
Abstract
Background:
The need for concomitant bony procedures to realign pathoanatomic risk factors in addition to medial patellofemoral ligament reconstruction (MPFL-R) remains unclear.
Purpose:
To evaluate a clinically derived 2-part classification of lateral patellar instability aimed at identifying patients indicated for a concomitant bony procedure.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The study included 122 patients (42 male, 80 female; mean ± SD age, 22 ± 6 years) who were assigned to a mild instability group (mIG) and a complex instability group (cIG) based on the reversed dynamic patellar apprehension test (ReDPAT) and J-sign. The mIG had a positive ReDPAT result <40° to 50° of knee flexion and an absent or low-grade J-sign (grade 1), and the cIG had a positive ReDPAT result >40° of knee flexion and/or a high-grade J-sign (grade 2 or 3). The mIG underwent isolated MPFL-R, and the cIG underwent MPFL-R and concomitant bony procedures depending on the established risk factor assessment. For evaluation, the BANFF Patellar Instability Instrument 2.0 (BPII 2.0) and numeric analog scale (0-10) for patellofemoral pain and subjective knee function were used. The minimal clinically important difference for the BPII 2.0 was ascertained by calculating half the standard deviation of baseline scores.
Results:
Radiographic analysis confirmed a significantly more pronounced pathoanatomic risk factor constellation in the cIG regarding severity of trochlear dysplasia, distal malalignment, and patellar height (all P < .05). At final follow-up, no patellar redislocation occurred in either group; 2 patients in the cIG reported patellar subluxation. Within both groups, all outcome scores improved significantly pre- to postoperatively (all P < .0001); no between-group difference was found regarding BPII 2.0 score and numeric analog scale for function. The minimal clinically important difference for the BPII 2.0 was met by 84% (32/38) of the mIG and 90% (76/84) of the cIG (P = .36), but the cIG experienced more patellofemoral pain than the mIG (1.3 ± 1.6 vs 2.1 ± 2.1; P = .036).
Conclusion:
Patients with a high-grade J-sign and/or a positive ReDPAT finding beyond 40° to 50° of knee flexion exhibited a significantly more pronounced pathoanatomic risk factor constellation; however, the correction of modifiable risk factors led to similarly good outcomes to patients who underwent isolated MPFL-R. A slightly higher level of patellofemoral pain after bony procedures was evident in these patients.
The medial patellofemoral ligament is the most important passive stabilizer of the patella between 0° and 30° of knee joint flexion. 1,11 In higher degrees of flexion, though, bony factors are crucial for stable patellar tracking. 38 Reconstruction of the medial patellofemoral ligament (MPFL-R) has been established in patients with recurrent lateral patellar instability (LPI), and the results are characterized by good functional outcome scores and low patellar redislocation rates. 24,28,34,36 However, bony risk factors for LPI—including trochlear dysplasia, patella alta, increased tibial tuberosity–trochlear groove (TT-TG) distance, and valgus or torsional deformities—negatively affect functional outcome scores and redislocation rates after isolated MPFL-R. 4,15,16,18,19,24,31,35
The current literature is still inconclusive regarding the indication and need for a concomitant bony correction in addition to MPFL-R. 9 Basing the decision solely on recommended thresholds of anatomic risk factors (eg, trochlear dysplasia, patellar height, TT-TG distance), which are influenced by nuances of imaging modalities and observer-dependent reliability, has been put into question. 29 Additionally, recent studies have emphasized the importance of a more clinically derived patellar instability assessment protocol. 26,29,44,45,48 In this regard, the importance of 2 clinical tests has recently been raised. First, the dynamic evaluation of the patellar apprehension test represents the patient-specific end of stable patellar tracking and the beginning of patellar stabilizer insufficiency. 8,48 Second, the J-sign evaluates patellar tracking during active knee joint motion, thereby reflecting overall patellar tracking or maltracking of an individual’s anatomy, and it affects clinical outcome scores and graft laxity after MPFL-R. 20,29,44,45
Accordingly, 2 major forms of recurrent LPI might be proposed 2 : a mild form characterized by a positive patellar apprehension test result ranging from 0° to 40° (50°) of knee joint flexion and an absent or low-grade J-sign (grade 1) and a complex form characterized by a positive patellar apprehension test result >40° of knee joint flexion and/or severe patellar maltracking (grade 2 or 3 J-sign).
The purpose of this study was to evaluate this clinically derived 2-part classification of LPI considering the preoperative J-sign and dynamic patellar apprehension test evaluation as a decision aid aimed at identifying patients indicative of a concomitant bony correction in addition to MPFL-R. The hypothesis was that in patients with complex LPI, the concomitant correction of bony pathoanatomy in addition to MPFL-R will yield equivalent results to patients with mild LPI who are candidates for isolated MPFL-R.
Methods
The protocol for this study received approval by the local ethics committee and participants provided informed consent. This was a retrospective analysis of a longitudinally maintained database; the study cohort comprised 122 patients (42 male, 80 female; mean ± SD age, 22 ± 6 years) who underwent surgical treatment for recurrent LPI between April 2015 and April 2019. To be included, patients had to have ≥2 objective lateral patellar dislocations with failed nonoperative treatment over a period of at least 6 months. The exclusion criteria were as follows: (1) previous patellar stabilizing surgery, (2) first-time patellar dislocation undergoing primary surgery attributed to an osteochondral flake fracture or a primary patellar stabilization procedure, (3) patellofemoral pain with patellofemoral malalignment but without objective findings of LPI, and (4) other previous knee ligament injuries or ligament surgery (eg, anterior cruciate ligament reconstruction).
Demographics, clinical evaluation, assessment of pathoanatomic risk factors, and patient-reported disease-specific quality of life were assessed in all patients before surgery. The clinical evaluation comprised the reversed dynamic patellar apprehension test (ReDPAT) 48 and evaluation of the J-sign. 44 The ReDPAT extends the knee joint from a deep flexion angle with lateral force applied to the medial side of the patella and checks for the first onset of a subjective apprehensive reaction. This flexion angle is measured with a goniometer and determines the patient-specific end of stable patellar tracking and the beginning of patellar stabilizer insufficiency. 48 For evaluation of the J-sign, the patient was asked to actively extend the knee from a seated position with knees flexed to 90°. The J-sign was defined as positive if there was a lateral patellar shift during active terminal extension. Grading of the J-sign was performed according to a modified clinical grading system published by Zhang et al 44 : grade 0 (normal), absence of J-sign; grade 1 (mild), 1 to 2 quadrants of motion; grade 2 (apparent), 2 to 3 quadrants of motion; grade 3 (severe), >3 quadrants of motion or complete patellar dislocation at extension. All investigations were performed by the senior author (P.B.).
All included patients underwent preoperative radiographic imaging of the affected knee (anteroposterior standing long-leg and true-lateral knee joint at 30° of flexion), as well as native magnetic resonance imaging (MRI). Additionally, torsional MRI scans were performed in cases with clinically considered rotational malalignment (>70° of internal hip rotation in the prone position). Images were assessed regarding established anatomic risk factors for LPI. The severity of trochlear dysplasia was evaluated according to the method described by Dejour and Le Coultre 10 (type A, mild dysplasia; types B-D, severe dysplasia). Patella alta was defined as patellar height >1.2 according to the Caton-Deschamps index. 7 The TT-TG distance and the tibial tuberosity–posterior cruciate ligament (TT-PCL) insertion distance were considered high when the values were >16 and >24 mm, respectively. 3,37 Valgus malalignment was considered when the values of the mechanical hip-knee-ankle axis were ≥4° on standing long-leg radiograph.
On the basis of clinical findings, patients were categorized into a mild instability group (mIG) and a complex instability group (cIG). The mIG had a positive ReDPAT finding <40° to 50° of knee flexion and an absent or low-grade J-sign (grade 1), and the cIG had a positive ReDPAT finding >40° of knee joint flexion and/or a high-grade J-sign (grade 2 or 3). Five patients could not be clearly assigned to one of the groups: they had a positive ReDPAT result between 40° and 50° but no high-grade J-sign and no pathoanatomic risk factor exceeding the aforementioned thresholds. These patients were assigned to the mIG. Thus, 38 patients were assigned to the mIG and 84 patients to the cIG (Figure 1).

Flowchart of patient evaluation, classification, and treatment. §Patients with a positive ReDPAT result up to 50° but without a severe J-sign and without pathoanatomic risk factors were assigned to the mild instability group. AP, anteroposterior; cIG, complex instability group; mIG, mild instability group; MPFL-R, medial patellofemoral ligament reconstruction; MRI, magnetic resonance imaging; ReDPAT, reversed dynamic patellar apprehension test.
The mIG underwent isolated MPFL-R using a pedicled quadriceps tendon autograft with femoral interference screw fixation. 47 The cIG underwent concomitant pathoanatomic risk factor correction in addition to MPFL-R. Deepening trochleoplasty was considered in type B or D trochlear dysplasia, and transfer of the tibial tuberosity was considered when the TT-TG distance exceeded 20 mm, the TT-PCL insertion distance exceeded 24 mm, and/or when the Caton-Deschamps index was ≥1.3. Torsional osteotomy was considered when the femoral antetorsion exceeded 25° on the rotational MRI scan, and valgus correction was performed when the genu valgum value of the hip-knee-ankle axis was ≥4°.
For the evaluations, the validated Banff Patellofemoral Instability Instrument 2.0 (BPII 2.0) 5 was used to assess patient-reported disease-specific quality of life before surgery and at the final follow-up. In addition, a numeric analog scale (0-10 points) was used to assess the intensity of patellofemoral pain (0, no pain; 10, most severe pain) and subjective knee joint function (0, severely restricted; 10, normal function) preoperatively and at final follow-up as previously published. 47
Statistical Analysis
The normality of the continuous data was assessed, and data are presented as mean ± SD. Categorical and dichotomous data are presented as frequency tabulations. Contingency tables using Fisher exact test, unpaired and paired 2-tailed t tests, Wilcoxon signed-rank tests, and Mann-Whitney U tests were used to assess the differences between the pre- and postoperative clinical data and between the mIG and cIG. The minimal clinically important difference (MCID) was ascertained with the distribution-based method by calculating half the standard deviation of the baseline BPII 2.0 score. 32 All analyses were performed using Prism (Version 4; GraphPad Software). The significance level was set at .05. The post hoc power analysis was performed with G*Power-1 (Version 3.1.3; Heinrich-Heine-University Software, Apps and Games; free download) (effect size d = 0.2 considered a "small" effect size; d = 0.5 considered a "medium" effect size; d = 0.8 considered a "large" effect size).
Results
Demographics, clinical findings, anatomic risk factor profiles, and operative treatment procedures are shown in Tables 1 and 2.
Demographics, Clinical Findings, and Anatomic Risk Factor Profile of the Study Cohort a
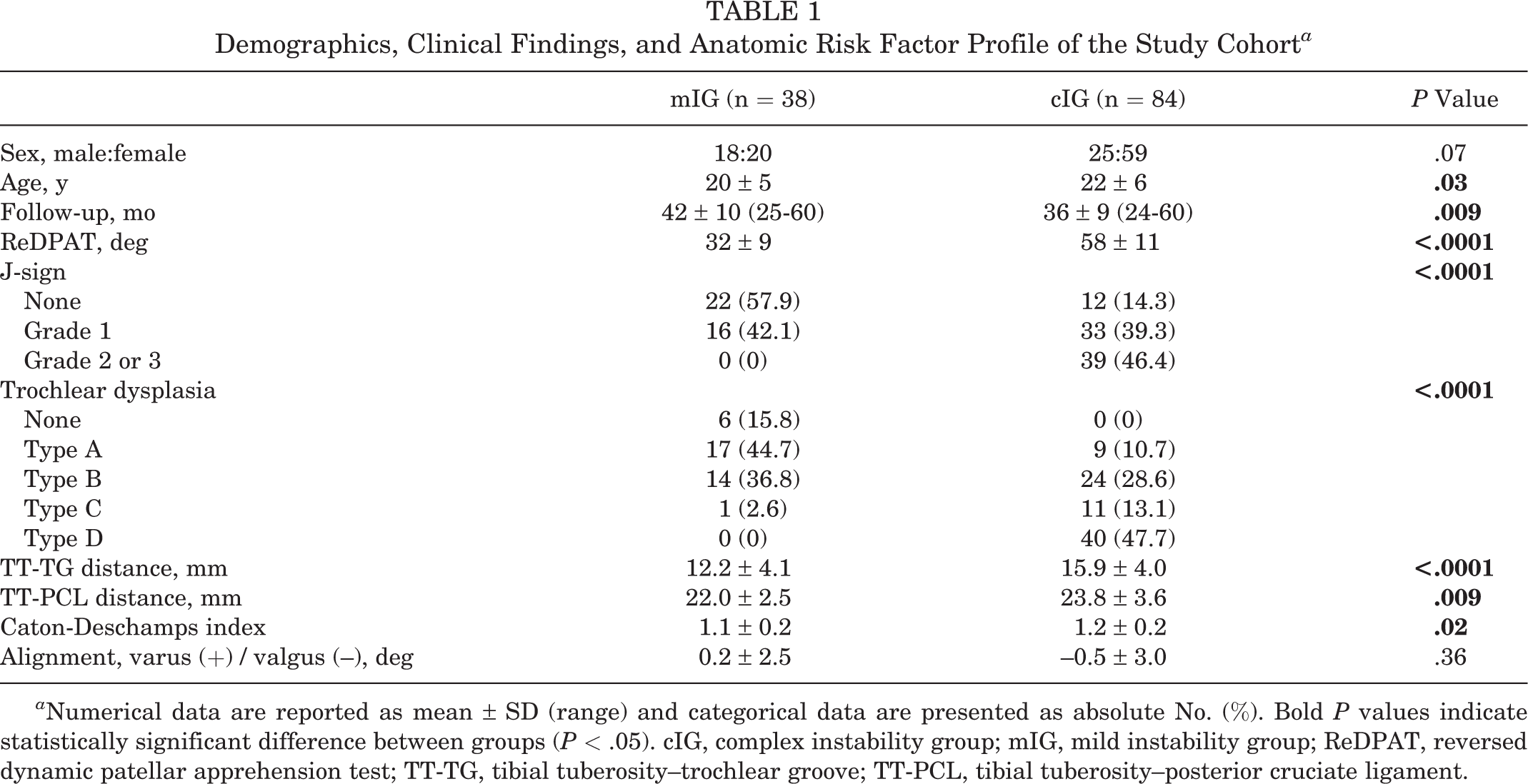
a Numerical data are reported as mean ± SD (range) and categorical data are presented as absolute No. (%). Bold P values indicate statistically significant difference between groups (P < .05). cIG, complex instability group; mIG, mild instability group; ReDPAT, reversed dynamic patellar apprehension test; TT-TG, tibial tuberosity–trochlear groove; TT-PCL, tibial tuberosity–posterior cruciate ligament.
Distribution of Operative Procedures Performed in the Study Groups and Associated Clinical Findings a

a Data are reported as mean ± SD or No. (%). Dashes indicate areas not applicable. cIG, complex instability group; DFO, distal femoral osteotomy; dTrochleoplasty, deepening trochleoplasty; mIG, mild instability group; MPFL-R, medial patellofemoral ligament reconstruction; ReDPAT, reversed dynamic patellar apprehension test; TTO, tibial tubercle osteotomy.
b One patient had an additional dTrochleoplasty, and 1 had an additional TTO.
In the mIG, evaluation was performed 42 ± 10 months postoperatively. The BPII 2.0 score increased from 38.9 ± 20.8 preoperatively to 81.1 ± 17.2 postoperatively (P < .0001). The patellofemoral pain score decreased from 6.4 ± 2.2 to 1.3 ± 1.7 (P < .0001), with concomitant improvement in subjective knee joint function from 4.3 ± 2.5 to 8.8 ± 1.4 (P < .0001).
In the cIG, evaluation was performed 36 ± 9 months postoperatively. The BPII 2.0 score improved from 42.9 ± 19.6 preoperatively to 80.4 ± 19.2 postoperatively (P < .0001). The patellofemoral pain score decreased from 5.6 ± 2.2 to 2.1 ± 2.1 (P < .0001), with improvement in knee joint function from 4.3 ± 2.1 to 8.3 ± 1.5 from pre- to postoperatively (P < .0001).
No difference was found between the mIG and cIG regarding postoperative BPII 2.0 scores (P = .95; power, 0.79; effect size, d = 0.5; alpha error probability, .05) and subjective knee joint function (P = .059; power, 0.69; effect size, d = 0.43; alpha error probability, .05). In addition, in the mIG and cIG, 84% (32/38) and 90% (76/84) of patients respectively achieved the calculated MCID of 9.9 points for the BPII 2.0, without any significant difference between the groups (P = .36).
At final follow-up, no gross patellar redislocation occurred in either group. However, 2 patients in the cIG reported patellar subluxation, and the cIG experienced slightly more postoperative pain than the mIG (1.3 ± 1.6 vs 2.1 ± 2.1; P = .036).
Discussion
The aim of this study was to evaluate a clinically derived 2-group classification of LPI considering the patients’ preoperative J-sign and dynamic patellar instability assessment. The main results indicated the following: (1) the clinical evaluation of patellar instability (ReDPAT) and patellar tracking (J-sign) provides meaningful information to classify LPI into mild and complex forms, and (2) concomitant bony correction in addition to MPFL-R yields encouraging results in complex LPI cases when compared with the results of isolated MPFL-R in mild LPI cases.
As stated by Cregar et al, 9 “the controversy surrounding if and when to address certain risk factors is in large part due to the complex etiology of recurrent instability.” Thus, appropriate treatment of LPI requires a profound understanding of the relevant contributions and interactions of the different patellar stabilizing mechanisms in the context of an individual’s anatomy. 48 Several studies have aimed to identify certain risk factors crucial for patient-reported outcomes and postoperative patellar stability. However, the significance of these risk factors relevantly varies among studies. 9 For example, Erickson et al 13 reported good to excellent outcomes after isolated MPFL-R in a bony pathoanatomy setting. Similarly, Liu et al 27 found no difference in the outcomes after MPFL-R in patients with and without trochlear dysplasia. Yet, Zimmermann et al 47 examined reasons for MPFL-R failure and found that recurrent instability was associated with the prevalence of severe trochlear dysplasia, valgus deformity, and increased patellar height. Likewise, Hopper et al 22 observed recurrent instability in all patients with severe trochlear dysplasia; Zhang et al 46 and Nelitz et al 30 reported inferior outcome scores in patients with increased femoral antetorsion; and Franciozi et al 15 showed that MPFL-R in combination with medialization of the tibial tuberosity at an increased TT-TG distance leads to a better clinical-functional outcome than isolated MPFL-R.
Patellar instability typically presents a constellation of clinical and radiologic parameters, which makes it difficult to weight all of them according to their impact on patellofemoral stability and, in particular, on patient-reported outcome measures. 29 The prevalence of trochlear dysplasia, patella alta, and increased TT-TG distance has been described in 68%, 60%, and 42% of patients, respectively, with 59% identified as having ≥2 abnormal factors. 39 In another study, 48 the prevalence of trochlear dysplasia, patella alta, increased TT-TG or TT-PCL distance, and valgus deformity reached 100%, 49%, 45%, and 22%, with 89% of patients identified as having ≥2 abnormal factors. Given this natural heterogeneity in patients with LPI and inconsistencies in reporting risk factors for MPFL-R failures, many published articles had limited applicability when reporting results after isolated MPFL-R. 9,42 As a synopsis of the available literature, a recent systematic review concluded that more severe trochlear dysplasia and femoral tunnel malpositioning appeared to be the most important parameters affecting postoperative patellofemoral stability and patient-reported outcomes after MPFL-R surgery. 9
Using computational analysis, Fitzpatrick et al 14 quantified the contribution of 4 key factors to patellar constraint (sulcus angle, patella alta, TT-TG distance, and femoral anteversion) and identified the sulcus angle as having the greatest impact. However, classification and interpretation of risk factors, particularly trochlear dysplasia, remains a major challenge. 43 Therefore, recent studies have emphasized the importance of a more clinically derived patellar instability assessment protocol. 8,29,44,45,48 Zimmermann et al 48 introduced the ReDPAT, a test that evaluates the patient-specific end of stable patellar tracking and the beginning of patellar stabilizer insufficiency in an individual patient. Test results correlated with the severity of trochlear dysplasia, valgus deformity, and total number of anatomic risk factors for LPI, indicating that the more factors present, the sooner the patellar instability becomes symptomatic in deeper knee flexion. Most notably, the results became positive at a mean knee flexion angle of 58° (20°-90°). In addition, Colatruglio et al 8 reported that in 90% of patients with significant patella alta and in the majority of patients with high-grade trochlear dysplasia, patellar apprehension persisted beyond 60° of knee flexion; these findings are in line with the results obtained in this study and with biomechanical principles of the patellofemoral joint and might explain why isolated MPFL-R may not be sufficient in certain patients.
Recent studies have highlighted the importance of the J-sign in that they demonstrated that a preoperative high-grade J-sign was associated with inferior clinical outcome scores and increased residual medial patellofemoral ligament graft laxity. 44,45 In addition, the presence of a high-grade J-sign correlated significantly with inferior quality-of-life scores in patients with recurrent LPI. 29 Since patellar maltracking has been associated with trochlear dysplasia, 35 patella alta, 33 increased TT-TG distance, 40 and increased femoral and tibial torsion, 46 it appears reasonable that patients with a preoperative high-grade J-sign yielded inferior clinical results after isolated MPFL-R, 44 as MPFL-R alone is not able to restore patellar kinematics and patellar tracking when anatomic patellofemoral malalignment is present. 12
Using a dynamic computed tomography investigation, Tanaka et al 41 proposed a 3-part classification of lateral patellar translation that has been adopted in clinical studies with good intra- and interobserver reproducibility 29,44,45 and was used for this investigation. However, other authors reported that when using visual assessment alone, surgeons identified patellar maltracking in only two-thirds of cases and correctly graded maltracking in half, 6 indicating that clinical evaluation is less reliable for communication between physicians. 21 Nevertheless, as long as it remains difficult to isolate individual factors that decisively influence postoperative results after MPFL-R, the J-sign presents an important clinical parameter reflecting the overall picture of an individual’s patellar tracking or maltracking probably better than can be expressed by the simple addition of anatomic risk factors depending on whether they exceed a given threshold. 29 In particular, it is likely that a risk factor on its upper limit influences overall patellar tracking in the orchestra of patellofemoral alignment parameters, although it is not formally added to the individual risk factor profile. 29 To overcome these drawbacks, further development of computed tomography and/or MRI to dynamically assess patellar tracking 17,41 is highly warranted but awaits widespread implementation in clinical practice.
Considering the current literature, it seems likely that at least some of the known pathoanatomic risk factors for LPI (ie, severe trochlear dysplasia) affect patellofemoral stability and patient-reported outcomes after patellar stabilizing surgery. Currently, the literature lacks the reverse conclusion that in those patients, the correction of modifiable risk factors leads to equivalent good results as for isolated MPFL-R in patients with mild forms of LPI. The findings of this study support the concept of restoring patellofemoral alignment in patients with a high-grade J-sign and/or patellar instability beyond 40° to 50° of knee flexion and thus might be considered a step forward. However, the higher level of postoperative pain gives us cause for concern, and the results need to be interpreted under consideration of the weaknesses of this study.
Limitations
First, the cIG underwent a consequent correction of bony malalignment, and although the results were encouraging, we cannot exclude the possibility that at least some patients would have achieved similar results with isolated MPFL-R. This answer is reserved for prospective randomized controlled trials, which, however, are difficult to realize owing to the aforementioned natural heterogeneity of the patient population with LPI. In this regard, this study first used a clinically derived classification of patellar instability for treatment decision making. The reliability of this classification, though, requires further independent verification. Second, we noted statistically significant differences between the mIG and cIG in age (20 ± 5 vs 22 ± 6 years) and follow-up time (42 ± 10 vs 36 ± 9 months). Yet, we do not consider that this difference introduced a relevant bias to the clinical results. Third, the postoperative evaluation was performed using a disease-specific quality-of-life questionnaire (BPII 2.0) and numeric analog scale to evaluate pain and knee joint function. The results were not correlated with objective clinical findings, functional performance, imaging, or another outcome score. In addition, distribution-based MCID values for the BPII 2.0 in this study exceeded those of previous investigations. 25 Nevertheless, the multitude of MCID calculation methods can lead to a range of values, which limits their transferability among studies. 23 Finally, the limitations and potential bias characteristics of a retrospective study need to be considered.
Conclusion
The results of this study indicate the following: (1) patients with a high-grade J-sign and/or a positive ReDPAT beyond 40° to 50° of knee joint flexion exhibited a significantly more pronounced pathoanatomic risk factor constellation, and (2) in these patients, the correction of modifiable risk factors led to similarly good results as for isolated MPFL-R in patients with mild forms of LPI considering the BPII 2.0 and subjective assessment of knee joint function. Although postoperative pain significantly improved, a slightly higher level after bony procedures was evident.
Footnotes
Final revision submitted September 12, 2022; accepted October 21, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee of Baden-Württemberg (No. F-2019-070).