
Abstract
Background:
The utility and safety of patient-specific cutting guides (PSCGs) in osteotomies about the knee is uncertain.
Purpose:
To compare the cost, accuracy of radiographic correction, and safety of PSCG versus standard cutting guide (SCG) corrective osteotomies about the knee.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients undergoing high tibial osteotomy (HTO) or distal femoral osteotomy (DFO) were retrospectively reviewed from 2017 to 2022. Those who underwent 3-dimensional PSCG osteotomy were propensity matched to patients undergoing traditional osteotomies. Procedure time and fluoroscopic details were extracted from operative notes. Hip-knee-ankle (HKA) angle, posterior tibial slope (PTS), and mechanical axis deviation were measured on pre- and postoperative radiographs. Intraclass correlation coefficients were calculated to determine the reliability between the intended and resultant correction of HKA. Time-driven activity-based costing (TDABC) analysis was performed to compare procedure costs.
Results:
A total of 42 patients were included, with 11 HTOs and 10 DFOs in each group. Between the SCG and PSCG groups, respectively, final HKA (2.7° vs 1.9°; P = .36), PTS (9.6° vs 9.0°; P = .79), and mechanical axis deviation (10.2 vs 5.8 mm; P = .21) were similar. The intraclass correlation coefficient between the intended and measured HKA correction was 0.841 (good) in the PSCG group and 0.623 (moderate) in the SCG group. PSCG osteotomies had a mean procedure time that was 18.5 minutes shorter than SCG osteotomies (P = .39). Fluoroscopy time (43 vs 99 seconds; P < .001), tourniquet time (99.9 vs 116.6; P = .12), and radiation dose (2.9 vs 7.8 mGy; P = .01) were lower in the PSCG group. TDABC analysis demonstrated a total cost of $27,026 for PSCG and $27,100 for SCG. The rate of hinge fractures (9.5% vs 33.3%) and return to the operating room (4.8% vs 19.0%) were lower in the PSCG group, although these differences were nonsignificant.
Conclusion:
Both traditionally guided osteotomies and PSCG-guided osteotomies accurately corrected lower extremity malalignment. Utilization of PSCG resulted in similar procedure times and cost, as well as less fluoroscopy and lower tourniquet time, compared with conventional osteotomy. PSCG trended toward a decreased rate of postoperative complications.
The knee is a complex, bicondylar joint that is capable of withstanding the daily mechanical stresses of weightbearing, as well as other stressors in its range of motion. Longevity of the articular surfaces that comprise the knee is dependent on neutral mechanical alignment.12,36 Corrective osteotomy is a well-known treatment for knee joint misalignment. After analysis of the deformity and identification of the center of rotation of angulation, the proper osteotomy location and type can be determined. Distal femoral osteotomy (DFO) may be used to treat valgus knee malalignment, particularly in patients with isolated lateral compartment osteoarthritis or lateral meniscal or focal chondral defects in younger patients. 38 Analogously, high tibial osteotomy (HTO) addresses varus malalignment in symptomatic patients with medial compartment overload and/or medial compartmental osteoarthritis. 20 Both DFO and HTO can also be used in combination with procedures to address meniscal, chondral, or ligamentous pathology.
In the past decade, use of patient-specific cutting guides (PSCGs) has been exponentially increasing in orthopaedic surgery, 14 especially with regard to instrumentation for total arthroplasty of the knee,8,40 hip,16,26 and ankle.25,42 This growing trend certainly extends to osteotomies performed for correction of lower limb alignment.13,30 The hypothesized advantages of PSCG include decreased cost and time savings with respect to procedure time,14,35 as well as possibly more accurate corrections. 5 While these are certainly aspirational surgical outcome goals, the current literature has conflicting results with respect to cost savings and surgical outcomes.3,4,25
In their landmark study, Lee et al 23 described value as outcomes divided by costs. However, this calculation does not take into consideration numerous factors, including the safety of the osteotomy, the learning curve of the surgeons involved, and the expected price reduction in the technology. Some authors have demonstrated improved accuracy and minimization of outliers using PSCG. 5 Thus, the purpose of this study was to compare the cost, accuracy of radiographic correction, and safety of PSCGs versus standard cutting guides (SCG) for osteotomies about the knee. The hypothesis was that PSCG would demonstrate similar radiographic outcomes to SCG, while also demonstrating a significantly reduced procedure time, tourniquet time, and overall cost.
Methods
Cohort Selection
Institutional review board approval was obtained from New York University School of Medicine before commencing study activities. Patients were included who had undergone primary DFO or HTO by 1 of 2 fellowship-trained sports medicine surgeons (M.J.A, L.M.J) at our institution from January 2017 to December 2022. Exclusion criteria included any revision procedure of a previous osteotomy or inflammatory arthropathies. All concomitant procedures were included; however, patients undergoing concomitant procedures outside of chondroplasty or partial meniscectomy were excluded from the time-based analyses. Demographic variables were tracked, including age, sex, body mass index (BMI), laterality, date of surgery, type of osteotomy performed, and concomitant procedures. Additional nondemographic variables that were tracked included total operative time and tourniquet time, duration of fluoroscopy and radiation dose, and intended intraoperative correction of malalignment, taken from operative report. Intraoperative and postoperative complications, including hinge fractures and any return to the operating room (OR) were documented. The presence of a hinge fracture was assessed both intraoperatively using fluoroscopy and postoperatively via radiographs during the first postoperative week and was classified as described by Takeuchi et al. 39 For the sake of the surgeon learning curve, the initial 5 osteotomies for each surgeon performed with the patient-specific system were eliminated from the time-based analysis.
Propensity Matching
Traditional osteotomies were selected for the SCG group using propensity matching based on age at surgery, sex, BMI, and type of osteotomy (DFO or HTO) using the nearest-neighbor method. There was a total of 42 patients who were included in this study with 21 PSCGs matched to 21 SCGs based on age, sex, BMI, osteotomy type, and concomitant procedures. Postmatching balance diagnostics indicated a 94.4% reduction in the standardized mean difference of the logit propensity score to 0.026 between groups and a variance ratio of 1.08.
Measurement of Lower Limb Alignment and Posterior Tibial Slope
Preoperative and postoperative hip-knee-ankle (HKA) angles and mechanical axis deviation (MAD) were measured on preoperative and postoperative upright full-length radiography by a sports medicine orthopaedic fellow (I.S.E.) and a board-certified sports medicine orthopaedic surgeon (L.M.J.), who were blinded to patient identity and surgical technique. The HKA is widely considered the gold standard of lower extremity mechanical alignment and is defined as the angle between 2 lines, with the first drawn from the center of the femoral head to the femoral intercondylar notch, with the second extending from the tibial interspinous point to the tibial midplafond (Figure 1). 27 The MAD is defined as the perpendicular distance between the mechanical axis of the lower extremity and the center of the knee joint (Figure 2). 37

Hip-knee-ankle angle measurement of the left lower extremity on full-length weightbearing radiograph (left) with 3-dimensional modeling of the same limb for the patient-specific cutting guide (right).

Mechanical axis of the left lower extremity on full-length weightbearing radiograph (left) with mechanical axis deviation of the same limb measured perpendicular to the axis to the center of the knee (right).
Posterior tibial slope (PTS) was measured on lateral radiographs as originally described by Dejour and Bonnin. 9 Two circles were drawn below the tibial tuberosity, with the first drawn 5 cm distal to the tibial tuberosity and the second as distal as possible (Figure 3). Each circle was extended to the level of the outer cortex. A line intersecting the centers of the 2 circles was determined to be the longitudinal axis of the tibia. The PTS was defined as the angle between a tangent line to the tibial plateau and a perpendicular line to the longitudinal tibial axis.

Right knee tibial slope measurement on lateral radiograph. To estimate the anatomic tibial axis, 2 circles were drawn on a true lateral knee radiograph below the tibial tubercle at the level of the outer cortex. A line intersecting the centers of the 2 circles represented the longitudinal axis of the tibia.
Surgical Technique for PSCG-guided HTO/DFO
For patients undergoing PSCG-guided HTO or DFO, surgical planning and modeling of PSCG and implant were based on a preoperative knee computed tomography (CT) scan. Based on the procedure (DFO vs HTO), an appropriate approach to the distal femur or medial proximal tibia was made. After exposure, the 3-dimensional (3D)–printed PSCG (BodyCad) were brought into the field and pinned in the appropriate location, which was confirmed via fluoroscopic imaging. The drills were then used to create holes through the PSCG drill guides (BodyCad) in the proposed path of the osteotomy. After this, an osteotome was used to open the osteotomy sites. This was then checked with a ruler to ensure the osteotomy was complete and the hinge was intact. After this, the anterior and posterior validators were placed to measure the appropriate depth of the osteotomy and the 3D guide for the plate placed (BodyCad). After this, the plate was placed and secured in 2 points with screws, after which the validators were removed. The plate was then secured with cortical and locking fixation at the surgeon’s discretion. Bone graft was used at the discretion of the operating surgeon. Final fluoroscopic images were taken to confirm final plate placement and osteotomy location, as well as correction of alignment.
Surgical Technique for Extramedullary HTO/DFO
The techniques for HTO and DFO osteotomies with standard extramedullary guides has been previously described. 10 DFOs and HTOs were fixed with implants at the discretion of the attending surgeon. After standard approaches to the tibia or femur as described above, opening-wedge osteotomy was performed using standard technique according to the implant used. The appropriate correction was determined by the attending surgeon. The use of autologous bone graft or bone graft substitute (allograft iliac crest wedges, demineralized bone matrix, etc) was also at surgeon discretion.
Postoperative Protocol
All patients were placed in a hinged knee brace in extension and made nonweightbearing for 6 weeks after the surgery. At the 6-week mark, standing radiographs were taken to evaluate for appropriate healing, and patients were allowed to begin progressive weightbearing, strengthening and range of motion under the guidance of a physical therapy protocol. At the 3-month mark, radiographs were taken again to evaluate healing and confirm maintained correction of alignment. After confirmation of proper healing and alignment correction, full weightbearing as tolerated was allowed with gradual return to activity.
Cost Analysis
The costs of preoperative imaging (ie, CT scan, anteroposterior knee radiograph, standing limb alignment radiograph) were based on the mean costs billed to insurance and patients at our facility, as determined by our institutional records. CT scans were routinely obtained for proprietary surgical planning involving PSCG, while advanced imaging was not obtained routinely for other included osteotomy techniques. To determine the total cost of the operation, a time-driven activity-based costing (TDABC) analysis was performed, a cost-analysis method that has been validated in the literature with respect to orthopaedics,15,22,34 with cost-per-minute data derived from our institution’s billing and insurance department, a figure that has been referenced previously in quality improvement research at the same institution. 6 Total OR time and tourniquet time of each surgery were collected based on operative records.
Statistical Analysis
Statistical analysis was performed in R Version 4.2.1. Intraclass correlation coefficient (ICC) estimates and their 95% CIs were calculated to determine interrater reliability based on a single-rater, absolute-agreement, 2-way mixed effects model for HKA, MAD, and PTS measurements performed by the 2 blinded readers. ICC values <0.50 were indicative of poor reliability, 0.50 to 0.75 as moderate, 0.75 to 0.90 as good, and >0.90 as excellent. 21 Additionally, ICC was calculated to determine the reliability of the intended intraoperative correction of HKA with HKA measured postoperatively. To compare ICCs between groups, a Fisher transformation was used to convert ICC values to a z-score, then compared using a Student t test. The Shapiro-Wilk test was used to assess continuous variables for normality with Student t tests used to compare the means of normally distributed variables and Mann-Whitney U test for nonnormally distributed variables. Categorical variables were compared between groups using Pearson chi-square test or Fisher exact test when appropriate. A P value of <.05 was considered statistically significant.
Results
Demographics
Of the 42 included patients, the mean age was 35.0 ± 13.5 years, the cohort was 52.4% male, and the mean BMI was 31.9 ± 6.1 kg/m2. There were no significant differences between SCG and PSCG groups with respect to demographic variables or the tracked intraoperative characteristics (Table 1).
Comparison of Demographics and Intraoperative Characteristics Between Standard and Patient-Specific Cutting Guide a

Data are presented as mean ± SD or n (%) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; MAT, meniscal allograft transplantation; MPFLR, medial patellofemoral ligament reconstruction; SCG, standard cutting guide; TTO, tibial tubercle osteotomy.
Operative and Tourniquet Time
There were nonsignificant differences found with respect to total procedure time or tourniquet time between SCG and PSCG, although the PSCG osteotomies took on average 18.5 minutes less and required 16.7 minutes less tourniquet time (Table 2).
Comparison of Operative and Surgical Time Between Standard and Patient-Specific Cutting Guides a

Data are presented as mean ± SD. Bold values indicate statistical significance. PSCG, patient-specific cutting guide; SCG, standard cutting guide.
Fluoroscopy Time and Radiation Dose
When comparing PSCG with SCG groups, PSCG had a mean intraoperative fluoroscopy time of 43.1 ± 25.4 seconds, while SCG had a mean fluoroscopy time of 98.8 ± 27.9 seconds (P < .001) (Table 2). Total radiation dose was also significantly less in PSCG compared with SCG (2.9 ± 2.1 vs 7.8 ± 6.7 mGy; P = .01).
Correction of Alignment
Preoperative and postoperative HKA and MAD were measured on upright, full-length anteroposterior radiographs for each included patient (Table 3). Two readers demonstrated an ICC of 0.912 (P < .001), demonstrating excellent interrater reliability. The PSCG group had lower HKA (1.9° vs 2.7°) and MAD (5.8 vs 10.2 mm) than the SCG group on postoperative radiographs, although these differences did not reach statistical significance. The absolute change in PTS was slightly greater in the PSCG group (2.6° vs 1.6°), although this difference was also nonsignificant.
Comparison of Alignment and Posterior Tibial Slope Measurements of Standard and Patient-Specific Cutting Guides a
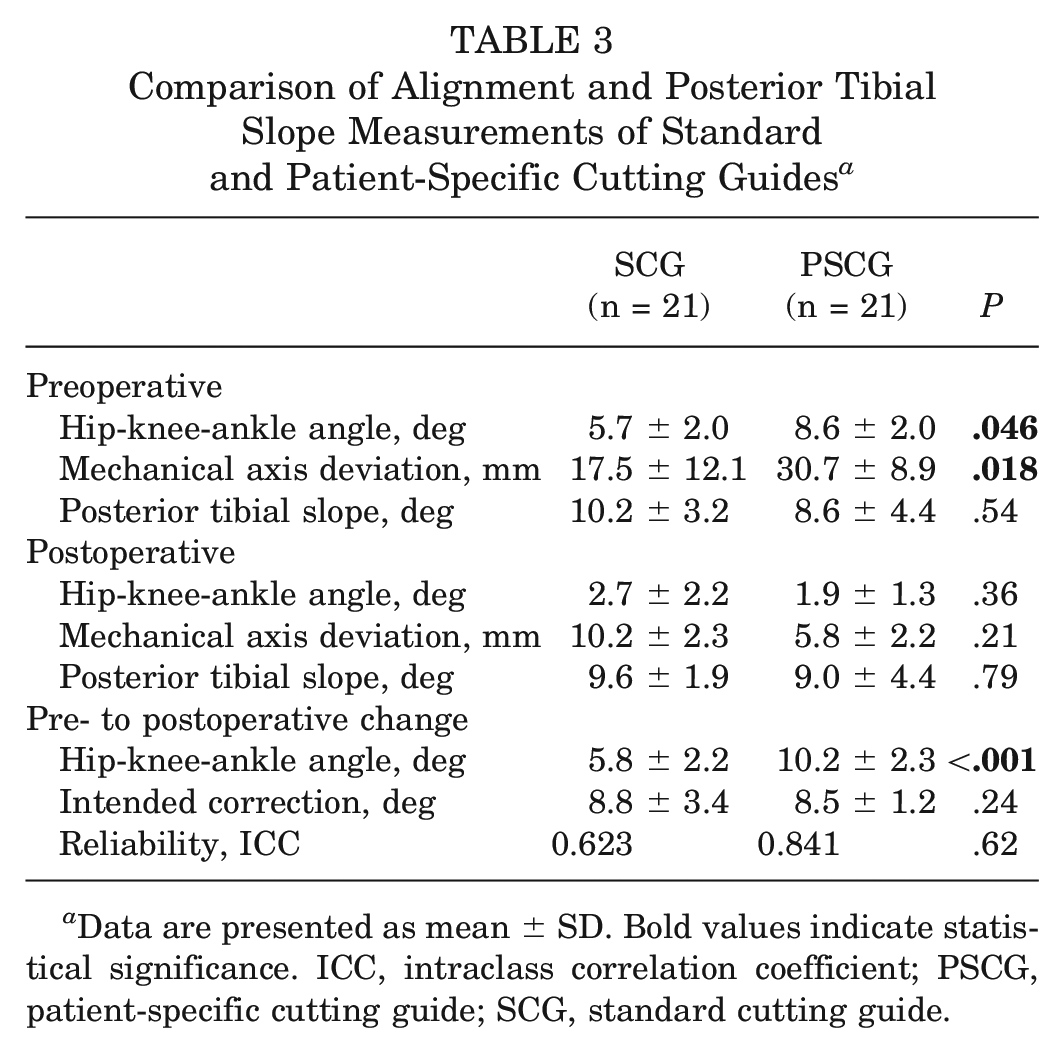
Data are presented as mean ± SD. Bold values indicate statistical significance. ICC, intraclass correlation coefficient; PSCG, patient-specific cutting guide; SCG, standard cutting guide.
The ICC calculated between the intended intraoperative correction and that measured on postoperative imaging demonstrated good reliability in the PSCG group (ICC, 0.84; 95% CI [0.59- 0.94]; P < .001), while there was moderate reliability in the SCG group (ICC, 0.62; 95% CI [0.07-0.88]; P = .02). The difference in reliability between groups was not found to be statistically significant.
Cost Analysis
Per our institutional records, OR time was determined to be billed at a rate of $145 per minute. Using this figure, the SCG group had a cost of $23,896.00 (164.8 minutes × $145/minute) vs $21,213.50 (146.3 minutes × $145/minute) in the PSCG group. The mean cost of the SCG and related hardware was found to be $2,140.80, while the cost of the PSCG system was uniform at $4775.00 per case, inclusive of the proprietary preoperative planning, 3D-printed guides, and customizable plate and screws. When including the cost of preoperative imaging and the HTO/DFO systems, PSCG was more expensive than SCG by $430.73 (Table 4).
Time-Driven Activity-Based Costing and Cost of Preoperative Imaging a

All values are in US dollars. CT, computed tomography; PSCG, patient-specific cutting guide; SCG, standard cutting guide; TDABC, time-driven activity-based costing. Dashes indicate not applicable.
Complications
Intraoperatively, there were 2 (9.5%) hinge fractures identified in the PSCG group and 7 (33.3%) hinge fractures identified in the SCG group (P = .13). In the PSCG group, there was 1 patient (4.8%) who returned to the OR for hardware removal at the 3-month mark (screws backing out), at which time there was noted to be union about the osteotomy site. There were 4 patients (19.0%) in the SCG group that required a return to the OR (P = .34). Two patients required removal of hardware after plate fixation for hinge fractures at 3 and 5 months postoperatively. The third patient underwent removal of hardware due to pain. Last, the fourth patient required manipulation under anesthesia 2 months postoperatively because of a lack of progression of knee flexion past 90°, following index medial patellofemoral ligament reconstruction, tibial tubercle osteotomy, osteochondral allograft transplantation to the patella and trochlea, and DFO. Complications are recorded in Table 5.
Osteotomy Construct and Complications a
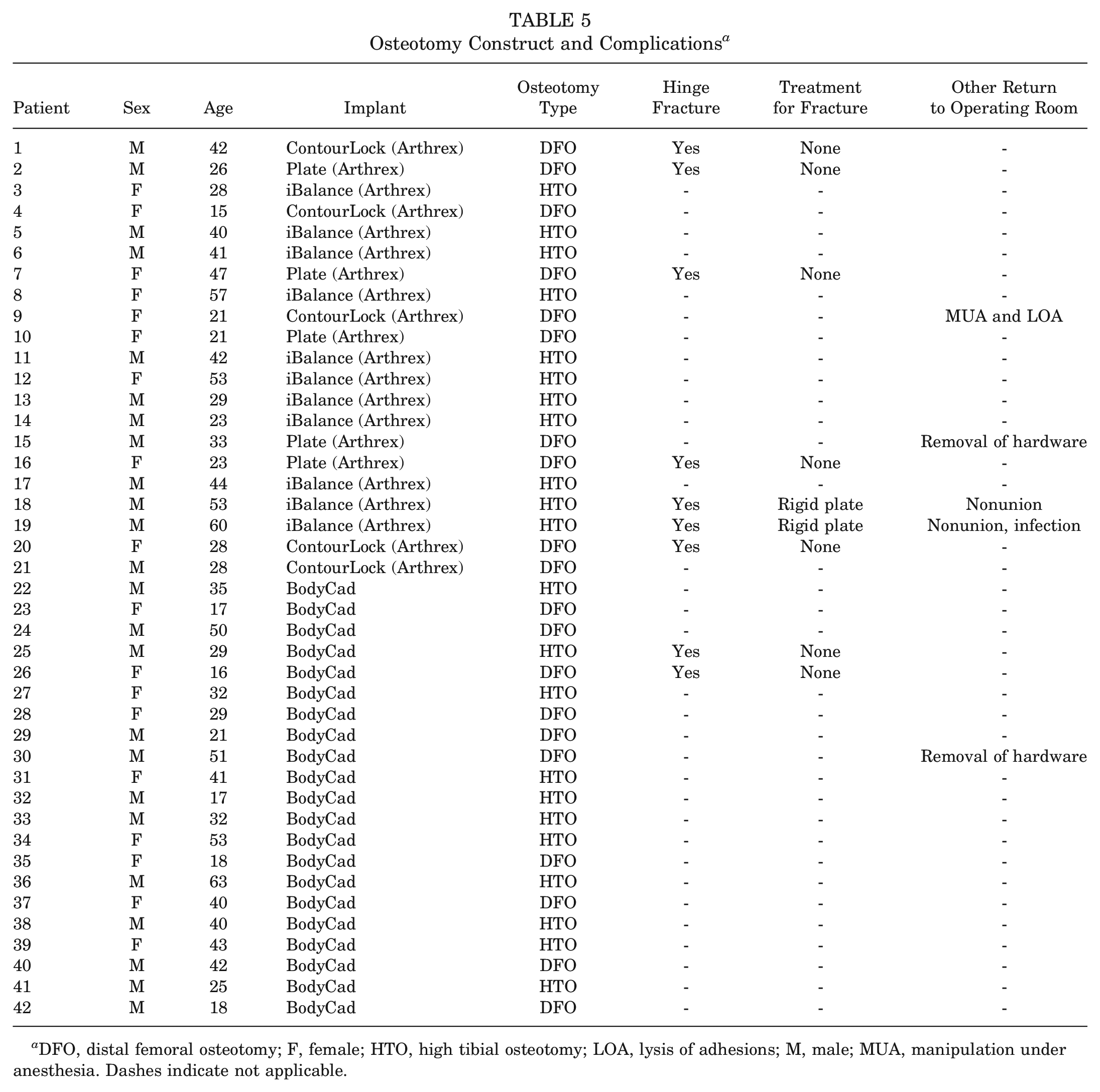
DFO, distal femoral osteotomy; F, female; HTO, high tibial osteotomy; LOA, lysis of adhesions; M, male; MUA, manipulation under anesthesia. Dashes indicate not applicable.
Discussion
Use of PSCG guides for knee osteotomies resulted in a significant reduction in fluoroscopy time and radiation dosage compared with the SCG group, while other metrics, such as cost per procedure, procedure time, accuracy of correction, and rate of hinge fracture and return to the OR were found to be similar. The mean operative time and tourniquet time were 18.5 and 16.7 minutes shorter respectively, for PSCG procedures compared with SCG, although these differences were not statistically significant. With respect to accuracy, PSCG demonstrated good reliability (0.841) between the intended intraoperative correction and that measured on postoperative imaging, while reliability was moderate for SCG (0.623). Last, there was a lower but nonsignificantly different incidence of hinge fractures (9.5% vs 33.3%) and return to the OR (4.8% vs 19.0%) when comparing PSCG and SCG groups.
In executing these osteotomies, intraoperative fluoroscopy is an important tool routinely utilized to ensure proper alignment during the procedure. While fluoroscopy poses minimal radiation dose to patients during such procedures, the dose of radiation over the course of an orthopaedic surgeon’s career, as well as that to OR staff and assistants, can accumulate with insidious repercussions, as has been demonstrated with respect to breast cancer rates among female orthopedists.7,41 One recent study found that PSCG for opening-wedge HTO utilized significantly fewer fluoroscopic images compared with conventional osteotomy. 30 The “as low as reasonably achievable” protocol suggests that surgeons should use the smallest dose of diagnostic radiation possible, and any radiation that has no direct benefit to the procedure should be avoided. 32 The American Academy of Orthopaedic Surgeons strongly supports minimizing the use of ionizing radiation in all orthopaedic settings whenever possible. Although the musculoskeletal system tolerates radiation better than other areas of the body, 33 mitigating unnecessary fluoroscopy and radiation costs to the patient, surgeon, and OR staff remains imperative in eliminating radiation burden. Radiation can be mitigated by the positioning of the x-ray tube beneath the patient, minimizing angles, patient positioning, and limiting the use of supportive blocks. 43 The precision fitting of the PSCG guide and knowledge of the relative distances of the osteotomy from the template allow for minimization of fluoroscopy use intraoperatively. Furthermore, as surgeons grow more comfortable with the technique and the PSCG jigs, it is reasonable to hypothesize fluoroscopy use will be used less frequently. Further study is required with larger sample sizes and more experience with PSCG procedure to better determine the effectiveness of PSCG at reducing fluoroscopy in osteotomies about the knee.
Contrary to the hypothesis, through TDABC analysis, there was not a significant difference in operative time or cost between procedures using SCG and PSCG. TDABC has been validated as a cost-analysis tool for both hip and knee arthroplasty, 2 and a recent systematic review by Koolmees et al 22 found that this analysis method determined a lower and more accurate cost for orthopaedic procedures. Multiple other retrospective studies have looked at the use of PSCG in lower extremity surgery and have not found PSCG to be inherently cost-saving using TDABC cost analysis.29,34 Establishing baseline metrics for accurate cost tracking will be increasingly important, as studies examining cost transparency and data-driven decision making in orthopaedic surgery will continue to proliferate. Ultimately, these metrics will help drive both payers and patients to certain procedures, underscoring the importance of expeditiously establishing appropriate templates for these calculations.
With respect to the efficiency of PSCG, Predescu et al 30 analyzed the use of PSCG in opening-wedge HTOs in 25 consecutive patients and found that PSCG-guided opening-wedge HTOs led to a lower tourniquet time, surgical time, and number of intraoperative fluoroscopic images versus conventional techniques. This study found similar results; however, the difference in surgical times was not statistically significant when excluding the first 5 uses of PSCG to mitigate the learning curve effect. It should be noted that the cases in the present study were some of the first PSCG-guided osteotomies performed at our institution. As with any complex new surgical technique, a learning curve is to be expected. 44 Jacquet et al 18 found that after a learning curve of 10 cases using PSCG for HTO, operative time was optimized. After the initial learning curve, they reported a potential shortening of 70% of operative time compared with conventional techniques. Despite the potential for PSCG to decrease operative time, one of its main disadvantages is increased time required for preoperative planning. Additional time spent by the physician adjusting and approving surgical plans designed by the PSCG manufacturer creates potential opportunity costs in the preoperative period. 27 However, as PSCG technology improves and becomes more familiar to surgeons, this increase in planning time may begin to decrease.
Similarly, with regard to accuracy of correction, SCG and PSCG showed no difference in final correction of mechanical axis deformity, HKA, and PTS. Jeong et al 19 found that PSCG-guided HTOs were able to accurately and efficiently correct varus malalignment while accommodating preexisting hardware, performing the procedure in 65 minutes and noting no pain and excellent range of motion, as well as angular correction of bone within 1.9° of the planned medial proximal tibial angle. Similarly, Munier et al 28 found patient-specific cutting blocks to be an effective means of correcting deformity, with 19 out of 20 measurements falling within <2° of the planned correction based on 3D analysis in 10 patients undergoing medial opening-wedge HTOs with PSCGs. Abdelhameed et al 1 did not find significant differences in precision of correction or Knee injury and Osteoarthritis Outcome Score results between patient-specific instrumentation (PSI) versus freehand techniques at 2-year follow-up. Furthermore, a recent systematic review covering 10 studies on PSI concluded that the use of PSI yielded a significantly lower rate of correction accuracy outliers compared with traditional surgical techniques. However, PSI did not demonstrate a statistically significant improvement in accuracy for achieving desired postoperative alignment. 5 This study demonstrates similar findings with regard to the accuracy of the cutting guides, which appear to be similar to SCG osteotomies in a relatively small sample, albeit utilizing less fluoroscopy. Similarly, the PSCG groups had a higher preoperative HKA and MAD as well as a larger pre- to postoperative correction, indicating that PSCG was used for larger deformities with equal accuracy and time to SCGs. It is plausible that surgeons may derive increased benefit in using PSCGs to plan for more severe deformities, where accurate correction is critical. Further investigation is warranted in exploring the relationship between the severity of deformity and cutting guide choice.
While Lee et al 23 have described health care value as outcome divided by cost on the institution scale, these calculations may not account for the safety of the incorporation of new technology or the projected evolution in efficiency and cost as surgeons become facile with new devices. Additionally, there may be other benefits that are difficult to quantify, such as the PSCG guide plan accounting for the necessary depth of the osteotome at different areas of the osteotomy site, which may enhance the safety profile. Last, while new technologies often improve quality of medical care and standardize outcomes, it is not uncommon for newer technologies to initially create a cost burden when being brought to market. 24 Usually, this cost burden reduces with time, as payers develop contracts with implant companies and/or reimburse implants separately, or the technology is reproduced at a lower cost. Future studies must incorporate economic factors, lower volume surgeons, clinic- and patient-centric outcome studies, and more accurate radiographic parameters in controlled studies to further evaluate the use of PSCG in osteotomies about the knee versus traditional cutting jigs.
Limitations
This study has several limitations, many of which are inherent to its retrospective nature. There is the possibility of selection bias, which we have tried to account for through use of propensity matching. Despite propensity matching, the present study found that surgeons trended more toward using PSCG for operations correcting larger preoperative deformities, potentially introducing a selection bias due to surgeon preference. Furthermore, heterogeneity among involved surgeons with respect to bone graft and implant choice may introduce variability in operation time, affecting the final time and cost analysis. The small sample size is a limitation, which could potentially result in false acceptance of the null hypothesis. Concomitant procedures between the 2 groups were similar but not identical, but procedures outside of chondroplasty or partial meniscectomy were excluded for the time-based cost analysis. Even so, the inclusion of additional concomitant procedures certainly poses a confounding factor in influencing the complication rate or accuracy in a comparison between osteotomy techniques. This study presents the integration of a new technology at our institution, and as such, the values for the operative time of the surgery are likely overestimated in the PSCG group. The learning curve represented by these surgeons may not be fully applicable to surgeons with less experience. In terms of the cost methodology, estimates of the cost of OR time are known to vary widely among different institutions, which diminishes the external applicability of these cost estimates. Other cost methodologies, while not validated in the same manner as TDABC for orthopaedic procedures, may be equally or more effective. Finally, the relative radiation dose of a single-extremity CT is 227 mGy × cm, 31 which may negate the effect of the reduced fluoroscopy for the patient found in this study. Even so, the reduced fluoroscopic burden is still advantageous to the surgeon and OR staff. 17 The use of CT-free preoperative planning tools has recently gained attention in total joint replacement; however, this experimental technology is largely limited to case reports and low–evidence level studies at this time. Finally, radiographs are not the most accurate tool for identifying the location of the osteotomy site preoperatively or determining the slope change after the osteotomy. 11
Conclusion
Both traditionally guided osteotomies and PSCG-guided osteotomies accurately corrected lower extremity malalignment. Utilization of PSCG resulted in similar procedure times and cost, but less fluoroscopy, compared with conventional osteotomy.
Footnotes
Final revision submitted December 22, 2024; accepted January 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.S.R. has received consulting fees from Anika Therapeutics Inc, Arthrex Inc, BodyCad USA, Bone Support, Flexion Therapeutics Inc, Heron Therapeutics Inc, Pacira Therapeutics Inc, Smith & Nephew, Stryker, and Xiros Inc; nonconsulting fees from Arthrex Inc and Smith & Nephew; and support for education from Gotham Surgical Solutions & Devices Inc. M.J.A. has received consulting fees from BodyCad USA, DuPuy Synthes, JRF Ortho, Medical Device Business Services, and Mitek; nonconsulting fees from Arthrex Inc; support for education from Arthrex Inc, Gotham Surgical Solutions & Devices Inc, and Suvon Surgical LLC; research support from Orcosa Inc; publishing royalties for Springer; speaking fees from Arthrex Inc; and hospitality payments from Arthrex Inc and Suvon Surgical LLC. L.M.J. has received support for education from Arthrex Inc, Gotham Surgical Solutions, Mitek, Smith & Nephew, and Suvon Surgical LLC; has received consulting fees from Medical Device Business Solutions; has received hospitality payment from Arthrex Inc, Flexion Therapeutics Inc, Gotham Surgical Solutions, and Horizon Therapeutics PLC; has stock or stock options in Lazurite; and receives publishing royalties from Wolters Kluwer Health–Lippincott Williams & Wilkins. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from NYU Langone (No. i19-01430_MOD14).