
Abstract

Keywords
Knee dislocations are uncommon and occur with a reported incidence of less than 0.02% of all orthopaedic injuries. These injuries are defined by complete disruption of the integrity of the tibiofemoral articulation. 27 They are challenging injuries to manage and are associated with the risk of potentially devastating immediate and short-term complications, including popliteal artery injuries, common peroneal nerve injuries, acute compartment syndrome, and deep venous thrombosis, and controversy still exists regarding their optimal treatment. 19,35,39 Despite the severity of these injuries, a recent systematic review has demonstrated that some level of sport participation is possible after multiligament knee injuries (MLKIs) for more than half of patients, but returning to preinjury levels of sport after surgical treatment is low, at just 22% to 33%. 11,12,16
Bilateral knee dislocations occur even less frequently than unilateral injuries, and the literature contains sporadic case reports only. 2,10,18,24,26,30,36 In view of the guarded prognosis of unilateral knee dislocations with respect to returning to preinjury levels of sport, it could be assumed that the results after bilateral knee dislocations would be considerably less favorable. To our knowledge, successful return to preinjury levels of sport in an elite athlete after bilateral knee dislocations has not previously been reported.
Case Presentation
Patient consent was obtained for this case report. A 25-year-old world-class downhill skier sustained bilateral knee dislocations after a fall at a speed of approximately 120 km/h during an international competition in January 2017. He fell as he was making a curve and collided against the track protection fence. He was transported to a local hospital, where computed tomography angiography was performed to exclude arterial injuries. Both knee dislocations were reduced approximately 1 hour after the accident. No neurological deficit was detected on physical examination. Plain magnetic resonance imaging (Figures 1 and 2) was performed, and applying the classification described by Schenck, 33 the right knee was attributed a KD-V grade, which consists in multiligamentous injury with periarticular fracture, and the left knee was attributed a KD-IV grade, with an injury of ACL, PCL, LCL, and MCL.
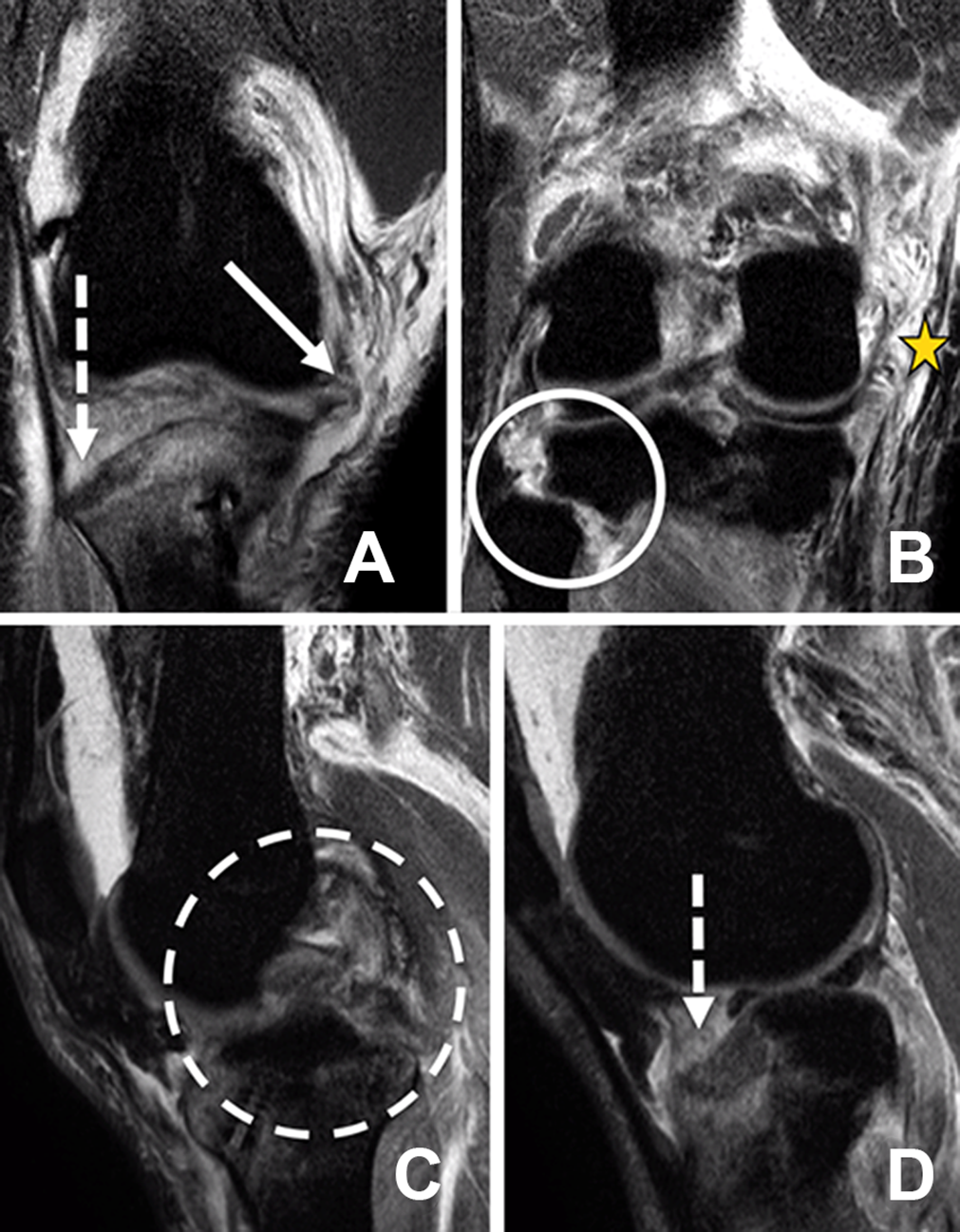
Magnetic resonance imaging of the right knee showing a (A) medial meniscal avulsion (solid arrow), and fracture of the lateral tibial plateau (dashed arrow); (B) complete rupture of the medial collateral ligament/posterior oblique ligament (star) and proximal tibiofibular dislocation (circle); (C) bicruciate rupture (dashed circle); and (D) fracture of the lateral tibial plateau (dashed arrow).

Magnetic resonance imaging of the left knee demonstrating a complete medial collateral ligament/posterior oblique ligament tear (star), bucket-handle tear of the medial meniscus (circle), and bicruciate rupture (dashed circle).
A summary of injuries is provided in Table 1. The patient had undergone anterior cruciate ligament (ACL) reconstruction of his right knee 2 years previously. After immobilization with extension splinting, the patient was transferred to our institution for definitive management by an experienced orthopaedic team with surgeons specializing in sport-related injuries of the knee.
Summary of Injuries Sustained by Each Knee a

a MCL, medial collateral ligament; POL, posterior oblique ligament; KD-V grade, which consists in multiligamentous injury with periarticular fracture; KD-IV grade, with an injury of ACL, PCL, LCL, and MCL.
Single-stage surgery was performed on each knee to manage all reconstructions and repairs. Because of the tibial fracture and the fibular head dislocation, the right knee was addressed first, at 9 days after the fall, and the left knee was operated on at 2 weeks after the fall.
In both knees, the surgical procedure commenced with arthroscopic evaluation and repair of meniscal injuries using a low pump pressure to minimize the risk of compartment syndrome. The tourniquet time for both knees was less than 1 hour because it was only applied for the duration of meniscal surgery and the subsequent lateral approach for safe exploration and identification of the peroneal nerve. In view of the need to reconstruct multiple structures, a complete fresh-frozen extensor mechanism allograft (Figure 3) was used to provide sufficient graft material for each knee. Table 2 provides details of the ligament reconstruction performed, graft type, and fixation type.
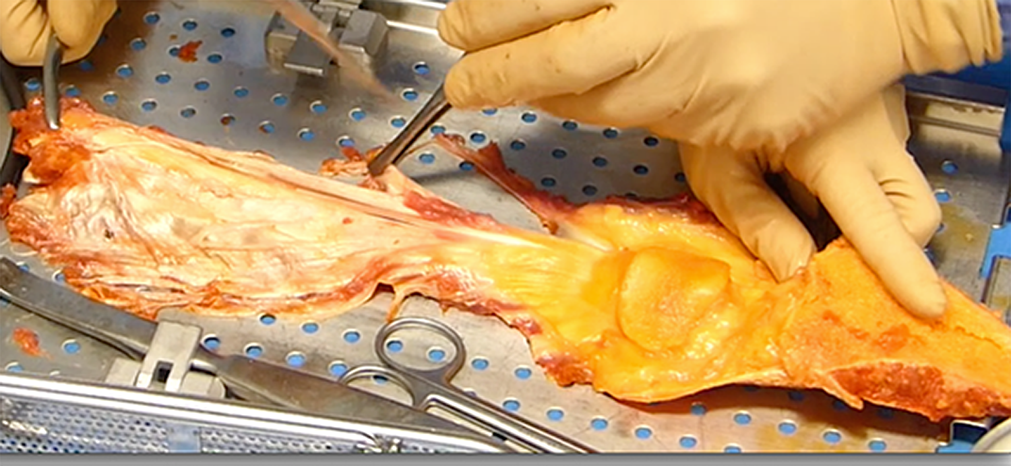
All grafts were obtained from a fresh-frozen single extensor mechanism allograft for each knee.
Graft Types Obtained From a Single Extensor Mechanism Allograft for Each Knee and Type of Fixation Used for Each Reconstruction a

a ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner; POL, posterior oblique ligament; QT, quadriceps tendon.
With respect to the right knee, the lateral tibial plateau fracture and the proximal tibiofibular dislocation were reduced and fixed with 4.5- and 3.5-mm metallic screws (Figure 4). The medial meniscal roots were reinserted through 2 bony tunnels, and the posterior root of the lateral meniscus was appropriately repaired. The medial collateral ligament and posteromedial corner were reconstructed with a single strip of allograft (Figure 5). 21 Using an all-inside bicruciate ligament reconstruction technique, the ACL and posterior cruciate ligament (PCL) were reconstructed. The ACL graft was tensioned and fixed before fixing the PCL in full extension, ensuring neutral anteroposterior positioning of the tibia under the femur. The PCL was then tensioned with the knee at 90° of flexion while applying anterior translation to the tibia to reduce the posterior drawer without any risk of overcorrection. 23,37
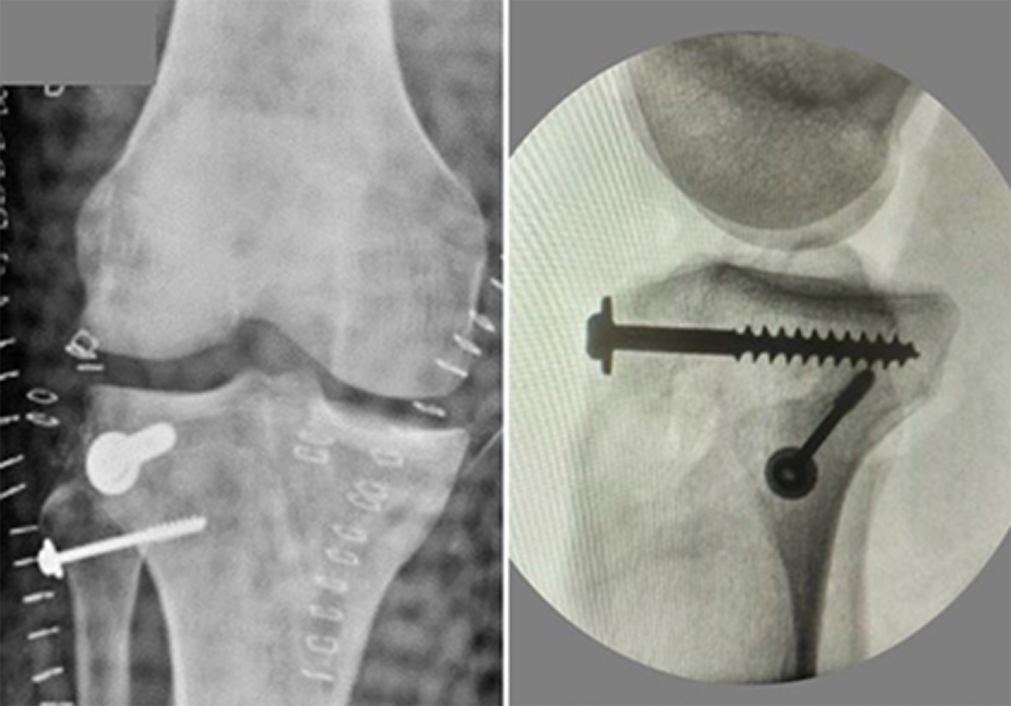
Postoperative radiographs of the right knee showing the reduction and fixation of a lateral tibial plateau fracture and proximal tibiofibular dislocation with 3.5-mm metallic screws and washers.

The medial collateral ligament and posteromedial corner were reconstructed as described by Lind et al 21 with the modification of an allograft rather than a semitendinosus autograft. SM, semimembranosus tendon.
With respect to the left knee, the vastus medialis and medial gastrocnemius were reinserted in their appropriate sites. The bucket-handle tear of the medial meniscus and the posterior horn of the lateral meniscus were repaired with all-inside repair. The posterolateral corner (PLC) was reconstructed using the modified LaPrade technique of Versailles 25 (Figure 6), which ensured anatomic reconstruction of the 3 main PLC stabilizers (PLC, popliteus tendon, and lateral collateral ligament) to restore posterolateral stability of the knee. For ligament reconstructions (ACL, PCL, medial collateral ligament, and posterior oblique ligament), the same surgical techniques described for the contralateral side were performed. Surgery lasted 4.0 hours for the right knee and 3.3 hours for the left knee, performed 1 week apart.

The posterolateral corner (PLC) was reconstructed using the modified LaPrade technique of Versailles, 25 which ensured anatomic reconstruction of the 3 main PLC stabilizers (PLC, popliteus tendon, and lateral collateral ligament) to restore posterolateral stability of the knee. Graft fixation was performed with a single interference screw and a suture.
Postoperatively, the patient remained in an open cast for 45 days without weightbearing but was immediately stimulated to focus on quadriceps isometric contraction, with flexion between 0° and 30°. At 6 weeks postoperatively, removal of the screw from the tibiofibular joint was performed with manipulation under anesthesia. The stability of the knees was evaluated and considered to be very good. Partial weightbearing was allowed after 6 weeks and full weightbearing at 10 weeks. Nine months after progressive strengthening and proprioception training as well as management of the psychological aspects of rehabilitation, under the supervision of the physical therapy team, athletic trainer, and ski federation psychologist, the patient performed the K-STARTS test, reaching a score of 90. 4 Ten months after the accident, he was able to return to skiing; 666 days after the accident, and after intensive training, he was asymptomatic and able to return to the Alpine Ski World Cup, referring to his knees as ‘practically normal’ (Figure 7). The physical examination findings at 2-year follow-up are demonstrated in the Supplementary Video.

(A) Partial weightbearing was allowed after 6 weeks and full weightbearing at 10 weeks. (B) The patient is shown 9 months after surgery performing the K-STARTS test and reaching a score of 90. (C) Twenty months after the accident, and after intensive training, the athlete was asymptomatic and returned to the Alpine Ski World Cup without complaints, referring to his knees as ‘practically normal.’
Discussion
This case report demonstrates that return to elite sport is possible after the surgical management of bilateral knee dislocations. This is an important message because, according to the systematic review published by Everhart et al, 12 the rate of return to preinjury levels of sport in competitive/elite athletes after the surgical management of unilateral MLKIs is very low (22%-33%). Bilateral knee dislocations occur much less frequently than unilateral MLKIs, and thus, similar case series reporting return-to-sport data after this more severe injury pattern are not available in the literature. 1,3,5 However, it would be logical to expect inferior outcomes when compared with unilateral knee dislocations. This case report is therefore important in demonstrating that return to elite sport is possible after bilateral knee dislocations, and it is also useful to highlight some of the concepts that we consider important in achieving optimal outcomes after MLKIs.
Hirschmann et al 16 have identified that timing of surgery significantly influences long-term outcomes. Patients treated more than 40 days after an injury had to give up professional sport more frequently than patients treated earlier. In their series of 24 unilateral multiligament knee reconstructions performed between 1983 and 2006, they reported that surgery was performed as early as possible after the injury but only when soft tissue swelling had resolved and range of motion had been regained to minimize the risk of arthrofibrosis. Twelve patients were operated on within the first week, 5 within 2 to 3 weeks, and 7 after 3 weeks. Despite this approach, they reported that at a median follow-up of 8 years (range, 1-23 years), 38% of patients had a flexion deficit and 25% an extension deficit. Our approach differed in that surgery was deferred until the patient was able to demonstrate good quadriceps activation. The interval between injury and the first surgical procedure was only 9 days because of the strong emphasis on frequent isometric quadriceps activation exercises, which were commenced shortly after the dislocations were reduced in the emergency department. Stiffness is a well-recognized and important complication after knee dislocations treated with multiligament reconstruction. 15,22,28,34,40 To minimize the recognized risk of long-term stiffness, 9 both knees underwent planned manipulation under anesthesia as well as removal of the screw from the tibiofibular joint at 6 weeks postoperatively. This procedure consisted of improving range of motion by the progressive application of increasing passive loads to increase the flexion-extension arc via the rupture of intra-articular adhesions and scar tissue.
Hirschmann et al 16 also reported that persistent pain (42%) and instability (25%) were additional frequent causes of failure to return to sport after the surgical management of unilateral knee dislocations in elite athletes. The pathophysiology of both pain and instability in this setting is multifactorial, but consideration must be given to graft choice and the avoidance of donor site morbidity. In the current case, there was clearly an insufficient available autograft to complete all reconstructions, and for that reason, the use of an allograft was mandated. However, to prevent additional trauma to the knees, the use of an autograft was completely avoided by using a single fresh-frozen (nonirradiated) extensor mechanism allograft (per knee) to provide sufficient graft material for all reconstructions. It should be recognized that the use of a fresh-frozen allograft in ligament reconstruction is still controversial, and both autografts and allografts have their advantages and disadvantages. 6,7,29,31 However, it is useful to note that Tian et al 38 reported that comparable objective and subjective clinical results can be achieved with the use of a fresh-frozen hamstring tendon allograft compared with an autograft in ACL reconstruction and also that Grassi et al, 14 in a recent meta-analysis, showed similar outcomes for autografts and allografts when irradiated grafts were excluded.
In general terms, another important consideration is that the literature clearly demonstrates a strongly positive relationship between increasing annual surgical volume and improved patient outcomes across a wide variety of surgical procedures. Although this type of study does not exist for MLKIs, Schairer et al 32 reported that annual volume was a significant determinant of reoperation rates after ACL reconstruction. Specifically, they reported a 29% decreased risk of subsequent ipsilateral knee surgery for ACL reconstruction by surgeons performing more than 35 cases per year. 32 Clearly, multiligament reconstruction is a considerably more complex surgical procedure, and although a minimal annual volume is not defined, it seems logical that this type of surgery is performed by high-volume centers only to achieve the best possible outcomes. The senior author (B.S.-C.) of this case report has an annual volume of ACL reconstruction of more than 650 cases and a multiligament reconstruction annual volume of more than 30 cases per year.
Technically, the procedure of multiligament reconstruction and meniscal repair after knee dislocations is very demanding. The gold standard remains a 2-stage procedure. 20 However, recent studies have shown evidence of benefits when a single-stage procedure is performed. 8 Anatomy remains the key to success. 13 More than isolated classic reconstruction, anatomic repair of fresh soft tissue, and protection with augmentation using an allograft is our philosophy. We do not recommend extensive debridement of the remnant tissue but mostly repair and augmentation. With this philosophy in mind, some teams have even proposed early repair using suture augmentation with promising results. 17
A further consideration, highlighted by previous authors, is that athletes and their relatives, managers, and coaches often lack necessary understanding of the severity of the injury and expect return to sport within 4 to 6 months after knee dislocations. 16 In our case, the athlete was able to return to his chosen sport 10 months after his accident and to a competitive level after 20 months. Appropriate expectations must be held to avoid complications associated with premature return to sport, and this also involves giving consideration to the severity of injury and psychological factors. 41 In the case of our athlete, psychological follow-up and the K-STARTS test (ACL-RSI) were used to allow the athlete to return to sport in a safer manner.
Conclusion
It is our opinion that important considerations for achieving optimal outcomes after the surgical management of knee dislocations include a multidisciplinary approach by a specialist team, with an emphasis on early postinjury quadriceps activation exercises, minimal delay between the injury and surgery, the experience level and annual volume of the surgeon, avoidance of donor site morbidity, consideration of planned manipulation at 6 weeks postoperatively, and realistic expectations of the timing of return to sport. This case report demonstrates that return to elite sport is possible after the surgical management of bilateral knee dislocations.
A Video Supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/2325967119845017
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.-C. is a paid consultant for and receives royalties from Arthrex. A.S. is a paid consultant for Arthrex. J.-M.F. is a paid consultant for Arthrex. S.B. is a paid consultant for Zimmer and Adler. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.