
Abstract
Background:
Hip microinstability is an increasingly recognized cause of pain and disability in young adults. It is unknown whether differences in passive hip range of motion (ROM) exist between patients with versus without hip microinstability.
Hypothesis:
Underlying ligamentous and capsular laxity will result in differences in clinically detectable passive ROM between patients with femoroacetabular impingement (FAI), patients with microinstability, and asymptomatic controls.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective review of all patients undergoing hip arthroscopy between 2012 and 2018 was conducted. Patients with a diagnosis of isolated microinstability based on intraoperative findings were identified and classified as having isolated FAI, instability, or FAI + instability. Patients without a history of hip injury were included as controls. Range of motion was recorded in the supine position for flexion, internal rotation, and external rotation. Univariate and multivariate analysis was performed on each measurement in isolation as well as combinations of motion to include total rotation arc, flexion + rotation arc, and flexion + 2× rotation arc Models were then created and tested to predict instability status.
Results:
In total, 263 hips were included: 69 with isolated instability, 50 with FAI, 50 with FAI + instability, and 94 control hips. A higher proportion of patients in the instability and FAI + instability groups were female compared with the FAI and control groups (P < .001). On univariate analysis, differences were found in all groups in all planes of motion (P < .001). Multivariable analysis demonstrated differences in all groups in flexion and flexion + rotation arc. In symptomatic patients, the best performing predictive model for hip microinstability was flexion + rotation arc ≥200° (Akaike information criterion, 132.3; P < .001) with a sensitivity of 68.9%, specificity of 80.0%, positive predictive value of 89.1%, and negative predictive value of 51.9%.
Conclusion:
Patients with hip microinstability had significantly greater ROM than symptomatic and asymptomatic cohorts without hip microinstability. Symptomatic patients with hip flexion + rotation arc ≥200° were highly likely to have positive intraoperative findings for hip microinstability, whereas instability status was difficult to predict in patients with a flexion + rotation arc of <200°.
Hip microinstability is increasingly recognized as a cause of pain and disability in young adults, although the diagnosis remains controversial. 2,4,15,19,22,23,25 Defined as extraphysiologic motion resulting in pain with or without hip joint unsteadiness, 4,27 hip instability is theorized to result from a combination of pathoanatomic factors. These risk factors include lack of adequate bony support (hip dysplasia), weakness of the periarticular hip muscular stabilizers, disruption of the labral suction seal, and ligamentous or capsular laxity/deficiency. 8 Additionally, although hip microinstability is increasingly described, no gold standard is available for diagnosis. 15,25 Currently, a combination of preoperative factors (history of giving way, soft tissue laxity on physical examination) and intraoperative factors (ease of hip distraction, ligamentum teres pathology, and the location of pathologic chondral and labral findings) have been proposed as the leading diagnostic criteria. 7,20,22,25,29 However, many of these are intraoperative findings, such that surgical intervention is required to confirm the diagnosis. Thus, further identification and validation of preoperative findings would be paramount in both recognizing and appropriately treating this unique cohort.
Multiple biomechanical studies have demonstrated that capsular deficiency or laxity, particularly anterior to the iliofemoral ligament, results in increased hip range of motion (ROM). 1,8,13 Furthermore, increased hip ROM has been associated with various degrees of hip dysplasia 17 as well as underlying generalized ligamentous laxity. 24 Specifically, elite ballet dancers have been shown to demonstrate excessive ROM, resulting in asymptomatic femoral head translation and/or subluxation, as well as labral and chondral compression. 3,9,18 Although excessive ROM has been associated with hip microinstability, to our knowledge, no investigation has focused on using this physical examination finding to aid in diagnosis of hip microinstability. This finding may allow for better preoperative discernment between patients with and without instability, especially in the setting of concomitant femoroacetabular impingement (FAI).
In this study, we aimed to determine whether hip ROM would differ among 4 groups: an asymptomatic cohort, patients with FAI, patients with FAI plus intraoperative findings consistent with instability, and patients with isolated hip microinstability. A secondary goal of the current study was to create a simple clinical tool to help surgeons predict a patient’s risk of intraoperatively diagnosed hip instability. Our hypothesis was that hip ROM would be significantly greater in patients with intraoperatively diagnosed hip instability relative to FAI patients and an asymptomatic control group and that hip ROM may be able to assist in the preoperative diagnosis of hip instability.
Methods
Study Groups
This study was reviewed and approved by the institutional review board at our university. A retrospective review of patients who underwent hip arthroscopy with the senior surgeon (M.R.S.) between 2012 and 2018 was conducted to identify pre- and postoperative diagnoses. We identified 69 patients with isolated hip microinstability (without bony FAI morphology) based on previously published intraoperative criteria (ease of hip distraction, residual hip subluxation after release of traction, straight anterior or lateral chondral and labral pathology). 4,6,7,14,15,22,26
The force required for hip distraction was measured based on a consistent and standardized method, recorded as the number of turns of traction (1 turn = 4 mm of axial traction) to obtain 10 mm of hip distraction, as has been previously reported. 6 The initial state was obtained by placing the patient firmly against a perineal post with body weight traction applied by the senior surgeon as previously described. 5,6 A diagnosis of hip microinstability was made based on ≤11 turns (≤44 mm of traction). 25 We also identified a consecutive series of 50 patients with isolated FAI (no intraoperative findings of hip microinstability) and FAI with a concomitant diagnosis of instability. Study inclusion criteria were patients aged 17 to 50 years undergoing primary hip arthroscopy with documented physical examination and imaging findings. The diagnosis of cam-type FAI was based on an alpha angle >55°. The diagnosis of pincer-type FAI was defined by a radiographic crossover sign and/or a lateral center-edge angle (LCEA) >35°. Mixed-type FAI was defined by meeting definitions of both cam-type and pincer-type FAI. Exclusion criteria were revision cases, hip dysplasia (LCEA <18°), or patients treated with hip arthroscopy for an alternative diagnosis (synovial chondromatosis, pigmented villonodular synovitis, etc).
Patient charts were reviewed, and hip ROM (flexion, internal rotation, and external rotation measured in the supine position) was recorded by visual estimation by the senior author (M.R.S.). ROM was recorded in the supine position with maximum hip flexion being recorded with the knee flexed. Internal and external rotation were recorded in the supine position with the hip and knee flexed to 90°. Prior research has shown good agreement between visual estimation and goniometry for hip ROM. 10,11
Control Group
Separately, based on an a priori power analysis, 47 individuals with 94 asymptomatic hips were recruited as a control group. This sample size would provide ≥80% power to detect a medium effect size (Cohen d = 0.5) difference in ROM measures. This number adjusts for pairwise comparisons among all diagnosis groups. These patients were recruited through sports preparticipation physical examinations or among patients seen at our clinic with upper extremity complaints. Patients were included if their age was 17 to 50 years and they had no history of hip pain or prior lower extremity fracture, major injury, or surgery. Because these data were collected prospectively and by >1 individual, hip ROM, including flexion and internal and external rotation, was recorded using a digital goniometer to ensure accuracy and consistency. Assessment of flexion was performed in the supine position and rotation was measured in the prone position with the hip in neutral flexion-extension. Radiographs were not obtained within the control group.
Statistical Analysis
Baseline demographic characteristics were collected and analyzed for each group. Univariate and multivariable analyses were performed to evaluate for differences between the 4 groups. Models were then created using a variety of isolated measurements and combinations of measurements (flexion, total rotation arc, flexion + rotation arc, flexion + 2× rotation arc). This analysis was performed excluding the asymptomatic control group because the laxity status of these patients was unknown. Each model was assessed using area under the curve, the Youden index, and the Akaike information criterion (AIC). The AIC was used to estimate model prediction error, with lower values indicating more optimal model performance. The optimal model was then identified, and the sensitivity, specificity, and negative and positive predictive values (NPV and PPV, respectively) were calculated. Additionally, models were created for specific demographic characteristics (males aged ≤30 years, males aged >30 years, females aged ≤30 years, females aged >30 years) to be used as clinical prediction tools. All analyses were completed in RStudio Version 1.1.456 using a level of significance of .05.
Results
In total, 263 hips were included in the initial analysis, with the majority being female (n = 173; 66%). The median age was 27.8 years (interquartile range, 20.5-35.9 years). No significant differences were found between the groups in age (P = .103). However, both instability groups had a higher proportion of female patients than the FAI and asymptomatic control group (P < .001) (Table 1).
Characteristics of the Study Population Overall and by Group a
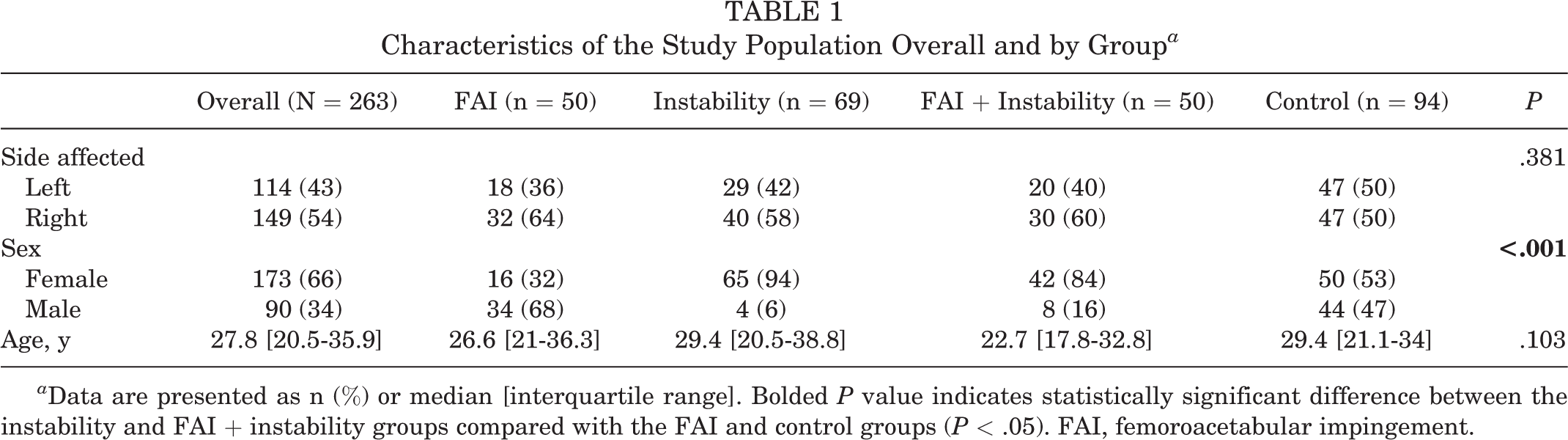
a Data are presented as n (%) or median [interquartile range]. Bolded P value indicates statistically significant difference between the instability and FAI + instability groups compared with the FAI and control groups (P < .05). FAI, femoroacetabular impingement.
In univariate analysis, significant differences were seen between all groups for flexion, internal rotation, external rotation, total rotation arc, flexion + rotation arc, and flexion + 2× rotation arc (P < .001 for all) (Figure 1).

Individual planes of motion and combinations of motion (eg, flexion + rotation arc) by diagnosis with significant differences between all planes of motion on univariate analysis. FAI, femoroacetabular impingement.
The results of the multivariable analysis after controlling for age and sex are shown in Table 2. With the FAI group serving as the baseline, significant differences were found between all groups in flexion and flexion + rotation arc (P < .05). In the flexion + 2× rotation arc measurement, no statistically significant difference was seen between the FAI group and the control group. In internal rotation, there was no significant difference between the FAI and FAI + instability groups, whereas total rotation arc showed significant differences only between the FAI and isolated instability groups. In external rotation, significant differences were found only between the FAI group and the asymptomatic control group.
Multivariable Analysis of Each Range of Motion Plane With FAI Group Used as Reference a

a Bolded P values indicate statistically significant values (P < .05). FAI, femoroacetabular impingement.
Models were then created using the instability, instability + FAI, and FAI groups (Table 3). After assessment of each model, flexion + rotation arc with a cutoff of 200° was found to have the best performance (AIC, 132.3) with the odds of instability being 7 times higher for patients above this cutoff compared with patients below (P < .001) (Figure 2). The sensitivity of this model was 68.9% and specificity was 80.0%, with PPV of 89.1% and NPV of 51.9%.
Evaluation of Each Microinstability Clinical Prediction Model Performance a
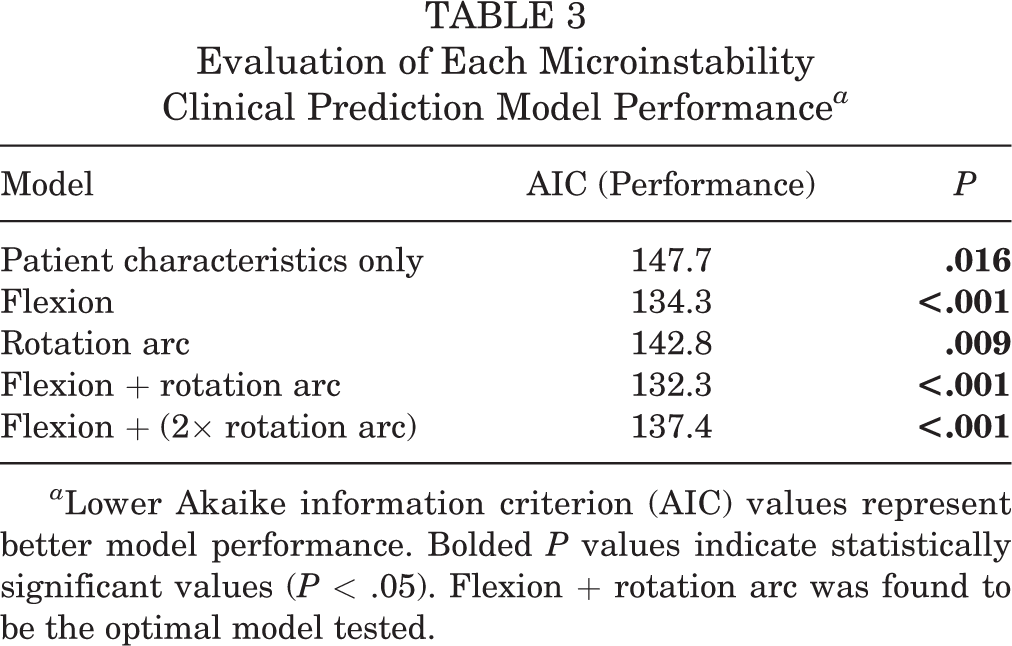
a Lower Akaike information criterion (AIC) values represent better model performance. Bolded P values indicate statistically significant values (P < .05). Flexion + rotation arc was found to be the optimal model tested.
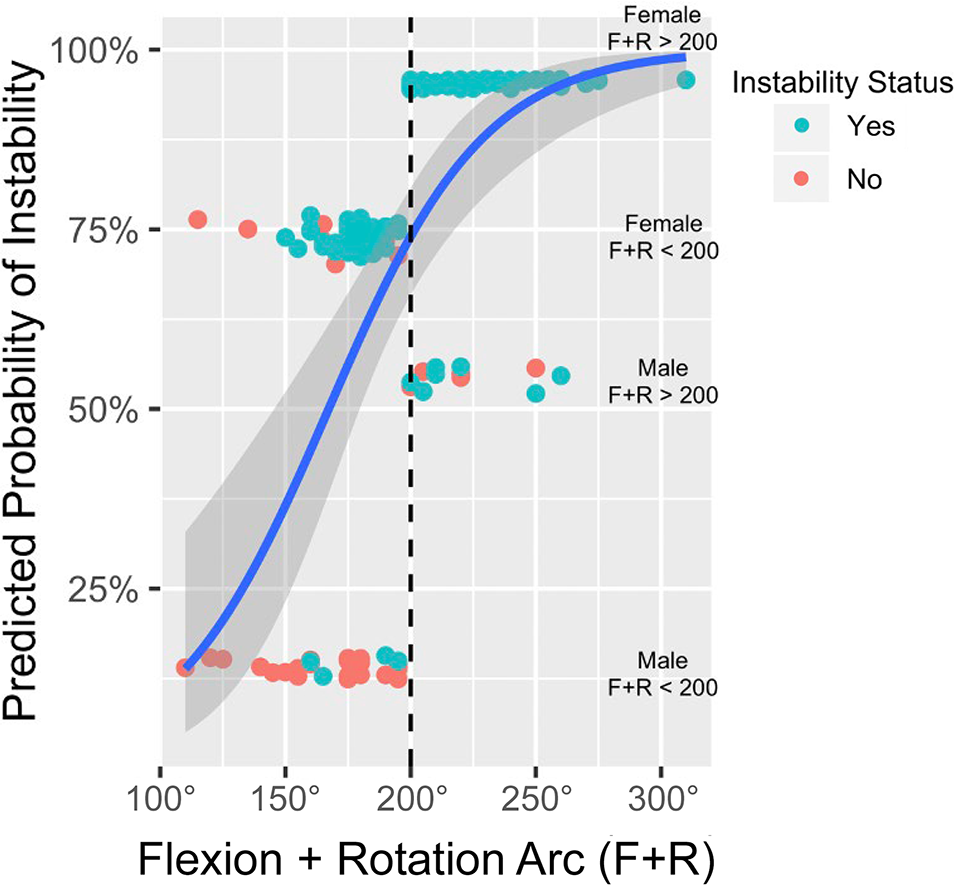
Graphic representation of the optimal clinical prediction model for instability: flexion + rotation arc of ≥200°. On the vertical axis, patients are stratified based on age and sex, with the likelihood of instability demonstrated. Female patients above the 200° threshold (dashed line) are represented by the top group, followed by female patients below the threshold, male patients above the threshold, and male patients below the threshold.
Regarding specific demographic scenarios, the optimal cutoff for female patients ≤30 years old (n = 86) was a flexion angle of 112.5° (PPV = 93.0%; NPV = 36.4%); for female patients >30 years old (n = 76), it was a flexion + rotation arc of 202.5° (PPV = 100%; NPV = 23.3%). For male patients ≤30 years old (n = 55), the optimal prediction tool was a flexion + rotation arc of 185° (PPV = 46.7%; NPV = 93.8%), whereas in male patients >30 years old (n = 30), the cutoff was 200° (PPV = 100%; NPV = 90.9%), 16 of the patients were missing ages so they were not categorized into one of the four age/sex groups.
Discussion
The results of this study demonstrate that there are differences in clinically detectable ranges of motion between patients with instability, patients with FAI, and an asymptomatic control group. In most planes (flexion, internal rotation, total rotation arc, flexion + rotation arc, and flexion + 2× rotation arc), patients with instability had greater ROM than patients with FAI or asymptomatic controls. This was true in univariate and multivariable analyses, controlling for age and male versus female sex.
Few studies have assessed ROM in relation to the intraoperative diagnosis in hip arthroscopy patients. Philippon et al 21 reported the clinical presentation of patients with FAI, demonstrating a mean hip flexion angle of 111°, internal rotation of 31°, and external rotation of 38°—all reduced relative to the contralateral hip. Mean hip flexion was consistent with our results in FAI patients, whereas we found slight differences in rotation with less internal and more external rotation in our study. . Our study used an asymptomatic control group for comparison rather than the contralateral hip given the high prevalence of similar anatomy in patients as well as the relative frequency of bilateral symptoms in patients with FAI. 16 In patients with generalized ligamentous laxity, Saadat et al 24 found increased flexion, internal rotation, and external rotation values as Beighton score increased. Similarly, Matsuda et al 17 demonstrated an association between the presence and severity of dysplasia, as well as the presence of a cam lesion, with hip internal and external rotation. Although generalized ligamentous laxity and borderline hip dysplasia are not synonymous with a diagnosis of microinstability, they are proposed risk factors and significant overlap likely exists.
Physical examination tests have been previously described for hip microinstability, including the abduction–hyperextension–external rotation (AB-HEER) test, the prone external rotation instability test, and the hyperextension–external rotation test. 14 Hoppe et al 12 demonstrated that the AB-HEER test was most accurate, with a sensitivity of 80.6% and specificity of 89.4%. The combination of positive examination findings on all 3 tests demonstrated a high PPV of 95.0%. Similar to our results, all tests had high PPV with moderate NPV. O’Neill et al 20 reported the axial distraction test as a physical examination maneuver in their series of iatrogenic instability cases, finding that 77% of patients had either pain, toggling, or apprehension. No studies have investigated the combination of these examination maneuvers and ROM in predicting the intraoperative diagnosis of hip microinstability.
This study is unique in that we used groups of patients with isolated instability, instability with FAI, and isolated FAI morphology to assess for differences in ROM in patients with symptomatic hips. We also used an asymptomatic control group to potentially identify normative values allowing for the variability of asymptomatic laxity in the native population. Through this analysis, we attempted to provide a simple, prospective clinical tool for predicting a patient’s risk of hip instability: hip flexion + rotation arc of ≥200°. Based on our results, patients with a hip flexion + rotation arc of ≥200° are highly likely to have a positive intraoperative diagnosis of instability (PPV, 89.1%). In patients with a hip flexion + rotation arc of <200°, an intraoperative instability diagnosis is much less predictable and other factors should be used for diagnosis. In younger female patients, an alternative metric may be more optimal, with a clinical predictor of flexion angle >112.5° demonstrating high PPV in our analysis. However, this should be applied in the appropriate context and in conjunction with the balance of the physical examination and intraoperative findings. To that end, we found that our control cohort as a whole had a slightly higher mean flexion than our instability cohort as a whole. We cannot specifically account for these findings, and the reasons are likely multifactorial. This finding does, however, require appropriate and thoughtful consideration for its application as a screening tool. We used our FAI cohort as our comparator for generating our model. This was chosen because we were unable to fully identify any underlying pathology in the asymptomatic controls. However, because we were able to find significant differences in ROM between our FAI cohort and those patients with instability, we believe that these criteria can be used to assist surgeons in identifying patients at risk for instability. Furthermore, this information could aid surgeons in preoperative counseling with their patients about the potential cause of their hip pain and likely intraoperative findings and procedures. This tool should be used as an adjunct to intraoperative findings—namely, ease of distraction, residual subluxation, and location of pathologic findings, in order to assess and determine a patient’s instability status. Heightened awareness of potential instability may help inform intraoperative capsular management decisions—specifically, capsular plication. 13,14
Limitations
This study is not without limitations. ROM measurements were retrospectively collected from patient charts through the assessment of a single, nonblinded surgeon for a portion of the study. These ROM measurements were obtained in the clinical setting and were based on visual measurements. This does call into question the reliability of the measurements; however, as mentioned previously, prior studies have validated the accuracy of visual ROM measurements about the hip. 11 Intrarater reliability was not calculated, and interrater reliability could not be assessed. However, this study was intended as a pilot study to identify potential models and threshold values for future prospective data collection and analysis. Moreover, prior studies have demonstrated the reliability of hip joint ROM, especially with experienced hip surgeons. 10 Therefore, consistent measurements from a single surgeon were deemed sufficient for analysis in this case. Another limitation to this pilot study is that additional variables also contribute to variability in ROM—namely, femoral version and spinopelvic kinematics. In a similar manner, we did not correlate the ROM findings with other physical examination findings associated with hip microinstability. These issues should be considered in future investigations. Further, the surgeon was not blinded to physical examination results at the time of surgery. This leaves open the possibility of confirmation bias for the diagnosis of instability. That stated, the diagnosis of instability or FAI was made based on strict intraoperative criteria and was not influenced by preoperative examination findings.
This study was also limited in that there is no true gold standard for diagnosis of instability intraoperatively. To that end, the prevalence of hip microinstability in our patient population is higher than previously reported in the literature. Potential causes of this finding include heightened awareness of the diagnosis, overdiagnosis within our cohort, or underdiagnosis within the literature. In this study, we used a consistent set of diagnostic criteria that have been used in prior investigations. 12,14,22,26,28 That stated, this method is not without its challenges, as it is based on a “zero traction” state based on body weight traction, which has the potential for variability. This begets another limitation, the fact that our patients were those who were indicated for surgery, potentially leading to selection bias. A further limitation was the baseline differences in demographic characteristics between groups, with a higher proportion of female patients represented in the instability cohorts. Because ligamentous laxity and microinstability are seen more frequently in female patients, these variables were difficult to control in the patient selection phase. Therefore, we sought to control for these variables in our statistical analysis by performing multivariable regression and attempting to create models specific to certain demographic characteristics.
Conclusion
This pilot study demonstrated that clinically detectable hip ROM differed between patients with FAI, patients with instability, and an asymptomatic control group. In patients who undergo hip arthroscopy, a ROM threshold of hip flexion + rotation arc ≥200° may help to identify patients with hip microinstability.
Footnotes
Final revision submitted January 25, 2023; accepted February 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.M.C. has received education payments from Arthrex and Smith & Nephew. A.M. has received education payments from Arthrex, Fones Marketing Management, and Smith & Nephew. M.R.S. has received consulting fees from Anika Therapeutics, Linvatec, Medacta, and Smith & Nephew; royalties and nonconsulting fees from Smith & Nephew; and honoraria from Medacta. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Stanford University (reference No. 48466).