
Abstract
Background:
Acute knee dislocations are devastating injuries that can be challenging for surgeons to treat. The bony integrity of the tibial plateau and the lateral femoral condyle has a fundamental meaning for translational and rotational knee joint stability. Posterolateral tibial plateau depression fractures (PLTPFs) and lateral femoral condyle impaction fractures (LFCIFs) can influence clinical outcomes, but their frequency and characteristics in the setting of acute knee dislocations are unknown.
Purpose:
To report the incidence of PLTPFs and LFCIFs in acute knee dislocations as well as to describe concomitant soft tissue lesions associated with these bony injuries.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
In this retrospective multicenter study, acute knee dislocations (at least bicruciate ligament injuries) were identified from hospital information systems based on diagnosis-related group coding as well as operation and procedure classification coding at 5 participating level 1 trauma centers from 2018 to 2022. The knee dislocations were categorized according to the Schenck classification. Soft tissue injuries were assessed on magnetic resonance imaging within 2 weeks of the trauma. PLTPFs and LFCIFs were categorized on magnetic resonance imaging and computed tomography according to the Menzdorf and Bernholt classifications.
Results:
A total of 157 knee dislocations were identified, comprising 106 men and 51 women with a mean age of 39.3 ± 15.1 years. A PLTPF was detected in 42 (26.8%) knee dislocations, with the highest frequency in Schenck type III medial dislocations. Of these 42 cases, 26 (61.9%) PLTPFs were rated as high-grade fractures, theoretically requiring reduction and fixation. An LFCIF was found in 31 (19.7%) of the cases.
Conclusion:
A PLTPF was observed in one-quarter, and an LFCIF in one-fifth, of acute knee dislocations. They occurred particularly in knee dislocations with medial collateral ligament ruptures. Almost two-thirds of all PLTPFs presented as high-grade fractures according to the Menzdorf or Bernholt classification, potentially requiring a surgical intervention.
Keywords
Posterolateral tibial plateau depression fractures (PLTPFs; so-called apple-bite fractures) and lateral femoral condyle impaction fractures (LFCIFs; so-called lateral femoral notch signs) can frequently be found as concomitant bony injuries with anterior cruciate ligament (ACL) ruptures or multiligament injuries of the knee.4,5,13,17,19,26 Their occurrence has been described in up to 49% (PLTPF) and 25.9% (LFCIF) of cases. 4 Other than ACL tears, PLTPFs and LFCIFs are typically associated with additional soft tissue injuries such as lesions of the medial collateral ligament (MCL) or the lateral meniscus, illustrating the increased biomechanical force that results in complex knee injuries.10,13,20,26 While the influence of an LFCIF on the clinical outcomes of ACL reconstruction has yet to be elucidated and remains rather vague, a higher grade PLTPF is associated with impaired functional outcomes, despite ligament reconstruction, as it typically increases anterolateral rotational instability and increases the pivot-shift phenomenon.6,10,20 Biomechanically, Milinkovic et al 18 were able to underscore the meaning of the bony integrity of the posterolateral tibial plateau in the ACL-deficient knee to support the posterolateral horn of the meniscus. A lack of more than 50% of bony support of the posterolateral horn of the meniscus resulted in increased tibial translation at 0° and 30° of knee flexion (Lachman test), an increased pivot-shift phenomenon, and increased internal rotation. 18
However, despite the generally accepted importance of PLTPFs to the outcomes of ligament instability, there is currently no uniform recommendation on which fracture grade should be treated. Currently, there are 2 major classifications that categorize PLTPFs, namely, by Bernholt et al 5 and Menzdorf et al, 17 both with moderate to good reliability. 19 Menzdorf et al 17 suggested a surgical intervention in PLTPFs with a depression of more than 2 mm and a lack of more than 50% of bony support of the posterior horn of the lateral meniscus (LMPH). After a follow-up of 18 months, good clinical outcomes were reported with no ACL failure. 17
Hence, while our understanding of the importance of PLTPFs and LFCIFs in the treatment of ACL or simple multiligament (ACL and MCL) injuries of the knee is growing, its meaning in the treatment of acute knee dislocations, defined as bicruciate ligament ruptures, is not yet known.3,9,14 While short-term outcomes in acute knee dislocations may be satisfactory, long-term outcomes are associated with revision knee arthroplasty in 2% to 9% of cases. 27 Hence, there is still a great need to enhance our understanding and treatment algorithms to improve overall clinical results. The influence of untreated concomitant bony lesions on surgical outcomes is unknown. Therefore, the goal of the present study was to analyze the frequency and severity of concomitant bony lesions, to identify the risk factors associated with bony lesions (particularly PLTPFs), and to describe associated injuries in the setting of an acute knee dislocation.
Methods
In this retrospective multicenter study, all patients who were surgically treated for a knee dislocation from January 2018 to December 2022 at 1 of 5 level 1 trauma centers were included. In the preparation of this article, the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist was used. 25 Patient data from each hospital’s information system were utilized and analyzed in an anonymous form. A knee dislocation as a special entity within multiligament injuries of the knee was defined as a bicruciate ligament injury, including an injury to both the ACL and posterior cruciate ligament (PCL). The search string included the diagnosis-related group codes I30B and I30C as well as the German operation and procedure classification (OPS) codes 5-803.3, 5-803.4, 5-803.5, and 5-803.c for open reconstruction; 5-813.6, 5-813.7, and 5-813.8 for arthroscopic reconstruction; and 5-813.k for suture repair of the PCL, which was defined as the smallest common denominator of a knee dislocation. To settle health care costs, every surgical intervention has to be classified according to the OPS codes in Germany. Ethical approval was granted by the local ethics committee (2021-300079-WF).
We included all patients with a surgically treated acute (within 2 weeks) bicruciate ligament injury, at least to both the ACL and PCL, at 1 of the 5 trauma centers with complete preoperative magnetic resonance imaging (MRI). Exclusion criteria were isolated cruciate ligament injuries, geriatric patients older than 70 years, and chronic injuries without MRI within 2 weeks of the acute injury. MRI was performed at 3 T as part of the clinical routine using a dedicated 16-channel knee coil with a maximum knee flexion of 10°. Standard imaging protocols included localizer, axial, coronal, and sagittal fat-saturated proton density–weighted T2 sequences as well as a coronal T1-weighted sequence with a reconstructed slice thickness of 3 mm. Radiological imaging was analyzed by 2 independent blinded observers (an experienced consultant in knee surgery and a resident in orthopaedics and trauma surgery) using a picture archiving and communication system in the clinic. Analyzed were the occurrence of PLTPFs and LFCIFs as well as soft tissue injuries. A PLTPF was defined as a depression fracture of the posterolateral tibial plateau. An LFCIF was defined as an impaction fracture of the lateral femoral condyle of more than 2 mm.
All acute knee dislocations were categorized using the Schenck classification with respect to the major ligament components involved (ACL, PCL, superficial MCL, deep MCL, lateral collateral ligament [LCL], popliteus tendon) and associated injuries. In addition, other soft tissue injuries such as those of the posterior oblique ligament (POL), the popliteus muscle, the biceps femoris muscle, the iliotibial band, the posterolateral capsule, the popliteofibular ligament (PFL), the medial patellofemoral ligament, and the patellar tendon were also recorded. For meniscal injuries, in addition to detecting injuries to the lateral and medial menisci, a distinction was made between injuries to the anterior horn, the meniscal body, or posterior horn. Additionally, neurovascular lesions were assessed.
Once neurovascular injuries were identified, a surgical intervention was performed within the first 2 weeks because of the highest potential to benefit from ligament repair according to the “Hamburg concept.”3 The indications for the surgical treatment of PLTPFs were determined using the Menzdorf classification.17,23 Surgical treatment of the PLTPF was considered if the LMPH was less than 50% supported by bone and there was a step of more than 2 mm (Menzdorf type 1b, 2b, or 2c or Bernholt type ≥IIB) (Figures 1 and 2).5,17

A 26-year-old soccer player with a Schenck type III medial knee dislocation and a Menzdorf type 2b posterolateral tibial plateau depression fracture (PLTPF). (A) On axial T2-weighted magnetic resonance imaging (MRI), the red circle marks the torn medial collateral ligament, and the red “&” marks the torn anterior cruciate ligament and posterior cruciate ligament. (B) On sagittal T2-weighted MRI, the arrowhead marks the lateral femoral condyle impaction fracture (LFCIF), the small arrow marks the lateral meniscus (which is no longer supported by bone), and the large arrow marks the PLTPF. (C) Coronal T2-weighted MRI. (D) Axial, (E) sagittal, and (F) coronal computed tomography. Here, the large arrow marks the PLTPF.
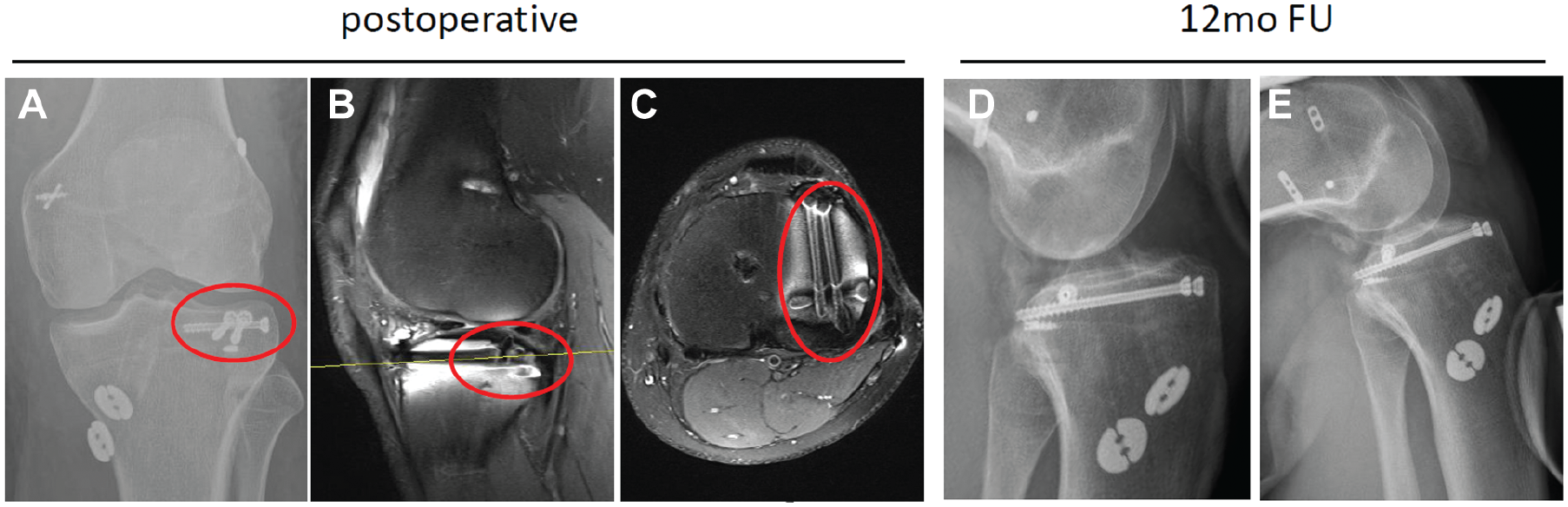
The same soccer player with a Schenck type III medial knee dislocation and a Menzdorf type 2b posterolateral tibial plateau depression fracture (PLTPF) from Figure 1. Immediately postoperative (A) coronal radiography and (B) sagittal and (C) axial magnetic resonance imaging demonstrating posterior cruciate ligament (PCL) suture augmentation, anterior cruciate ligament (ACL) reconstruction, medial collateral ligament repair, and anatomic arthroscopic reduction and internal fixation of the PLTPF (red circle) using cannulated screws with the jail technique.8,27,28 Stress radiography at 12-month follow-up of (D) the ACL at 30° of flexion and (E) the PCL at 90° of flexion, demonstrating stable ligaments.
Statistical Analysis
Data are presented as means and standard deviations for continuous data and counts and percentages for categorical data. Comparisons of categorical data (sex, knee dislocation classification, PLTPF/LFCIF occurrence, soft tissue injuries) were performed using the chi-square test. The Shapiro-Wilk test and the Kolmogorov-Smirnov test were performed to determine if the data were normally distributed. Comparisons of 2 unpaired groups (eg, demographic characteristics between fracture groups) with parametric and nonparametric data were performed using the unpaired t test and the Wilcoxon signed-rank test, respectively. The interobserver reliability of the collected data was examined using the Cohen kappa coefficient to assess agreement between the 2 independent observers. The interpretation was evaluated according to Landis and Koch 16 as follows: <0.00, no agreement; 0.00-0.20, low agreement; 0.21-0.40, moderate agreement; 0.41-0.60, substantial agreement; 0.61-0.80, good agreement; and 0.81-1.00, almost perfect agreement. The level of significance for all tests was set at P ≤ .05. All data were analyzed using SPSS Statistics (Version 26.0; IBM).
Results
Of a total of 753 cases found using the search string, we were able to include 157 acute knee dislocations from the 5 study centers in the years 2018 to 2022. The mean age was 39.3 ± 15.1 years, and the total cohort included 106 men and 51 women. The mean body mass index was 29.6 ± 7.3 kg/m2 (range, 18.4-55.6 kg/m2). In 23% of cases, a high-energy trauma mechanism, such as a vehicle accident, was the cause of the injury; in 57%, a low-energy trauma mechanism, mostly in the context of recreational activities, was the cause of the injury. In 20% of cases, an ultra low–energy mechanism was identified as the cause of the knee dislocation.
Posterolateral Tibial Plateau Depression Fractures
A PLTPF was detected in 42 (26.8%) knee dislocations. In terms of sex and age, there was no statistically significant difference between the groups with PLTPFs and without PLTPFs (Table 1). An increased incidence of PLTPFs was noted in knee dislocations classified as Schenck type III medial (P < .001) (Table 2).
Characteristics of Patients for PLTPFs a
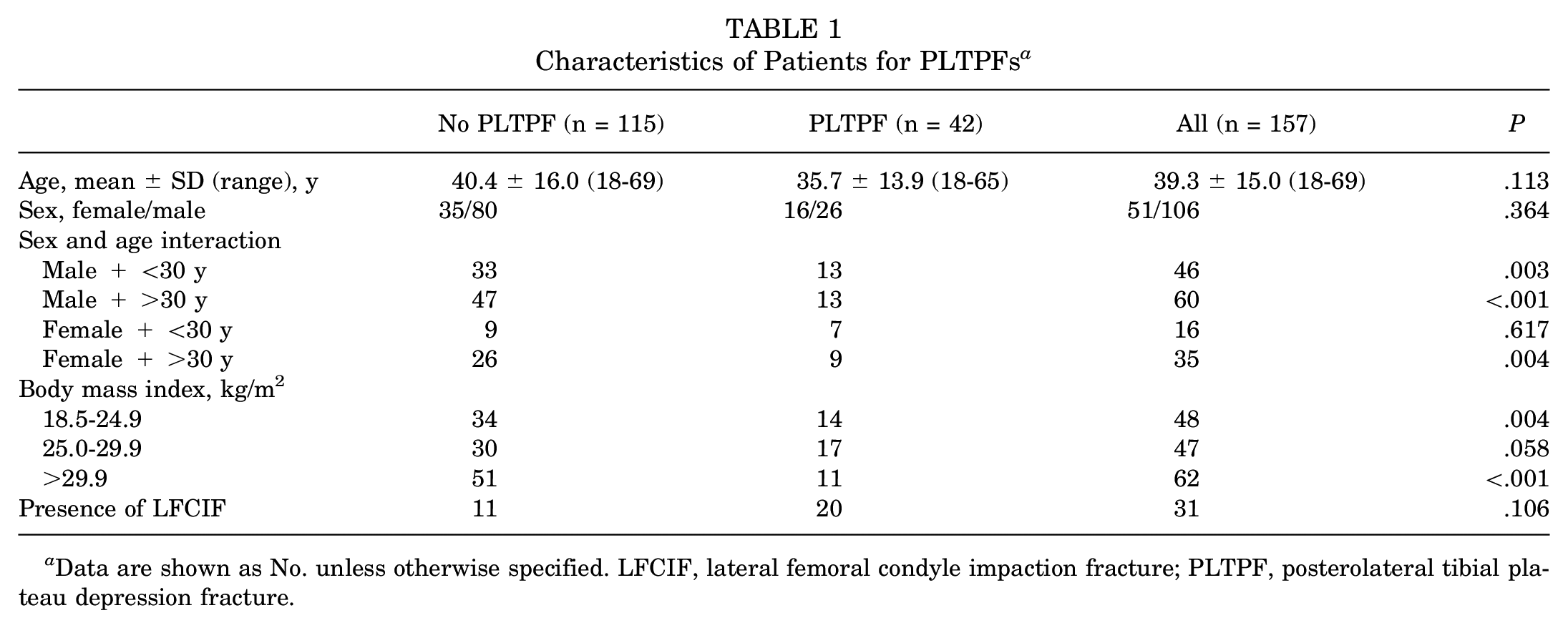
Data are shown as No. unless otherwise specified. LFCIF, lateral femoral condyle impaction fracture; PLTPF, posterolateral tibial plateau depression fracture.
Schenck Classification of Knee Dislocations for PLTPFs a
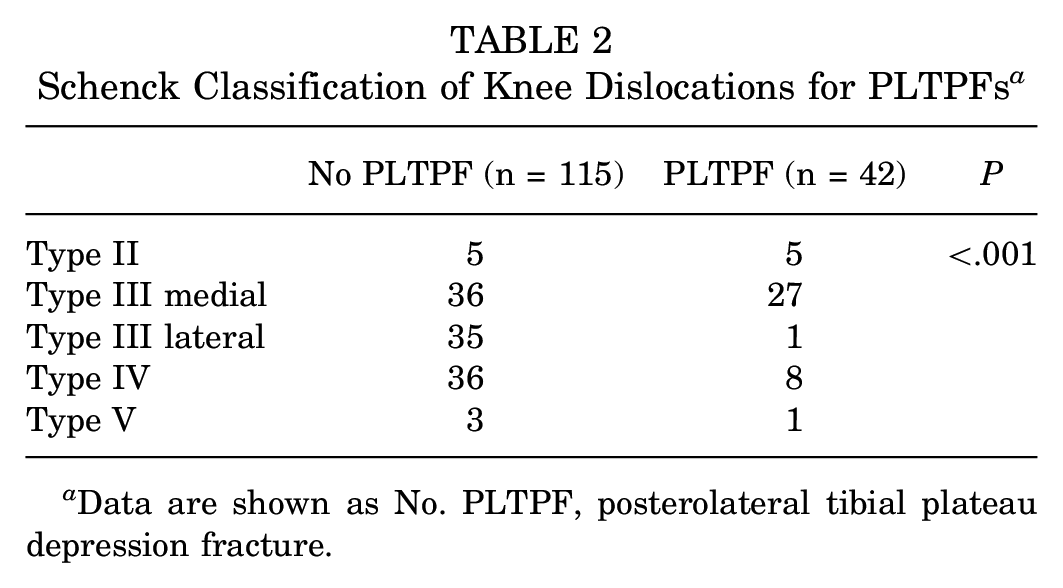
Data are shown as No. PLTPF, posterolateral tibial plateau depression fracture.
A subgroup analysis of cases with a PLTPF showed significantly more superficial MCL (n = 32 [76.2%]) and deep MCL (n = 34 [81.0%]) injuries than cases without a PLTPF (P < .001). Also, significantly more LMPH injuries were observed in cases with PLTPFs than in cases without PLTPFs (17 [70.3%] vs 7 [29.2%], respectively; P < .001). Injuries to the medial meniscus (P < .001) and LCL (P = .002) were significantly less common with concurrent PLTPFs. A significantly lower frequency was also found for injuries to the other soft tissue structures examined (LCL, popliteus tendon, POL, popliteus muscle, biceps femoris muscle, iliotibial band, posterolateral capsule, PFL, medial patellofemoral ligament, patellar tendon, and neurovascular structures) with the occurrence of PLTPFs (Figure 3). Of all PLTPFs, 26 (61.9%) were rated as high-grade fractures, theoretically requiring reduction and fixation. High-grade PLTPFs showed significantly more MCL lesions (26 [78.8%] vs 9 [60.0%], respectively; P = .005) and less frequent LCL injuries (3 [20.0%] vs 12 [44.4%], respectively; P = .02) than low-grade PLTPFs. The same result was shown for other lateral structures such as the popliteus tendon (15 [55.6%] vs 0 [0.0%], respectively; P < .001), popliteus muscle (14 [51.8%] vs 0 [0.0%], respectively; P < .001), posterolateral capsule (12 [44.4%] vs 0 [0.0%], respectively; P < .001), and PFL (12 [44.4%] vs 1 [6.7%], respectively; P < .001) (Figure 3).
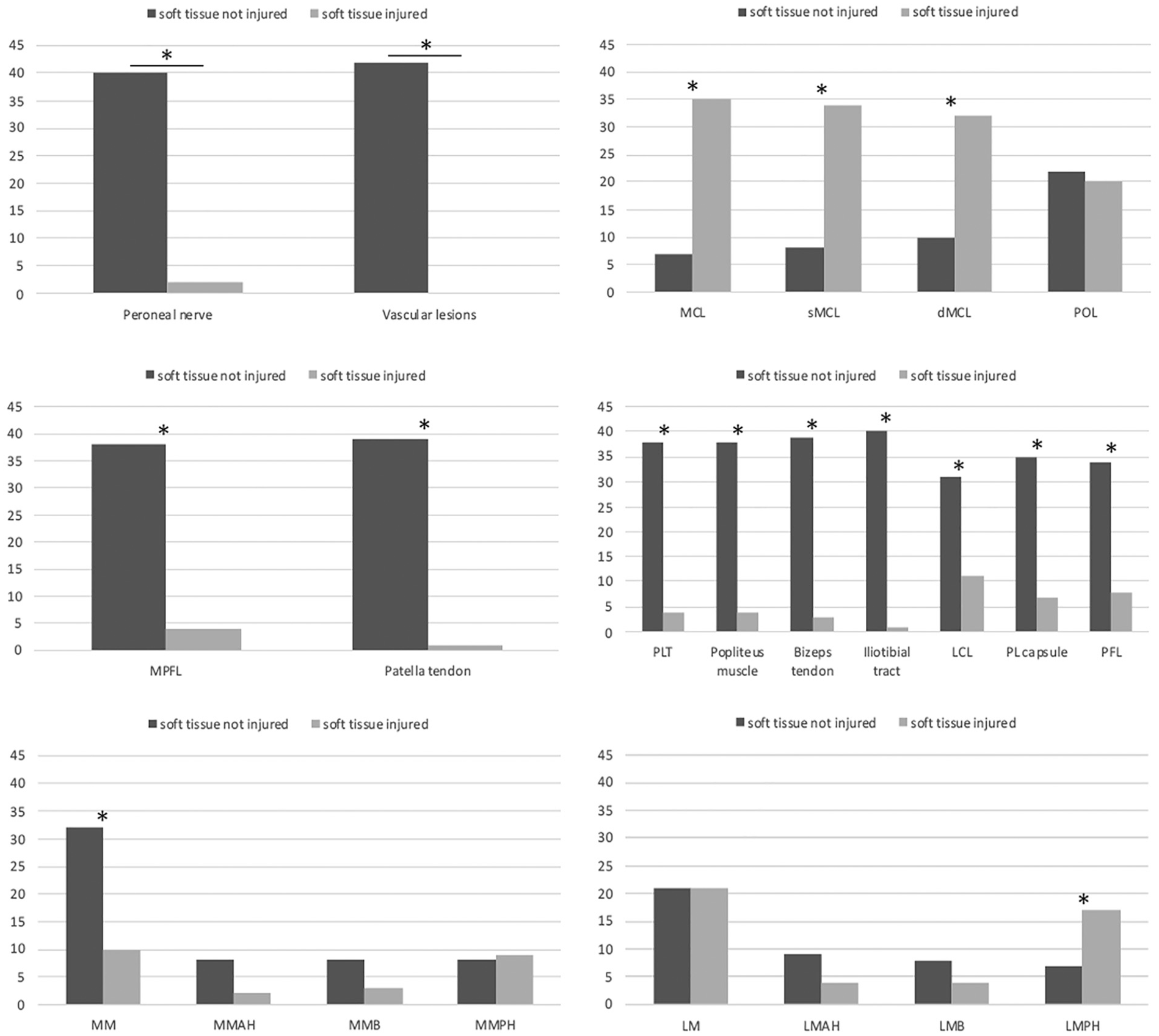
Subgroup analysis of injured and noninjured soft tissue structures in the presence of a posterolateral tibial plateau depression fracture (PLTPF). The asterisk indicates that there was a significant difference between injured and intact soft tissue structures in the presence of a PLTPF. The y-axis shows the number of cases with a PLTPF and an intact or injured soft tissue structure. dMCL, deep medial collateral ligament; LCL, lateral collateral ligament; LM, lateral meniscus; LMAH, lateral meniscus anterior horn; LMB, lateral meniscal body; LMPH, lateral meniscus posterior horn; MCL, medial collateral ligament; MM, medial meniscus; MMAH, medial meniscus anterior horn; MMB, medial meniscal body; MMPH, medial meniscus posterior horn; MPFL, medial patellofemoral ligament; PFL, popliteofibular ligament; PL capsule, posterolateral capsule; PLT, popliteus tendon; POL, posterior oblique ligament; sMCL, superficial medial collateral ligament.
Lateral Femoral Condyle Impaction Fractures
An LFCIF was found in 31 (19.7%) of the cases. There was no significance with respect to age and sex (Table 3). A large prevalence of LFCIFs was observed in Schenck type III medial knee dislocations (Table 4).
Characteristics of Patients for LFCIFs a

Data are shown as No. unless otherwise specified. LFCIF, lateral femoral condyle impaction fracture; PLTPF, posterolateral tibial plateau depression fracture.
Schenck Classification of Knee Dislocations for LFCIFs a

Data are shown as No. LFCIF, lateral femoral condyle impaction fracture.
With respect to concomitant soft tissue injuries, an increased incidence of MCL injuries was detected (P = < .001), comparable with the cases with PLTPFs. With regard to meniscal injuries, a significantly lower prevalence of medial meniscal injuries was detected in cases with LFCIFs (P = .02). There was no association with lateral meniscal injuries. The lateral stabilizers were less frequently injured in the presence of an LFCIF (Figure 4). The simultaneous occurrence of LFCIFs and PLTPFs was observed in 20 cases (12.7%).

Subgroup analysis of injured and noninjured soft tissue structures in the presence of a lateral femoral condyle impaction fracture (LFCIF). The asterisk indicates that there was a significant difference between injured and intact soft tissue structures in the presence of an LFCIF. The y-axis shows the number of cases with an LFCIF and an intact or injured soft tissue structure. dMCL, deep medial collateral ligament; LCL, lateral collateral ligament; LM, lateral meniscus; LMAH, lateral meniscus anterior horn; LMB, lateral meniscal body; LMPH, lateral meniscus posterior horn; MCL, medial collateral ligament; MM, medial meniscus; MMAH, medial meniscus anterior horn; MMB, medial meniscal body; MMPH, medial meniscus posterior horn; MPFL, medial patellofemoral ligament; PL capsule, posterolateral capsule; PLT, popliteus tendon; POL, posterior oblique ligament; sMCL, superficial medial collateral ligament.
For interobserver reliability, good agreement was found according to the assessment of the Cohen kappa, with a 95% confidence interval of 0.929 to 1.000.
Discussion
Our study showed that a PLTPF occurred in 26.8% of cases, and an LFCIF in 19.7% of cases, in the setting of acute knee dislocations. A PLTPF and an LFCIF coexisted as part of an acute knee dislocation in 12.7% of cases. A particularly frequent occurrence was found in Schenck type III medial knee dislocations (PLTPF: 64.3%; LFCIF: 58.1%), as the majority of the cases had an injury more frequently to the deep MCL than to the superficial MCL. However, the medial meniscus was hardly affected, but lesions of the LMPH were frequently observed, especially in cases with a PLTPF (70.3%). Most interestingly, of all knee dislocations with a PLTPF, 26 (61.9%) were rated as high-grade fractures, theoretically requiring a surgical intervention according to Menzdorf et al. 17 To the best of our knowledge, our study is the first to report the incidence of PLTPFs and LFCIFs with a focus on knee dislocations.
PLTPFs are commonly seen in primary ACL ruptures and are an important risk factor for increased rotational instability and impaired postoperative outcomes if left untreated in the clinical setting. 6 Biomechanically, high-grade PLTPFs lead to increased anteroposterior translational instability and increased anterolateral rotational instability, resulting in a so-called Bankart knee. 18 Surgical reduction and fixation during primary ACL reconstruction is safe and provides good outcomes. 17 Hence, the influence of PLTPFs in primary ACL lesions is clinically established, while their effect on multiligament knee injuries with acute knee dislocations in particular is not known to date. However, awareness of the occurrence of PLTPFs and evaluation of their severity in the setting of acute knee dislocations have not been elucidated thus far.
In one of the largest studies analyzing concomitant fractures, in primary ACL injuries, Bernholt et al 4 were able to find a PLTPF in 49.3%, and an LFCIF in 25.9%, of their cases. In contrast to Bernholt et al 4 and in the setting of an acute knee dislocation, involving at least a bicruciate ligament injury, a lower incidence of PLTPFs (26.8%) and of LFCIFs (19.7%) was observed in the current study. In general, this is in line with other studies analyzing multiligament injuries without involvement of the PCL. In a study of 115 primary ACL ruptures, a PLTPF occurred less frequently in patients with an MCL lesion compared with patients without an MCL lesion (12 vs 17, respectively; P = .04). 13 Yet, although PLTPFs may be less frequent in multiligament injuries, specifically in acute knee dislocations, the fracture severity seemed to be higher in knee dislocations. However, despite its lower incidence, the severity of a PLTPF seemed to be associated with the severity of the ligament injury. With respect to reference data in the literature and based on our data, higher grade PLTPFs requiring a surgical intervention were more commonly observed in knee dislocations (61.9%) than in primary ACL injuries (6.1%-11.3%).5,13
According to the literature, LFCIFs and PLTPFs are caused by anterior subluxation with valgus stress and internal rotation of the tibia. 12 The results of this study suggest that the trauma mechanism in our cohort of knee dislocations, especially with involvement of the MCL, must be similar to that in ACL injuries. Because the main stabilizer against valgus stress is the MCL, it is injured significantly more frequently than lateral soft tissue structures such as the LCL.2,24 Nevertheless, the POL, which is a stabilizer against passive internal rotation, was not frequently injured in cases with PLTPFs or LFCIFs in either primary ACL ruptures1,7,24 or in knee dislocations according to our data. However, because the POL stabilizes the knee joint near extension and the MCL mainly in flexion, a trauma mechanism close to slight flexion is to be assumed in the majority of knee dislocations. 29 Porrino et al 21 found that MCL injuries were associated with lateral tibial plateau fractures while analyzing injuries of the knee. The lower rate of LCL ruptures with PLTPFs also supports this theory because ruptures of the LCL involve a varus-like trauma mechanism that somewhat contradicts PLTPFs. 24 This is also supported by the fact that other lateral structures, such as the popliteus tendon, the popliteus muscle, the biceps femoris muscle, the iliotibial band, the posterolateral capsule, and the PFL, were less frequently injured with simultaneous PLTPFs in our study.
In the context of acute knee dislocations with PLTPFs, a significant association with tears of the LMPH was found. This was most likely because PLTPFs were located in the same area. In our study cohort, 35 (22.3%) of the knee dislocations showed an LMPH tear, which is in line with other studies 15 but is higher than for primary ACL ruptures (7%-14%).11,22 However, the highest rate of LMPH tears was still shown in ACL ruptures with concomitant PLTPFs (13.1%). 6 Overall, these findings result in a theory that PLTPFs and LFCIFs are less common but, if present, demonstrate a higher severity when other peripheral ligaments (MCL and/or LCL) are torn in addition to the ACL. A possible explanation could be that in the setting of a primary ACL rupture with an intact MCL and/or LCL, the trauma energy of the subluxation can only partially be compensated by the peripheral ligaments and has to run through bony meniscal structures. Instead, in an acute knee dislocation, the usually high-impact initial trauma energy primarily results in a multiligament injury and less frequently remains “within the joint.” Yet, if the trauma energy is high enough to harm bony structures, then higher grade fractures are more likely, theoretically requiring a surgical intervention. This is supported by the fact that there were only 8 cases of Schenck type IV knee dislocations with a PLTPF compared with 28 type III knee dislocations with a PLTPF in the current study.
Limitations
Limitations of this study are its retrospective design, on the one hand, and the lack of clinical follow-up data, on the other hand. Also, the recommendation for operative treatment was based on the data of Menzdorf et al 17 and was up to the discretion of the surgeon; thus, it may not be generalizable. However, this study represents the largest case series to date on the topic of concomitant bony injuries in the setting of acute knee dislocations.
Conclusion
A PLTPF was observed in one-quarter, and an LFCIF in one-fifth, of acute knee dislocations. They occurred particularly in knee dislocations with MCL ruptures. Almost two-thirds of all PLTPFs presented as high-grade fractures according to the Menzdorf or Bernholt classification, potentially requiring a surgical intervention. Given the relevant effect of high-grade PLTPFs on translational and rotational stability of the knee, their reduction and fixation in the context of acute knee dislocations might be incorporated into an acute treatment strategy.
Footnotes
Final revision submitted January 6, 2025; accepted January 27, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hamburg Ethics Committee (2021-300079-WF).