
Abstract
Background:
Overall outcomes of revision anterior cruciate ligament reconstruction (ACLR) are well documented, although the durability of results, to the best of the authors’ knowledge, has not been compared between short-term and midterm follow-up.
Purpose:
The primary aim was to assess the durability of revision ACLR outcomes at <5 years after revision (short-term) to outcomes at ≥5 years after revision (midterm). For this study's purposes, durability was defined as not requiring additional revision surgery or the maintenance of good patient-reported outcomes (PROs). The secondary aims were to compare the outcomes between male and female patients, between patients with allografts and those with autografts, and between patients with traumatic mechanisms of a rerupture and those with atraumatic mechanisms of a rerupture.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective chart review with the prospective collection of PROs in 53 knees that underwent revision ACLR. PROs included scores for the International Knee Documentation Committee subjective knee form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Marx activity rating scale, ACL–Return to Sport after Injury scale, visual analog scale for pain, and satisfaction. The time to return to sport or activity and the incidence of reruptures were collected as well. Data were analyzed via the Mann-Whitney U test, chi-square test, Fisher exact test, and odds ratios.
Results:
The mean follow-up from first revision surgery was 5.29 ± 2.96 years (range, 2.0-20.5 years) for the entire cohort. No significant differences in outcomes were found between the short-term (<5 years from revision; 21/53 knees) and midterm (≥5 years from revision; 32/53 knees) groups, except in satisfaction (4.0/5 vs 2.5/5, respectively; P = .014) and requiring second revision surgery (0.0% vs 25.0%, respectively; P = .016). The mechanism of a rupture after primary ACLR leading to revision ACLR was traumatic in 64.7% and atraumatic in 35.3%, but no difference in outcomes was found based on the mechanism of reinjuries (P > .05). When comparing male to female patients, male patients were more active based on the Marx score at the time of follow-up than female patients (7.0 vs 2.0, respectively; P = .046). Patients treated with autografts were younger and had higher KOOS Activities of Daily Living subscores than those treated with allografts, although no other differences were found (P > .05).
Conclusion:
Our study demonstrates that revision ACLR offered patients durable results after the failure of primary ACLR from short-term to midterm follow-up. Patient sex and graft choice did not drastically affect postoperative outcomes. Orthopaedic surgeons may decide, based on their clinical acumen, which graft choice is best for the individual patient and be confident that revision ACLR can achieve desirable results for patients, regardless of the reinjury mechanism and sex. Future work on this topic is needed to look at long-term results.
The anterior cruciate ligament (ACL) is vital to the inherent stability of the knee, resisting excessive anterior translation of the tibia relative to the femur. A rupture of the ACL is detrimental to a patient's quality of life. Much focus is placed on the limitations to an athlete after an ACL rupture and subsequent ACL reconstruction (ACLR), although the nonathlete also faces noticeable limitations in activities of daily living, recreation, and quality of life. An inevitable risk of ACLR is failure of the ACL graft, which occurs with all graft types, although relative risks differ between grafts compared; for example, the hamstring tendon autograft is known to have a higher failure rate compared with the bone–patellar tendon–bone autograft. 11 Graft failure encompasses both a rerupture and graft insufficiency, leading to chronic instability of the knee. 11 The majority of patients with reinjuries to the reconstructed ACL undergo revision ACLR. 12 Reruptures requiring revision ACLR are most often caused by traumatic mechanisms such as during sports or physical activities, although atraumatic mechanisms such as biological failure of the graft occur as well. 11
Although patient-reported outcomes (PROs) after ACLR are known to be lower than before the injury and after primary ACLR, the results are still considered good and reasonable. 7 Rates of return to sport at any level and at the preinjury level are less than those after primary ACLR as well.3,7 PRO measures commonly used to assess subjective outcomes include the International Knee Documentation Committee (IKDC) subjective knee form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Lysholm knee scoring scale, and ACL–Return to Sport after Injury (ACL-RSI) scale.
Previous literature has demonstrated that multiple factors are associated with an increased risk of reruptures after ACLR. Among the risk factors are male sex, younger age at the time of primary ACLR, family history, White race, higher baseline activity level, return to a higher level of activity after ACLR, and ACLR within 1 year after the initial injury. 18 Many studies in the current literature have compared primary ACLR to revision ACLR,3,17,18 compared graft types in revision ACLR,1,5,6,10 or followed a cohort of patients from before revision to after revision.7,9,14,16 However, there is a lack of research evaluating the durability (defined as not requiring additional revision surgery or the maintenance of good PROs) of revision ACLR outcomes. The purpose of this study was to fill that void and compare revision ACLR outcomes at <5 years after revision (short-term) to outcomes at ≥5 years after revision (midterm). The secondary aims were to compare the outcomes between male and female patients, between patients with allografts and those with autografts, and between patients with traumatic mechanisms of a rerupture and those with atraumatic mechanisms of a rerupture. It was hypothesized that there would not be a difference in short-term and midterm outcomes after revision ACLR, indicating that revision ACLR offers patients durable results after primary graft failure. Additionally, it was hypothesized that there would be no difference in outcomes between male and female sex, allografts and autografts, and traumatic and atraumatic mechanisms of a rerupture.
Methods
Patient Enrollment and Data Collection
This was a retrospective chart review with the prospective collection of PROs in patients who had undergone revision ACLR. Study approval was obtained from the academic center's institutional review board (2020-0116). Using Current Procedural Terminology coding for ACLR (code 29888) over an 8-year period (2012-2020), more than 1000 patients were found. After the removal of duplicates and a retrospective chart review, 109 patients underwent revision ACLR at least 2 years before the time of the retrospective chart review. Patients were excluded if they had a multiligamentous knee injury, were <2 years after revision ACLR, or did not have ≤2 years of follow-up PROs. Of the 109 patients, 53 met inclusion and exclusion criteria. A total of 4 sports medicine fellowship-trained orthopaedic surgeons cared for all patients at a tertiary academic medical center; surgeons used both fresh-frozen and irradiated allografts, comprising either the Achilles tendon, bone–patellar tendon–bone, hamstring tendon, or tibialis anterior tendon.
Patient factors including sex, age, and sport played were collected via electronic medical records. Injury details such as primary ACL rupture mechanism, date of primary ACLR, ACL rerupture mechanism, date of revision ACLR, graft used in each procedure, and concomitant knee injuries present during each procedure were also collected. A traumatic mechanism of ACL injuries was defined as an injury sustained during sports or other physical activities. An atraumatic mechanism of ACL reruptures was defined as requiring revision for chronic knee instability or insufficiency of the graft.
At the same time as the retrospective chart review, patients were contacted for PROs. The PRO measures included the IKDC form, KOOS, Marx activity rating scale, ACL-RSI scale, visual analog scale (VAS) for pain, and satisfaction. The KOOS total score was composed of 5 subscores for the following subscales: Symptoms, Pain, Activities of Daily Living, Sports and Recreation, and Quality of Life. Pain was measured using the VAS from 1 to 5, with 1 being “no pain” and 5 being “extreme pain.” Satisfaction was measured on a scale of 1 to 5, with 1 being “very unsatisfied” and 5 being “very satisfied.” Individual questions on the ACL-RSI scale, from OrthoToolKit, 13 were modified on a scale of 0 to 10 (normally on scale of 0-100) (Figure 1).

Anterior Cruciate Ligament–Return to Sport after Injury scale, modified from OrthoToolKit. 13 The questionnaire's individual questions and response scoring.
Our team attempted to contact each of the 109 patients for follow-up surveys (PROs) via email, telephone, or in-person visits. Overall, 53 patients returned surveys via 1 of these 3 methods. The remaining 56 patients were contacted over 10 times for follow-up, but ultimately, these patients did not complete the surveys. The PROs were calculated using orthotoolkit.com at the time the patient filled out the surveys, and the answers to each question were recorded separately. Based on the scoring systems used to calculate each PRO, each answer was awarded a specific number of points. These assigned points are explained when referenced in each table.
Statistical Analysis
Patients were divided into 2 groups: <5 years (short-term) and ≥5 years (midterm) after revision ACLR. We searched the sports medicine and orthopaedic literature, and the benchmark of 5 years was used as the time point for “midterm” outcomes; therefore, we chose this cutoff to coincide with current literature. Dependent ordinal variables or continuous variables without a normal distribution (IKDC, KOOS, ACL-RSI, Marx, VAS pain, satisfaction, time to return to sport after revision) were analyzed using the Mann-Whitney U test. The Shapiro-Wilk test was used to determine if the null hypothesis (normal distribution of the data) should be rejected; a P value ≤.05 was a rejection of the null hypothesis, and therefore, the Mann-Whitney U test was used for the dependent variables. Individual questions on PRO measures with more than 2 possible responses were considered as ordinal variables and analyzed with the Mann-Whitney U test. Median and mean rank values are reported for the Mann-Whitney U test. Dichotomous dependent variables (individual questions on PRO measures with only 2 possible responses) were analyzed using the chi-square test or Fisher exact test. Frequencies and percentages are reported for the chi-square and Fisher exact tests. Odds ratios and 95% confidence intervals were calculated for time to return to sport at the preinjury level after revision ACLR. The Bonferroni correction for multiple comparisons was used to minimize the risk o type I errors. Statistical significance was defined as a P value ≤.05. All statistical analyses were deemed appropriate with the use of Laerd Statistics 8 and conducted using SPSS Statistics for Windows (Version 28.0; IBM).
Results
A total of 53 knees were included in the study; 20 (37.7%) were male, and 33 (62.3%) were female. Overall, 21 (39.6%) were <5 years after revision ACLR (short-term group), and 32 (60.4%) were ≥5 years after revision ACLR (midterm group). There were 8 knees that required second revision surgery, all of which were in the midterm group. The mean age at the time of first revision surgery was 29.62 ± 12.84 years. The mean follow-up from first revision surgery was 5.29 ± 2.96 years (range, 2.0-20.5 years) for the entire cohort. The mean follow-up for patients <5 years from first revision ACLR (short-term) was 3.02 ± 0.81 years (range, 2.0-4.5 years), and for patients at ≥5 years (midterm), it was 6.88 ± 2.89 years (range, 5.0-20.5 years). The short-term and midterm groups were regarded as separate; no patients were included in both groups. Of the 53 patients, 2 had an unknown mechanism of a rerupture and therefore were excluded from the analysis of traumatic versus atraumatic rerupture mechanisms.
Table 1 lists the postoperative PRO scores, and second revision ACLR rates compared between patients with <5 years since revision ACLR and those ≥5 years from revision. No significant differences in PROs were found between the short-term and midterm groups, except in satisfaction and requiring second revision surgery. The midterm group had significantly lower satisfaction (2.5/5) versus the short-term group (4.0/5) (P = .014). The midterm group more often required second revision surgery (25.0%) than the short-term group (0.0%) (P = .016) (Table 1).
Patient-Reported Outcomes Between Short-term and Midterm Groups a

ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; VAS, visual analog scale.
Table 2 outlines the reasons for not returning to the previous level of sport in the short-term versus midterm group. The only significant difference found was that more patients in the short-term group indicated that they returned to the same sport at a different level versus those in the midterm group (23.8% vs 3.1%, respectively).
Return to Previous Level of Sport Between Short-term and Midterm Groups a

Data are presented as n (%).
To investigate the differences in satisfaction and return to sport between groups, individual questions comprising the ACL-RSI scale were analyzed; this is summarized in Table 3. Patients in the midterm group were significantly more nervous about playing their sport (P = .043) and were less confident that they could play their sport without concern for their knee (P = .016).
ACL-RSI Scores Between Short-term and Midterm Groups a

ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury.
Postoperative PRO scores, time to return to sport, and second revision ACLR rates were compared between patients with traumatic mechanisms versus those with atraumatic mechanisms; no statistically significant differences were found (Table 4).
Patient-Reported Outcomes Between Patients With Traumatic Retears and Patients With Atraumatic Retears a

ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; VAS, visual analog scale. Averages of patients’ responses on a scale of 0-10 as outlined in Figure 1.
The same outcomes were compared between male and female patients, which are listed in Table 5. Male patients had significantly higher postoperative Marx scores than their female counterparts (P = .046); no difference was found in other PRO scores, time to return to sport, or second revision ACLR rates.
Patient-Reported Outcomes Between Male and Female Patients a

ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; VAS, visual analog scale.
To elucidate if specific activities led to the difference in Marx scores between female and male patients, the individual questions were analyzed. Male patients engaged in cutting, decelerating, and pivoting activities more often than female patients after revision ACLR (P = .011, P = .019, and P = .047, respectively). For all 3 of these activities, female patients engaged in these activities <1 time per month, while male patients engaged in these activities between 1 time per month and 1 time per week (Table 6).
Marx Scores Between Male and Female Patients a
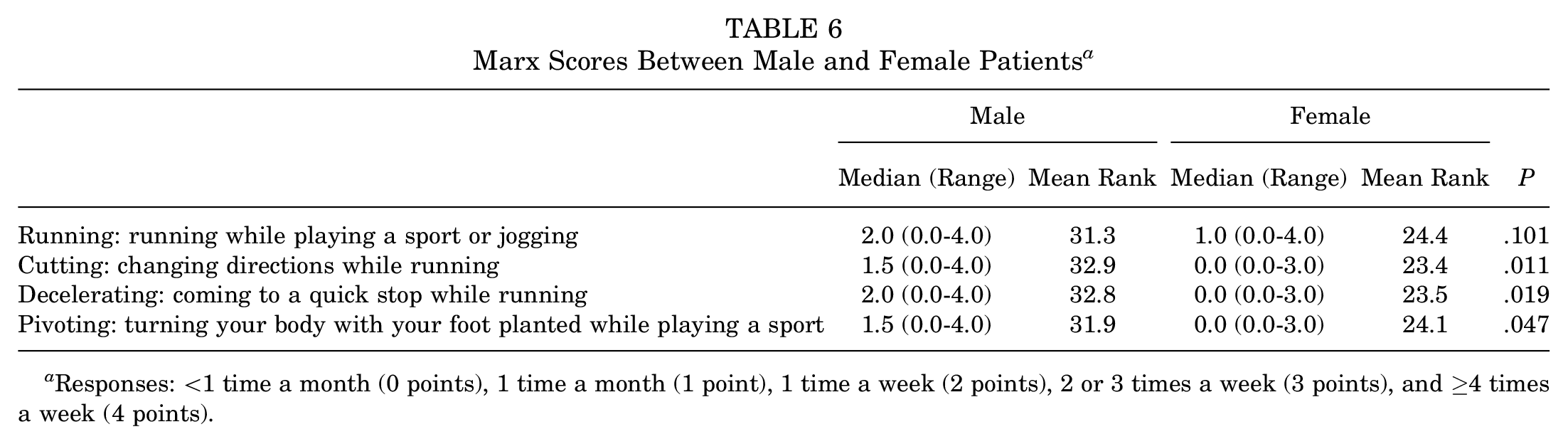
Responses: <1 time a month (0 points), 1 time a month (1 point), 1 time a week (2 points), 2 or 3 times a week (3 points), and ≥4 times a week (4 points).
In an attempt to understand why female patients did not perform these activities as often as male patients, the reasons for not returning to sport at the previous level were analyzed (Table 7). However, no differences were detected between the sexes.
Return to Previous Level of Sport Between Male and Female Patients a

Data are presented as n (%).
Table 8 lists the postoperative PRO scores, time to return to sport, and second revision ACLR rates for patients treated with autografts versus those treated with allografts for revision ACLR. Patients with allografts were significantly older than patients with autografts (34.0 vs 20.5 years, respectively; P = .033). Patients with autografts had higher postoperative KOOS Activities of Daily Living subscores than patients with allografts (P = .042). No other PRO scores, time to return to sport, or second revision rates differed.
Patient-Reported Outcomes Between Patients With Autografts and Patients With Allografts a

ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; VAS, visual analog scale.
To better understand the difference in KOOS Activities of Daily Living subscores, each individual question was analyzed between patients with autografts and patients with allografts. Patients with allografts had more difficulty with descending stairs (P = .033), bending to the floor/picking up an object (P = .036), getting in/out of the car (P = .043), going shopping (P = .002), putting on socks/stockings (P = .012), rising from bed (P = .008), and lying in bed/maintaining their knee position (P = .005) (Table 9).
KOOS Activities of Daily Living Subscores Between Patients With Autografts and Patients With Allografts a

Responses: none (6 points), mild (4 points), moderate (3 points), severe (1 point), and extreme (0 points). KOOS, Knee Injury and Osteoarthritis Outcome Score.
Table 10 summarizes the odds ratios for return to sport at the preinjury level (at least 2 years after revision) based on the number of years after primary ACLR that revision was performed. Patients who underwent revision at 4 to 6 years after primary ACLR had increasingly greater odds of returning to their preinjury level of sport.
Odds Ratios for Return to Sport at Previous Level a

ACLR, anterior cruciate ligament reconstruction.
The graft types used in revision ACLR are listed in Table 11. The short-term and midterm groups showed no differences in the graft type used; no difference was found between traumatic and atraumatic rerupture mechanisms either. However, female patients were more often treated with bone–patellar tendon–bone autografts than male patients (P = .035), and male patients were more often treated with hamstring tendon autografts than female patients (P = .002).
Graft Types Used in Revision ACLR a

Data are presented as n (%). ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone; HT, hamstring tendon; QT, quadriceps tendon; ST/G, semitendinosus/gracilis tendon.
Discussion
This study's purpose was to assess the durability of revision ACLR by comparing patients at <5 years after revision (short-term) and those at ≥5 years after revision (midterm). No significant differences in outcomes were found between the short-term and midterm groups, except in satisfaction (4.0/5 vs 2.5/5, respectively; P = .014) and requiring second revision surgery (0.0% vs 25.0%, respectively; P = .016). Revision ACLR was performed in patients with either traumatic (64.7%) or atraumatic (35.3%) mechanisms, although this did not affect PROs. The only difference noted between male and female patients was that male patients were more active at the time of follow-up based on Marx scores (7.0 vs 2.0, respectively; P = .046). Patients with autografts had higher KOOS Activities of Daily Living subscores compared with patients with allografts (97.0 vs 88.0, respectively; P = .042).
The current literature often compares revision ACLR to primary ACLR. It has been shown by Sroufe et al 17 that postoperative PROs were not different in patients who underwent revision ACLR compared with patients who underwent primary ACLR at 7 months after surgery. However, both revision and primary ACLR outcomes were inferior compared with those of the uninjured patient group. 17 This could potentially be because the knees of the uninjured group had a relatively maintained ACL anatomy, unlike those who endured an ACL rupture. In a retrospective study by Barié et al, 1 patients overall had good PROs (measured by the KOOS) but had very low rates of return to sport at the preinjury level at a mean of 4.4 years after revision ACLR. Patients in the short-term period after revision ACLR have been documented as having IKDC scores ranging from 80.3 to 86.1; failure rates of 2% to 19.2%; and KOOS subscores of 85.0 to 93.0 (Pain), 70.0 to 87.3 (Symptoms), 94.0 to 97.7 (Activities of Daily Living), 65.0 to 82.8 (Sports and Recreation), and 55.0 to 71.8 (Quality of Life).1,4,6,16,17 The results are within the ranges of published data available. Nagaraj and Kumar 12 and Legnani et al 9 reported midterm data (5.2 and 6.3 years’ follow-up, respectively), with IKDC scores of 69.8 to 72.8 and a KOOS total score of 85.8. The median IKDC and KOOS scores in the midterm group are slightly lower than those reported by these studies. Neither of the previously mentioned research compared short-term to midterm data, as was done in this study. PROs largely did not differ between the short-term and midterm groups, which may suggest that revision ACLR offers successful functional results that last from the early to late postoperative years. The fact that 25.0% of patients in the midterm group required second revision surgery, compared with 0.0% in the short-term group, may appear alarming. However, patients in the midterm group had follow-up times ranging from 5.0 to 20.5 years after their first revision ACLR. This provides a substantial amount of time for a reinjury to the ACL graft in comparison to the short-term group, with follow-up times ranging from 2.0 to 4.5 years.
Our secondary aims were to compare PRO scores, time to return to sport, and second revision rates for traumatic versus atraumatic mechanisms of a rerupture, male versus female sex, and allografts versus autografts in revision ACLR. In a retrospective study of patients who were 5.2 years after primary ACLR, 51 of 856 (5.9%) had graft failure, and 33 of 51 chose to undergo revision ACLR. Of the 33 patients, 21 (63.6%) graft failures were caused by a rerupture of the ACL graft (traumatic), and 12 (36.4%) were caused by persistent laxity (atraumatic). A retrospective study found 44.1% of failures to be caused by traumatic mechanisms. 15 Our cohort had a mean follow-up of 5.29 ± 2.96 years and was composed of 64.7% traumatic and 35.3% atraumatic mechanisms, demonstrating that most revision procedures are likely performed because of a traumatic event leading to a graft rupture. However, the reason for revision ACLR is likely not associated with outcomes, as postoperative subjective outcome scores, return-to-sport data, and second revision rates did not differ between mechanisms. We did not perform KT-1000 arthrometer measurements at every visit. Traumatic failures were determined by a history of any injury/event and a clinical examination during office visits. A traumatic mechanism of ACL injuries was defined as an injury during a sport or physical activity event. When taking into account patient sex on outcomes after revision ACLR, male patients were significantly more active over 5 years after surgery than their female counterparts, although all other subjective outcome scores and return-to-sport data were not different. A systematic review found that 88% of meta-analyses reported that female patients had inferior self-reported activity after an ACL injury or ACLR based on return-to-sport data, the Tegner score, and the Marx score. 2 Potentially, female patients are in general less active after revision ACLR, as they are after primary ACLR. Additionally, their baseline activity level may already be lower than that of male patients, but the difference from before the injury to after revision may not differ. This study did not obtain preoperative or preinjury activity level data and therefore cannot draw a conclusion on whether female patients truly have inferior activity levels than male patients after revision ACLR. However, it is notable that male and female patients had similar outcome scores aside from the Marx score as well as overall successful outcomes. The difference in the use of hamstring tendon autografts and bone–patellar tendon–bone autografts between the sexes is likely because the treating surgeon utilized a different graft type from the one used in primary reconstruction. Revision ACLR can offer desirable outcomes to patients, regardless of the indication for revision or patient sex.
The use of autografts versus allografts in revision ACLR is well examined. The MARS (Multicenter ACL Revision Study) Group 10 published data on 1205 patients undergoing revision ACLR, with 48% treated with autografts and 49% treated with allografts; the median time from previous ACLR was 3.4 years. They found that the use of autografts predicted improved IKDC scores, KOOS Sports and Recreation subscores, and KOOS Quality of Life subscores. The use of autografts resulted in patients being less likely to suffer a rerupture of the revised ACL. 10 However, a meta-analysis of 32 studies determined that once irradiated allografts were excluded from analysis, autograft and allograft use for revision ACLR did not differ in outcomes. 5 This study's findings support the conclusion that allograft and autograft use in revision ACLR had comparable outcomes, and the choice of a graft can be made on an individual basis. Although a difference was found in KOOS Activities of Daily Living subscores between graft types, patients with allografts were also significantly older than patients with autografts, which is a confounding factor (Table 8). If preoperative or preinjury data were available in this study population, improvements from before revision to after revision would have been compared between the 2 graft types to assess if the use of one offered better results.
Revision ACLR offered durable results to patients suffering from failure of primary ACLR, with outcome scores, time to return to sport, and rerupture rates similar at <5 years and ≥5 years after revision. The mechanism of a rerupture after primary ACLR did not affect revision outcomes. Minute differences in outcomes may be present between sexes and between graft choices, although results were largely alike. Revision ACLR is a viable option for patients, regardless of the retear mechanism, sex, or graft choice; surgeons can feel confident in recommending revision ACLR to their patients.
Our study is not without limitations. One limitation of the study is the nonconsecutive nature of patient data, as patients were not compared with themselves at separate time points but rather were compared with a similar patient group at a different time point in their recovery. It was attempted to minimize this potential limitation by comparing groups that were similar in characteristics, with a significant difference only noted in the age between those treated with allografts and those treated with autografts (Table 8). Other limitations include the small sample size and the fact that a single surgeon did not perform all surgical procedures, both of which could skew and limit the generalizability of the results.
Conclusion
Our study demonstrates that revision ACLR offered patients durable results after the failure of primary ACLR from short-term to midterm follow-up. Patient sex and graft choice did not drastically affect postoperative outcomes. Orthopaedic surgeons may decide, based on their clinical acumen, which graft choice is best for the individual patient and be confident that revision ACLR can achieve desirable results for patients, regardless of the reinjury mechanism and sex. Future work on this topic is needed to look at long-term results.
Footnotes
Final revision submitted December 22, 2024; accepted January 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.B. has received education payments from Legacy Ortho and CDC Medical. B.G. has received consulting fees from Mitek, Medical Device Business Services, and Zimmer Biomet and education payments from Legacy Ortho. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.