
Abstract
Background:
There is a paucity of outcomes data on surgical reconstruction for multiligament knee injury (MLKI) in the orthopaedic literature.
Purpose:
To examine functional and return-to-sports (RTS) outcomes and revision rates after single-stage reconstruction for MLKIs in a cohort containing a large proportion of competitive athletes over a 20-year period.
Study Design:
Case series; Level of evidence, 4.
Methods:
We identified all patients at our institution who underwent surgical reconstruction for an anterior cruciate ligament (ACL) or bicruciate (ACL-posterior cruciate ligament) MLKI between 2001 and 2020 and had ≥2 years of postoperative outcome data. Patient-reported outcomes were evaluated using the International Knee Documentation Committee (IKDC) form, a surgical satisfaction survey, and questions about subsequent knee surgery and RTS administered via telephone. Summary statistics for all outcomes data were calculated, and predictors of IKDC scores at follow-up were examined using univariable linear regression.
Results:
Out of 151 patients eligible for this study, outcomes data were collected in 119 patients (79%). The mean follow-up time was 8.3 ± 4.4 years, and the mean IKDC score at follow-up was 79 ± 17. A total of 83 competitive athletes were included; 62 of these athletes attempted to return to preinjury sport. Among the 62 who attempted RTS, 50 (81%) were successful, and 12 were unable to return due to limitations from their surgery. At follow-up, 112 of the overall cohort of 119 patients (94%) were either satisfied or very satisfied with their surgical outcome, and 91% stated the surgery met or exceeded their expectations. In addition, 24% had subsequent ipsilateral knee operations after their index multiligament knee reconstruction. Older age at surgery and female sex were associated with worse IKDC scores at follow-up.
Conclusion:
Despite the severity of the injuries in our cohort, we found high levels of patient-reported function and a high rate of successful RTS in the competitive athletes. Older age and female sex were associated with worse patient-reported knee function at follow-up.
Keywords
Among musculoskeletal injuries necessitating operative management, multiligament knee injuries (MLKIs) are uncommon, often occurring by knee joint subluxation or dislocation, with potentially devastating complications to the knee neurovasculature, structure, and function resulting from the injury and further complications, such as arthrofibrosis, arising after operative treatment.2,26,38,41,43,51,66,69 MLKIs are defined as any combination of injuries to the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), lateral collateral ligament (LCL), and/or structures of the posterolateral corner (PLC), with a cruciate ligament almost always involved.11,39,40,58 When compared with isolated ACL reconstructions, not only are multiligament knee reconstructions much less common, but the complication and revision rates are higher and patient-reported outcomes (PROs) and rates of return-to-sports (RTS) are worse.1,4,39,48,68,70,85
MLKIs can be classified via injury mechanism, including high-energy trauma, such as a motor vehicle accident (MVA), lower-energy mechanisms, which commonly occur in sports, or ultralow-energy mechanism, such as a simple fall in an obese patient.15,84 High-energy trauma has been associated with worse postoperative activity scores. 15 Owing to their complex pathology and overall rarity, MLKIs can prove difficult to manage, and debate in the existing literature focuses on the timing of surgery, graft choice and tensioning sequence, tunnel placement, and the advantages and disadvantages of ligament repair versus reconstruction.21,23,34,52,60-62,74,82 Prior studies have demonstrated surgical intervention within three weeks of injury is associated with significant improvements in Lysholm scores and with no significant increase in postoperative complication rates.34,51,74 Two recent systematic reviews and meta-analyses demonstrated no significant differences in revision rates, complications, joint laxity, strength, range of motion, or patient-reported functional outcomes between early and delayed surgery for MLKIs.57,82 Further research has suggested that, by staging repair, knee biomechanics remain disrupted, leading to nonphysiologic loading of the reconstruction until staged reconstruction is complete, potentially leading to increased degenerative changes within the knee joint. 65 Clinical decision-making regarding surgical timing may be further affected by neurovascular status, reduction stability, and other systemic injuries requiring treatment more urgently. 64 The decision to repair versus reconstruct a ligament depends on a variety of factors, including specific ligament(s) involved, injury severity, and injury chronicity.29,35,44,45,53 A hybrid technique combining ACL reconstruction with suture-augmented repair of other involved ligaments has demonstrated potential in generating good outcomes6,23,31; however, patient outcomes may vary with different surgical approaches, as well as other cohort-specific factors including age, sex, and body mass index (BMI).20,67 Although debate regarding surgical staging continues in these areas, past work has supported surgical intervention in a single-stage approach, as opposed to nonoperative management or a multistage surgical approach. 50
While early, midterm, and long-term outcomes studies as well as complementary systematic reviews and meta-analyses regarding the operative management of MLKIs exist in the literature, many of these studies have relatively small sample sizes that are heterogeneous, with a minimal or absent subpopulation of competitive athletes. ¶ The purpose of the current study was to analyze surgical outcomes, including patient-reported measures, RTS rates in competitive athletes, and postoperative complications, after operative reconstruction of ACL and bicruciate-based MLKIs over a 20-year period at a single institution, in a patient population including a large subpopulation of competitive athletes. We hypothesized that, after acute, single-stage surgical treatment of ACL and bicruciate-based MLKIs, (1) we would find high levels of knee-related function at follow-up, including the ability to RTS at preinjury level and low rates of postoperative complications, and (2) age, sex, and follow-up time would be significantly associated with knee-related function at follow-up.
Methods
Participants
Institutional review board approval was obtained for the study protocol. We utilized a prospectively collected operative database to retrospectively identify potential study participants based on diagnosis and procedure performed between January 2001 and August 2020. The electronic health records (EHRs) of potential study participants were then reviewed. Potential participants met inclusion criteria if they (1) underwent ACL reconstruction plus reconstruction or repair of an additional knee ligament (PCL, MCL, LCL, and/or any structures of the PLC) and (2) had at least 2 years of follow-up. We excluded patients if they had (1) absent or incomplete medical records or (2) index procedures performed by surgeons no longer associated with our institution due to inability to complete accurate follow-up. ACL-sparing MLKIs were excluded from this study to focus on outcomes of ACL reconstruction in the context of multiligament reconstructions and better understand the outcomes associated with the unique injury patterns seen with ACL-based MLKI. 91
Demographics and Injury Characteristics
Demographic and clinical data collected from the EHR included sex, age at surgery, laterality of injury, BMI, prior ipsilateral knee surgery and type, whether a competitive athlete at the time of injury and surgery, primary sport and level of competition if a competitive athlete, injury setting, and time from initial injury to operative treatment for the MLKI (categorized as acute or chronic). Surgery timing was categorized as acute if the index procedure at our institution occurred <6 weeks from the date of injury and chronic if operative treatment occurred ≥6 weeks after initial injury.24,50 Prior ipsilateral surgery categories included none, ligamentous, vascular, meniscal/articular, trauma, combination, or other. Patients were deemed competitive athletes if they participated in competition for a sport at the time of injury and not exclusively for leisure. Athletic status was gathered from clinical intake forms and/or clinical notes and was further confirmed during follow-up postoperative data collection. Injury setting categories included athletic, nonathletic, and MVA.
Operative Data
Operative data collected from the EHR included the knee ligaments that were surgically treated, with the LCL and structures of the PLC being grouped into a single category (LCL/PLC) for lateral-sided knee injuries. For each ligament involved, the operative technique, graft type, and graft source were recorded. ACL reconstruction was categorized as primary, first revision, or second revision. In the setting of LCL/PLC injuries, presence of peroneal nerve injury was determined based the presence of weakness and/or decreased dermatomal sensation on preoperative physical examination. Additional procedures not involving knee ligaments/structures of the PLC were categorized as meniscal, chondral, both, other, or complication.
Surgical Management
In each case, operative management was tailored to the unique combination of injuries present, with a focus on restoring normal anatomy and kinematics. Exact techniques used to repair or reconstruct each ligament are described in the following. Any concomitant ligamentous, chondral, or meniscal injuries were addressed during the same surgery. In the event a patient had severely limited knee range of motion preoperatively or if the surgeon determined that surgical delay for swelling control was needed, the patient was referred to preoperative physical therapy. While similar surgical techniques were utilized by all surgeons throughout the study, surgical techniques inevitably evolved throughout the duration of the study.
ACL Reconstruction
ACL reconstructions were preferentially performed with a bone-patellar tendon-bone autograft as described previously. 3 The femoral tunnel was created using a transtibial technique, followed by transtibial graft passage, fixation with femoral interference screw, and then tibial interference screw fixation. Final graft tensioning was performed with the knee in full extension.
PCL Reconstruction
PCL injuries were treated via reconstruction or an augmented repair using a quadrupled hamstring autograft in most cases, utilizing a transtibial technique, tibial interference screw, and suspensory femoral fixation. 55 The final graft tensioning in the PCL reconstruction was typically performed with the knee in 90° of flexion. Allograft was utilized in some cases at the discretion of the surgeon.
MCL Repair/Reconstruction
MCL injuries were all primarily repaired to restore stability and overall function. Criteria for MCL repair included complete meniscotibial coronary ligament tear from the tibia with synovial fluid extravasation, complete proximal MCL tear with the presence of a capsular tear or Stener lesion, MCL flipped into the joint space, or persistent laxity after cruciate reconstruction with a capsular injury present.
LCL/PLC Repair/Reconstruction
LCL/PLC injuries were repaired acutely or reconstructed using a hamstring or Achilles tendon allograft in most cases using the techniques described by Clancy et al, 10 Dugas et al, 17 and LaPrade. 49 Graft selection was dependent on the combination of ligaments injured and grafts available for each patient. In the event of PLC injury without LCL disruption, either semitendinosus or gracilis were used in preparing the graft. If both the PLC and LCL were injured, the semitendinosus was used in the PLC reconstruction, and the gracilis was used for the LCL reconstruction. For combined PLC and PCL injuries, the quadrupled hamstring autograft was used to reconstruct the PCL and a hamstring allograft was used to reconstruct the PLC. The peroneal nerve was identified and released in each case of lateral ligament repair or reconstruction. Lateral meniscus injuries were typically repaired prior to PLC repair. The sequence of injuries addressed varied based on injuries present. Final tensioning sequence typically followed this order: PCL at 90° of flexion, ACL/MCL in full extension, and finally PLC. Final tensioning of the PLC was performed with the knee at 25° to 30° of flexion with valgus and internal rotation force.
Postoperative Rehabilitation
Rehabilitation protocol specifics and intervention timing evolved throughout the duration of this study to optimize recovery; however, overall goals remained consistent. Immediately after surgery, patients were placed in a drop lock brace set at 0° or 10° of flexion (if LCL/PLC were injured) and permitted to be <50% weightbearing using 2 crutches, with range of motion permitted between 0° and 45°. By postoperative day 5, patients progressed to 90° of flexion and approximately 100° of flexion at postoperative day 7. At approximately 12 days postoperatively, patients progressed to 75% weightbearing status. Patients with LCL/PLC involvement were allowed to progress to full extension at weeks 3 to 4. Between weeks 6 and 8 (depending on severity of injury), patients progressed to full weightbearing and were provided a functional ACL/PCL brace. General goals of early to midstage rehabilitation included restoring knee range of motion as well as regaining lower extremity strength (quadriceps, hamstring, hip) and neuromuscular control. At 6 to 8 months postoperatively, patients were permitted to gradually re-enter sport-specific activity, including running, if they had a satisfactory clinical examination, satisfactory isokinetic testing, including demonstrating quadriceps strength of >80% of the contralateral quadriceps, and a functional hop test of >75% of the contralateral leg. For most athletes, return to practice occurred at approximately 8 months postoperatively, and return to competition occurred at approximately 10 months.
Subsequent Operative Procedures and PRO Data Collection
Data regarding subsequent ipsilateral knee surgeries at our institution were collected during our initial chart review of potential participants. Follow-up data collection was performed via telephone calls, and patients were asked if they had any subsequent surgical procedures performed on their ipsilateral knee outside of our institution. For patients with confirmed subsequent ipsilateral knee operations, procedures were categorized as chondral, arthritic/total knee arthroplasty, ligamentous, arthrofibrosis, meniscal/chondral, complication (eg, postoperative infection), or hardware removal.
In addition to collecting data related to subsequent procedures during follow-up telephone calls, we collected PRO data using the International Knee Documentation Committee (IKDC) subjective knee form 37 as well as an institutional-specific surgical satisfaction survey and an institutional-specific RTS assessment. The IKDC is a knee-specific questionnaire that includes 18 questions evaluating pain, swelling, stiffness, instability, and activity limitations. Scores range from 0 to 100, with higher scores indicating better knee function; there is an additional subsection evaluating changes in overall knee function before and after injury. The IKDC has been shown to be valid, reliable, and responsive to changes in knee function over time in individuals after knee injuries and surgeries. 37 Both the institution-specific surgical satisfaction survey and the RTS assessment contained categorical-level questions related to satisfaction and RTS, respectively, and were not numerically scored. The full RTS assessment is included as Supplementary Material (available online).
Statistical Analysis
We calculated summary statistics (means and standard deviations or counts and percentages) for baseline and/or follow-up demographic, clinical, surgical, and outcomes data. Key baseline demographic, clinical, and surgical variables were compared between patients with successful follow-up (ie, the study cohort) and those with incomplete follow-up using independent t tests (continuous data) and chi-square tests (categorical data). In addition, as secondary analyses, the IKDC scores at follow-up and the rate of RTS at preinjury level (in competitive athletes) were compared in the study cohort between (1) patients with 2-ligament versus >2-ligament MLKI using independent t tests and (2) patients with ACL- only (no PCL involvement) versus bicruciate MLKI using chi-square tests. We also examined the association between preinjury demographic and injury variables (age, BMI, and prior ipsilateral knee surgery) and IKDC scores at follow-up using univariable linear regression models. Lastly, we calculated the baseline demographic, clinical, and surgical variables for the subcohort of competitive athletes and compared IKDC scores at follow-up between the competitive athletes and the nonathletes using independent t tests. For all analyses, we considered P values of <.05 to be statistically significant. All statistical analyses were performed using SPSS version 28.0 (IBM Corp).
Results
Cohort Characteristics
Of the 151 patients who met the study eligibility criteria, we successfully contacted 119 (79%) patients who had a minimum 2-year follow-up (mean follow-up time, 8.3 ± 4.4 years) (Figure 1).
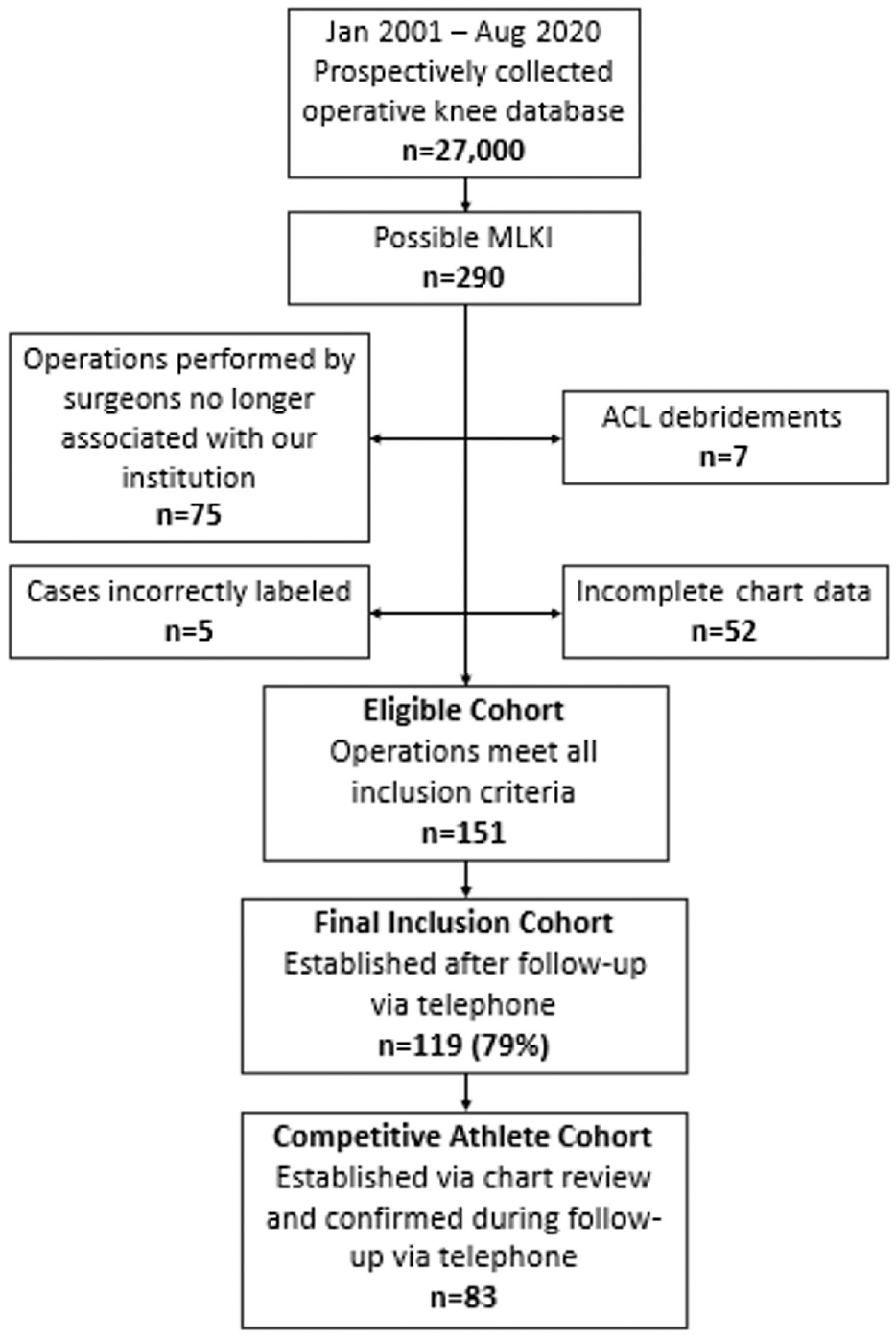
Flowchart of the cohort selection process. ACL, anterior cruciate ligament; MLKI, multiligament knee injury.
Patients with successful follow-up (n = 119) did not differ from patients with unsuccessful follow-up (n = 32) in age, BMI, percentage of competitive athletes, percentage of patients with prior ipsilateral knee surgery, or percentage of patients with >2 surgically treated ligaments. There was a significantly greater percentage of female patients in the successful versus the unsuccessful follow-up group (20% versus 3%; P = .02). Full comparisons of demographic data between the successful and unsuccessful follow-up groups are presented in Appendix Table A1.
The demographic and clinical data of the of the 119 patients who completed follow-up and were included in the study are shown in Table 1. There were 95 (80%) male and 24 (20%) female patients, with a mean age at the time of surgery of 24.1 ± 10.8 years; 107 (90%) of the patients were treated acutely (<6 weeks from their injury), with an average time from injury to surgery of 14.4 days. During their index procedure, 82 patients (69%) had 2 ligaments treated, while 37 patients (31%) had >2 ligaments treated. Other concomitant procedures were performed in 67 (56%) of the 119 patients who completed follow-up, with the treatment of isolated meniscal lesions being the most common concomitant procedure (58/67; 87%). Lateral meniscus involvement was more common, with 50 of 67 (75%) procedures addressing some form of lateral meniscus injury. These lateral meniscus injuries were treated via repair in 26 cases, lateral root repair in 1 case, and partial lateral meniscectomy in 23 cases. Medial meniscus injuries were treated via repair in 12 cases, medial root repair in 5 cases, meniscectomy in 3 cases, and meniscocapsular repair in 3 cases, with some cases involving both medial and lateral menisci. Isolated chondral lesions were addressed in 3 cases with concomitant procedures, and both meniscal and chondral lesions were addressed in 2 (2%) of those with concomitant procedures. Of the 47 patients with lateral knee injuries, 11 (23%) presented with evidence of peroneal nerve involvement on physical examination, including 7 with both motor and sensory deficits, 3 with sensory deficits alone, and 1 patient with only a motor deficit. One patient, whose injury occurred by an MVA causing an isolated bicruciate tear, had a history of popliteal artery reconstruction.
Demographic and Clinical Data for the Study Cohort (N = 119) a

Data are presented as mean ± SD (range) or n (%) unless otherwise indicated. ACL, anterior cruciate ligament; allo, allograft; aug, augmentation; auto, autograft; combo, combination; debride, debridement; HT, hamstring; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner; PTG, patellar tendon graft; recon, reconstruction; ST, semitendinosus; TA, tibialis anterior.
Low energy: injury occurring by activities of daily living, injury during sports, or fall from standing. High energy: injury occurring by motor vehicle accident or fall from a substantial height.
Patient-Reported Outcomes
The mean total IKDC score at follow-up was 79 ± 17, and the mean current knee function, an item in the IKDC questionnaire, was 7.3 ± 2.1 (out of a maximum of 10) (Table 2). Regarding satisfaction, 112 (94%) were either satisfied or very satisfied with their index procedure, and 108 (91%) felt their surgery either met or exceeded their expectations (Table 2).
Outcomes and RTS Data for the Study Cohort (N = 119) a
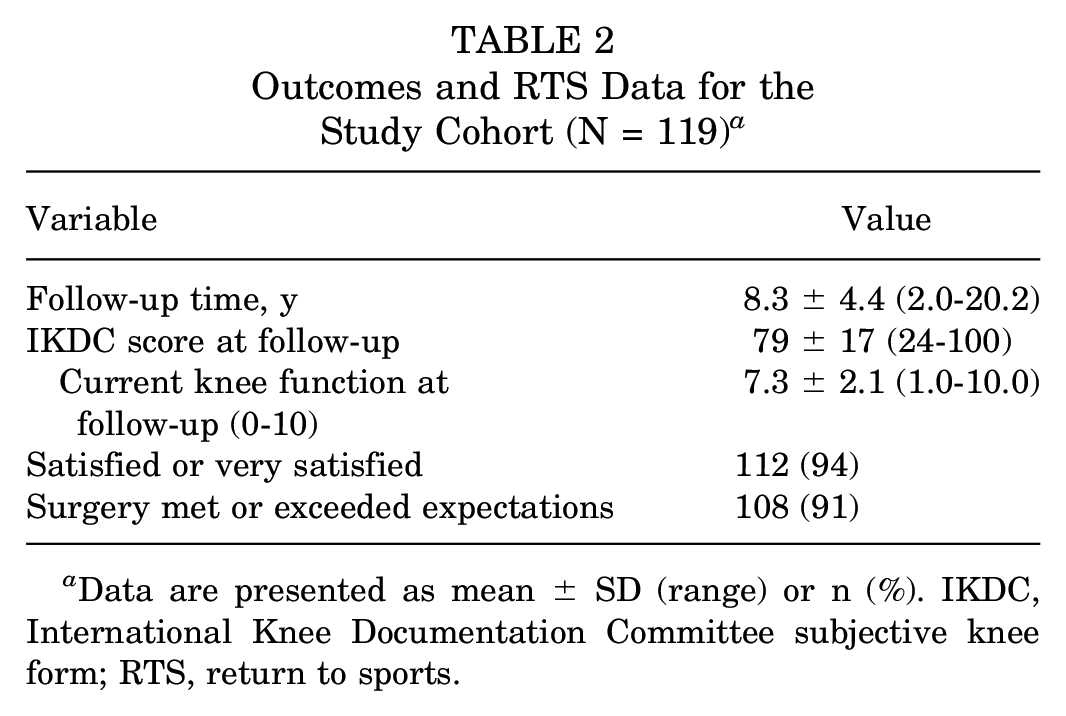
Data are presented as mean ± SD (range) or n (%). IKDC, International Knee Documentation Committee subjective knee form; RTS, return to sports.
Complications and Failures
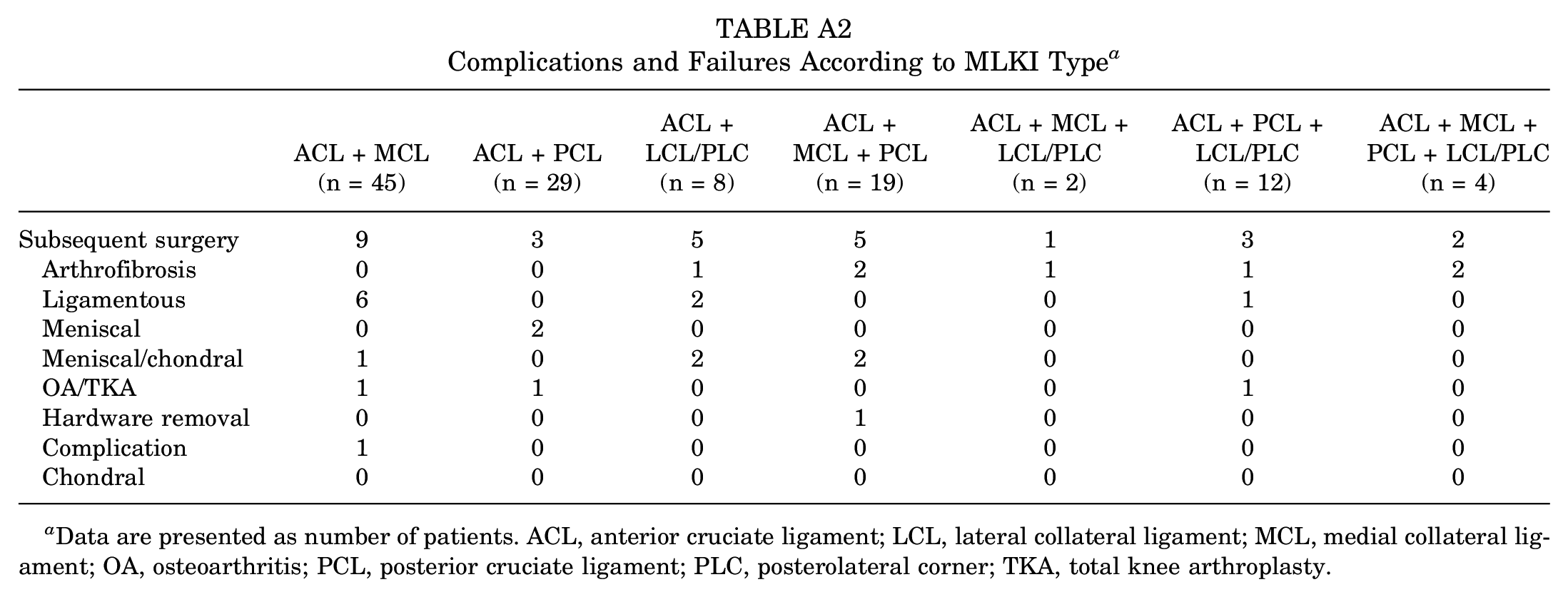
Of the 119 study patients, 28 patients (24%) required subsequent ipsilateral knee operations, with 9 (8%) procedures to address ligamentous failure, 8 of which were performed at our institution. Of these 8 procedures for ligamentous failure at our institution, 6 procedures addressed failure of the ACL reconstruction, 1 revision addressed PCL laxity, and 1 addressed anterolateral ligament injury. Ligament failure was most prevalent in patients that underwent ACL reconstruction plus MCL repair, with 6 (13%) of these 45 patients requiring revision surgery to address ligament failure and 3 (7%) requiring subsequent procedures to address other issues. In addition, 7 patients (6%) underwent a mixture of manipulation under anesthesia and lysis of adhesion for postoperative arthrofibrosis. Of these 7 patients, 5 patients underwent bicruciate reconstructions, and 5 had involvement of the PLC. Two patients converted to total knee arthroplasty at 10.4 and 14.2 years postoperatively (43.8 and 59.5 years old at time of total knee arthroplasty, respectively). Complete details regarding complications and failures categorized by MLKI type can be found in Appendix Table A2.
In the subcohort of patients with evidence of peroneal nerve involvement after their injury, we noted similar IKDC scores (80.11 ± 13.1) and similar RTS rates (6/8 athletes; 75%) after operative treatment of their MLKI. Of the 11 patients with peroneal nerve involvement at the time of injury, only 1 had a subsequent surgical procedure, undergoing posterior tibial tendon transfer for chronic foot drop.
When the study cohort was divided into patients with 2-ligament (n = 82) versus >2-ligament (n = 37) MLKI, the IKDC scores were not significantly different at follow-up (2-ligament: 87 ± 17; >2-ligament: 75 ± 17; P = .11). However, when categorized into patients with ACL-only (n = 76) versus bicruciate (n = 43) MLKI, significantly higher IKDC scores were seen in those with ACL-only injuries at follow-up (ACL-only: 82 ± 17; bicruciate: 75 ± 17; P = .03). Older age at surgery (R2 = 7.1%; P < .01) and female sex (R2 = 4.5%; P = .02) were associated with worse IKDC scores at follow-up. Prior ipsilateral knee surgery was not significantly associated with IKDC scores at follow-up; however, a trend was found (R2 = 2.9%; P = .06).
Competitive Athletes and RTS Outcomes
Of the 119 patients in the study cohort, 83 (70%) were deemed competitive athletes based on initial chart review, with athletic status at the time of injury and surgery confirmed at follow-up. American football was the primary sport for most of these athletes (n = 55; 66%), followed by soccer (n = 6; 7%), basketball (n = 5; 6%), and wrestling (n = 4; 5%). Table 3 presents the demographic and clinical data in the subcohort of competitive athletes.
Demographic and Clinical Data for the Subcohort of Competitive Athletes (n = 83) a

Data are presented as mean ± SD (range) or n (%) unless otherwise indicated. ACL, anterior cruciate ligament; allo, allograft; aug, augmentation; auto, autograft; combo, combination; HT, hamstring; LCL, lateral collateral ligament; MCL, medial collateral ligament; MVA, motor vehicle accident; PCL, posterior cruciate ligament; PLC, posterolateral corner; PTG, patellar tendon graft; rec, recreational; recon, reconstruction; ST, semitendinosus; TA, tibialis anterior.
The outcomes and RTS data for the competitive athletes are listed in Table 4. There were 77 athletes (93%) who were either satisfied or very satisfied with their index procedure, and 75 (90%) reported that the procedure met or exceeded their expectations. Overall, 62 competitive athletes attempted to return to their preinjury sport, and 50 (81%) were able to successfully RTS. Of those who were unable to return, 12 athletes reported limitations specifically from their surgery. When considering all reasons for unsuccessful RTS (eg, insufficient talent for next level or personal interest), 60% of athletes were able to RTS at their previous level. Lastly, of the 50 patients who returned to competitive sports participation, 32 (64%) felt their performance was about the same or improved compared with their performance prior to injury. Competitive athletes demonstrated significantly higher total IKDC scores compared to nonathletes (athletes: 82.4 ± 15.8; nonathletes: 71.1 ± 18.6; P < .01).
Outcomes and RTS Data for the Competitive Athletes (n = 83) a

Data are presented as mean ± SD (range) or n (%). IKDC, International Knee Documentation Committee subjective knee form; RTS, return to sports.
Discussion
In this study, we have demonstrated that most patients undergoing single-stage MLKI reconstruction have satisfactory functional outcomes, and most competitive athletes are able to successfully return to their preinjury sport at a similar level of competition. However, RTS rates are not on par with those seen after isolated ACL reconstruction, reflecting the greater extent of injury and more difficult recovery.33,42,50,59
Of the 119 study patients, 76% did not require additional ipsilateral surgical intervention. Our repeat surgery rate of 24% was similar to the repeat surgery rates previously reported, ranging from 9% to 39%.9,13,76 ACL reconstruction graft failure was the most common complication observed in our cohort, followed by arthrofibrosis. Our rate of ACL reconstruction graft failure (8%) is similar to the rate of graft failure and subsequent revision reported previously (7%). 70 Further, none of our LCL/PLC repairs or reconstructions required revision. Similar outcomes studies evaluating PLC injuries in the setting of MLKI have presented PLC repair failure rates of 37% and PLC reconstruction failure rates of 9%, with mean IKDC scores ranging from 60 to 73.1 ± 25.8 after surgical treatment.75,88 The rate of arthrofibrosis presented in this study (6%) is comparable to or lower than those described elsewhere in the literature, ranging up to 20%.15,75 Similar studies regarding sports-related MLKI reported that arthrofibrosis occurred in 9% of single-stage MLKI reconstructions and in 18% of variably staged MLKI reconstructions.9,50 Arthrofibrosis has also been reported to occur at higher rates after PCL reconstruction, a trend we also observed, as 5 of 7 total cases of arthrofibrosis were noted in patients who had a PCL reconstruction as part of their operative MLKI treatment.2,80 Interestingly, we observed no significant difference in arthrofibrosis development after medial- or lateral-sided injuries. While medial- sided injuries are more typically associated with postoperative stiffness and arthrofibrosis, MCL involvement was not found to be associated with development of arthrofibrosis after acute, single-stage operative management of MLKI.50,56
The mean IKDC score for the study cohort was found to be 79 ± 17, comparable to IKDC scores reported in a previous study. 83 Wajsfisz and colleagues 83 reported a mean IKDC score of 73 after surgical treatment of MLKIs involving the PLC, and Heitmann and colleagues 31 reported an average score of 76 ± 15 at 1 year after hybrid repair and reconstruction of bicruciate MLKIs. We did not observe a significant difference in IKDC scores between 2-ligament and >2-ligament MLKIs. Although previous work from Cook and colleagues 13 found associated poorer outcomes with increasing number of injured and surgically treated ligaments, other studies have similarly found no significant difference in outcomes based on number of ligaments injured and subsequently addressed.5,81 However, we found that MLKIs with bicruciate involvement had significantly worse IKDC scores than those with an ACL-based MLKI without PCL injury. This finding is supported by a similar previous studyies, which reported both worse objective clinical findings (such as deficits in range of motion) and worse PROs in patients treated for a bicruciate MLKI when compared with patients with involvement of only one cruciate ligament. 7
When examining clinical or demographic factors associated with follow-up IKDC scores, our study found that older age at surgery and female sex were associated with poorer scores. Similar associations are seen throughout the existing MLKI literature. Specifically, older age at surgery has been linked with poorer outcomes after both MLKI and isolated ACL reconstruction. 27 In addition, female sex has been associated with poorer self-reported postoperative outcomes after MLKI and isolated ACL reconstruction in prior studies.47,78 The consistent association between female sex and poorer outcomes across a variety of procedures suggest that further research is needed to understand the underlying cause of these outcomes and develop new strategies to improve outcomes of female patients.
In this cohort, MLKIs occurred via low-energy injury mechanism (ie, activities of daily living, injury during sports, or fall from standing) in the majority (94%) of cases. Multiple studies,18,22 including a meta-analysis, 15 have suggested that patients with high-energy injury mechanisms (ie, MVA or fall from a substantial height) tend to have lower PRO scores. In addition, high-energy injuries are more likely to present with concomitant injuries requiring intervention, such as fracture, head trauma, or vascular injury. Management of concomitant injuries, especially in the setting of polytrauma, can alter the time to surgical management of MLKI, how surgical reconstruction is staged, what surgical procedures are performed, and postoperative rehabilitation.14,22 Further, increasing severity of injury is associated with increasing mortality, and patients with MLKI from high-energy injuries may not survive their injuries or be stable enough to undergo reconstruction. 12 The postoperative outcomes reported in this study are not generalizable to all patients with high-energy trauma, especially patients with numerous, concomitant nonorthopaedic injuries; however, we feel that characterization of outcomes for low-energy MLKIs are important, given that many of these injuries occur in young athletes with intention to RTS and/or prior level of activity.
Our study is unique in that it presents RTS data for a large number of athletes actively participating in competitive sports at the time of their injury that necessitated a single-stage MLKI reconstruction. We found that, overall and for all reasons, 60% of athletes returned to preinjury level of competitive sports. Notably, reasons outside of surgical treatment of their MLKI, including graduating from the current level of play and not being talented enough to continue at the next level and nonorthopaedic medical concerns, influenced the decision of many athletes who did not RTS. Our RTS rate was similar to rates reported in other large studies and meta-analyses, which ranged from 0% to 89%, and further supports operative management for MLKIs.4,9,19,20,86 A prior meta-analysis evaluating the efficacy of nonoperative treatment showed no significant differences in RTS or return-to-preinjury employment in patients managed nonoperatively compared with those treated operatively but consistently showed lower knee function and PRO scores after nonoperative management. 16 Studies reporting higher RTS rates enrolled fewer participants or studied small cohorts of only elite/professional athletes.4,9,33
We also found that competitive athletes had higher postoperative IKDC scores when compared with nonathletes. These findings are interesting considering that, in prior studies, competitive athletes have been found to be less likely to RTS, despite having higher function assessed via questionnaire scores than their nonathlete peers.19,20,33 However, in our cohort of athletes, there was a lower proportion of bicruciate involvement than in the nonathlete cohort, which could potentially contribute to the difference in outcomes observed. In prior work reporting longitudinal outcomes after operative management of ACL-based MLKIs occurring in sports, data were reported from small cohorts of elite athletes or from larger cohorts of patients participating in sports at a wide range of levels, including a large proportion of recreational athletes.4,9,50 We argue that these reported surgical outcomes may not be generalizable to the outcomes of competitive athletes.4,33,50 The injuries incurred by participants in recreational sports and expectations of postoperative function differ from those of competitive athletes. Notably, the most similar long-term outcomes study by Borque and colleagues 9 included only elite athletes and lacked outcomes data on American football and basketball athletes, making it less applicable to athletes competing in popular American sports at the most common levels of competition. Most athletes in our study competed at the high school or college level, which represent the most common levels of competition, with only a fraction of athletes continuing from high school to college and even fewer advancing to the professional level. Our study may have wider prognostic utility due to its larger sample size and inclusion of athletes actively competing in a variety of sports.
Limitations
This study has several limitations. First, there was a lack of baseline, preoperative data, which limited our ability to provide definitive comparisons of changes in function from before to after surgery. Second, our study was affected by several forms of bias inherent to collecting PROs, including recall bias in our RTS surveys, which may have been exacerbated by prolonged follow-up periods, as well as confirmation bias in our surgical satisfaction questionnaire. Further, patients who were dissatisfied with their procedures may have been less likely to participate in ongoing research. Whereas these biases are inherent to our case series study design, the instruments utilized in this study were valid and designed to reduce bias as much as possible. In addition, patients whose procedures were performed by surgeons no longer associated with the host institution were excluded from participation in an attempt to minimize variation in follow-up; however, this reduced the number of cases eligible for inclusion in this study, introducing another source of limitation. This study also did not contain radiographic follow-up data, thus preventing us from evaluating long-term joint health. Further, we lacked clinical follow-up data such as physical examination findings, preventing us from making conclusions regarding objective measures such as knee range of motion or joint stability. However, the IKDC evaluates patients’ perceptions of their knee function, including questions related to symptoms, such as stability issues or stiffness.
Another limitation relates to our exclusion criteria. Because we excluded patients with ACL-sparing MLKIs and nonoperatively treated MLKIs, the results of this study are not universally generalizable to all MLKIs. Our cohort also contains little data on MLKIs incurred through high-energy or ultralow-energy injury mechanisms, further limiting generalizability. Although the sample size of this study was relatively small, it represents one of the largest MLKI outcome studies at present. Last, a number of patients who were historically treated at our institution were unable to have their eligibility status assessed, as their paper medical records were discarded and not included in our current EHR. Although these limitations exist, we believe this study has clinical relevance in further developing our understanding of functional outcomes after MLKI as well as better understanding which preoperative factors and injury characteristics may be associated with poorer outcomes. Future studies will aim to further characterize the factors associated with long-term outcomes and RTS success, to help develop and optimize surgical and rehabilitation treatment approaches for both athletes and nonathletes.
Conclusion
In this study, acute, single-stage reconstruction of MLKIs resulted in low rates of postoperative complications, high levels of patient-reported function evaluated at a minimum 2-year follow-up, and a high rate of successful RTS in competitive athletes. Older age at time of surgery and female sex were associated with worse longitudinal outcomes.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241266619 – Supplemental material for Outcomes of Surgical Treatment for Multiligament Knee Injuries in a Cohort Including Competitive Athletes With Long-Term Follow-Up
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241266619 for Outcomes of Surgical Treatment for Multiligament Knee Injuries in a Cohort Including Competitive Athletes With Long-Term Follow-Up by Eric A. Mussell, Anna E. Crawford, Matthew P. Ithurburn, Branum O. Layton, Glenn S. Fleisig, Marcus A. Rothermich, Benton A. Emblom, Michael K. Ryan, Jeffrey R. Dugas, James R. Andrews and E. Lyle Cain in Orthopaedic Journal of Sports Medicine
Footnotes
Appendix
Complications and Failures According to MLKI Type a
| ACL + MCL |
ACL + PCL |
ACL + LCL/PLC |
ACL + MCL + PCL |
ACL + MCL + LCL/PLC |
ACL + PCL + LCL/PLC |
ACL + MCL + PCL + LCL/PLC |
|
|---|---|---|---|---|---|---|---|
| Subsequent surgery | 9 | 3 | 5 | 5 | 1 | 3 | 2 |
| Arthrofibrosis | 0 | 0 | 1 | 2 | 1 | 1 | 2 |
| Ligamentous | 6 | 0 | 2 | 0 | 0 | 1 | 0 |
| Meniscal | 0 | 2 | 0 | 0 | 0 | 0 | 0 |
| Meniscal/chondral | 1 | 0 | 2 | 2 | 0 | 0 | 0 |
| OA/TKA | 1 | 1 | 0 | 0 | 0 | 1 | 0 |
| Hardware removal | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| Complication | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Chondral | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Data are presented as number of patients. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; OA, osteoarthritis; PCL, posterior cruciate ligament; PLC, posterolateral corner; TKA, total knee arthroplasty.
Final revision submitted January 26, 2024; accepted February 13, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.A.R. has received education payments from Arthrex, Smith + Nephew, and Zimmer Biomet; consulting fees from Zimmer Biomet; and nonconsulting fees from Arthrex. B.A.E. has received consulting fees, nonconsulting fees, and royalties from Arthrex. M.K.R. has received grant support from Arthrex; education payments from Arthrex, DJO, Fones Marketing Management, and Smith & Nephew; consulting fees and nonconsulting fees from Arthrex and Zimmer Biomet; and hospitality payments from Linvatec and Prime Surgical. J.R.D. has received consulting fees from Arthrex, Bioventus, DJO, Royal Biologics, and Smith + Nephew; nonconsulting fees from Arthrex; royalties from Arthrex and In2Bones; and hospitality payments from Stryker. J.R.A. has received nonconsulting fees from Arthrex. E.L.C. has received education payments from Prime Surgical and Zimmer Biomet; consulting fees from Arthrex, DJO, Smith + Nephew, and Zimmer Biomet; nonconsulting fees from Arthrex, Medical Device Business Services, and Smith + Nephew; royalties from Arthrex; and hospitality payments from Encore Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from SterlingIRB (ref No. 9023-ELCain).
¶
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.