
Abstract
Background:
Hip arthroscopy is an effective treatment for femoroacetabular impingement and labral tears, with improvements in patient-reported outcomes (PROs). Whether anatomic and management differences between sexes translate into divergent outcomes remains uncertain.
Purpose:
To systematically review sex-based differences in radiographic findings, intraoperative pathology, surgical management, and postoperative outcomes after hip arthroscopy.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A literature search of the PubMed, CENTRAL, and Scopus databases was performed on February 27, 2025, in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Articles were included if they reported sex-specific preoperative and postoperative PROs in individuals undergoing hip arthroscopy for femoroacetabular impingement or labral pathology, were published in the English language, and had a minimum 2-year follow-up. Data on patient demographics, radiographic parameters, intraoperative findings, surgical management, and outcomes were extracted. The methodological quality of each study was independently evaluated using the methodological index for non-randomized studies.
Results:
Six studies including 3914 hips (2260 female, 1654 male) met inclusion criteria. Four studies were level 3 and 2 were level 4 evidence, all with moderate methodological quality. All studies demonstrated significant postoperative improvements in PROs (p < .05). Of 4 studies reporting alpha angles, all of them found significantly greater values in male patients (p < .05). Of 6 studies, 1 identified significantly higher Non-Arthritic Hip Score and modified Harris Hip Score totals in men within the 30- to 44-year age subgroup (p = .008; p = .015), and 1 reported significantly higher Hip Sports Activity Scale scores in men (p = .01). One study found that a greater proportion of female patients achieved Patient Acceptable Symptom State thresholds for the 12-item International Hip Outcome Tool (p = .0008). No sex-based differences were observed in minimal clinically important difference achievement, revision arthroscopy, or conversion to total hip arthroplasty (p > .05).
Conclusion:
Male and female patients demonstrated comparable improvements in PROs, achievement of clinically meaningful thresholds, revision rates, and rates of conversion to total hip arthroplasty after hip arthroscopy. Although men exhibited larger alpha angles and more advanced chondral damage, and women more frequently underwent capsular repair, these sex-based differences did not translate into clinically significant disparities in postoperative outcomes.
Hip arthroscopy has become an established procedure for the management of femoroacetabular impingement (FAI) and labral tears, with consistent improvements in patient-reported outcomes (PROs) across diverse populations patients.9,15,24,26,35,37,39 However, increasing evidence suggests that biological sex may influence both the presentation of hip pathology and the subsequent outcomes.7,28
Men tend to have larger alpha angles and greater chondral damage, whereas women more often demonstrate acetabular retroversion, ligamentous laxity, or borderline dysplasia.27,29 These differences may guide intraoperative management and postoperative recovery, underscoring the relevance of sex-specific considerations in surgical planning.2,12,13,42 Despite these differences, previous studies have reported inconsistent results, with some showing sex-based disparities in outcomes and complication rates,3,11,21,33,34 while others found equivalent improvements after hip arthroscopy.4,16,17
Given these uncertainties, a systematic synthesis of the available evidence is warranted. The purpose of this review was to evaluate sex-based differences in radiographic parameters, intraoperative findings, surgical management, and postoperative outcomes after hip arthroscopy for FAI and labral pathology. It was hypothesized that while radiographic and intraoperative differences would be observed between men and women, postoperative PROs and achievement of clinically meaningful thresholds including the minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS) would not differ significantly.
Methods
Study Search and Identification
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 31 A comprehensive search of PubMed, the Cochrane Central Register of Controlled Trials (CENTRAL), and Scopus was performed on February 27, 2025. The search strategy is summarized in Appendix Table A1. Studies were included if they reported sex-specific preoperative and postoperative outcomes for patients undergoing hip arthroscopy with a minimum 2-year follow-up and were published in the English language. Exclusion criteria included review/commentary articles, case reports, studies without sex-stratified data, non-English articles, wrong outcomes/study design ID and duplicate or overlapping patient cohorts from the same institution; in such cases, the study with the largest sample size was retained. This study was registered in PROSPERO (ID CRD 42025646042).
Titles and abstracts were independently screened by 2 reviewers (S.S. and M.A.), followed by full-text assessment of potentially eligible studies. Any disagreements at either stage were resolved by a third senior author (A.E.J.).
Data Extraction
A standardized data extraction form adapted from Cochrane was used. 14 Extracted data included study year and design, number of male and female hips, mean patient age, follow-up duration, radiographic surgical management, and outcomes. Radiographic parameters included the alpha angle, lateral center-edge angle (LCEA), Tönnis angle, and Tönnis grade. The Tönnis grade classifies hip osteoarthritis from grade 0 (none) to grade 3 (severe with joint space loss and deformity). 40 The following PROs were evaluated: Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), 12-item International Hip Outcome Tool (iHOT-12), Copenhagen Hip and Groin Outcome Score (HAGOS), Hip Sports Activity Scale (HSAS), and visual analog scale (VAS) for pain. All data were independently extracted by 2 reviewers (S.S. and M.A.), and any discrepancies were resolved by a senior author (A.E.J.).
Quality Assessment
The same 2 reviewers independently assessed the methodological quality of all included studies using the methodological index for non-randomized studies (MINORS) criteria. 38 Noncomparative studies were scored out of 16, while comparative studies were scored out of 24. For noncomparative studies, scores <8 were considered poor quality, 9 to 14 moderate quality, and 15 to 16 good quality. For comparative studies, cutoff values were ≤14 for poor, 15 to 22 for moderate, and 23 to 24 for good quality. Any discrepancies were resolved by a senior author (A.E.J.)
Statistical Analysis
Forest plots were created using Revman (Version 5.4; Cochrane, 2020). Preoperative alpha angles and LCEAs, as well as preoperative and final follow-up PROs, were analyzed. Heterogeneity was assessed with I2. I2 statistics and results were visualized as forest plots. Because of the retrospective design and heterogeneity of the included studies, quantitative pooling was not performed. 6 Previous guidelines in the Cochrane Handbook were used to assess how much bias due to heterogeneity possibly confounded the results. 5
Results
Study Characteristics and Demographics
A total of 4739 studies were identified through the initial database. After the removal of 1772 duplicates, 2967 studies were screened by title and abstract. Of these, 2923 studies were excluded for not meeting the inclusion criteria, including review articles or commentaries, case reports, studies unrelated to hip arthroscopy or FAI, articles not providing sex-specific analyses, and non-English publications. A total of 44 full-text studies were reviewed for eligibility, of which 38 were excluded: 5 reported unrelated outcomes, 24 had an inappropriate study design, and 9 were overlapping cohorts from the same institutions. Ultimately, 6 studies fulfilled all inclusion criteria and were included.1,8,20,22,25,36 A summary of the study selection process is presented in Figure 1.

Flowchart according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Among the 6 included studies, 4 studies were level 31,8,20,25 and 2 were level 4 evidence.22,36 Studies were performed between 2019 25 and 2025. 36 The studies comprised 3914 hips (1654 male and 2260 female). The patient ages ranged from 32.0 20 to 39.2 years. 22 MINORS scores ranged from 13 36 to 20. 20 All studies showed moderate quality. MINORS criteria assessment of included studies is given in Table 1.
MINORS Criteria Assessment of Studies a

MINORS, methodological index for non-randomized studies.
Radiographic Measurements
Radiographic comparisons between sexes were reported in 4 studies.1,20,22,36 Three studies demonstrated significantly greater alpha angles in men, with mean values ranging from 62.6° to 69.0° compared with 55.8° to 62.1° in women (p < .05).1,20,22 One study conducted an age-stratified analysis, identifying a significant difference favoring men only in the 30- to 44-year age subgroup (59.0° vs 50.4°; p = .006), while no sex differences were observed in younger or older patients (Table 2). 36 The forest plot in Figure 2 demonstrates moderate heterogeneity (I2 = 48%) for alpha angle comparisons.
Comparison of Radiographic Measurements Between Men and Women, Including Alpha Angle, LCEA, Tönnis Angle, and Tönnis Grade a

Data are presented as mean ± SD, unless otherwise indicated. Bold P values indicate statistically significant differences between groups (p < .05). LCEA, lateral center-edge angle.

Forest plot for alpha angle comparisons between men and women. IV, inverse variance.
No significant differences in LCEA were observed across 3 studies, with values ranging from 30.4°± 5.9° to 35.8°± 7.2° in men and 30.5°± 6.0° to 34.7°± 5.5° in women (all p > .05). One study evaluated the Tönnis classification and found a higher prevalence of grade 0 (no radiographic changes) in female patients (73.1% vs 44.2%) and grade 1 changes (mild joint space narrowing and subchondral sclerosis) in male patients (55.8% vs 26.9%) (p = .001), without differences in Tönnis angle 22 (Table 2).
Intraoperative Findings and Surgical Treatments
Five studies reported intraoperative findings and surgical procedures stratified by sex.1,20,22,25,36 Significant results are summarized in Table 3 and presented in detail in Appendix Table A2.
Intraoperative Findings and Surgical Treatments a

ALAD, acetabular labrum articular disruption.
Labral Pathology. One study found that type 2 tears were more frequent in women (27.4% vs 11.6%), whereas types 1 to 2 combined tears were more common in men (47.0% vs 33.1%) (p < .001). 20 Another study reported that labral tear prevalence was comparable (73.0% vs 71.1%) between sexes with labral repair performed at similar rates (92.1% vs 78.3%). 22
Cartilage Pathology. One study reported significantly greater prevalence of severe acetabular cartilage damage in male patients, with higher rates of ALAD grades 3 to 4 and Outerbridge grades 3 to 4 compared with female patients (44.2% vs 13.6% and 43.1% vs 15.1%, respectively; both P < .001). In contrast, no sex-based differences were observed in femoral head cartilage lesions. 20 Another study found rim chondral injuries more frequent in men (82.6% vs 69.2%; p = .04), 22 while an age-stratified analysis of Outerbridge grading in other study showed no significant sex-specific differences. 36
Capsular Management. One study reported higher rates of capsular repair or plication in female patients (88.8% vs 50.4%), while capsulotomy without repair was more frequent in male patients (49.6% vs 11.2%; both p < .001). 20
Femoroacetabular Procedures. One study reported that femoroplasty and acetabuloplasty were significantly more common in men than women (97.0% vs 85.8% and 94.8% vs 82.6%; both p < .001). 20 Another study also found higher femoroplasty rates in men (85.3% vs 65.4%; p = .005), although acetabuloplasty rates were comparable between sexes. 22 A third study reported high overall use of femoral osteochondroplasty (96.9% vs 87.1%) and cartilage procedures (76.5% vs 67.2%) in men compared with women, although without statistical comparison. 25
Other Intraoperative Findings. In 1 study, psoas impingement was more frequently observed in women (19.2% vs 9.6%; p = .001). 22
Patient-Reported Outcomes
All included studies demonstrated significant postoperative improvements compared with baseline in PROs after hip arthroscopy for both men and women (p < .05) (Table 4).
Patient-Reported Outcomes a
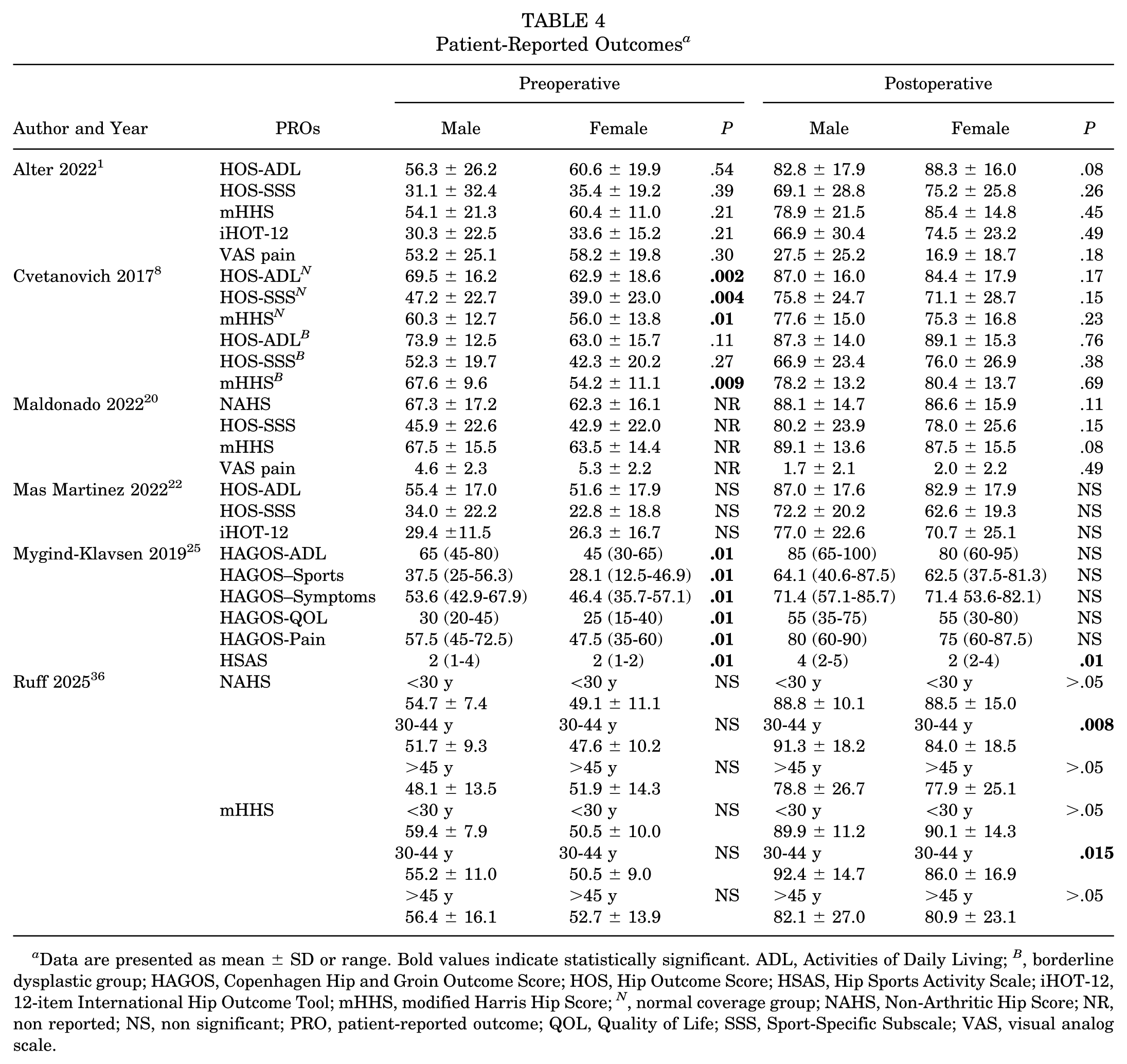
Data are presented as mean ± SD or range. Bold values indicate statistically significant. ADL, Activities of Daily Living; B , borderline dysplastic group; HAGOS, Copenhagen Hip and Groin Outcome Score; HOS, Hip Outcome Score; HSAS, Hip Sports Activity Scale; iHOT-12, 12-item International Hip Outcome Tool; mHHS, modified Harris Hip Score; N , normal coverage group; NAHS, Non-Arthritic Hip Score; NR, non reported; NS, non significant; PRO, patient-reported outcome; QOL, Quality of Life; SSS, Sport-Specific Subscale; VAS, visual analog scale.
Three studies1,8,22 reported HOS-ADL scores, comprising 277 male hips and 325 female hips. One study reported that female patients had significantly lower preoperative HOS-ADL scores compared with male patients (69.5 vs 62.9; p = .002); however, this difference was no longer present at final follow-up (p > .05). 8 The other 2 studies found no significant sex-based differences at either baseline or follow-up.1,22
Four studies1,8,20,22 reported HOS-SSS scores, including 412 male and 471 female hips. One study found men to have significantly higher preoperative HOS-SSS scores compared with women, while postoperative improvements were similar between groups. 8 The remaining studies reported no significant sex-based differences in HOS-SSS outcomes.1,20,22
Four studies1,8,20,36 reported mHHS scores, comprising 409 male and 471 female hips. One study found that men had significantly higher preoperative mHHS in both the normal coverage group (60.3 vs 56.0; P = .01) and the borderline dysplasia group (67.6 vs 54.2; p = .009), with no postoperative differences (p > .05). 8 Another study reported significantly higher postoperative mHHS in men aged 30 to 44 years (92.4 vs 86.0; P = .015). 36 The remaining 2 studies observed no significant sex-based differences in mHHS scores (p > .05).1,20 Heterogeneity varied across the above outcomes. Figures 3 to 5 display forest plots of mHHS, HOS-ADL, and HOS-SSS (I2 = 0%, 42%, and 60%, respectively).

Forest plot for modified Harris Hip Score totals. IV, inverse variance.

Forest plot for Hip Outcome Score–Activities of Daily Living scores. IV, inverse variance.

Forest plot for Hip Outcome Score–Sport-Specific Subscale scores. IV, inverse variance.
Two studies evaluated iHOT-12 outcomes, comprising 155 male and 213 female hips. Neither study identified any statistically significant sex-based differences in postoperative iHOT-12 scores (p > .05).1,22
Two studies reported VAS pain outcomes, comprising 190 male and 268 female hips. Neither study found any statistically significant sex-based differences in postoperative VAS pain scores (p > .05).1,20
Two studies reported NAHS outcomes, comprising 267 male and 321 female hips. One study found that men aged 30 to 44 years demonstrated significantly higher postoperative NAHS compared with women in the same age group (91.3 vs. 84.0; p = .008). No significant sex-based differences were observed in patients <30 years or >45 years (p > .05). 36 The other study observed no significant sex-based differences across age groups or follow-up periods (p > .05). 20
One study evaluated both HAGOS and HSAS outcomes. Male patients demonstrated significantly higher preoperative scores across HAGOS domains as well as higher HSAS levels (p = .01). Postoperatively, no significant sex-based differences were observed in HAGOS subdomains, including ADL, Sport/Recreation, Symptoms, Pain, and Quality of Life (p > .05). However, male patients continued to report significantly higher HSAS scores compared with their female counterparts (4 [2-5] vs 2 [2-4]; p = .01). 25
MCID and PASS
MCID was reported in 3 studies,20,22,36 while PASS was reported in 1 study. 22 No significant sex-based differences in MCID rates were observed for NAHS, mHHS, HOS-SSS, or VAS across studies (p > .05).20,22,36 However, 1 study found that a significantly greater proportion of women met PASS thresholds for iHOT-12 compared with men (73.0% vs 50.9%; p = .0008). No other PASS comparisons were statistically significant (p > .05) 22 (Table 5).
Rates of Achieving the MCID and PASS by Sex a

Data are presented as n (%). Bold values indicate statistically significant. ADL, Activities of Daily Living; HOS, Hip Outcome Score; iHOT-12, 12-item International Hip Outcome Tool; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; NS, non significant; PASS, Patient Acceptable Symptom State; PRO, patient-reported outcome; SSS, Sport-Specific Subscale; VAS, visual analog scale.
Revision Arthroscopy and Conversion to Total Hip Arthroplasty
Three studies reported revision arthroscopy and conversion to total hip arthroplasty (THA), with no statistically significant differences between sexes20,22,36 (Appendix Table A3).
Discussion
The most important finding of this review is that both male and female patients experienced significantly superior PROs after hip arthroscopy for FAI and/or labral pathology, regardless of baseline anatomic and radiographic differences. Across the included studies, male patients consistently exhibited higher preoperative alpha angles, whereas no statistically significant sex-based differences were reported in LCEA. Intraoperatively, male patients more frequently exhibited severe chondral lesions and underwent femoroplasty at higher rates, whereas female patients more often received capsular repair and had a higher incidence of psoas impingement. However, most studies did not demonstrate statistically significant sex-based differences in intraoperative pathology. There were no consistent sex-based disparities in achieving the MCID, revision rates, or conversion to THA.
Superior postoperative PROs in male patients were identified in only 2 studies.25,36 Ruff et al 36 reported higher postoperative NAHS and mHHS scores among men aged 30 to 44 years, while Mygind-Klavsen et al 25 observed higher HSAS levels in men. These differences likely reflect age-specific characteristics or activity demands rather than sex as an independent determinant of outcome. Notably, no study demonstrated superior postoperative PROs in women. Overall, these observations align with previous evidence indicating that both sexes achieve clinically meaningful improvement after hip arthroscopy. 7 This is consistent with Maerz et al, 19 who reported that although women had lower preoperative and postoperative scores, the degree of improvement was equivalent or greater, and sex was not an independent predictor of outcome after adjustment for confounders.
Because the MCID reflects relative improvement from baseline, differences in initial scores should be considered. Most included studies, however, reported no clinically significant sex-based differences in preoperative PROs, thereby minimizing the risk of systematic bias. Although Mas Martinez et al 22 reported that a higher proportion of women reached PASS on the iHOT-12, the rates of MCID achievement were comparable between sexes across other studies.20,22,36 These findings indicate that both men and women reliably achieve clinically meaningful improvement after hip arthroscopy, consistent with previous evidence showing that sex does not independently influence the likelihood of achieving clinical benefit.10,11,19
Four studies reported alpha angle measurements,1,20,22,36 with 3 demonstrating significantly greater alpha angles in male patients.1,20,22 Ruff et al 36 found this difference to be significant only in the 30- to 44-year age subgroup, suggesting age-related effects. These findings are consistent with previous reports noting that cam morphology predominates in men.30,41 Conversely, no statistically significant differences in LCEA were identified between sexes.20,22,36 However, previous literature has reported significantly greater acetabular coverage in women,18,23,32 suggesting that sex-based variations in acetabular morphology may exist in broader populations beyond those represented in this review.
Five studies stratified intraoperative findings and surgical management by sex,1,20,22,25,36 with 2 demonstrating statistically significant differences.20,22 Male patients exhibited a higher prevalence of advanced chondral injury, including Outerbridge grade 3 to 4 acetabular lesions 20 and rim chondral lesions, 22 and underwent femoroplasty more frequently.20,22 These findings are consistent with the morphometric study by Zhang et al, 43 which demonstrated larger cam deformity volumes in men, predisposing them to more extensive chondrolabral damage. Similarly, previous systematic reviews have shown that men more commonly have cam-type morphology and complex chondrolabral injury, contributing to higher rates of femoroplasty and combined femoroplasty/acetabuloplasty.30,41 Conversely, female patients more frequently demonstrated psoas impingement and generalized ligamentous laxity, 22 which contributed to higher rates of capsular repair or plication. 20
Three studies evaluated revision hip arthroscopy and conversion to THA, with no statistically significant sex-based differences.20,22,36 These findings align with previous systematic reviews indicating that sex is not an independent predictor of revision surgery or THA conversion after hip arthroscopy.7,30,41
Limitations
This review synthesized only sex-stratified analyses and excluded overlapping patient cohorts from the same institutions to minimize duplication bias and strengthen the validity of the synthesized results. By focusing exclusively on studies that directly compared male and female patients, it provides a targeted and internally consistent evaluation of sex-based differences in hip arthroscopy outcomes. Nonetheless, several limitations should be acknowledged. The overall body of evidence remains limited, with only 6 eligible studies, all of moderate quality and predominantly retrospective in design. In addition, there was a lack of consistency in PROs and heterogeneity in outcome measures, which reduced comparability across studies. Given these constraints, no quantitative pooling was performed. 6
Conclusion
Male and female patients demonstrated comparable improvements in PROs, achievement of clinically meaningful thresholds, revision rates, and rates of conversion to THA after hip arthroscopy. Although men exhibited larger alpha angles and more advanced chondral damage, and women more frequently underwent capsular repair, these sex-based differences did not translate into clinically significant disparities in postoperative outcomes.
Footnotes
Appendix
Rates of Revision Arthroscopy and Conversion to THA a

| Author and Year | Revision Hip Arthroscopy | P | Conversion to THA | P | ||
|---|---|---|---|---|---|---|
| Female | Male | Female | Male | |||
| Maldonado 2022 20 | 97/860 (11.3) | 37/466 (7.9) | >.05 | 38/860 (4.4) | 29/466 (6.2) | >.05 |
| Mas Martinez 2022 22 | 0/52 (0.0) | 2/104 (1.9) | NR | 0/52 (0.0) | 4/104 (3.8) | NR |
| Ruff 2025 36 | 2/103 (1.9) | 5/48 (10.2) | >.05 | 7/103 (6.6) | 1/48 (2.0) | >.05 |
Data are presented as n (%). NR, non reported; THA, total hip arthroplasty.
Final revision submitted August 28, 2025; accepted October 6, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.