
Abstract
Background:
Knee dislocations leading to multiligament knee injuries (MLKIs) in professional athletes are rare. Restoring athletes to preinjury sport levels is challenging and crucial because of their physical demands. Existing research on MLKIs lacks conclusive recommendations regarding repair/reconstruction techniques and staging as well as the ligament repair sequence for predicting return to play (RTP).
Purpose/Hypothesis:
The purposes were to (1) assess the RTP rate, time to RTP, and rate of return to previous levels and (2) analyze the reoperation rate in a cohort of professional athletes treated for knee dislocations with single-stage repair/reconstruction. The hypothesis was that a single-stage surgical approach and an individualized postoperative protocol would enable these patients to return to their previous professional sport levels.
Study Design:
Case series; Level of evidence, 4.
Methods:
Consecutive professional athletes who underwent surgery after sustaining a knee dislocation (types III-V) between 2007 and 2022, with a minimum 2-year follow-up, were included. Collected information included demographic and injury characteristics, surgical procedures, and postoperative outcomes. Primary outcomes were RTP rates, time to RTP, and rates of return to previous levels, with reoperation rates and complications as secondary outcomes.
Results:
There were 9 elite athletes included with a mean age of 26.6 years and a mean preoperative Tegner activity score of 9.5 (range, 8-10). The mean follow-up period was 5.8 years (range, 2-15 years). All patients underwent surgery within 3 weeks, except for 1 patient who required initial vascular treatment. At a mean of 12 months (range, 8-22 months), 88.8% of professional athletes returned to their preinjury level, with the exception of 1 patient with a traumatic injury of the common peroneal nerve. The mean postoperative International Knee Documentation Committee score was 89.9 (range, 71.3-97.7), the mean postoperative Lysholm score was 91.1 (range, 80-98), and the mean postoperative Tegner score was 8.5 (range, 3-10). At the last follow-up, 3 athletes had retired for reasons unrelated to their knees. Additionally, 3 patients (33.3%) required further surgery for early stiffness, with 2 patients undergoing arthroscopic arthrolysis and 1 patient undergoing manipulation under anesthesia with screw removal. No other complications were observed.
Conclusion:
Early single-stage surgery in professional athletes with MLKIs after knee dislocations led to high rates of RTP and return to previous levels. Postoperative stiffness requiring surgical intervention was seen in one-third of patients.
Keywords
A knee dislocation is often a high-energy injury that has a guarded prognosis, with a reported incidence of 0.02% to 0.2% of all orthopaedic injuries.7,19,28 Once the potentially devastating immediate and short-term complications are excluded, including popliteal artery and common peroneal nerve (CPN) injuries 44 and acute compartment syndrome, 46 the goal of the management of multiligament knee injuries (MLKIs) is to restore a congruent and stable joint to allow early range of motion (ROM). 42 However, given the multitude of combinations of ligamentous injuries that may occur in MLKIs, there needs to be a proper evaluation of the extent of ligamentous injuries.8,28,47 After a thorough diagnosis, a clear plan can be devised to manage these optimally. Reconstruction of the cruciate ligaments remains the gold standard, but there is debate on the best method for collateral ligament injuries and the timing of surgery.14,30,35,36,55
MLKIs in professional athletes present several challenges in the literature. First, there are inconsistencies in defining MLKIs as well as the distinction between recreational and professional athletes, leading to a large variability in reports on return to play (RTP).3,6,21 Second, professional athletes who have not experienced a true knee dislocation are more common and, when treated appropriately, have a better chance of RTP. 10 Knee dislocations that result in MLKIs (types III-V) in professional athletes, on the other hand, can be rare, and the outcomes are devastating, given the severity of the injury.20,27,52 Additionally, limited research exists on the outcomes of traumatic knee dislocations in elite athletes.5,15,27,53 Despite extensive efforts, only a small percentage of athletes return to their previous level of activity.5,18,27 Demanding functional requirements and injury severity in elite athletes present significant challenges for orthopaedic surgeons, underscoring the need for further research and standardized definitions to improve outcomes.
The purpose of this study was to evaluate (1) the RTP rate, time to RTP, and rate of return to previous levels as well as (2) the reoperation rate in a cohort of professional athletes treated for knee dislocations with single-stage repair/reconstruction using a standardized surgical approach and postoperative protocol.
Methods
Study Design and Participants
Institutional review board approval (COS-RGDS-2024-06-003-SONNERY-COTTET-B) was granted for this retrospective review of consecutive cases. Consecutive professional athletes who had sustained a radiographically documented knee dislocation that was treated by the senior author (B.S.-C.) from March 2007 to March 2022 were considered for study inclusion. The minimum follow-up period was 2 years. All athletes underwent a complete knee examination, radiography, and magnetic resonance imaging and had at least a type III knee dislocation based on the Schenck classification 49 (Figure 1). Recreational athletes or the general population were excluded, as were elite professional athletes who suffered a type I or II knee dislocation or a nondocumented knee dislocation (Figure 2).

Radiography and magnetic resonance imaging of a right knee, showing a (A) posterolateral knee dislocation (type III-L), (B) complete rupture of the lateral collateral ligament (white star), and (C) bicruciate ligament rupture (white circle).

Flowchart diagram.
Data were obtained from the senior surgeon’s existing registry, which included information such as age, sex, date of injury, time to surgery, affected side, type of graft used, surgical techniques employed, involvement of menisci/cartilage, type of sport, presence of vascular or nerve injuries, postoperative complications, and clinical scores (International Knee Documentation Committee [IKDC] form, Lysholm knee scale, and visual analog scale [VAS] for pain). The final data were obtained through direct telephone calls with the patients in April 2024 and verified using available public information from the media. In all cases, the information collected pertained to the first year after the patient returned to sport, with a minimum follow-up of 2 years.
Patients were defined as professional athletes via participation in competitions at national and/or international levels at the time of injury and whose primary source of income stemmed from engaging in their sport. The primary outcomes assessed were the RTP rate, time to RTP, and rate of return to previous levels. RTP and its timing were defined as the duration from surgery to the first competitive game or participation. Return to previous levels was deemed achieved when an athlete satisfied the criteria for inclusion on a team competing within the same league or game or its comparable counterpart in another country. The reoperation rate and complications were secondary outcomes.
Surgical Management
Once urgent vascular and neurological lesions were resolved or excluded by a clinical examination and computed tomography angiography, surgery was performed as early as possible when soft tissue swelling had settled and the patient was able to demonstrate good quadriceps activation. Single-stage surgery was then performed to manage all reconstruction and repair procedures, with the major goal of restoring anatomic ligament positioning and joint biomechanics (Table 1).
Surgical Pearls a

CPN, common peroneal nerve.
Surgery was performed with the patient under general anesthesia. An evaluation under anesthesia was always performed before the start of surgery. The patient was placed in the supine position in the standard arthroscopic position with a lateral post proximal to the knee at the level of the padded tourniquet, allowing full ROM when desired. The tourniquet was applied and inflated only for exploration of the CPN if needed and during the arthroscopic part of the procedure, with efforts made to minimize its duration to a maximum of 2 hours to reduce limb ischemia.
The first and crucial step involved addressing collateral ligament injuries. Regardless of whether they were medial or lateral, the primary focus was on identifying all anatomic structures from superficial to deep. Once recognized during arthrotomy of the capsule (Figure 3), it was possible to analyze or even treat many of the meniscal or cartilage lesions when applying varus or valgus stress before performing any repair. After the accurate identification of torn structures, we repaired all of them from deep to superficial, 17 including the capsule, which allowed the reduction of arthroscopic fluid extravasation, which in turn decreased the risk of compartment syndrome as we attempted to reseal the knee joint. 46 After repair of the superficial medial collateral ligament and posterior oblique ligament, the skin was left open to perform extra-articular augmentation (reconstruction) procedures, aiming to promote early motion and reduce proprioceptive deficits.

(A, B) Superficial medial collateral ligament rupture (white star) and tibial capsular avulsion and meniscotibial ligament (blue star). (C) Common peroneal nerve (CPN; white arrow). (D) Popliteal tendon avulsion (blue arrow).
The posterolateral corner was approached using a method previously described by Guy et al, 26 ensuring the accurate identification of various structures, including the biceps femoris tendon, gastrocnemius, lateral collateral ligament, and popliteus tendon. The CPN was then easily identifiable and was isolated if necessary. For the posterolateral corner, because of the predominantly varus bony morphology, we performed reconstruction to protect the lateral anatomic repair site, with a preference for one of the anatomic techniques,26,41,50 often supported by arthroscopic visual control. 24
Surgery of the posteromedial corner involved similar steps, including the accurate identification of primary structures and repair of the capsule and medial collateral ligament/posterior oblique ligament. 48 We primarily performed repair, but in cases of poor-quality structures, closure of the capsular disruption with anatomic reconstruction using an allograft was conducted to protect the repair site.
The second step was the arthroscopic component, which began with the evaluation and repair of meniscal injuries that could not have been repaired during the initial open stage of surgery. Next, the cruciate ligaments were managed via an all-inside arthroscopic bicruciate ligament reconstruction technique. The posterior compartment was assessed using a transseptal approach. 24 All tunnels were drilled before passage of the grafts to ensure the avoidance of tunnel collision. With regard to the order of tensioning, the anterior cruciate ligament (ACL) graft was tensioned and fixed before fixing the posterior cruciate ligament (PCL) in full extension, ensuring neutral anteroposterior positioning of the tibia under the femur. The PCL was then tensioned with the knee at 90° of flexion while applying anterior translation to the tibia to reduce the posterior drawer without any risk of overcorrection.39,57 In 3 cases, in view of a femoral tear of the PCL, as well as the presence of a good-quality stump both on preoperative magnetic resonance imaging and during arthroscopic visualization, repair of the PCL was decided. In these cases, with an outside-in technique, femoral reinsertion of the PCL was carried out using a femoral button.
Considering the need to reconstruct multiple structures, a different fresh-frozen allograft was used to provide sufficient graft material for each knee. Utilizing an allograft reduces the surgical time and has been proven to be a safe and effective option with no further donor site morbidity. 9
Details of the ligament repair/reconstruction technique, graft type, and additional procedures are provided in Table 2 and Figure 4. In summary, based on the injury pattern, collateral ligament repair was performed first, after which the ACL was fixed, followed by the PCL, and finally reconstruction of the collateral ligaments.
Characteristics of Procedures a

ACL, anterior cruciate ligament; ALL, anterolateral ligament; BPTB, bone–patellar tendon–bone; BQT, bone–quadriceps tendon; GT, gracilis tendon; HT, hamstring tendon; LCL, lateral collateral ligament; LM, lateral meniscus; MCL, medial collateral ligament; MM, medial meniscus; PCL, posterior cruciate ligament; PLC, posterolateral corner; POL, posterior oblique ligament; PTT, posterior tibial tendon; single-strip allograft, usually cut as a strip from excess tendon from another allograft being used.

(A) Anterolateral view. Common graft of anterior cruciate ligament (ACL) and lateral collateral ligament (LCL) to avoid multiple tunnels. Anatomic graft position for posterior cruciate ligament (PCL) and popliteus tendon. (B). Medial compartment view. Posterior oblique ligament (POL) and superficial medial collateral ligament (MCL) reconstruction with independent grafts.
Postoperative Protocol
Postoperatively, rehabilitation was conducted at a specialized center in 2 separate phases. The first phase, from 0 to 6 weeks, focused on ensuring the quality of initial postoperative care. The main objectives were to activate the vastus medialis oblique muscle through biofeedback, allow knee flexion without forcing it, and protect the ligament reconstruction site with partial weightbearing and a brace locked in extension, except during prescribed exercises. ROM exercises were aimed at obtaining full extension while avoiding genu recurvatum. The rationale behind this protocol is to protect the reconstruction grafts from mechanical stress and allow sufficient motion to prevent arthrofibrosis. Second arthroscopic arthrolysis or manipulation under anesthesia (MUA) was preemptively planned in case the patient showed signs of stiffness at 6-week follow-up (flexion <90°). However, if the patient demonstrated good ROM, the procedure was not performed.
The second phase, from 6 to 8 weeks, aimed to gradually restore full weightbearing and continue to recover ROM. The brace was removed at 6 weeks. The first milestone was reached when sufficient flexion was achieved, allowing cycling and gradual weaning off of the crutches.
Subsequent rehabilitation took place at the athlete’s club. Generally, the rehabilitation timeline was adapted to each athlete’s recovery, following the surgical and medical team’s guidelines, avoiding psychological pressure, and allowing step-by-step progress. The second milestone was achieved when ROM was restored, the knee had no effusion, and ligament testing produced “normal” findings, allowing a gradual return to running, never before 4 to 5 months, especially if meniscal repair was performed; at this stage, a functional brace was not used.
The third milestone involved undertaking specific rehabilitation protocols, either at the club or at the center, including the reintegration of running, sprinting, jumping, and changing directions, before undergoing the K-STARTS (Knee Santy Athletic Return to Sport) test, 22 which provides the physical and psychological status of each patient and the specific work needed. The final milestone involved a gradual return to their sport, at least 1.5 to 2 months before competitions, to reintegrate the cognitive aspect of RTP.59,61 The knee’s reactions were checked daily before and after sessions to moderate the intensity of the sessions and ensure the progression of recovery. Ultimately, each patient’s rehabilitation and return to sport were tailored based on individual injury patterns and the recovery progress.
Results
Patient Characteristics
A total of 9 professional athletes, with 1 athlete with bilateral knee dislocations, 53 were included from March 2007 to March 2022. The mean age was 26.6 years, and there were 7 men and 2 women. The mean preoperative Tegner activity score was 9.5 (range, 8-10), and the mean follow-up was 5.8 years (range, 2-15 years). The distribution of MLKIs was 50.0% type III-M (n = 5), 20.0% type III-L (n = 2), 10.0% type IV (n = 1), and 20.0% type V (n = 2). All patients underwent surgery within the first 3 weeks, except for patient 9, who suffered a traumatic popliteal artery injury and CPN injury requiring initial vascular treatment by arterial dilation. The preoperative condition of each patient is shown in Table 3.
Patient and Injury Characteristics a
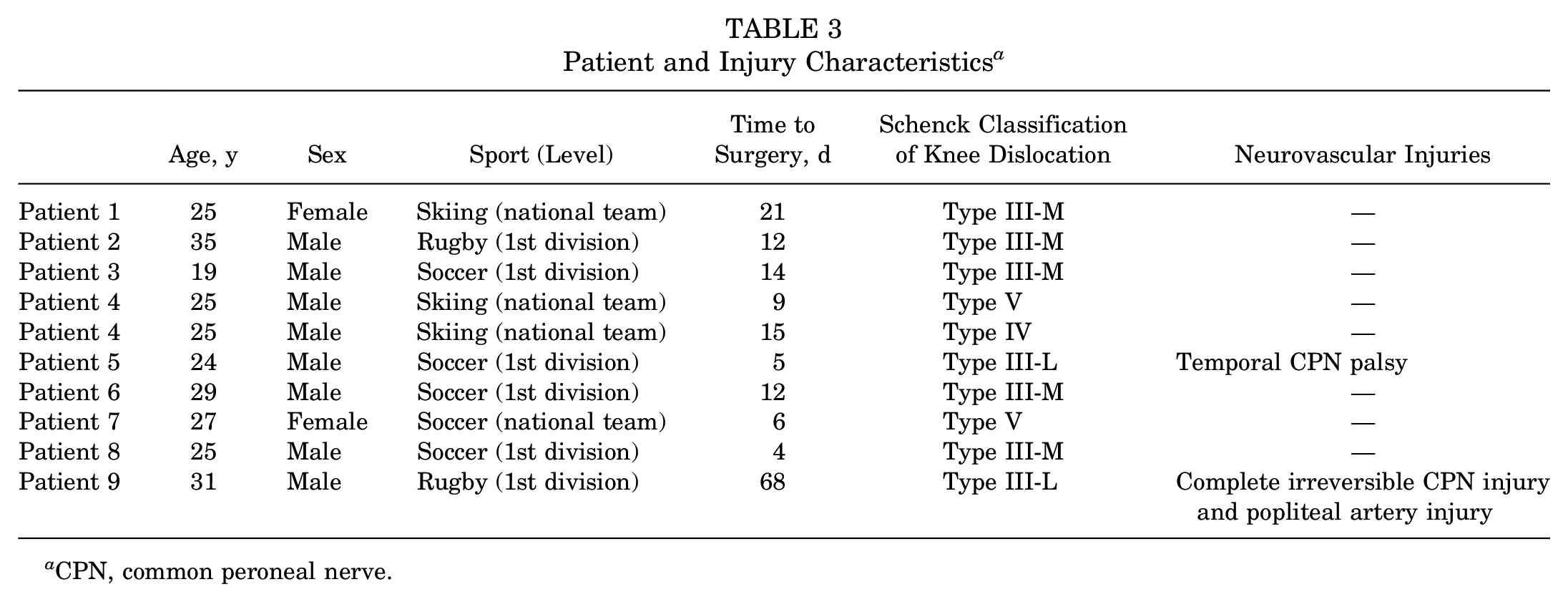
CPN, common peroneal nerve.
Postoperative Outcomes
In this cohort, 88.8% of patients (n = 8) returned to their previous level of sport, with a mean time to RTP of 12 months (range, 8-22 months). Patient 9 was not able to return to his previous level because of an irreversible lesion of the CPN. Individual RTP rates, times to RTP, and rates of return to previous levels are summarized in Table 4. Primary and secondary outcomes, including the Lysholm, IKDC, Tegner, and VAS pain scores, are summarized in Tables 5 and 6. At the last follow-up, 5 patients were still active, while 3 patients had retired. Of the retired athletes, patient 1, a female skier, retired after a 15-year competitive career. Patient 2, a professional rugby player, retired at the age of 37 years after 2 years of competitions. Finally, patient 4, a professional skier who suffered bilateral dislocations, retired after 3 years because of a new accident not involving the knees and decided to pursue a career as a ski instructor.
Clinical Outcomes a
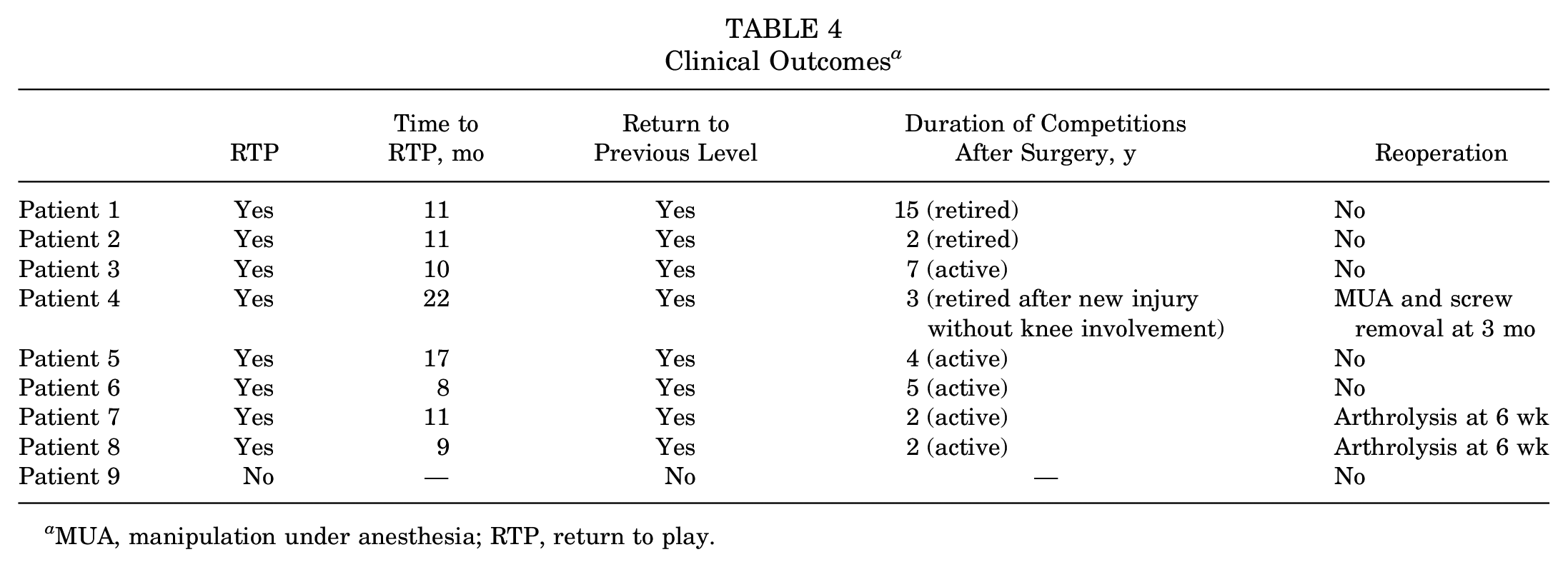
MUA, manipulation under anesthesia; RTP, return to play.
Patient-Reported Outcome Scores a
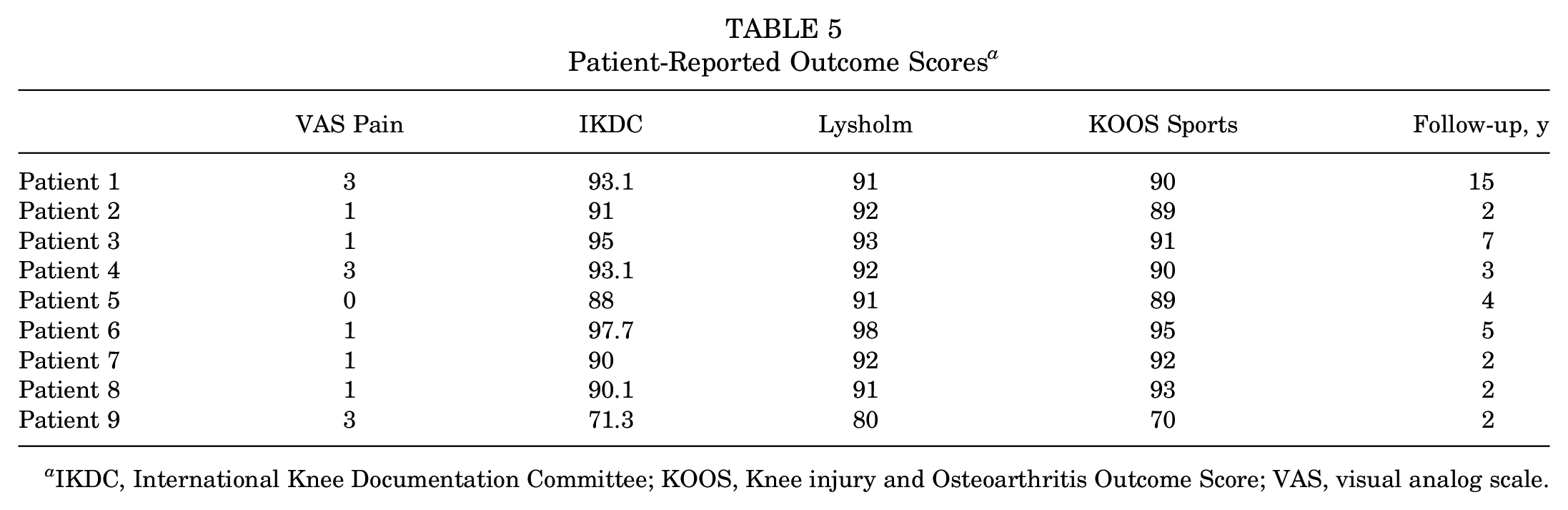
IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; VAS, visual analog scale.
Clinical Outcomes and Patient-Reported Outcome Scores of Entire Cohort a
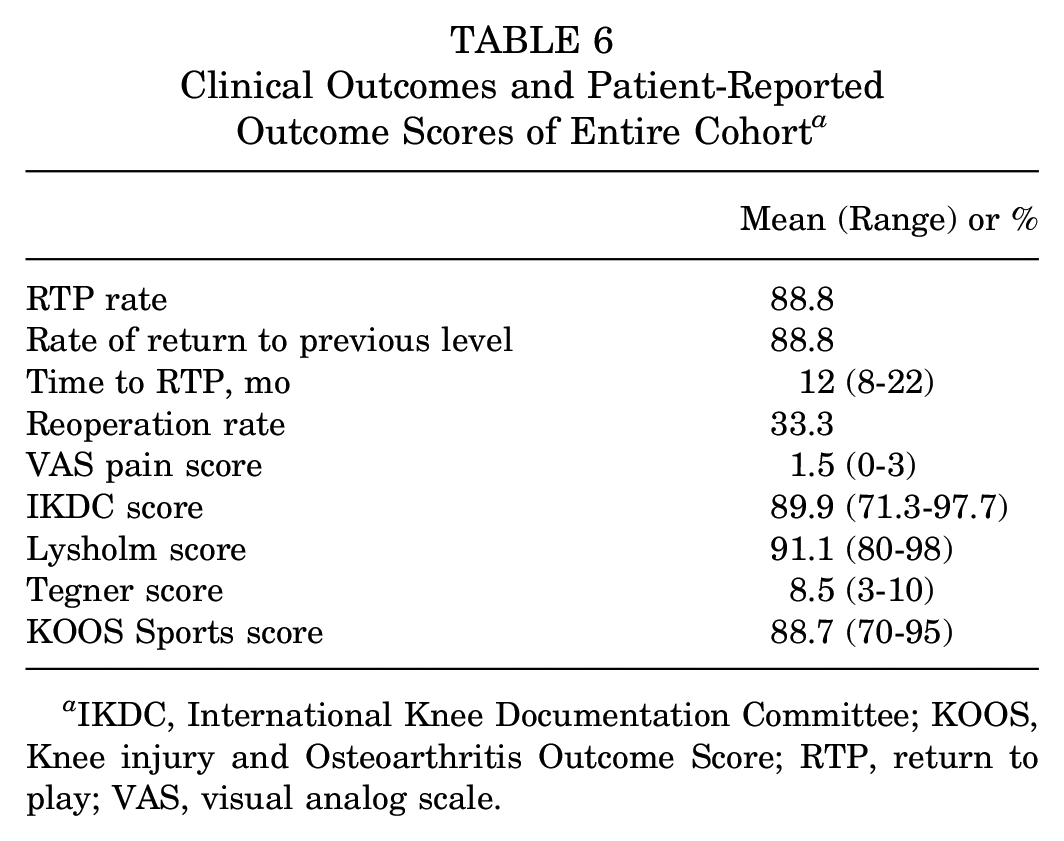
IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; RTP, return to play; VAS, visual analog scale.
Reoperations and Complications
At the final follow-up, 3 patients (33.3%) had undergone secondary surgery, consisting of 2 cases of planned arthroscopic arthrolysis and 1 case of bilateral MUA with screw removal because of early stiffness. As mentioned above, a second arthroscopic arthrolysis or MUA was planned preemptively to facilitate mobilization if the patient showed signs of stiffness at the 6-week follow-up visit. The remainder of the patients showed good ROM, and arthrolysis was not performed. None of the patients had any other complications (graft or meniscal rupture, joint infection, or postoperative hematoma) that required surgery.
In this cohort, 2 patients with a type III-L knee dislocation suffered a CPN injury preoperatively. Patient 5 recovered from CPN palsy after 6 months and was able to return to sport with a delayed time to return. Patient 9 had a complete injury of the CPN, thus preventing him from returning to sport. After knee recovery, tibialis posterior tendon transfer was performed to manage foot drop, allowing the patient to achieve a good quality of life.
Discussion
The primary main finding of this study is that 88.8% of the professional athletes who experienced MLKIs with knee dislocations were able to return to play, specifically at the same preinjury levels after 1-stage surgical management. The mean time to RTP was 12 months. In addition, 33.3% of patients needed arthroscopic arthrolysis or MUA in the early rehabilitation period.
This study contributes novel insights into the management of MLKIs by focusing on RTP and return to previous levels, specifically among professional athletes. The existing literature has demonstrated improvements in patient-reported outcomes in the nonprofessional athlete population with advancing management strategies.10,12,14,43 However, there remains a notable gap in understanding RTP rates and timing among elite athletes, particularly those who sustained a documented knee dislocation of type ≥III. To date, only a few studies have delved into these outcomes in elite athletes.
According to a systematic review by Everhart et al, 20 the rate of return to preinjury levels of sport in competitive/elite athletes after the surgical management of MLKIs was very low (22%-33%). Also, Hirschmann et al 27 investigated the surgical treatment of bicruciate ligament injuries and found that while 79% of athletes returned to sport, only 33% were able to return to preinjury levels. Conversely, Bakshi et al 3 examined National Football League players undergoing reconstruction of ≥2 knee ligaments and reported a 64% RTP rate. However, the limited information provided on injury patterns and severity in their study disallows a direct comparison. Borque et al 6 also reported on 136 professional athletes with surgically treated MLKIs, with 85.8% returning to the same or higher level. However, only 18 patients (13.2%) of those had bicruciate ligament injuries, with no information on documented knee dislocations. In a recent study, 29 patients with documented type III knee dislocations undergoing surgical management had worse clinical and functional outcomes than those without.
The current study showed excellent rates of RTP and return to previous levels within this specific cohort. Of the 9 patients, 8 were able to resume their previous elite careers, including 1 patient who experienced bilateral dislocations. The only case in which RTP was not achieved was of a patient with an irreversible preoperative peroneal nerve injury. In general, patients with complete nerve palsy tend to have worse outcomes compared with those with incomplete palsy. 62 On average, patients returned to play at 12 months (range, 8-22 months). Variations in return times can be attributed to the differing preoperative conditions observed within this small cohort. For instance, one patient experienced a reversible peroneal nerve lesion after 6 months, while another required a longer recovery period because of bilateral involvement. These higher success rates can be attributed to advancements in surgical techniques and rehabilitation protocols over time.
Our surgical approach prioritized early repair of collateral ligaments, capsular and meniscal repair, and allograft augmentation to bolster the repair construct, 23 especially on the lateral side. This strategy was designed to preserve knee stability and function, recognizing the crucial role of proprioception mediated by mechanoreceptors within ligaments.16,51,63 Furthermore, advancements in our understanding of the anatomy of the medial and lateral structures of the knee have led to repair that closely replicates native tissue,2,4,31,33,55,56 thereby playing a pivotal role in sustaining knee stability and reinstating appropriate tension and alignment for optimal ligament function. Correspondingly, recent evidence also suggests the potential benefits of single-stage procedures. 12 We emphasize the importance of a methodical approach to ligamentous injuries, beginning with a thorough assessment and classification of the extent of each lesion. Once this inventory is completed, the surgical strategy should prioritize the sequential repair of ligamentous structures, starting from the deep layers (capsule) and proceeding superficially, layer by layer. This approach ensures the comprehensive restoration of knee stability and function, addressing the primary structures responsible for joint integrity. Only after performing these repair techniques should classic reconstruction techniques (eg, LaPrade, Arciero, and Lind techniques)1,32,37 be considered, thereby providing a solid foundation for successful long-term outcomes in athletes returning to sport. This personalized approach not only optimizes the outcomes of the surgical procedure but also minimizes the risk of potential complications.
The second main finding is a reoperation/complication rate of 33.3% after 1-stage surgery. Of the 9 patients, 3 underwent knee arthrolysis or MUA in the early postoperative period to minimize the recognized risk of long-term stiffness.13,38,40,45 Our approach differed from those in other studies 27 in that surgery was deferred until the patient was able to demonstrate good quadriceps activation. 54 Also, during early postoperative rehabilitation, motion was initially restricted, which may have contributed not only to early stiffness but also to ligament healing.
Additionally, this cohort of athletes had a low VAS pain score at follow-up of 1.5 (range, 0-3). Hirschmann et al 27 reported that persistent pain (42%) and instability (25%) were frequent causes of failure to return to sport. The pathophysiology of both pain and instability in this setting is multifactorial, but due consideration must be given to graft choice and the avoidance of donor site morbidity. To prevent additional trauma to the knee and major muscular imbalance, in the current study, a fresh allograft was routinely utilized to improve collateral ligament repair or PCL reconstruction. Both autografts and allografts have their advantages and disadvantages.11,60 However, Tian et al 58 reported that comparable objective and subjective clinical results were achieved with a fresh-frozen hamstring tendon allograft compared with an autograft in ACL reconstruction. Also, in a recent meta-analysis, Grassi et al 25 showed similar outcomes for autografts and allografts when irradiated grafts were excluded. Moreover, we were proactive in performing meniscal repair to avoid future biomechanical imbalance. Additionally, none of the patients in our cohort required a major cartilage procedure.
Finally, this cohort is highly specific, with high-energy injuries linked to sports activities. This differs greatly from the general population that typically suffers these types of injuries that are associated with more severe polytrauma. When coupled with other abnormalities in polytrauma, knee-focused rehabilitation efforts are greatly hindered.
There are some limitations in this study. First, it is a unicentric study, and it would be beneficial to broaden the analysis to other centers. Second, this study involves a small retrospective cohort of patients with strict inclusion criteria and heterogeneous injury patterns, limiting its comparability to other similar series. Additionally, because of the small number of patients and the absence of objective measures of ligament laxity, no statistical analysis was performed.
Professional athletes face unique challenges because of the rigorous demands of their sports and the high expectations for returning to preinjury performance levels. In our view, achieving optimal outcomes in elite athletes with MLKIs involves restoring joint congruity through a combination of anatomic ligament repair/reconstruction and biomechanically effective reconstruction, allowing for early rehabilitation, and facilitating high rates of RTP. To this end, we advocate for a multidisciplinary approach led by a specialist team, emphasizing early quadriceps activation exercises after the injury, minimizing the delay between the injury and surgery, utilizing allografts to avoid donor site morbidity, being prepared to perform MUA at 6 weeks postoperatively if needed, having a supervised gradual rehabilitation program, and maintaining realistic expectations regarding the timing of RTP.
Conclusion
Early single-stage surgery with a combination of repair/reconstruction in professional athletes with MLKIs after knee dislocations led to high rates of RTP and return to previous levels, with a 33.3% rate of reoperations, because of surgical interventions performed to regain early motion.
Footnotes
Final revision submitted December 16, 2024; accepted January 10, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.-C. has received consulting fees and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ramsay Santé (COS-RGDS-2024-06-003-SONNERY-COTTET-B).