
Abstract
Background:
Ischemic preconditioning (IPC) involves brief periods of circulatory occlusion and reperfusion to stimulate protective effects on tissues. Studies on IPC prior to knee surgery have shown improvements in postoperative pain and decreased opioid consumption. Through a combination of neural and circulating humoral factors, IPC has also been shown to have systemic effects outside the area of ischemia.
Purpose:
To determine whether preoperative IPC of the operative limb at the thigh affects postoperative pain scores or opioid consumption after hip arthroscopy.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
Adult patients undergoing hip arthroscopy for femoroacetabular impingement or labral tear were prospectively enrolled and randomized to IPC or control groups. Limb preconditioning was performed within 24 hours before surgery using the Delphi Personalized Tourniquet System with the cuff on the proximal thigh. The IPC group received a 30-minute treatment consisting of 3 rounds of 5 minutes at limb occlusion pressure alternating with 5 minutes of reperfusion. The control group received the same protocol at 20% of limb occlusion pressure. Arthroscopy was performed according to standard of care. Surveys were administered through RedCap starting the day of surgery through postoperative day 7. Patients were asked to rate their pain from 0 to 10 with the visual analog scale (VAS) and to record use of pain medication. Statistical analysis included chi-square and t tests.
Results:
A total of 68 patients (34 IPC, 34 control) were enrolled. Demographic characteristics and specific surgical procedures were similar between groups. Survey compliance was higher in the IPC group than the control group, 6.3 ± 2.7 days versus 3.7 ± 3.38 days, respectively (P < .05). Both groups reported significant reductions in their VAS pain scores from the day of surgery to postoperative day 7 (P < .05). No significant difference was found between the groups in VAS pain scores at any time point. No significant difference was found between the groups in mean daily opioid consumption (expressed as morphine milligram equivalents) or acetaminophen consumption.
Conclusion:
IPC of the operative limb at the thigh did not appear to decrease pain scores or pain medication use after hip arthroscopy. This study suggests that although IPC of the limb at the level of the thigh may be useful for some orthopaedic procedures, it may not have a significantly beneficial effect for hip arthroscopy patients.
Registration:
NCT04925791 (ClinicalTrials.gov identifier).
Optimizing pain control after hip arthroscopy has received a lot of recent attention, 26 especially in the setting of the global push to decrease opioid use. 13 In a recent survey among international hip arthroscopy surgeons, 15% of those surveyed reported that they have had to admit a patient to the hospital due to lack of pain control. 6 Many surgeons use a multimodal approach to pain control including oral medication, peripheral nerve blocks, local anesthetics, and local anesthetic infiltration, although this approach is not standardized.7,10,13,14,26,28,29 Reasons some patients may have uncontrolled pain despite a multimodal regimen include differences in individual pain tolerances, compliance to the medication regimen, and variation of patient sensitivity to the administered medication. Identifying effective nonpharmacologic pain control interventions after hip arthroscopy would be of significant benefit to surgeons and their patients.
Ischemic preconditioning (IPC) is a technique involving the exposure of brief periods of circulatory occlusion followed by reperfusion. It was initially developed as a technique to protect myocardium from ischemic injury during elective cardiac surgery.8,9,18,22,27 It was later shown to protect against ischemic reperfusion injury in skeletal muscle.1,21 IPC is defined as a brief episode of ischemia that initiates a response that protects organs from sustained ischemic events, and it has the potential to attenuate ischemic/reperfusion effect of the surgical insult. 30 IPC may be remote (stimulus is applied to a distant organ or tissue, which then protects against index ischemia) or local (stimulus is applied to the same organ or tissue that will subsequently sustain the ischemic injury). The mechanism is not well understood but is thought to be a combination of neural and circulating humoral factors. 25
In the orthopaedic literature, IPC has been investigated as a potential pain control intervention. In a study of patients undergoing total knee arthroplasty, Memtsoudis et al 16 found that 5 minutes of tourniquet inflation before extended tourniquet use during surgery resulted in lower postoperative pain scores. In a follow-up randomized study, Memtsoudis et al 15 found that IPC resulted in lower pain scores 1 to 2 days postoperatively. The mechanism of why IPC may modulate pain is not well understood, but it is thought that IPC may modulate sensitivity to a painful stimulus. 28
The purpose of this study was to determine whether preoperative IPC of the operative limb would decrease postoperative pain scores or opioid consumption after hip arthroscopy.
Methods
This study was a prospective, single-blind, randomized controlled trial that took place at the Cedars Sinai Kerlan Jobe Institute and was approved by the Cedars Sinai institutional review board. This study was registered on ClinicalTrials.gov (NCT04925791). Patients were enrolled between October 2021 and December 2023. Inclusion criteria were patients 18 years or older undergoing hip arthroscopy by a single surgeon for femoroacetabular impingement or labral tear. Exclusion criteria were age younger than 18 years and history of clotting disorder or venous thromboembolism. Patients were prospectively enrolled and randomized to 1 of 2 groups using the National Institutes of Health randomization tool: IPC group (received IPC before hip arthroscopy) or control group (did not receive IPC before hip arthroscopy).
Patients were screened and enrolled for study participation during routine preoperative visits. A flow diagram of patient recruitment is included in Figure 1. Limb preconditioning was performed within 24 hours before surgery using the Delphi Personalized Tourniquet System (PTS) with the cuff on the proximal thigh of the operative limb. Limb preconditioning was applied and supervised by an athletic trainer or an orthopaedic fellow. The protocol for limb preconditioning was adapted from Da Silva et al, 3 who investigated the effects of IPC on athletic performance. The IPC group received a 30-minute treatment consisting of 3 rounds of 5 minutes at limb occlusion pressure (LOP) alternating with 5 minutes of reperfusion. The control group received the same protocol at 20% of LOP (which does not occlude blood flow to the limb). LOP was patient specific, calculated, and automatically regulated using the Delphi PTS. A schematic of the limb preconditioning protocol is shown in Figure 2.
Flow diagram of patient recruitment.

Schematic of the limb preconditioning protocol used for the ischemic preconditioning (IPC) and control groups. LOP, limb occlusion pressure.
Surveys were administered through RedCap starting the day of surgery and continuing through postoperative day 7. Patients were asked to rate their pain from 0 to 10 using a visual analog scale (VAS) averaged over the previous 24 hours. They were also asked to record pain medication use (prescribed medications and acetaminophen), including the name of the medication and the dose. Narcotic dosing was converted into morphine milligram equivalents according to previously published conversion factors. 4 Data collection included review of charts for baseline characteristics and demographics including age, sex, and body mass index. Also recorded were surgical procedures performed during hip arthroscopy, Outerbridge grading of chondromalacia if present, 20 and whether there were any early postoperative complications (within first 7 days postoperatively).
Arthroscopy was performed by a single sports fellowship–trained surgeon (M.B.) according to standard of care. Patients were placed supine on a postless hip distractor table. Arthroscopy was then performed using a standard anterolateral portal, a modified anterior portal, and a distal anterolateral accessory portal. Interportal or T capsulotomies were then used to complete intra-articular work. After diagnostic arthroscopy, procedures were performed as indicated, including labral debridement, labral repair, labral reconstruction, acetabuloplasty, femoral osteochondroplasty, chondroplasty, subspine decompression, acetabular biocartilage implantation, capsular plication, excision of heterotopic ossification, and trochanteric bursectomy. Patients received a standardized preoperative and postoperative pain regimen, including preoperative blocks of the hip pericapsular nerve group, 5 preoperative acetaminophen (1000 mg), preoperative celecoxib (200 mg), preoperative gabapentin (300 mg), postoperative tramadol (50-100 mg every 4-6 hours as needed for pain) or oxycodone (5-10 mg every 4-6 hours as needed for pain), postoperative naproxen (500 mg twice daily), and postoperative over-the-counter acetaminophen as needed.
Statistical Analysis
An a priori power analysis was used to determine the required sample size for the study. For a 2-sided t test of independent means with an alpha value of .05, a power of .80, a large effect size (0.70), and a 1:1 allocation ratio of patients, a sample size of 68 (34 patients per group) was determined to be required for this study. Statistical analysis was performed using Microsoft Excel. Patient characteristics and procedure details were compared between IPC and control groups using independent t tests and chi-square analysis for continuous and categorical variables, respectively. Independent t tests were used to compare postoperative VAS scores at each time point. Independent t tests were also used to compare pain medication use (narcotic use expressed as morphine milligram equivalents as well as acetaminophen consumption in milligrams) at each time point. Paired t tests were used to compare VAS scores within the groups.
Results
The study enrolled 68 patients (34 patients in the IPC group and 34 patients in the control group). Demographic characteristics and specific surgical procedures were similar between groups (Table 1). Mean age was 30.6 ± 9.7 years in the IPC group and 28.2 ± 8.2 years in the control group. Regarding sex distribution, 50% (17 patients) of patients in the IPC group were male compared with 47% (16 patients) in the control group. Survey compliance was higher in the IPC group than the control group, 6.3 ± 2.7 days versus 3.7 ± 3.38 days, respectively (P < .05). Surgical procedures performed during hip arthroscopy were similar between the groups.
Demographics, Baseline Patient Characteristics, and Surgical Procedures Performed a

Values are expressed as % (n) or mean ± SD. Boldface indicates statistical significance. IPC, ischemic preconditioning.
Both groups reported significant reductions in their VAS pain scores from the day of surgery to postoperative day 7. The IPC group improved from a mean of 4.92 to 2.04 and the control group improved from a mean of 4.92 to 2.75 (P < .05). No significant differences were noted between the groups in VAS pain scores at any time point from the day of surgery to postoperative day 7 (Table 2; Figure 3). No significant difference was found between the groups in mean daily opioid consumption (expressed as morphine milligram equivalents) from the day of surgery to postoperative day 7 (Table 3; Figure 4). We found no significant differences in acetaminophen consumption.
Visual Analog Scale Scores for the IPC and Control Groups From the Day of Surgery to Postoperative Day 7 a

Data are expressed as mean ± SD (n). IPC, ischemic preconditioning; POD, postoperative day.

Line graph illustrating mean visual analog scale (VAS) pain scores for the ischemic preconditioning (IPC) and control groups with standard error bars. POD, postoperative day.
Narcotic Pain Medication Use in Morphine Milligram Equivalents for IPC and Control Groups From the Day of Surgery to Postoperative Day 7 a

Data are expressed as mean ± SD (n). IPC, ischemic preconditioning; POD, postoperative day.
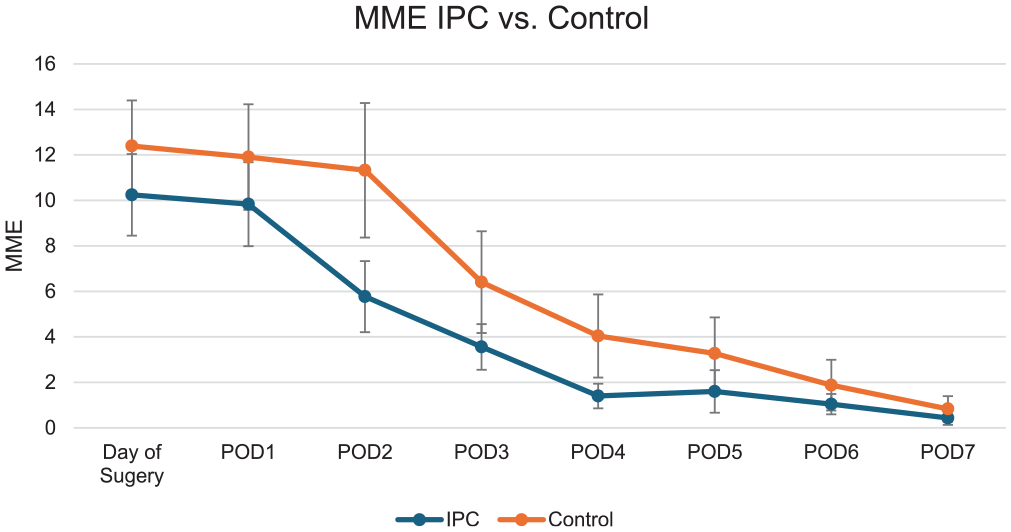
Line graph illustrating mean opioid consumption for the ischemic preconditioning (IPC) and control groups with standard error bars. MME, morphine milligram equivalents; POD, postoperative day.
Discussion
This study showed that IPC of the operative limb before hip arthroscopy did not significantly decrease pain (measured by VAS score) or pain medication use in the first 7 days postoperatively.
The first study investigating orthopaedic applications of IPC for pain control after surgery was conducted in 2006 by Orban et al, 19 who compared a group of patients undergoing knee ligamentoplasty without IPC to a group who received IPC. In this study, IPC involved inflation of the tourniquet for 5 minutes, followed by deflation of the tourniquet for 10 minutes before prolonged inflation of the tourniquet for the surgical procedure. The investigators found that postoperative morphine consumption was lower in the group that received IPC than in the control group. Groups in this study were small, 10 or 11 patients. Another study that investigated the use of IPC before knee surgery was published by Memtsoudis et al, 16 who found that IPC before total knee arthroplasty did not significantly affect the levels of circulating inflammatory factors after surgery. Those investigators also found that the IPC group had lower median pain scores and shorter length of stay postoperatively. In a follow-up study, Memtsoudis et al 15 completed a randomized controlled trial looking at the effect of IPC on pain after knee arthroplasty, and they found lower pain scores in the IPC group at rest and during exercise. The investigators reported modest differences in pain scores and no difference in analgesic consumption, length of hospitalization, and time to various physical therapy milestones.
Given promising reports in the literature for the use of IPC to improve pain control after knee surgery, the current study was performed to investigate the effect of IPC after hip arthroscopy. No significant differences in pain scores or analgesic consumption were found between the groups in the first 7 days postoperatively. Several factors should be considered in interpreting these findings. It is possible that the current multimodal pain regimen may be adequately effective and masking a benefit of IPC. It is also possible that the level of pain after hip arthroscopy may be too low for the benefit of IPC to be detectable. Few studies have published early postoperative pain scores after hip arthroscopy. Cunningham et al 2 published an observational study with mean pain scores from postoperative day 1 to postoperative day 14. They found that at postoperative day 1, mean pain score was between 4 and 5. By day 7, mean pain scores had decreased to between 3 and 4. In our study, both the IPC and control groups had similar mean pain scores on postoperative day 1: 4.7 and 4.2, respectively. By day 7, mean pain scores were lower than in the study by Cunninham et al: 2 in the IPC group and 2.8 in the control group. Ramos et al 23 reported pain medication use after hip arthroscopy. They also reported results in morphine equivalent dosages, reporting a mean of 27.3 on postoperative day 1, 22.3 on postoperative day 4, and 8.5 on postoperative day 9. In the current study, both the IPC and control groups reported lower morphine equivalent dosages than Ramos et al 23 at day 1 and day 4. This finding may be attributed to differences in pain control regimen, differences in patient population, or inaccurate reporting of pain medication use on the surveys. In the current study, no significant difference was noted in pain medication use between the IPC and control group at any time point. We found a trend toward less narcotic use in the IPC group at postoperative days 2 and 3, but this difference did not reach statistical significance (P values .08 and .09, respectively). To put this in perspective, at day 3 there was a difference of 5.5 morphine milligram equivalents between the groups. This is equivalent to one 50-mg tramadol tablet. It must be considered whether a difference of 1 tablet per day is enough to justify IPC as a preoperative intervention, given that the protocol requires the purchase of and access to a specialized machine and necessitates trained personnel to supervise the treatment, which takes approximately 30 minutes.
Another factor to consider in interpreting the findings of this study is that IPC may not provide a pain control benefit when the surgical site is proximal to the site of occlusion. Although previous studies have investigated IPC in the setting of knee surgery (operative site distal to level of occlusion), systemic effects and circulating factors from IPC have been proposed. This may provide benefit to tissues proximal to the site of occlusion, which was investigated in this study (where the surgical site was the hip and the level of occlusion was the]thigh). Additionally, portions of several muscles that cross the hip joint are included distal to the site of occlusion (sartorius, rectus), suggesting there may be some local effects. The remote effects of IPC have been explored in the cardiac literature, where IPC of a limb is used to help protect myocardium against ischemic reperfusion injury.8,9,27 The mechanism of this effect, although not well understood, is thought to include both circulating humoral mediators and neural pathways. 25 Additional proposed local effects of IPC include vasodilation, improved oxygen delivery to tissue, increased efficiency of metabolism, reduction in production of lactate during exercise, and changes in fatigue pereption. 25
The effects of IPC on pain sensitivity are of more interest to the orthopaedic surgeon. Although the exact mechanisms that contribute to pain receptor modulation in IPC are incompletely understood, some studies have suggested that IPC may modulate sensitivity to a painful stimulus. Slysz and Burr 28 performed cold water immersion tests on participants before and after receiving IPC. The investigators found that after IPC, participants reported less time spent in pain during the cold water immersion test. Additional evidence has implicated an important role of opioids as an endogenous substance released by preconditioned tissue.11,12 Therefore, the local release of endogenous opioids may alter pain receptor sensitivity. 12 Additionally, from a physiologic standpoint, IPC has been shown to induce a protective genomic response, which results in increased expression of immediate early response genes, oxidative stress defense genes, and prosurvival genes.17,24 The connection between this oxidative protective genomic response and pain modulation pathway has not been clearly established.
The current study has several limitations. The site of occlusion in the thigh was distal to the surgical site, which may limit the local effects of IPC in this setting. We noted a wide variation in survey compliance, and the IPC group completed significantly more surveys than the control group, 6.3 ± 2.7 days versus 3.7 ± 3.38 days, respectively. It is possible that this difference is related to difficulties with blinding. Although patients were blinded to their treatment groups, treatment was performed preoperatively with the patients awake. Because the control group had cuffs inflated to only 20% of LOP, it may have been possible for them to assume that they were in the control group. This may have affected their motivation to comply with surveys. Due to attrition, the study may not be adequately powered later in the postoperative interval. Also, patients were asked to provide 1 VAS score to illustrate pain for the previous 24 hours. However, pain levels likely fluctuate significantly over that time period. Finally, pain medication calculations relied on accurate patient reporting on the surveys, and pill counting by study staff was not part of this study.
Conclusion
IPC of the operative limb at the thigh did not appear to decrease pain scores or pain medication use after hip arthroscopy. Although IPC may be useful for some orthopaedic procedures, this study suggests that it may not have a significantly beneficial effect for hip arthroscopy patients.
Footnotes
Final revision submitted January 13, 2025; accepted February 24, 2025.
Presented as a poster at the annual meeting of the AOSSM, Denver, Colorado, July 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.O. has received support for education from Smith & Nephew and Saxum Surgical, hospitality payments from Arthrex and EnduroMed, and a grant from Arthrex. A.U. has received support for education from Micromed, Smith & Nephew, United Orthopedics, Medical Device Business Services, and Kairos Surgical and a grant from Arthrex and Medical Device Business Services. M.B. has received honoraria from Verical Corporation; support for education from Arthrex, Saxum Surgical, and Micromed; and consulting fees from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Cedars Sinai institutional review board (STUDY00001182).