
Abstract
Background:
In cases of massive irreparable posterior-superior rotator cuff tears (MIPSRCTs), the results of lower trapezius tendon transfer (LTTT), which acts as a dynamic stabilizer of the glenohumeral joint, can be augmented by superior capsular reconstruction (SCR) using the long head of the biceps tendon (LHBT). The LHBT acts as a static stabilizer and augments the mechanical advantage of the transfer by enhancing the resistance to superior migration of the humeral head proximally.
Purpose:
To compare the results of arthroscopic-assisted lower trapezius tendon transfer (aaLTTT) with or without SCR using the LHBT in cases of MIPSRCT.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients with MIPSRCT between January 1, 2018, and March 2022 were retrospectively analyzed. They were divided into 2 groups. Group A included all patients with MIPSRCT who were treated with aaLTTT using SCR with LHBT. Group B included all patients with MIPSRCT who were treated by aaLTTT alone. Patients with a healthy and structurally intact LHBT underwent SCR in conjunction with LTTT. The results were assessed using the Subjective Shoulder Value (SSV), Constant-Murley score (CMS), Shoulder Pain and Disability Index (SPADI), active range of motion (AROM), acromiohumeral distance, motor power of shoulder movements, and patient satisfaction, as well as their ability to return to work.
Results:
The study included 60 patients, 30 patients in each group. There were 28 men (46.7%) and 32 women (53.3%), with a mean age of 53.4 ± 5.9 years (range, 36-64 years). The mean follow-up period was 30.0 ± 3.6 months (24-38 months). All patients experienced significant improvement in their self-reported shoulder condition (SSV) and reduction in their pain level (visual analog scale). There was no significant difference between the groups in either parameter. Regarding their functional outcome, patients in both groups had a significant increase in their CMS (group A: 39.5 ± 9.3 preoperative, 88.4 ± 0.7 at 24 months; group B: 36.4 ± 6.3, 72.4 ± 5.5) and a significant decrease in their SPADI (group A: 71.5 ± 9.4 preoperative, 19.2 ± 2.6 at 24 months; group B: 75.0 ± 7.0, 30.3 ± 4.9), but patients in group A had significantly better results than group B (P < .001). All affected AROM aspects improved in both groups. This improvement was significantly greater in the LHBT SCR group (treatment group, A) regarding abduction (158.5°± 4.8° vs 116.7°± 11.6°, P < .001) and external rotation in abduction (73.1°± 2.5° vs 56.2°± 4.2°, P < .001) at a 2-year follow-up.Patient satisfaction was significantly higher among group A patients (A: 90% vs B: 73.3%, P< .001) while no significant difference occurred in their rate of returning to the same work (A: 60% vs B: 66%, P = .38).
Conclusion:
aaLTTT augmented with LHBT SCR can be a sound option in the treatment of MIPSRCT with the potential to enhance patients’ functional outcome, satisfaction, and AROM with no increased risk of complications or morbidity.
Keywords
Rotator cuff injury is a common cause of shoulder pain. Massive rotator cuff tears (RCTs) account for 10% to 40% of all tears. 2 There is currently no consensus on the definition of a massive RCT. Among the more commonly used definitions is that of Cofield et al, 7 who described a massive RCT as one with a diameter >5 cm. Another widely used definition is that used by Gerber et al, 17 who state that a massive RCT is the complete detachment of 2 or more cuff tendons from the proximal humerus. Burkhart 3 also suggested that massive tears be defined as tears >5 cm and then further classified them according to pattern and edge mobility.
The Delphi consensus study, with 90% agreement, defined massive tears as retraction of tendon(s) to the glenoid rim in either the coronal or axial plane and/or a tear with ≥67% of the greater tuberosity exposed, measured in the sagittal plane. Posterosuperior tears are much more common than anterosuperior tears.4,15,16,19,20,21,24 Some tears are irreparable, whereas others are mechanically reparable but will not function at all. Therefore, the term functionally irreparable rotator cuff tear (FIRCT) was introduced. 5
Clinically, characteristics of an irreparable RCT include long duration of symptoms and weakness of external rotation (ER). Radiologic criteria include reduction of the acromiohumeral distance (AHD) to <6 mm on a true anteroposterior radiograph, torn tendon(s) retraction to the glenoid level (stage 3 Patte classification), and fatty infiltration of the rotator cuff muscles >50% (more than Goutallier III).23,32
Recently, tendon transfers have gained acceptance as a treatment option for irreparable cuff tears. Local tendon transposition, distant tendon transfer, and deltoid flap transposition have also been proposed. 30
Various approaches have been suggested, including local tendon transpositions, distant tendon transfers, and deltoid flap transpositions. Among the distant tendon transfers, the latissimus dorsi transfer for massive irreparable posterior-superior rotator cuff tears (MIPSRCTs) and, more recently, the lower trapezius tendon transfer (LTTT) have been proposed. 16
The LTTT transfer was first described and performed by Elhassan et al 12 to restore shoulder function in a patient with a traumatic brachial plexus injury. Given its proximity to the axis of motion of the posterosuperior rotator cuff, LTTT effectively replicates the biomechanical function of the posterosuperior cuff. This has led to favorable functional outcomes and has contributed to the increasing adoption of LTTT as a preferred surgical option for managing irreparable posterosuperior RCTs.18,26
The primary objective of this study was to compare the results of arthroscopic-assisted lower trapezius tendon transfer (aaLTTT) with or without superior capsular reconstruction (SCR) using the long head of the biceps tendon (LHBT) in cases of MIPSRCTs. The study hypothesized that augmented long head of the biceps (LHB) SCR improves shoulder functional outcome compared with LTTT alone.
Methods
This is a retrospective analysis of patients with MIPSRCTs who sought treatment from January 1, 2018, through the end of March 2022, treated using aaLTTT. Institutional review board approval for the study was granted by the Clinical Research Ethics Committee (IRB No. 0018122017).
Patients were divided into 2 groups. Group A included all patients with MIPSRCTs who were treated with aaLTTT using SCR with LHBT. Group B included all patients with MIPSRCTs who were treated by aaLTTT alone after at least a 2-year follow-up.Patients with a healthy and structurally intact LHBT underwent SCR in conjunction with LTTT. Conversely, in cases where the LHBT was frayed or degenerative, only the LTTT procedure was performed. All cases were performed at the same institution with the same surgeon.
The inclusion criteria were as follows: posterosuperior RCT (involving 2 tendons or measuring ≥5 cm) retracted to at least the glenoid level (Patte 3 tears) on preoperative magnetic resonance imaging (MRI) and fatty degeneration of their muscle bellies (Goutallier ≥3). Patients with radiologic evidence of preoperative glenohumeral arthritis or subscapularis tendon tear >I Lafosse were excluded from the study.
Outcome Measures
A total of 60 patients were enrolled, meeting the inclusion criteria (30 per group). The results were retrospectively assessed after a minimum of 2 years postoperatively using the Subjective Shoulder Value (SSV), visual analog scale (VAS), Constant-Murley score (CMS), 8 Shoulder Pain and Disability Index (SPADI), 27 and active range of motion (AROM) and compared with the preoperative values recorded in patients’ records. Motor power of the shoulder, acromiohumeral distance (AHD), patient satisfaction, and patients’ ability to return to work were also assessed.
AROM, including forward flexion (FF), abduction (ABD), and external (ER) and internal rotation (IR) measurements, was evaluated using a goniometer. Preoperative data of the patients were collected. At the final follow-up visit, muscle strength was assessed using a dynamometer and compared with the contralateral, unaffected side during an in-office evaluation.
Preoperative radiographs were collected for all patients to assess AHD measurements (Figure 1A). Noncontrast MRI (Figure 1, B and C) was performed for all patients. All our patients had supraspinatus and infraspinatus tears retracted or medial to the glenoid surface (Patte 3) and fatty degeneration involving more than half of the 2 muscle bellies, rendering them irreparable both anatomically and functionally.

(A) Anteroposterior radiograph showing proximal migration of the humeral head due to a massive irreparable posterior-superior rotator cuff tear. (B) Magnetic resonance imaging (MRI) showing a tear of the supraspinatus retracted to the level of the glenoid. (C) An MRI showing severe fatty infiltration of the supraspinatus muscle.
Patients’ preoperative functional scores were retrieved from hospital records. The SSV, 29 in addition to the VAS, measures patients’ estimation of their shoulder condition along with their pain levels. CMS 31 and SPADI 27 were used to assess the pre- and postoperative functional outcomes. Patient satisfaction after surgery was assessed by asking patients whether they were completely satisfied, satisfied with reservations, or not satisfied with the outcome of the procedure during the main follow-up visits. Only completely satisfied patients with no reservations were considered satisfied in the statistical analysis. The ability to return to work was assessed for employed patients.
Surgical Technique
All patients were operated on under general anaesthesia combined with an interscalene block. All cases underwent surgery in the beach-chair position on a special operation table, which allows exposure of the scapula and the parascapular region up to the midline of the back.
The extremity to be operated on was prepared with the proper sterilizing agent, starting from a point lateral to the dorsal spinous processes (at least 12 cm lateral to the medial border of the scapula and inferior to scapular spinous process) down to the hand, to the sternum edge in the midline and down to the level of the nipple across the chest (Figure 2). Similarly, the ipsilateral leg was sterilized from the anterior superior iliac spine down to the toes. The pneumatic tourniquet was inflated just before beginning the peroneus longus procedure.

Preoperative marking with evident wasting of shoulder muscles and scars from the previous attempt at repair.
Diagnostic arthroscopy was initially performed to confirm the diagnosis and the integrity of the LHBT (Figure 3). All patients received decompressive acromioplasty and subacromial bursectomy. Preparation of the posterosuperior cuff humeral attachment site was done using a bur to create a bleeding surface, ensuring not to accidentally erode the cortex, which could jeopardize the stability of the upcoming anchors.

Arthroscopic view through the posterolateral portal. The tendon grasper is used to confirm irreducibility of the massive posterosuperior rotator cuff tear (red star), which is retracted to the level of the glenoid (G). The long head of the biceps tendon (yellow circle) can be seen attached to its labral anchor (blue rectangle) and the bold humeral head (HH).
In treatment group A, LHBT was used for SCR after releasing the transverse humeral ligament (Figure 4). All cases in group B had their LHBT tenotomized. In both groups, the LTTT was done using the peroneus longus autograft. A minimum graft length of 26 cm was a prerequisite for this procedure (Figure 5). A long, curved, blunt dissector or finger was passed from the posterior to the subacromial space. The tunnel needed to be wide enough and positioned subdeltoid, superficial to the scapula and infraspinatus, to minimize impingement and maintain a more anatomic line of pull. Care needed to be taken to avoid compressing the suprascapular nerve along the superior scapular notch.

(A) Confirming the mobility of the long head of the biceps tendon (LHBT; yellow circle) to the site of planned repair to act as superior capsular reconstruction (blue cross). The rotator cuff tendon can be seen (red star). (B) Release of the transverse humeral ligament superficial to the LHBT. (C) Penetration of the LHBT with a suture-retrieving instrument to pass a fiberwire. (D) A loop stitch is tied through the LHBT. (E) Fixation of the LHBT with a knotless anchor to the humeral side of the superior capsular reconstruction. LHB, long head of the biceps; THL, transverse humeral ligament.
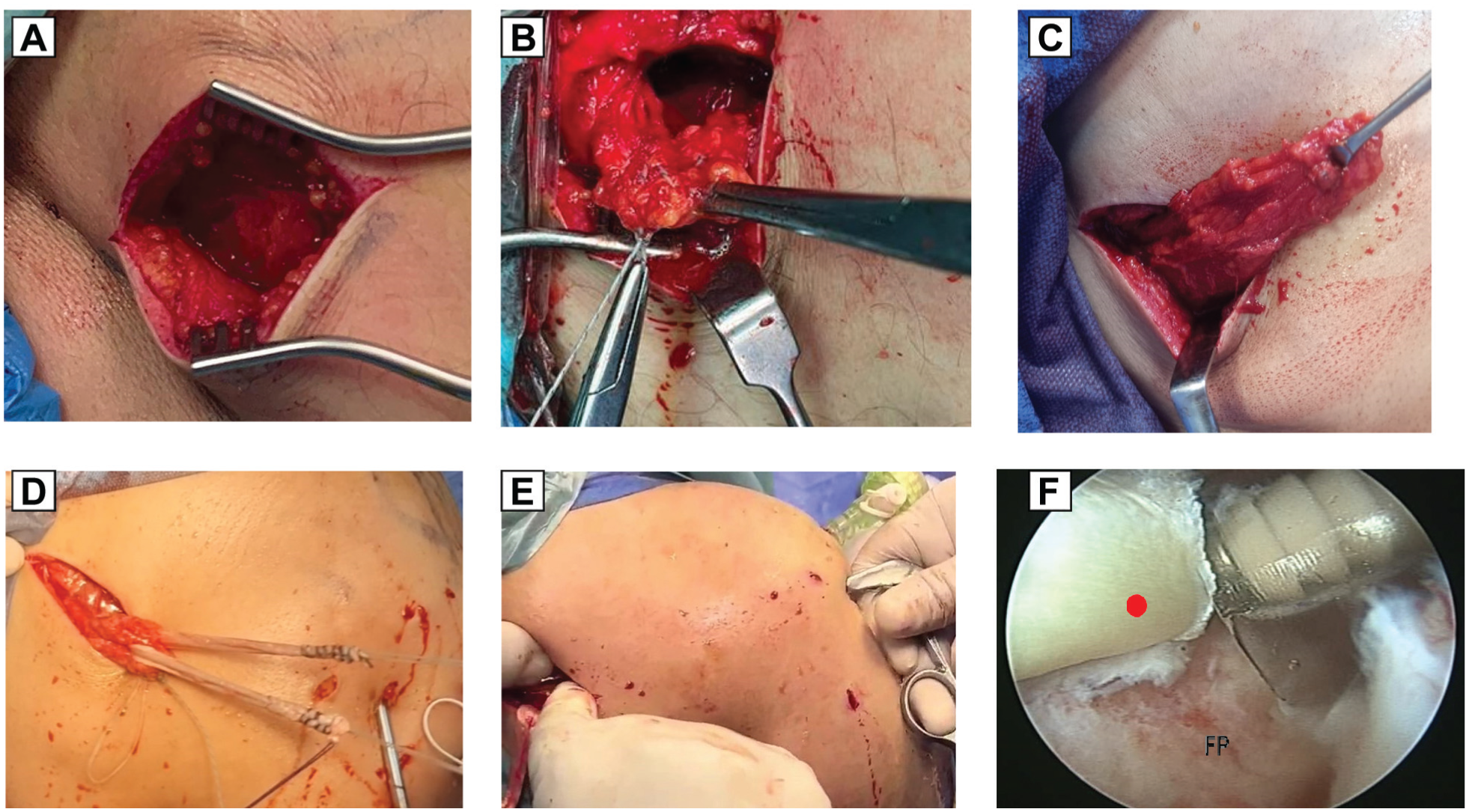
(A) Transverse incision below scapular spine. (B) Whipstitching of the tendon. (C) Lower trapezius tendon excursion. (D) Passage of the peroneus longus graft within the lower trapezius tendon. (E) Passage of ends of the peroneus longus graft by pulling its threads with a tendon grasper (inserted under arthroscopic visualization) through a previously prepared tunnel underneath the scapular spine, deltoid, and teres minor. The tunnel should be immediately under the deltoid. (F) Fixation of the peroneus longus graft end (red circle) to the humeral head footprint (FP) with a knotless anchor, with the shoulder in abduction/external rotation 45°/45°.
Postoperative Rehabilitation
An abduction brace was used by the patients for 6 weeks postoperatively, with the shoulder in 30° ABD and 30° ER. The postoperative rehabilitation was the same for all patients. The first phase (0-6 weeks) was the maximal protection stage, in which the main goals were minimizing pain, protecting the integrity of the repair, and restoring pain-free passive range of motion (PROM). AROM exercises of the elbow, wrist, hand, and cervical spine were started immediately, and PROM of the shoulder was performed in postoperative week 3. The second phase (6-12 weeks) was the AROM stage. The main goals of this stage were restoring functional AROM and proprioception, encouraging use of the operative upper extremity for light activities of daily living, and weaning from the orthosis. Active assisted range of motion (ROM) and AROM exercises were initiated in supine and side-lying positions, then progressed to antigravity positions as appropriate. The third phase (12 weeks to 6 months) was the strengthening stage, with the main goals of regaining muscle strength and shoulder stability and enhancing optimal PROM/AROM. Unrestricted use of the operated limb was allowed at 6 months postoperatively.
Statistical Analysis
Documented data were analyzed using the Statistical Package for the Social Sciences, version 23.0 (SPSS). The quantitative data were presented as mean ± standard deviation and ranges when their distribution was parametric (normal), while nonnormally distributed variables (nonparametric data) were presented as median with interquartile range. Moreover, qualitative variables were presented as numbers and percentages. Data were explored for normality using the Kolmogorov-Smirnov and Shapiro-Wilk tests. An independent samples t test of significance was used when comparing 2 groups. The confidence interval was set at 95%, and the accepted margin of error was 5%. P < .05 was considered significant, P < .001 was considered highly significant, and P > .05 was considered insignificant.
Results
The study included 60 patients, with 30 patients in each group (Figure 6), including 28 men (46.7%) and 32 women (53.3%). Their mean age was 53.4 ± 5.9 years (range, 36-64 years). A total of 40 patients had tears in their dominant hand (66.7%). Sixteen patients related their symptoms to a significant traumatic incident (26.7%), and 23 patients (38.3%) had previous failed attempts at repair: 11 mini-open (18.3%) and 12 arthroscopic (20%). Patients’ demographic data are presented in Table 1.

Flowchart of the study population.
Patients’ Demographic Data and Preoperative Evaluation From Patient Records a

Values are presented as number (%) or mean ± standard deviation unless otherwise indicated. CMS, Constant-Murley score; ER1, external rotation in adduction; ER2, external rotation in abduction; ROM, range of motion; SPADI, Shoulder Pain and Disability Index; SSV, Subjective Shoulder Value; VAS, visual analog scale.
The mean preoperative passive abduction was 154.2°± 11.6° (range, 135°-180°). The mean preoperative active abduction was 61.2°± 32.8° (range, 14°-120°). Active ER in adduction (ER1) was limited to 58 patients (mean 20.4°± 4.2°; range, 13°-26°) and was limited in all patients in abduction (ER2; mean 22.1°± 13.3°; range, 0°-47°). Mean active FF was 74.5°± 15.8° (50°-110°), while IR was least affected both actively and passively.
Preoperatively, 46 patients had reduced AHD at <6 mm, 28 patients had AHD <5 mm, and only 10 had AHD <3 mm. None had an acetabularized acromion, so all were classified as having Hamada grade 1 or 2. The mean preoperative AHD was 5.2 ± 1.3 mm (3-7 mm).
Regarding associated injuries, 18 patients had associated partial tears of the teres minor with fatty degeneration of the muscle belly in only 14 (8 patients with Goutallier grade 2 and 6 with grade ≥3). Seven patients had fatty degeneration grade ≤2 with no tears in their teres minor muscle belly. Fifteen patients had either degeneration or partial upper border subscapularis tears, while none had complete tears or fatty degeneration of the muscle belly.
The mean preoperative SSV was 19% ± 12.7% (0%-40%), mean VAS was 6.9 ± 0.96 (5-9), mean preoperative CMS was 35.2 ± 11.0 (range 9-55), and mean SPADI was 73.2 ± 8.4 (range, 50-89).
The treatment group and the control group had 30 patients in each. There was no significant difference between the 2 groups in terms of patient demographics, preoperative clinical findings, or radiologic findings (Table 1).
The mean follow-up period was 30.0 ± 3.6 months (24-38 months), and the mean age of the patients was 53.4 ± 5.9 years (range, 36-64 years).
All patients experienced significant improvement in their self-reported shoulder condition (SSV) and reduction in their pain level (VAS). There was no significant difference between the 2 groups in either variant. Regarding their functional outcome, patients in both groups had a significant increase in CMS and a significant decrease in SPADI, but patients in SCR group A had significantly better results than group B (Table 2).
Comparison Between the 2 Groups Regarding Postoperative Outcomes a

Independent samples t test was used to compare the mean ± SD between groups. Paired samples t test was used to compare the variance between preoperative and postoperative values. CMS, Constant Murley score; FU, follow-up; PO, postoperative; SPADI, Shoulder Pain and Disability Index; SSV, Subjective Shoulder Value; VAS, visual analog scale.
P < .001 is highly significant.
All affected AROM aspects improved in both groups, except IR, which was least affected preoperatively. This improvement was significantly greater in the LHBT SCR group (treatment group A) regarding ABD and ER in ABD (ER2) at the 2-year follow-up.The ER with arm beside the trunk (ER1) and FF improved in both groups, with no significant difference between the groups, despite being better in the treatment group (Table 3).
Comparison Between the 2 Groups Regarding Range of Motion a

Independent samples t test was used to compare the mean ± SD between groups. Paired samples t test was used to compare the variance between preoperative and postoperative values. ABD, abduction; ADD, adduction; ER1, external rotation in adduction; ER2, external rotation in abduction; FF, forward flexion; FU, follow-up; PO, postoperative.
P < .05 is significant.
P < .001 is highly significant.
The AHD was not affected by the outcome in patients with >6 mm preoperatively, whereas in those with proximal migration (AHD <5 mm), the mean increased to 5.4mm. The mean improvement of AHD was statistically significant in both groups (1.1 mm, P < .001). LHBT SCR did not generate a significant difference regarding AHD. This observed migration (AHD 5-6 mm) was not associated with a lower functional outcome during the study period (Table 4).
Comparison Between the 2 Groups Regarding Acromiohumeral Distance a

Independent samples t test was used to compare the mean ± SD between groups. Paired samples t test was used to compare the variance between preoperative and postoperative values. AHD, acromiohumeral distance; FU, follow-up; PO, postoperative.
P < .001 is highly significant.
P < .05 is significant.
Mean shoulder motor power was higher in group A. The difference between the groups was statistically significant regarding only the power of lateral abduction and ER in abduction (ER2) (Table 5).
Comparison Between 2 Groups Regarding Postoperative Motor Power at the End of Follow-Up a

Independent samples t test was used to compare the mean ± SD between groups. ABD, abduction; ADD, adduction; ER1, external rotation in adduction; ER2, external rotation in abduction; FF, forward flexion; FU, follow-up; PO, postoperative.
P < .001 is highly significant.
Regarding patients with minimal tears or degeneration of the subscapularis or teres minor, and those with fatty degeneration of the teres minor, there was no significant difference compared with patients without these lesions. Shoulder stiffness was reported in 1 patient in the SCR group due to noncompliance with the rehabilitation protocol, which required arthroscopic release and manipulation under general anaesthesia 4 months after the surgery.
Additionally, patient satisfaction was significantly higher among group A patients (A: 90% vs B: 73.3%), while no significant difference was observed in the rate of returning to the same work (A: 60% vs B: 66%) (Table 6).
Comparison Between the 2 Groups Regarding Final Follow-Up Satisfaction and Return to Work a
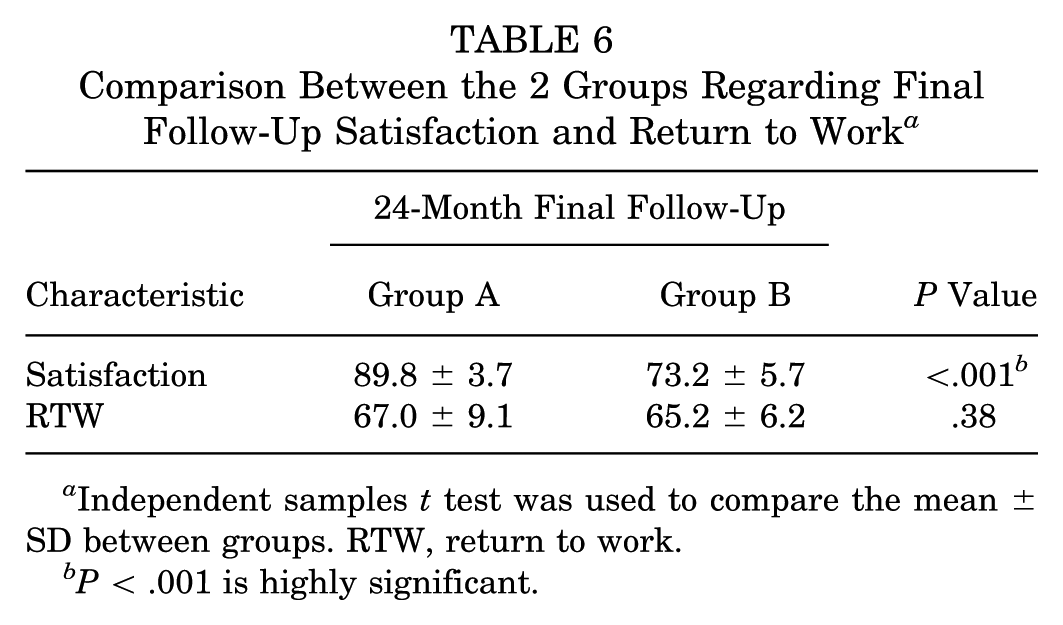
Independent samples t test was used to compare the mean ± SD between groups. RTW, return to work.
P < .001 is highly significant.
Adding SCR to LTTT was strongly correlated with higher patient satisfaction (P < .001). In addition, higher preoperative and postoperative abduction and ER (P = .018), along with better postoperative power in ER (P = .026), were also statistically related to achieving satisfaction.
Apart from biceps cramps, observed in 6 cases (20%) in group A and spontaneously resolving within 6 months after biceps tenotomy, no complications were encountered during this study.
Discussion
The most important finding in this study was that adjuvant SCR using the LHBT in combination with LTTT has the potential to significantly improve patients’ functional outcomes, satisfaction, and AROM without increasing the risk of complications or donor site morbidity, affirming the hypothesis of this study.
In 2016, Elhassan et al 14 presented the LTTT technique for massive posterosuperior RCTs, and in 2020, they published the results of the arthroscopically assisted technique. Since then, there has been growing evidence of the efficiency of this procedure. 13
Evidence regarding the efficiency of LTTT for MIPSRCTs is growing. LHBT-based SCR is indicated in MIPSRCTs with an intact subscapularis, functional deltoid, and usable biceps tendon, especially in young or active patients with minimal arthritis who aim to restore function and avoid arthroplasty. In 2023, Desai et al 11 did a systematic review of the technique, which yielded 37 full-text citations, of which only 5 met their inclusion criteria.13,14,25-27 In 2024, Rodrigo de Marinis et al 10 also systematically reviewed the literature, and only 2 additional articles were included.29,30 Reflecting the scarcity of high-quality evidence, both reviews included 5 common studies, which comprised all the studied articles in the earlier one. None of the articles combined SCR with LTTT. Baek et al 1 essentially compared the results of LTTT to SCR and found that LTTT transfer was associated with better results.
We hypothesized that there is no contradiction between them and that, when performed together, they might improve the functional outcome of patients with MIPSRCTs by enhancing the stability of the humeral head, especially during side ABD.
Improvement in AROM after LTTT transfer is mainly expected in ER and FF. 25 Even though significant improvement in ABD has been reported in some studies, 14 it has not been as noticeable as ER and FF in others,13,14 while a considerable part of the available literature did not mention ABD ROM in their patients.27,29,30,31 This is supported by growing evidence that the main indication for this procedure is ER lag.14,26,27,30 We believe that SCR can improve this aspect of ROM by partly improving the force coupling in the coronal plane against the deltoid muscle, which performs most of the work regarding this specific action.
This study was carried out to assess the value of SCR using the LHBT along with aaLTTT using an autologous peroneus longus tendon graft. To our knowledge, this is the first study to address this issue.
The LHBT tenotomy and tenodesis during LTTT were repeatedly reported in some of the related studies,13,14,27 while other authors overlooked the management of this structure when illustrating their techniques.1,30
However, LHBT transfer during LTTT was performed in a considerable number of patients, as reported by Ye et al, 34 who compared the results of repairing massive reparable RCTs (control group) to those of LTTT in irreparable RCTs (study group). Both groups, in their work, included patients who underwent LHBT transfer using a technique similar to our LHBT SCR (control: 39%, study: 73%). Essentially, they routinely repaired the supraspinatus if feasible (no repairs were done in our work), and the effect of the LHBT transfer on the outcomes of their basic procedures was not specifically mentioned in their results, making comparison of their work to ours methodically unsound.
In 2022, Chiu et al 6 published a thoroughly illustrated technical note on a similar technique to ours for the same indication. They used an autologous semitendinosus tendon (STT) graft, tenotomized and rerouted the LHBT for posterior cortical fixation, and also used cortical fixation with an endobutton for STT fixation. A suture anchor was used for these purposes, and we did not perform LHBT tenotomy during SCR. However, the results of their work were not as well presented as their technique, in comparison to ours.
In 2023, Kandeel 22 published a technical note demonstrating a technique that entailed SCR using the acromially attached intra-articular part of the LHBT and middle trapezius (MT) transfer using the subpectorally tenotomized LHBT as a tendon graft, which had to be 10 cm long, in a biceps-based MT transfer augmented partial repair. Yet, the results of this novel technique remain to be determined through dedicated case series.
In this study, patients who underwent concomitant LHBT SCR combined with LTTT demonstrated significantly greater and earlier improvements in ABD range of motion and ER in ABD, as well as in the motor power of both movements. Additionally, these patients achieved superior outcomes on the CMS, SPADI, and overall patient satisfaction. A positive trend was also observed toward improved outcomes in SSV and active FF ROM.
Our mean active ER in the LHBT SCR group was 54° at the side, which was close to the results of other studies,13,14,25,29,30 but it was 74° in 90° of ABD, which was considerably higher than theirs. Our mean postoperative abduction was higher than in other studies. This can be explained by the greater stability of the glenohumeral articulation in ABD through SCR. When comparing patients in this group to those in a similar group in Ye et al, 34 our mean ABD was considerably higher (156.5° vs 123.26°). This may be because only 73% of their patients underwent biceps transfer.
Several scoring systems have been employed to assess the functional outcomes of the LTTT.10,24 We chose VAS to indicate the level of pain and SSV to assess the overall patient’s view of their shoulder relative to their norm. We also used CMS, which combines ROM and power as objective measurements, performed by physicians, with the patient-measured level of pain and daily activities. SPADI focuses exclusively on patients’ self-reported shoulder status. In 2019, it was recommended as the best shoulder-specific instrument in patients with RCTs. 15 Surprisingly, SPADI was not used in many case series focused on LTTT for MIPSRCT. 9
Patient satisfaction in our control group was rather close to that reported by Stone et al, 30 with very satisfied patients (73% vs 66.7%). They had 33.3% of their patients somewhat satisfied, whereas we considered this to be incomplete satisfaction and treated it as dissatisfaction. Patients with LHBT SCR in our study reported 90% satisfaction, which is closer to that indicated by Rodríguez-Vaquero et al. 28 However, their series included 6 patients, while ours included 60, divided into 2 groups. It is worth noting that patient satisfaction is rarely mentioned in the available literature on LTTT. 10 “Return-to-work” analysis is also scarce in the literature. About 60% of our employed workers in both groups returned to the same work. The rest modified their jobs to less physically demanding ones, as they were manual laborers.
Radiologically, MRI was not routinely performed postoperatively in our study. It was done to further investigate some of our “not completely satisfied” patients. No cases of retear were observed, which helped counsel them. Our mean improvement of AHD was 1.6 mm. This is remarkably lower than the 5.7-mm improvement reported by Elhassan et al, 14 which can be theoretically attributed to the discrepancy in the thickness of the Achilles tendon graft they used and the thickness of the peroneus tendon we used. It is, however, comparable with that of Baek et al 1 (1.5 mm), although they also used an Achilles tendon graft.
LTTT is gaining popularity in the face of other treatment options for MIPSRCTs. However, more randomized controlled trials are needed to compare it to those choices, such as latissimus dorsi transfer (LDT). Two studies compared LDT directly with LTTT for FIRCT.26,29 The first study, by Baek et al, 1 comparing arthroscopic LDT with aaLTTT, found a statistically significant difference favoring aaLTTT over LDT in terms of active ER, American Shoulder and Elbow Society score, and activities of daily living that require active ER score. Woodmass et al, 33 in contrast, found the results of both techniques to be equivalent, and they, interestingly, had a significant improvement in ER only with arthroscopic LDT. Reviewing the LTTT, de Marinis et al 10 linked this exclusive finding to their patients’ higher preoperative mean ER and suggested that the indication is critical for achieving greater ER improvement.
Leading complications after LTTT include seroma or hematoma at the posterior harvest zone,13,14,25,27 followed by arthritic progression, infection,13,14,29 transient neurapraxia, 13 and persistent pain or weakness. 25 The reported reoperation rate ranged between 0% and 20%. 10 We had 1 case of reoperation (1.6%) in the form of arthroscopic release and manipulation under anesthesia and superficial infection at LTTT harvest in 3 patients (5%). No difference existed between both groups regarding the complication rate, and it is worth noting that no donor site morbidity at the ankle was recorded during the period of the study.
The limitations of the study are that it is an observational, retrospective cohort study, which may introduce confounding factors, and a relatively small sample size (30 cases per group), which may increase the risk of type II errors. No blinding was used during data analysis, which may also increase the risk of assessment bias. The long-term impact of peroneus longus tendon harvesting on foot biomechanics is unknown, although current evidence supports the safety of this procedure.
Conclusion
Arthroscopic-assisted LTTT with peroneus longus autograft may be a sound option in the treatment of MIPSRCTs. Adjuvant SCR with LHBT with aaLTTT has the potential to enhance patients’ functional outcomes, satisfaction, and AROM with no increased risk of complications or morbidity.
Footnotes
Acknowledgements
The authors thank all staff members in the Department of Orthopaedic Surgery at all university hospitals in Egypt who participated in the study.
Final revision submitted September 11, 2025; accepted October 6, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Clinical Research Ethics Committee of the Faculty of Medicine, Al-Azhar University, Cairo, Egypt (IRB No. 0018122017).