
Abstract
Background:
Massive irreparable rotator cuff tears are a devastating problem, especially for the middle-aged active population. Tendon transfer seems to be a feasible treatment option for this age group. Biomechanical studies have shown that lower trapezius tendon transfer, rather than latissimus dorsi tendon transfer, could restore the kinematics of the shoulder.
Purpose:
To evaluate the functional outcome, efficacy, and safety of arthroscopy-assisted lower trapezius transfer with peroneus longus augmentation for irreparable posterior superior rotator cuff tears.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study included 20 patients who had massive rotator cuff tears, symptomatic global shoulder pain, and the inability to move their upper limbs actively. The patients were examined by manual testing using a goniometer, and the study had a follow-up period of at least 24 months.
Results:
The mean age of the patients was 53.4 ± 4.3 years (range, 40-60 years). Thirteen patients had associated biceps pathology. The mean American Shoulder and Elbow Surgeons score improved from 22.88 ± 7.25 preoperatively to 84.44 ± 4.54 postoperative (P < .001). The mean visual analog scale improved from 7.9 ± 1.33 preoperatively to 2.7 ± 1.3 postoperatively (P < .001). All patients regained a good functional range of shoulder motion at the end of the follow-up without major shoulder complications.
Conclusion:
Arthroscopy-assisted lower trapezius transfer with peroneus longus augmentation for irreparable rotator cuff tear is advisable because it shows marked improvement in the functional outcome and range of motion without major complications.
Keywords
Rotator cuff tears are a common cause of shoulder disability and pain. 36 Treatment options include surgical and nonsurgical options depending on the clinical findings, with evidence supporting both options.29,31 Massive rotator cuff tears are defined as defects >5 cm or tears involving >1 tendon.24,33
The advances in surgical techniques have allowed the repair of large symptomatic tears, but massive tears may not be amenable for repair, particularly when associated with marked retraction, fatty degeneration of muscles, and involvement of multiple muscles. Surgical options used for massive irreparable tears include debridement and decompression of tendons, partial tendon repair, tendon transfers (latissimus dorsi tendon [LDT] transfer and lower trapezius tendon [LTT] transfer), augmentation by grafts, superior capsular reconstruction, subacromial balloon spacer, interposition graft, and reverse shoulder arthroplasty.9,27
On magnetic resonance imaging (MRI), the criteria for massive irreparable rotator cuff tears preoperatively include a fatty degeneration index >3 for the supraspinatus muscle and a fatty degeneration index >2 for the infraspinatus muscle with a coronal oblique tear distance >31 mm and a sagittal oblique tear distance >32 mm. Definitive assessment for irreparability is made intraoperatively after tendon mobilization. 24 Massive irreparable rotator cuff in those with decreased functional demands or mild pain and/or shoulder dysfunction is often managed nonoperatively, especially in patients at high risk of surgical complications. 37 Otherwise, surgical treatment should be considered to improve the function of the shoulder, especially in young and middle-aged groups.
The LTT transfer has recently gained popularity in treating irreparable rotator cuff tears. The main objective is to decrease pain and improve the strength and function of the shoulder joint. 2
The trapezius muscle has a large origin; it consists of 3 segments: upper, middle, and lower trapezius fibers. The lower trapezius muscle fibers originate from T4 to T12, converge laterally, and are inserted on the medial scapular spine.13,25 The tendinous portion of the LTT is triangular and is innervated by the accessory nerve (motor) and from C3 and C4 (sensory). 27 The voluntary contractions of the trapezius muscle in normal individuals have been studied. The ability of the lower trapezius muscle to contract without activation of the upper part has been shown. This demonstrates the independent control of the lower trapezius by voluntary command. 21
The procedure may be performed as an open or arthroscopy-assisted procedure. There is some variability in techniques.11,14,15 The LTT needs to be augmented by a tendon graft. The most commonly used grafts are the Achilles tendon allograft and hamstring tendon autograft.10,13,35
The aim of this study was to evaluate the efficacy, safety, and functional outcomes of arthroscopy-assisted LTT transfer with peroneus longus augmentation for irreparable posterior superior rotator cuff tears. We hypothesized that arthroscopy-assisted LTT transfer with peroneus longus augmentation for irreparable rotator cuff tears would improve the postoperative functional outcome of patients when compared with their preoperative evaluation.
Methods
This study was approved by the Institutional Ethics Committee of the hospital, and all study participants provided both written and verbal informed consent.
From January 2020 to July 2021, a prospective case series study was conducted on 20 patients. All of them had symptomatic global shoulder pain and pseudoparalytic shoulders, which is the inability to actively elevate or externally rotate their upper limb, which was documented using manual shoulder testing. All cases were treated with an arthroscopy-assisted transfer of LTT to reconstruct posterior superior cuff tear with peroneus longus tendon autograft augmentation. The injury pattern and pain, range of motion (ROM), complications, functional results, and patient satisfaction were assessed using the visual analog scale (VAS) pain scale, basic shoulder tests, and the American Shoulder and Elbow Surgeons (ASES) score. The follow-up period was 24 months.
Inclusion and Exclusion Criteria
All patients included in this study had symptomatic shoulder pain, loss of active shoulder elevation and external rotation, and a massive rotator cuff tear reaching the glenoid rim or beyond, as well as fatty changes in muscle (Goutallier class 3 or 4 for the supraspinatus muscle and grade 3 for the infraspinatus muscle), a nonarthritic glenohumeral joint (Patte grade 3), an acromiohumeral interval <7 mm (Hamada grade 1 or 2), and an intact or repairable subscapularis.
Exclusion criteria included patients with reparable tears, revision cases, rotator cuff arthropathy, C3-4 nerve root injury, or spinal accessory nerve damage to the trapezius muscle; older patients (>70 years of age); patients who failed to adhere to postoperative physical therapy; patients with many medical comorbidities (American Society of Anesthesiologists grade 3 or 4), and patients with a current active infection (Figure 1).
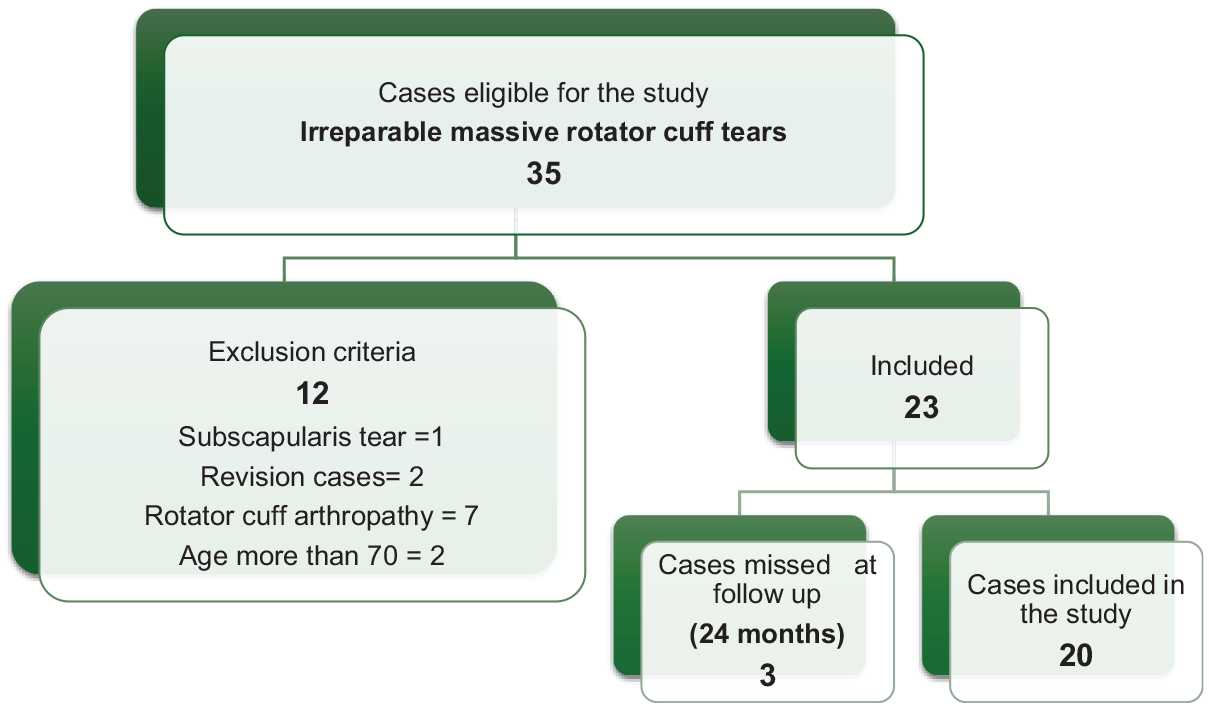
Flowchart of included/excluded patients.
History, Physical Examination, and Imaging
All patients were assessed. Pain and loss of active ROM were the main complaints for all patients without improvement after nonoperative treatment for >6 months. Patients were clinically evaluated for skin conditions, ROM measured by a goniometer, neurovascular function, and related trauma.
On examination for posterior superior rotator cuff tears, all patients had positive empty can and external rotation tests with the arm to the side (different grades of muscle strength). No patients with subscapularis findings were included in our study (negative external rotation lag signs and hornblower sign), as indicated with nearly normal belly-press and lift-off tests.
Also, routine anterior-posterior radiography and recent (<1 month preoperatively) MRI were conducted for all patients. The acromiohumeral distance and presence of arthritis (Hamada grade) were measured on plain radiographs, and the Goutallier classification of fatty infiltration was measured on sagittal T1-weighted MRI and the extent of retraction on coronal MRI (Figure 2).

Preoperative radiograph and coronal and axial magnetic resonance imaging scans.
Surgical Technique
All patients were operated on under general anesthesia and were given prophylactic antibiotics (1 g third-generation cephalosporin) with induction of anesthesia. All patients were placed in a beach-chair position with the ipsilateral shoulder and arm freely draped for easy movement and manipulation during surgery. The ipsilateral lower limb was also draped from the thigh to the foot, and a thigh tourniquet was applied for harvesting the peroneus longus tendon graft. It is important to adequately expose the ipsilateral medial border of the scapula for easy exposure of the LTT to be harvested. The desired incision and portals for tendon harvesting and arthroscopy were identified and marked.
We started with diagnostic shoulder arthroscopy to evaluate the glenohumeral joint and the rotator cuff. Any partial subscapularis tendon tears were repaired to aid in restoring the force couples around the shoulder. Long head of the biceps tendon (superior labral anterior-posterior lesion, fraying) pathology is also typically addressed by arthroscopic debridement and suprapectoral or subpectoral biceps tenodesis (Figure 3).

Diagnostic arthroscopy and orientation of the tear.
An LTT harvesting incision was made approximately 2 cm inferior to the spine of the scapula and a 4- to 6-cm horizontal incision was made from its medial border (Figure 4).
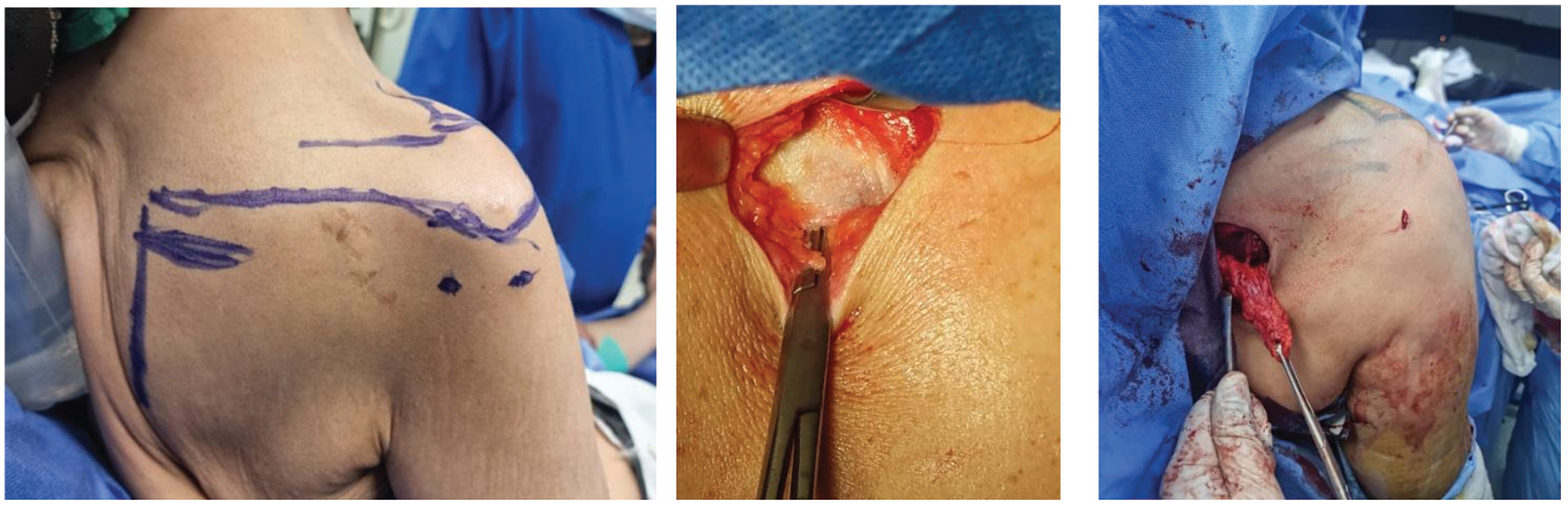
Patient positioning, portal landmarks, and lower trapezius harvesting site and lower trapezius tendon after harvesting.
Skin and subcutaneous tissue were incised, and then the fat pad in the lateral aspect of the incision was identified and excised to the extent overlying the LTT. The underlying infraspinatus fascia is an important depth landmark and should be differentiated from the LTT to avoid inadequate harvest.
The LTT was identified from its insertion, released from its insertion, mobilized, and whip-stitched with a heavy nonabsorbable suture (No. 5 FiberWire; Arthrex). Then, the peroneus longus tendon was harvested using an incision approximately 2 cm posterior to the lateral malleolus. The peroneus longus tendon was identified by its anterior position and its tendinous nature at this site. The tendon was harvested, and its distal end was tied to the peroneus brevis (Figure 5).

Peroneus longus identification and harvesting.
At the side table, the graft was prepared by removing any remaining muscle tissue and suturing and strengthening the graft with 1 No. 5 FiberWire suture on each side. The length of the graft after preparation ranged from 24 to 28 cm, and the single-fold diameter ranged from 5 to 7 mm.
The posterior superior cuff footprint, located 1 cm distal to the anatomic footprint at the greater tuberosity, was debrided until a bleeding bone was encountered. The plane between the infraspinatus and deltoid muscles was developed arthroscopically from the lateral portal to the lower trapezius harvesting incision. Thereafter, a large opening of the infraspinatus fascia was performed from the lower trapezius harvest incision to facilitate graft passage.
The peroneal tendon autograft was then retrieved arthroscopically into the glenohumeral joint using a long tissue-grasping instrument from the anterior lateral portal (Figure 5). As a result, the peroneal tendon autograft could travel between the deltoid and infraspinatus muscles, eventually reaching the subacromial region.
One of the ends of the peroneal tendon autograft was fixed to the anterior part of the footprint of the supraspinatus with 1 No. 5 SwiveLock suture anchor (Arthrex) (Figure 5). Then the other end of the peroneus longus tendon autograft was passed through, sutured, and looped to the LTT, and then passed back to the glenohumeral joint and fixed to the posterior of the footprint of the infraspinatus muscle by 1 No. 5 SwiveLock suture anchor.
The final step of this procedure was to suture the medial end of the peroneus longus tendon autograft to the LTT. First, the arm was placed in abduction and external rotation. The end of the peroneal tendon autograft was then weaved and enfolded into the LTT. An assistant must pull the LTT and the peroneal tendon autograft in opposite directions to provide maximal tension. Multiple heavy nonabsorbable sutures (No. 5 FiberWire) were then used to achieve sound fixation of both tendons (Figure 6). Then, a shoulder immobilizer brace was applied to avoid excessive adduction and internal rotation.

Peroneal tendon graft passage, fixation in the greater tuberosity, and after fixation of tendon graft.
Postoperative Rehabilitation Protocol
The recovery after arthroscopy-assisted LTT transfer entails 6 months of gradual rehabilitation in the early postoperative period, which consists of about 8 weeks. The patient is placed in an external rotation brace at 40° of abduction and 40° of external rotation. The brace is removed between 8 and 16 weeks postoperatively, and progressive active-assisted ROM is permitted with limitations to internal rotation. At 12 weeks after surgery, the internal rotation limitations are removed, and at 4 months, an 8-week progressive strengthening program is started. After completing the program, patients are permitted to engage in full strengthening and unrestricted activity.
Statistical Analysis
Data were collected, revised, coded, and entered into the Statistical Package for Social Science (SPSS) Version 23 (IBM Corp). Quantitative data are presented as mean, standard deviation, and range and median and interquartile range. Qualitative variables are presented as numbers and percentages. A comparison between the paired groups regarding quantitative data and nonparametric distribution was conducted using the Wilcoxon signed-rank test. The confidence interval was 95%, and the accepted error margin was 5%. A P value <.05 was considered significant.
Results
This prospective case series included 20 patients (12 [60%] male, 8 [40%] female) with a mean age of 53.4 ± 4.3 years (range, 40-60 years). The demographic and clinical data of all patients are summarized in Table 1.
Demographic and Clinical Data of the Studied Patients a

Data are presented as n (%) unless otherwise indicated. SLAP, superior labral anterior-posterior.
The mean operative time was 120 minutes (range, 90-150 minutes), 5 patients had associated superior labral anterior-posterior lesions (25%), and 8 patients had biceps tendon fraying (40%). There were no intraoperative complications.
The follow-up period was a minimum of 24 months (mean, 27 ± 3 months; range, 24-30 months). The mean ASES score improved from 22.88 ± 7.25 preoperatively to 84.44 ± 4.54 postoperatively (P < .001). The mean VAS score improved from 7.9 ± 1.33 preoperatively to 2.7 ± 1.3 postoperatively (P < .001).
All patients regained good functional range of shoulder motion at the end of follow-up. The mean improvement of shoulder abduction measured by manual testing ROM was 110.5°± 14.77° postoperatively from 28.5°± 11.48° preoperatively (P < .001). The mean improvement of external rotation measured by manual testing ROM was 66.5°± 10.77° postoperatively from 13.0°± 6.57° preoperatively (P < .001). No major shoulder complications with good shoulder function were reported at the end of the follow-up period (Table 2).
Comparison Between the Studied Parameters Before and After Surgery at the End of Follow-up. a

Boldface P values indicate statistical significance. ASES, American Shoulder and Elbow Surgeons; ER, external rotation; VAS, visual analog scale.
Wilcoxon signed-rank test.
Regarding donor-side outcomes, the mean American Orthopaedic Foot & Ankle Society (AOFAS) score was 97.1 ± 1.9. One patient who had transient paresthesia on the dorsolateral aspect of the foot, which resolved completely after 3 months postoperatively, and there were no complaints regarding the ankle or foot at the end of the follow-up time.
Discussion
Our study shows that arthroscopy-assisted LTT transfer with augmentation by peroneus longus autograft led to improved shoulder functional outcome, pain, and ROM at 24 months of follow-up without marked donor-side complications.
Management of irreversible rotator cuff injuries is a major surgical endeavor. Although tendon transplants have been used, further comparison studies are needed to prove their usefulness in long-term follow-up. The LDT transfer is the most typically used for posterior superior rotator cuff injuries, with the LTT transfer offering a surgical option. 1
Open LTT transfer has been used to restore external rotation in patients with brachial plexus injuries, with promising results.4,12 Both open and arthroscopy-assisted LTT in the management of irreparable rotator cuff tear resulted in 80% improvements in both ROM and function, with a satisfactory rate of return to work. 34 Although the LDT has a higher excursion than the trapezius, 20 biomechanical studies suggest that it is less favorable in terms of anterior-posterior balancing force and concavity compression forces than the trapezius. 26
Hartzler et al 19 reported the biomechanical effects of the LTT transfer in rotator cuff–deficient shoulder models. They demonstrated that compared with the LDT transfer, the LTT transfer better restored shoulder kinematics and glenohumeral force couples in the adducted position. Importantly, despite the improved biomechanics with an LTT transfer, the kinematics and the level of the joint reaction forces never normalize in either an LDT or LTT transfer.
In another biomechanical study, the authors evaluated the external rotation moment arm (ERMA) of LTT and LDT transfers with the arm at the side and 90° of abduction. They reported significantly larger ERMA in the LTT transfer compared with the LDT transfer with the arm at the side; however, in 90° of abduction, the LDT transfer had a significantly higher ERMA than the LTT transfer. The ERMA of the LTT was comparable to the previously reported amounts for the infraspinatus and teres minor muscles with the arm at the side. The ERMA was the greatest for the LTT transfer when the tendon was attached to the infraspinatus insertion of the greater tuberosity as compared with the proximal diaphysis. LTT transfer also exhibited a function similar to that of an intact rotator cuff during external rotation, primarily in abduction. 8
Elhassan et al 16 described their approach of arthroscopy-assisted LTT transfer with Achilles tendon allograft augmentation as an alternative to LDT transfer for posterior superior irreparable rotator cuff tear, and it gained widespread recognition and popularity. 17 Previous studies use autologous hamstring tendon 35 and Achilles tendon allograft7,15 for LTT by both onlay and inlay methods for fixation.
The combination of LTT with superior capsular shoulder reconstruction is another option that has been described.6,32 Comparing both techniques regarding ROM, a rapid return to activities of daily living, a good functional outcome, and cost-effectiveness could be potential benefits. When both techniques were compared in cases of grade 4 fatty infiltration of the infraspinatus, it was found that both led to improvement in functional outcome; however, LTT was superior regarding ROM, the progression of arthritis, and the rate of failure. 3
Peroneus longus autograft was used in this study because it is a strong graft with a large diameter and length that can be folded to reconstruct 2 tendons when inserted into the anatomic sites at the greater tuberosity.
Use of the peroneus longus tendon autograft has been gaining popularity in the last decade. It was first described by Kerimoğlu et al 23 for anterior cruciate ligament (ACL) reconstruction. Use of the anterior half of the tendon also has been described, for either ACL reconstruction 38 or lateral ankle reconstruction, 28 without significant donor site complications after 24 months of follow-up.
Rhatomy et al 30 found no difference in ankle eversion strength or plantarflexion of the first ray after peroneus longus harvesting 6 months after surgery. In another study, the use of a full-thickness peroneus longus tendon graft was investigated in 37 cases of revision ACL reconstruction and a multiligament knee injury 18 ; the authors found that the ankle ROM and AOFAS score were comparable to those of the other limb after 24 months of follow-up. On a larger scale, Hossain et al 22 used the peroneus longus tendon in 439 cases of ACL reconstruction and demonstrated excellent Foot and Ankle Disability Index and AOFAS scores after 24 months of follow-up.
However, peroneus longus tendon should also be considered with caution, especially in high-performance athletes. In a recent study of 82 patients with a mean follow-up of 46.6 ± 30.3 months, Cakar et al 5 found that the mean AOFAS score was 98.7 ± 3.3 on the donor side, but 17 patients (20.7%) complained of hypoesthesia or hyperalgesia distal to the harvesting scar, 2 patients had compartment syndrome, and 1 patient experienced transient foot drop. Therefore, patients should be counseled regarding such uncommon complications.
The lateral limb of the peroneus longus autograft was first anchored at the rotator cuff footprint, and the medial limb was used to regulate the final tension by pulling the free limb, with appropriate tension adjusted when pulling the medial end of the tendon with maximum abduction and external rotation of the shoulder.
Transfer of the lower trapezius to reconstruct an irreparable rotator cuff tear is feasible without extensive dissection and with a low risk of nerve compression. According to this study, the similarity in the pull line of the lower trapezius augmented with the peroneus longus tendon could work to replicate the functions of the posterior superior cuff muscles. It could be another alternative to the already available transfers (in terms of tendon transfer or graft augmentation).
To the best of our knowledge, there have been no prior studies describing the use of peroneus longus autograft for augmentation for LTT in cases of irreparable posterior superior rotator cuff tears.
However, the study carries some limitations, such as the relatively small sample size and the lack of comparison with other graft options (eg, the effect of peroneus longus harvesting on long-term foot mechanics). Such limitations should motivate researchers to conduct a long-term follow-up for such cases. It is advisable to use peroneus longus autograft when allograft is not available as there are no data to compare both grafts. Another potential limitation is that perineal or soft tissue complications may be underreported due to the wording of survey questions, as transient complications were not explicitly included in the question stem.
We believe that further studies are required to define the indications of the several techniques described for the treatment of massive rotator cuff tear on an individual basis.
Conclusion
Arthroscopy-assisted LTT transfer with peroneus longus augmentation for irreparable rotator cuff tear is advisable because it shows marked improvement in functional outcome and ROM without major complications.
Footnotes
Acknowledgements
The authors appreciate the participation of all the staff members in the Department of Orthopedic Surgery, Al-Azhar University, Cairo, Egypt.
Final revision submitted November 7, 2024; accepted December 16, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Faculty of Medicine, Al-Azhar University Institutional Ethical Committee, Cairo, Egypt.
Data Accessibility Statement
The data sets used and analyzed during the study are available from the corresponding author upon request.