1 or more ARFs, MPFL reconstruction may not be sufficient as an isolated procedure, because the lack of bony constraint and an increased laterally directed force vector may lead to overload of the MPFL graft. Several authors have found an association between the presence of ARFs and unsatisfactory outcomes as well as failure after isolated MPFL reconstruction. § Therefore, failure to consider additional risk factors must also be regarded as an important risk factor for redislocation after MPFL reconstruction. 13,56,59,73
Revision surgery after primary MPFL reconstruction is complex, and the results have been reported to be worse than after primary procedures. 13,56 Thorough knowledge of possible risk factors is therefore necessary for adequate preoperative patient assessment and consecutive individualized treatment. However, few studies have specifically analyzed patients after failed MPFL reconstruction . 13,56 The purpose of this study was thus to perform a detailed failure analysis among patients with patellar redislocation after primary MPFL reconstruction. The hypothesis was that ARFs and femoral tunnel malposition are commonly observed in this group of patients.
Methods
Ethical approval for this study was granted from the Technical University Munich. A retrospective cohort design was used to conduct a failure analysis of patients with patellar redislocation after primary isolated MPFL reconstruction.
A chart review was performed using an electronic medical record system to identify all patients undergoing revision surgery after primary MPFL reconstruction between November 2012 and April 2019 at our institution. A total of 83 patients were initially identified. For the purpose of this study, only patients with patellar reinstability, defined as at least 1 patellar redislocation after primary isolated MPFL reconstruction, were included. Excluded were patients undergoing revision surgery for other reasons, such as patellofemoral pain, patellofemoral cartilage defects, and restricted range of motion. Further exclusion criteria were previous or concomitant soft tissue or bony procedures at the ipsilateral knee; absence of preoperative imaging, with conventional radiographs and magnetic resonance imaging (MRI) representing the minimum requirement; and metal implants in the knee area with artifacts on MRI scans or motion artifacts. A flowchart of patient inclusion in the analysis is shown in Figure 1.

Flowchart of patient inclusion in the analysis. MPFL, medial patellofemoral ligament; MRI, magnetic resonance imaging; ROM, range of motion.
Preoperative (prerevision) workup consisted of a thorough clinical examination and an extended radiographic analysis. In all patients, we performed conventional radiographs of the affected knee in 3 planes as well as MRI. Additional radiographic examination of coronal and torsional limb alignment depended on the clinical examination: Coronal limb alignment was evaluated visually with the patient in a standing position and neutral foot position. 35 Patients were asked to adduct their lower limbs until either the knees or ankles touched. Neutral coronal alignment was assumed if knees and ankles touched simultaneously. 35 If either the knees or ankles touched first, coronal malalignment was assumed and a standing full-leg radiograph was performed for further evaluation (n = 21; 81% of patients). Screening for abnormal femoral torsion was performed with the patient in the prone position with the hips extended and the knees flexed to 90°. Passive internal and external rotation of the hip was then measured with a goniometer. The maximal external-internal rotation angle was defined as the angle between the tibia and a virtual axis vertical to the ground. 15 In addition, the trochanteric prominence angle test was performed, as described in detail elsewhere. 61 In brief, external rotation of the hip was measured when the greater trochanter was at its most laterally prominent position. Values indicating increased femoral torsion were maximal internal rotation greater than 60°, maximum external rotation less than 30°, and trochanteric prominence angle test greater than 25°. 15,61 Tibial torsion was estimated in the same patient position by measuring the transmalleolar angle, which was defined as the angle between a line perpendicular to the axis connecting the most prominent aspects of the medial and lateral malleolus and the line of the longitudinal axis of the thigh. 74 If the transmalleolar angle was greater than 35°, increased tibial external torsion was assumed. In the case of clinically abnormal femoral and/or tibial torsion, axial MRI scans that included the hip, knee, and ankle were performed for further evaluation (n = 18; 69% of patients). Furthermore, in patients with unclear position of the femoral tunnel, a computed tomography (CT) scan of the knee with 3-dimensional reconstruction was obtained.
Data Collection
Preoperative clinical notes of all patients were reviewed to collect demographic data, including sex, age at surgery, and body mass index (BMI). Furthermore, relevant information about the primary surgery and the mechanism of injury leading to redislocation of the patella was collected. Redislocations occurring during high-impact sports (eg, football, basketball, downhill skiing) and contact injuries were considered traumatic redislocations, whereas redislocations that occurred during low-impact sports or activities of daily living were considered nontraumatic.
All analyzed images were obtained before revision surgery (after the failed primary isolated MPFL reconstruction). Imaging was analyzed regarding femoral tunnel position and the prevalence of ARFs associated with patellofemoral instability (trochlear dysplasia, patella alta, lateralization of the tibial tuberosity, valgus malalignment, and torsional deformity). 1 –4,14,17,22,75 All radiographic measurements were performed by 2 orthopaedic residents specifically trained in the measurements obtained in the present study (J.M., D.P.B.). To determine the interobserver reproducibility, intraclass correlation coefficients (ICCs) were calculated.
The following measurements and classifications were performed:
Femoral Tunnel Position
The position of the femoral tunnel was analyzed on lateral radiographs through use of the landmarks described by Schöttle et al 68 or, if available, on 3-dimensional CT reconstructions according to Fujino et al. 30 The femoral tunnel was considered nonanatomic if the center of the tunnel was more than 7 mm away from the Schöttle point, as described by Servien et al. 72
Trochlear Dysplasia
The shape of the trochlea was categorized according to the Dejour classification on MRI through use of the 3 most proximal images demonstrating articular cartilage. 16 Significant trochlear dysplasia was defined as a flat or convex trochlea (Dejour type B, C, and D). 48,75
Caton-Deschamps Index (CDI)
The CDI was determined on lateral radiographs as the ratio between the distance from the lower border of the patella to the tibial plateau and the length of the retropatellar surface. 9 Knees with a ratio greater than 1.2 were considered to have patella alta (pathologic CDI). 9,17
Patellotrochlear Index (PTI)
The PTI was measured on sagittal MRI as described by Biedert and Albrecht. 8 In contrast to the original protocol, imaging was obtained with the knee in a slightly flexed position instead of a fully extended position. The length ratio between the articular surface of the patella and the articulating trochlea was calculated. A ratio less than 0.28 was considered pathologic. 9
Tibial Tuberosity–Trochlear Groove (TT-TG) Distance
The TT-TG distance was measured on axial MRI scans as the mediolateral distance between the midpoint of the insertion of the patellar tendon and the trochlear groove. 17,67 A TT-TG distance of greater than 20 mm was considered pathologic. 17
Tibial Tuberosity–Posterior Cruciate Ligament (TT-PCL) Distance
The TT-PCL distance was measured on axial MRI scans as described by Seitlinger et al 70 and defined as the mediolateral distance between the midpoint of the insertion of the patellar tendon and the medial border of the PCL. A TT-PCL distance of greater than 24 mm was considered pathologic. 70
Coronal Mechanical Axis
Coronal mechanical alignment was measured on standing full-leg radiographs as the angle between a line from the center of the femoral head to the center of the knee and a line from the center of the ankle to the center of the knee. Positive values indicate a mechanical valgus axis, and a valgus angle greater than 5° was considered pathologic. In patients with no measurement (n = 5; 19% of patients), frontal mechanical axis was considered normal based on the clinical examination described above.
Femoral and Tibial Torsion
Torsion of the lower extremity was assessed on rotational MRI as described by Schneider et al. 65 Femoral torsion was calculated as the angle between a line through the center of the femoral head and neck and a tangent along the posterior border of the femoral condyles. Tibial torsion was measured as the angle between the dorsal tibial condylar line and a line through the medial and lateral malleolus. For femoral torsion, positive values indicate internal femoral torsion and values greater than 25° were considered pathologic. 80 For tibial torsion, positive values indicate external tibial torsion and values greater than 35° were considered pathologic. 80 In patients with no measurement (n = 8; 31% of patients), torsion was considered normal based on the clinical examination described above.
Statistical Analysis
Statistical analysis was performed with SPSS software (version 25.0; IBM-SPSS). Continuous variables were calculated as mean ± SD (normal distribution) or median and range (nonnormal distribution). Categorical variables were reported as count and percentage.
Normal distribution of all data was evaluated with the Kolmogorov-Smirnoff test. For each ARF, the prevalence of pathologic values based on the above-mentioned thresholds was calculated. Furthermore, the total number of ARFs was calculated for each patient (combined prevalence). The number of ARFs per patient and the combined prevalence of ARFs was compared between patients with traumatic versus nontraumatic redislocations and between patients with anatomic versus nonanatomic femoral tunnel position through use of the Fisher exact test, Mann-Whitney U test, or unpaired t test, as appropriate. ICCs were calculated to determine the interobserver reproducibility. ICC values greater than 0.9 were considered excellent, values between 0.8 and 0.9 were considered good, and values less than 0.8 were considered poor.
Results
A total of 26 patients (69% female) with a mean age of 25 ± 7 years were included. The left knee was affected in 54%, and the mean BMI was 24 ± 5 kg/m2. The primary MPFL reconstruction was performed at our institution in 46% of patients, whereas 54% of patients underwent MPFL reconstruction elsewhere. MPFL reconstruction was performed with a gracilis tendon autograft in 24 patients (92%) and with a semitendinosus tendon autograft in 2 patients (8%).
The cause of redislocation was traumatic in 31% of patients and nontraumatic in 69%. Position of the femoral tunnel was considered nonanatomic in 50% of patients. ARF measurements and corresponding interobserver ICCs are shown in Table 1, and the prevalence of ARFs is shown in Table 2. In summary, trochlear dysplasia was the most common ARF with a prevalence of 50%, followed by elevated TT-PCL distance (36%) and valgus malalignment (35%).
Anatomic Risk Factor Measurements a
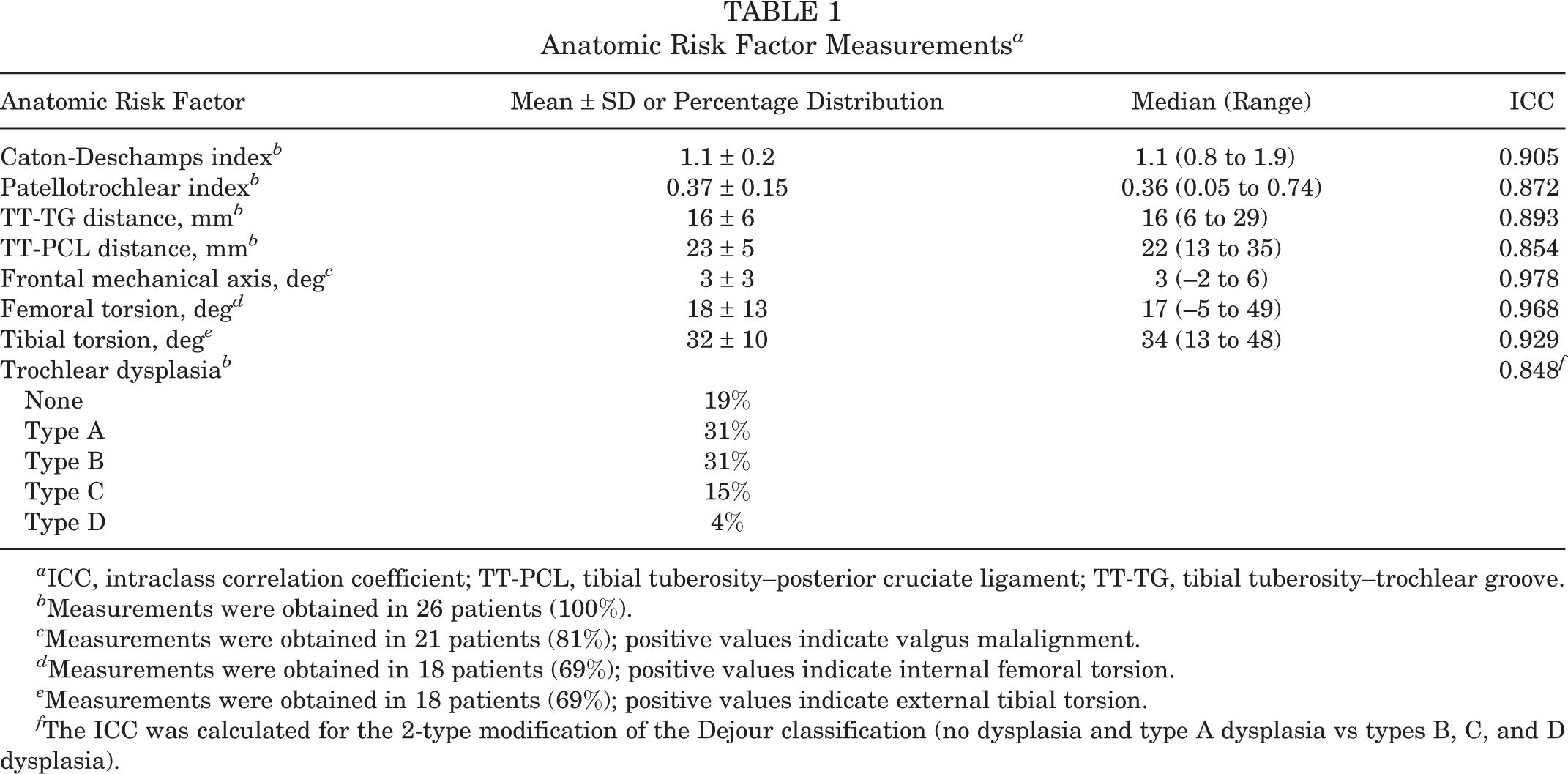
a ICC, intraclass correlation coefficient; TT-PCL, tibial tuberosity–posterior cruciate ligament; TT-TG, tibial tuberosity–trochlear groove.
b Measurements were obtained in 26 patients (100%).
c Measurements were obtained in 21 patients (81%); positive values indicate valgus malalignment.
d Measurements were obtained in 18 patients (69%); positive values indicate internal femoral torsion.
e Measurements were obtained in 18 patients (69%); positive values indicate external tibial torsion.
f The ICC was calculated for the 2-type modification of the Dejour classification (no dysplasia and type A dysplasia vs types B, C, and D dysplasia).
Prevalence of Anatomic Risk Factors a
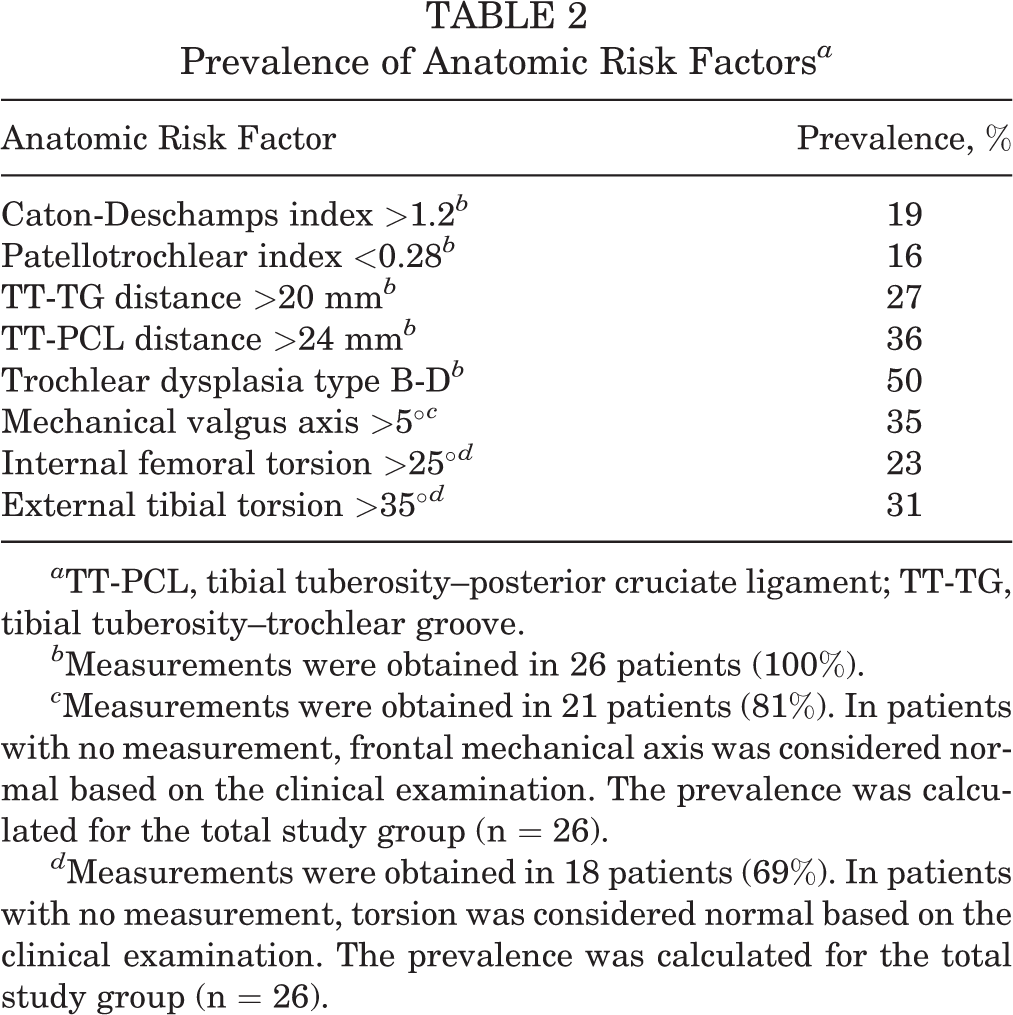
a TT-PCL, tibial tuberosity–posterior cruciate ligament; TT-TG, tibial tuberosity–trochlear groove.
b Measurements were obtained in 26 patients (100%).
c Measurements were obtained in 21 patients (81%). In patients with no measurement, frontal mechanical axis was considered normal based on the clinical examination. The prevalence was calculated for the total study group (n = 26).
d Measurements were obtained in 18 patients (69%). In patients with no measurement, torsion was considered normal based on the clinical examination. The prevalence was calculated for the total study group (n = 26).
The combined prevalence of ARFs is summarized in Table 3. The median number of ARFs per patient was 3 (range, 0-6), and 65% of patients had 2 or more ARFs (Figure 2).
Combined Prevalence of Anatomic Risk Factors


Combined prevalence of anatomic risk factors (ARFs). The majority of patients (65%) had 2 or more ARFs.
The results of the group comparison between patients with a traumatic versus nontraumatic redislocation are shown in Table 4. The group of patients with nontraumatic redislocations showed a significantly higher number of ARFs per patient, and the presence of 2 or more ARFs was significantly more common in this group (P < .001 for both) (Figure 3).
Group Comparison Between Traumatic and Nontraumatic Redislocations a

a ARF, anatomic risk factor.
b Statistically significant difference between both groups.

Comparison of patients with a traumatic and nontraumatic redislocation. The presence of 2 or more anatomic risk factors (ARFs) was significantly more common in patients with nontraumatic redislocations.
Group comparison between patients with anatomic versus nonanatomic femoral tunnel position did not show any significant differences with regard to the presence of ARFs (P > .05).
Discussion
The most important finding of the present study was that multiple ARFs and femoral tunnel malposition are commonly observed in patients with patellar redislocation after primary MPFL reconstruction. Trochlear dysplasia was the most common ARF, observed in 50% of patients. No ARF was observed in only 15% of patients, whereas 2 or more ARFs were observed in 65%. The group of patients with nontraumatic redislocations had a significantly higher number of ARFs per patient, and the presence of 2 or more ARFs was significantly more common in this group versus patients with traumatic dislocations.
Reconstruction of the MPFL has become a widespread surgical procedure for recurrent patellar dislocation. 66 One of the most critical steps of MPFL reconstruction is anatomic placement of the femoral tunnel, and several studies have demonstrated significant negative clinical and biomechanical effects of tunnel malposition. 37,59,63,77 In the present study, a nonanatomically placed femoral tunnel was found in 50% of patients. Therefore, femoral tunnel malposition seems to be a common problem in patients with reinstability after primary MPFL reconstruction. This association can be well explained by biomechanical studies. The native MPFL has been found to be nearly isometric between 0° and 110° of knee flexion. 78 Nonanatomic graft placement, however, has been shown to dramatically alter graft isometry; placement of the attachment site only 5 mm distally or proximally has led to significantly increased length of the MPFL during flexion. 78 This increased strain on the MPFL graft can cause stretching and elongation of the graft, leading to insufficiency and consecutive redislocation of the patella. 11 In other clinical studies, malpositioned femoral tunnels have been associated with postoperative complications, 81 recurrent patellar instability or patellofemoral pain, 37,59 and tunnel widening. 69 Despite knowledge about the importance of anatomic tunnel placement, the rate of nonanatomic placement is reported to be as high as 60%. 52,72 The femoral MPFL insertion site can be identified fluoroscopically through use of radiographic landmarks on a true lateral knee radiograph or by palpation of anatomic landmarks. Many authors prefer the radiographic method because this technique can be performed percutaneously with very small skin incisions. Several radiographic landmarks have been described in the past, 7,68,78 with the “Schöttle point” 68 being the most commonly used reference. Despite the widespread use of this method, several authors have questioned its accuracy and have recommended that radiographic landmarks should not be the sole basis for femoral attachment location. 39,62 The most accurate method may therefore be a combination of radiographic and anatomic landmarks. 39 The femoral insertion of the MPFL has been reported to be located in between the adductor tubercle and the medial epicondyle, with a closer relationship to the adductor tubercle (2 mm anterior and 4 mm distal, according to LaPrade et al 43 ).
Patellofemoral instability must be considered a multifactorial problem because patellofemoral stability depends on the interaction of dynamic and static soft tissue restraints, the surface geometry of the patella and trochlea, and limb alignment. Increasing evidence shows that the bony geometry and limb alignment play a major role in patellofemoral instability. Several studies have identified multiple ARFs predisposing to first-time patellar dislocation and recurrence after first-time dislocation, including trochlear dysplasia, patella alta, lateralization of the tibial tuberosity, valgus malalignment, and torsional deformity. 1 –4,14,17,22,75 Whereas some authors have found good clinical outcomes and low redislocation rates after isolated MPFL reconstruction even in the presence of ARFs, 24,49,51,60,76 other authors have found a correlation between ARFs and unsatisfactory outcomes and failure after MPFL reconstruction. ∥ Therefore, additional stabilization procedures are increasingly performed in combination with MPFL reconstruction, such as trochleoplasty, 5,6,10,34,54 medialization or distalization of the tibial tuberosity, 12,26,44,50 and osteotomies to correct torsion and/or valgus malalignment. 19 –23,27,28,55 The results of the current study suggest that the presence of ARFs is related to failure after MPFL reconstruction, as only 15% of patients had no ARFs, whereas 2 or more ARFs were observed in 65% of patients.
In the present study, trochlear dysplasia was the most common ARF, with a prevalence of 50%, followed by elevated TT-PCL distance (36%) and valgus malalignment (35%). Trochlear dysplasia and a lateralized tibial tuberosity (defined as a pathologic TT-PCL or TT-TG distance) are well-accepted risk factors for recurrence after first-time patellar dislocation and for failure after MPFL reconstruction. 4,14,33,37,42,75,82 Both factors are included in well-established risk scores such as the patellar instability severity score. 4 The role of valgus malalignment and torsional deformities in patellofemoral instability is less well understood. However, increasing evidence shows that both valgus and torsional malalignment promote patellar instability. Valgus malalignment has been shown to alter the force vector on the patella by increasing the Q-angle, leading to lateralization of the patella. 19,28,53,57 In patients with isolated MPFL reconstruction but uncorrected valgus malalignment, the increased laterally directed force vector may lead to failure of the MPFL graft due to repetitive overloading. The same is true for increased internal femoral torsion and increased external tibial torsion. Biomechanical studies have demonstrated that both deformities result in lateralization of the patella and abnormal lateral patellofemoral loads. 31,40,41,45 –47 Furthermore, Kaiser et al 41 showed that isolated MPFL reconstruction cannot restore patellar stability in cases with higher degrees of internal femoral torsion. In the present study, increased internal femoral torsion and increased external tibial torsion were found in 23% and 31% of patients, respectively. Therefore, assessment of frontal and torsional alignment is important in patients with patellar instability, especially after failed MPFL reconstruction.
Only a few studies have specifically analyzed patients after failed MPFL reconstruction. Nelitz et al 56 analyzed 19 patients who underwent revision surgery after MPFL reconstruction because of disabling pain and/or loss of flexion (n = 13) or recurrent instability (n = 6). Those investigators observed 3 main reasons for failure after MPFL reconstruction: failure to consider ARFs, technical errors, and inappropriate patient selection. Trochlear dysplasia was the most common ARF, which was observed in 5 of 6 patients with recurrent instability. In 2 patients, concomitant excessive femoral anteversion was detected. Femoral tunnel malposition was commonly observed in patients with pain and loss of flexion. Chatterton et al 13 evaluated 23 patients undergoing revision surgery after failed primary MPFL reconstruction and compared patient outcomes with 224 primary MPFL reconstructions. Those authors found an incorrectly placed femoral tunnel in 67% of patients with failed MPFL reconstruction. Severe trochlear dysplasia types C and D were seen in 36% of patients with failed MPFL reconstruction compared with 30% of patients with primary MPFL reconstruction. However, this difference was not statistically significant. Subjective outcomes did not improve significantly after revision MPFL reconstruction, and the final results were poorer in the revision group than in the primary MPFL group.
The current study has several limitations. First, this was a descriptive study without a control group. Therefore, we were unable to prove that the identified ARFs were causative for failure. Second, it remains unclear which factors are the most relevant. Therefore, no conclusions about surgical decision making could be drawn. Further research is necessary to determine to what extent each factor contributes to MPFL failure. Third, valgus alignment and torsion were assessed only in patients with conspicuous clinical examination. In patients without radiographic evaluation, leg axis and torsion were considered normal for data analysis. Therefore, valgus and torsional malalignment may have been underestimated in the present study. Fourth, there are other possible factors for failure that could not be assessed in the present study, such as surgeon experience, initial tension of the graft, failure of the graft to incorporate, abrasion of the graft at the femoral or tibial attachment site, and overly aggressive rehabilitation.
Despite these limitations, the findings of the present study have several implications for clinical practice. First, extensive knowledge of both anatomic and radiographic landmarks for anatomic femoral tunnel placement is necessary in order to avoid tunnel malposition. 7,30,39,67 Second, given the high prevalence and combined prevalence of ARFs, a focused clinical examination and adequate imaging are crucial to assess all relevant anatomic parameters in order to understand an individual patient’s risk profile. We recommend conventional radiographs of the affected knee in all 3 planes as well as MRI in all cases. Additional radiographic measurement of coronal alignment and torsion is recommended if the clinical examination as described in the Methods section is conspicuous. If coronal malalignment is suspected, an additional standing full-leg radiograph should be performed. In the case of conspicuous internal rotation of the hip or external rotation of the lower leg, torsion of the femur and tibia should be assessed with hip-knee-ankle CT or MRI. 65 After all ARFs have been identified, a tailored approach should be considered. In our opinion, isolated revision MPFL reconstruction should be limited for patients without ARFs. In accordance with other authors, we recommend additional stabilization procedures such as trochleoplasty, 5,6,10,34,54 osteotomies to correct torsion and/or valgus alignment, 19 –23,27,28,55 or transfer of the tibial tuberosity 12,26,44,50 in order to address all possible associated patellar instability risk factors. This is especially important in revision cases because isolated MPFL reconstruction has been shown to be insufficient. Our treatment algorithm for patients with reinstability after primary MPFL reconstruction is presented in Figure 4.
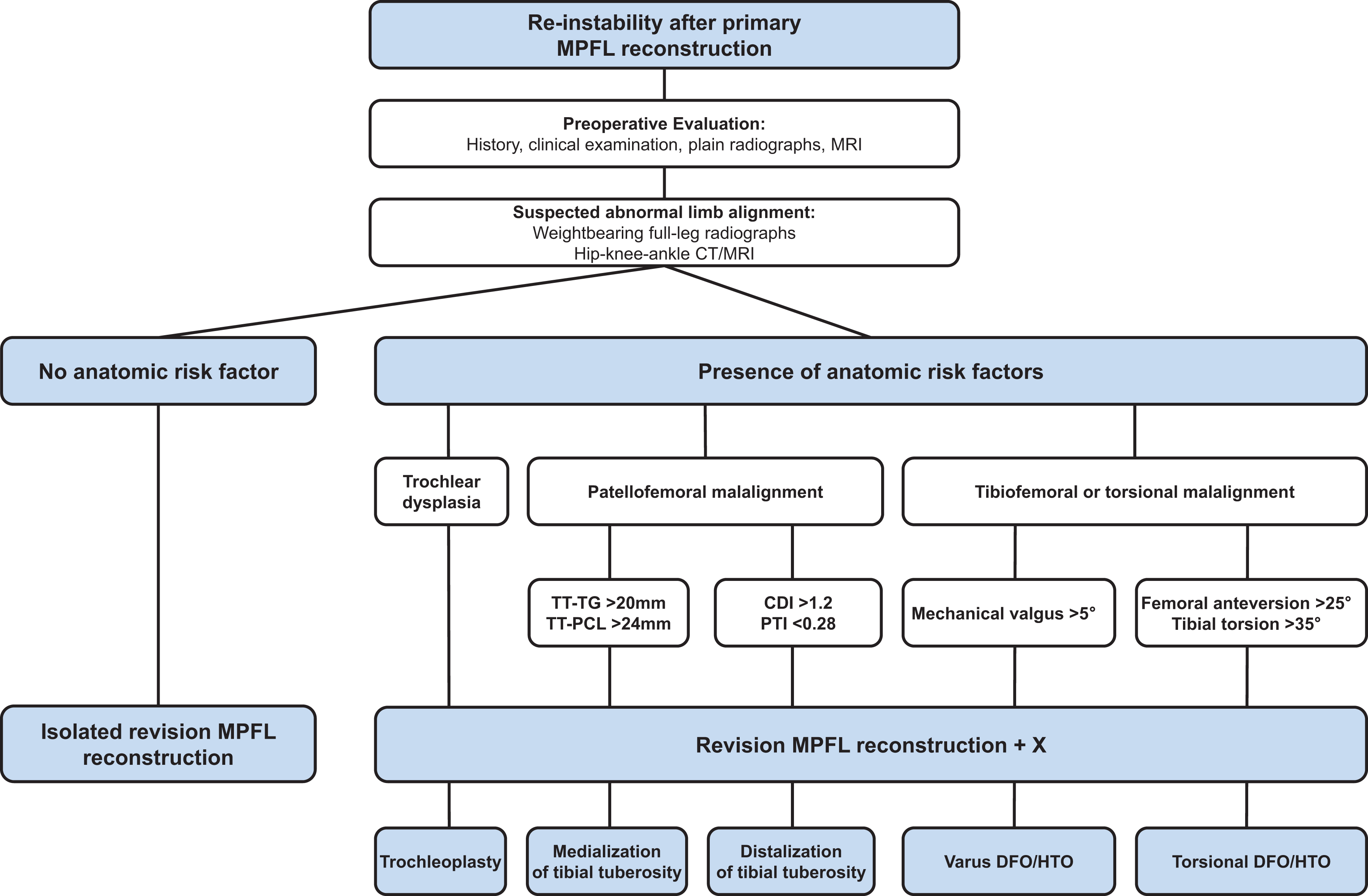
Treatment algorithm for patients with reinstability after primary MPFL reconstruction. CDI, Caton-Deschamps index; CT, computed tomography; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; MPFL, medial patellofemoral ligament; MRI, magnetic resonance imaging; PTI, patellotrochlear index; TT-PCL, tibial tuberosity–posterior cruciate ligament distance; TT-TG, tibial tuberosity–trochlear groove distance.
An individualized treatment plan is still necessary because it remains unknown when to surgically correct ARFs in isolation or in combination. In most cases, complex corrections are required, and extensive experience in patellofemoral surgery is necessary to achieve satisfying outcomes for patients.
Conclusion
Multiple ARFs and femoral tunnel malposition are commonly observed in patients with reinstability after primary MPFL reconstruction. A focused clinical examination and adequate imaging including radiographs, MRI, standing full-leg radiographs, and torsional measurement with CT or MRI are recommended to assess all relevant anatomic parameters in order to understand an individual patient’s risk profile. During revision surgery, care must be taken to ensure anatomic placement of the femoral tunnel through use of anatomic and/or radiographic landmarks.