
Abstract
Background:
The widespread historical abandonment of lateral extra-articular procedures in anterior cruciate ligament (ACL) injuries occurred as a result of concerns about high rates of adverse events. Recently, the popularity of lateral extra-articular procedures has resurged, warranting an urgent evaluation of their safety profile.
Purpose/Hypothesis:
The aim of this study was to perform an interim analysis of the ongoing SANTI randomized controlled trial to determine whether combined ACL and anterolateral ligament reconstruction (ACL + ALLR) is associated with an increased rate of adverse outcomes when compared with isolated ACL reconstruction (ACLR). The hypothesis was that there would be no significant difference between groups at a minimum follow-up of 1 year.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
Recruitment commenced in November 2016. Patients scheduled for ACLR were randomized to either isolated ACLR (with bone–patellar tendon–bone [BPTB] autograft) or combined ACL + ALLR (with hamstring tendon autograft). All patients with a minimum follow-up of 1 year by March 2019 were included. The evaluated parameters included complications and reoperations, knee laxity parameters, range of motion, and scores on the Tegner, Lysholm, International Knee Documentation Committee (IKDC), and Knee injury and Osteoarthritis Outcome Score (KOOS) instruments.
Results:
A total of 224 patients (112 in each group) with a mean ± SD follow-up of 12.3 ± 1.9 months (range, 12-19 months) formed the study population. A significantly higher rate of reoperation for cyclops syndrome was noted in the isolated ACLR group compared with the combined ACL + ALLR group (8.9% vs 0%, respectively; P = .0012). No significant differences were found in frequency of graft rupture (ACLR, 5.4%; ACL + ALLR, 0.9%; P = .1191), range of motion deficits, pain, or reoperation for meniscectomy between groups. No cases of postoperative infection, venous thromboembolism, or arthrofibrosis were seen. Subjective IKDC (81.2 vs 86.8; P = .0048), Lysholm (88 vs 92; P = .0131), and some components of the KOOS were significantly better in the combined ACL + ALLR group.
Conclusion:
This study demonstrates no evidence of an increased risk of short-term adverse events after combined ACL + ALLR compared with isolated ACLR with BPTB graft.
Registration:
NCT03740022 (ClinicalTrials.gov Identifier)
The most frequently used graft choices for anterior cruciate ligament reconstruction (ACLR) in contemporary practice are hamstring tendon and bone–patellar tendon–bone (BPTB) autograft. 17 Although the latter is widely considered the gold standard 5,7,15 and is particularly advocated for high-risk populations, 12,21 numerous meta-analyses comparing these graft types have been unable to demonstrate a clear advantage of one over the other. 8,25,32,39,40 However, it has been reported that the credibility and quality of published meta-analyses have been limited. 25 As a result, it is recommended that decisions regarding graft choice be made on an individual basis, taking into account patient factors and preferences, surgeon experience, and the best available evidence. 25
Recently, several authors have reported a multitude of advantages of combined ACL and anterolateral ligament (ALL) grafts. These advantages have been attributed to load sharing with the ACL graft and improved knee kinematics. 6,23 Comparative studies have demonstrated that concomitant ALL reconstruction (ALLR) is associated with a significantly reduced risk of ACL graft rupture 19,43 and of reoperation for secondary meniscectomy. 42 It has also been reported that the combined procedure is associated with significantly improved knee stability 18,19,26 and rates of return to the preinjury level of sport 26,43 when compared with isolated ACLR. Significant advantages are reported in specific populations, including patients with hyperlaxity, 19 patients with chronic ACL injury, 18 young patients participating in pivoting sports, 43 and patients undergoing revision ACLR. 26 This body of evidence has provided the justification for a randomized controlled trial (RCT) that is currently under way, which seeks primarily to determine whether there is a significant difference in ACL graft failure rates between patients receiving combined ACL + ALLR with hamstring tendon autograft and those undergoing isolated ACLR with BPTB autograft. In this study, the choice of BPTB graft rather than hamstring tendon graft for isolated ACLR was based on the aforementioned fact that BPTB is widely considered the gold standard for young, active patients.
In view of the reported advantages and highly topical nature of ALLR, it is unsurprising that a recent survey of surgical trends identified a resurgence in lateral extra-articular procedures. 46 This trend is in contrast to the widespread abandonment of nonanatomic, iliotibial band–based, lateral extra-articular procedures in the 1980s. 3,11,22,34 This abandonment occurred due to reports of poor outcomes and high rates of complications including infection, stiffness, arthrofibrosis, reoperation for removal of metalwork, and overconstraint. 3,33,35,44 However, Thaunat et al 45 recently reported that there was no evidence of these historical concerns in a large, noncomparative, retrospective series of patients who underwent combined ACL + ALLR. 45 Despite these promising findings, it is recognized that the increased frequency with which lateral extra-articular procedures are being performed warrants a more thorough investigation of the safety profile of current surgical techniques. From an ethical perspective, this concern also mandates that adverse outcomes be monitored during the study period of the ongoing RCT and that an interim analysis of results be undertaken.
The aim of this study was to perform an interim analysis of the ongoing SANTI RCT to determine whether combined ACL + ALLR is associated with an increased rate of adverse outcomes compared with isolated ACLR. The hypothesis was that there would be no significant difference between groups at a minimum follow-up of 1 year.
Methods
Approval was granted for this single-center, prospective RCT, and all patients provided informed consent to participate. All patients who presented with ACL-deficient knees and required surgery for symptomatic instability were screened and considered for study eligibility according to the criteria listed in Table 1.
Inclusion and Exclusion Criteria for Patient Enrollment

A sample size calculation based on the primary outcome measure of graft rupture was performed. Based on data from a previous study, 43 graft rupture rates of 7% in the isolated ACLR group and 2% in the combined ACL + ALLR group were estimated at 2 years of follow-up. It was determined that 296 patients were required in each of the 2 groups to allow an 80% chance of detecting a significant (alpha = 5%) difference in graft rupture rates, with an expected dropout rate of 10%. 9
After patients provided their consent to participate in the study, their allocation to either the isolated ACLR group or the combined ACL + ALLR group in a 1:1 ratio was randomized by use of online software (CSRandomization; ENNOV Clinical). The process of randomization was performed by a research assistant independently of the surgical team. The surgery was performed by 1 of 3 highly experienced senior surgeons (M.T., J.-M.F., B.S.-C.), who respectively perform > 300, > 400, and > 600 ACLRs per year. The surgical technique was standardized according to the technical descriptions below. Meniscal and chondral abnormalities were addressed at the time of ACLR.
Isolated ACLR With BPTB Graft
A 2-incision technique was used. 16 A 10 mm–diameter BPTB graft was harvested with a 9 to 11 × 25–mm bone wedge from the tibia and a 10 × 15–mm bone plug from the patella. No remnant was preserved. After both femoral and tibial tunnels were drilled with an outside-in technique, the BPTB autograft was passed from the femur to the tibia under direct arthroscopic vision. Press-fit graft fixation was obtained in the femoral tunnel, and tibial fixation was achieved with a 9-mm bioabsorbable interference screw (Bio-Interference screw; Arthrex) placed anterior to the graft with the knee at 20° of flexion (Figure 1).

Anterior cruciate ligament reconstruction with bone–patellar tendon–bone graft.
Combined ACL + ALLR With Hamstring Tendon Graft
The semitendinosus and gracilis tendons were harvested with an open tendon stripper. The tibial attachment of the semitendinosus tendon was preserved but the gracilis was detached. The ACL graft comprised a tripled semitendinosus tendon and a single strand of gracilis, the additional length of which formed the ALL graft. An outside-in femoral guide (Arthrex) was placed through the anteromedial portal at the native ACL footprint. Externally, the guide was positioned proximal and posterior to the lateral epicondyle (at the femoral origin of the ALL), and a femoral tunnel was drilled over a guide wire (from 8 to 9 mm average size). For the tibial part of the ALLR, two 4.5 mm–diameter sockets were drilled via stab incisions, 1 just posterior to the Gerdy tubercle and the second one just anterior to the fibula head. These were then converted into a single tunnel using a right-angled clamp. A suture was then passed through the tunnel to create a loop for passage of the ALL graft. The hamstring tendon ALL grafts were routed from the tibia to the femur through the knee and fixed on the tibial side with a bioabsorbable interference screw (Arthrex). The ACL graft was then secured with an outside-in femoral interference screw (Bio-Interference screw; Arthrex) at 20° of flexion. The ALL graft was passed deep to the iliotibial band, but superficial to the fibular collateral ligament, from the femur to the tibia and subsequently shuttled through the tibial bony tunnel and back proximally to the femur. On the femoral side, the sutures holding the ACL graft were then tied around the ALL graft, with the knee placed in full extension and neutral rotation 10,37 (Figure 2).

Combined anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon graft. (Reprinted with permission from Rosenstiel N, Praz C, Ouanezar H, et al. Combined anterior cruciate and anterolateral ligament reconstruction in the professional athlete: clinical outcomes from the Scientific Anterior Cruciate Ligament Network international study group in a series of 70 patients with a minimum follow-up of 2 years. Arthroscopy. 2019;35(3):885-892. ©2019, Elsevier.)
All patients underwent the same rehabilitation. This entailed brace-free, immediate full weightbearing after the procedure and progressive range of motion exercises. The main focus of the early rehabilitation period was on quadriceps activation exercises and regaining full extension. A gradual return to sports activities was allowed, starting at 4 months for nonpivoting sports, 6 months for pivoting noncontact sports, and 8 to 9 months for pivoting contact sports.
Clinical Assessment
Clinical evaluation was undertaken before surgery, postoperatively at 3 and 6 weeks, and then at 3 and 6 months. For the purposes of the interim analysis, the final clinical assessment was at 12 months postoperatively. However, patients continued to be prospectively monitored for the main study, and adverse outcomes were included in the interim analysis, as they occurred, even if they occurred after the 12th postoperative month. At each clinical assessment, an independent, trained evaluator recorded knee range of motion, side-to-side anteroposterior laxity difference (Rolimeter; Aircast), and the Lachman test. The pivot-shift test was evaluated through use of the Kinematic Rapid Assessment (KiRA) system (Orthokey Ltd), 28 and the difference in the tibial acceleration range between knees, before ACLR (under anesthesia), was recorded.
Outcome Measures
The main outcomes of interest for this interim analysis were any adverse events, complications, and reoperations. Graft rupture (determined by clinical examination findings and magnetic resonance imaging evaluation) and contralateral ACL rupture rates were recorded. Additional outcomes recorded included the Tegner, Knee injury and Osteoarthritis Outcome Score (KOOS), International Knee Documentation Committee (IKDC) subjective, and Lysholm scores.
Statistical Analysis
All calculations were made using SAS for Windows (Version 9.4; SAS Institute Inc), with the level of statistical significance set at P < .05. Descriptive data analysis was conducted depending on the nature of the considered criteria. For quantitative data, this included number of observed (and missing, if any) values, means, standard deviations, medians, first and third quartiles, and minimums and maximums. For qualitative data, this included the number of observed (and missing, if any) values and the number and percentage of patients per class. Comparison between unpaired variables was performed using the chi-square or Fisher exact test for categorical variables and the Student or Wilcoxon test for quantitative variables (normality of variables checked). Comparison between paired variables was assessed using the chi-square or Mantel-Haenszel test for categorical variables and the paired Student test or Wilcoxon signed rank test for quantitative variables.
Results
Recruitment to this single-center, prospective RCT commenced in November 2016. All patients who had a minimum follow-up of 12 months after ACLR, on March 25, 2019, were included in the interim analysis. Overall, 224 patients (112 in each group) met this requirement and formed the study population. The mean duration of follow-up was 12.3 ± 1.91 months (range, 12-19 months). The demographic characteristics are reported in Table 2. The mean patient age was 25.3 ± 4.6 years (range, 18-35 years), and 77.7% of patients were male.
Patient Demographics a

a Values are expressed as n (%) unless otherwise noted. Combined ACL + ALLR, anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft; isolated ACLR, anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft.
Complications and Adverse Events
None of the 224 patients included in the interim analysis were diagnosed with postoperative infection (deep or superficial) or venous thromboembolism after ACLR, and none underwent hardware removal. The complications and adverse events that did occur are comprehensively reported in Table 3. There were no significant differences in the frequencies of graft rupture, contralateral ACL rupture, or reoperation for meniscectomy or meniscal repair. However, a significant difference was noted in the rate of reoperation for cyclops syndrome between groups: isolated ACLR group, n = 10 (8.9%); combined ACL + ALLR group, n = 0 (P = .0012). Tables 4 and 5 report data demonstrating that at 12 months of follow-up, there was no significant difference between the groups with respect to pain or range of motion deficits. No other adverse events or complications related to ACLR occurred during the study period. However, in order to be explicit in the reporting of adverse outcomes, the following diagnoses arising from new trauma are reported: 1 patient in the isolated ACLR group experienced a posterior cruciate ligament rupture, and 1 patient in the combined ACL + ALLR group sustained a medial malleolar fracture.
Complications and Adverse Events a

a Values are expressed as n (%). Secondary meniscal procedure defined as reoperation for meniscectomy or meniscal repair. All variables were compared via the Fisher exact test except for cyclops syndrome, which was analyzed using the chi-square test. Boldface values indicate statistical significance. Combined ACL + ALLR, anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft; isolated ACLR, anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft.
Objective IKDC Score: Range of Motion at 1-Year Follow-up a
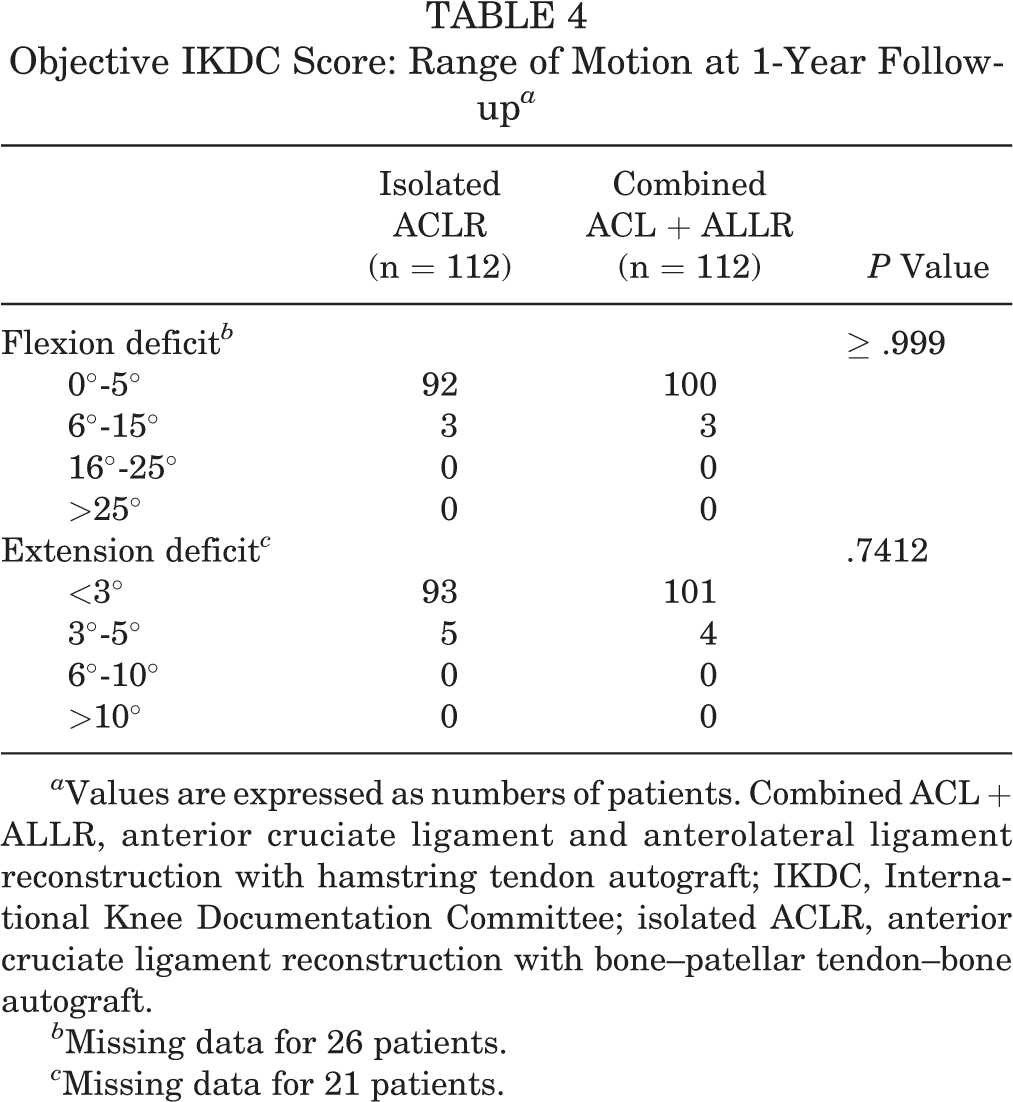
a Values are expressed as numbers of patients. Combined ACL + ALLR, anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft; IKDC, International Knee Documentation Committee; isolated ACLR, anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft.
b Missing data for 26 patients.
c Missing data for 21 patients.
Subjective IKDC Score: Pain at 1-Year Follow-up a

a Values are expressed as numbers of patients. Combined ACL + ALLR, anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft; IKDC, International Knee Documentation Committee; isolated ACLR, anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft.
b Missing data for 25 patients.
Knee Stability
No significant differences were found between groups with respect to side-to-side anteroposterior knee laxity or evaluation of the pivot shift via the KiRA system (Table 6).
Postoperative Outcomes a

a Values are expressed as n (%) or mean ± SD. P values are presented for the Kruskal-Wallis test. Combined ACL + ALLR, anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft; IKDC, International Knee Documentation Committee; isolated ACLR, anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft; KiRA, Kinematic Rapid Assessment.
Clinical Outcome Measures
Clinical outcomes with respect to the IKDC, Lysholm, Tegner, and KOOS values and the mean KiRA and Rolimeter values are reported in Tables 6 and 7. The mean KOOS and Lysholm values at baseline and at 1-year follow-up are reported in Figures 3 and 4.
KOOS Values a

a Data are presented as mean (range). Postoperative KOOS Symptoms, Pain, ADL, and QoL were compared via a Student t test. Postoperative KOOS Sports/Recreation was compared via a Wilcoxon test. ADL, Activities of Daily Living; combined ACL + ALLR, anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft; isolated ACLR, anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, Quality of Life.
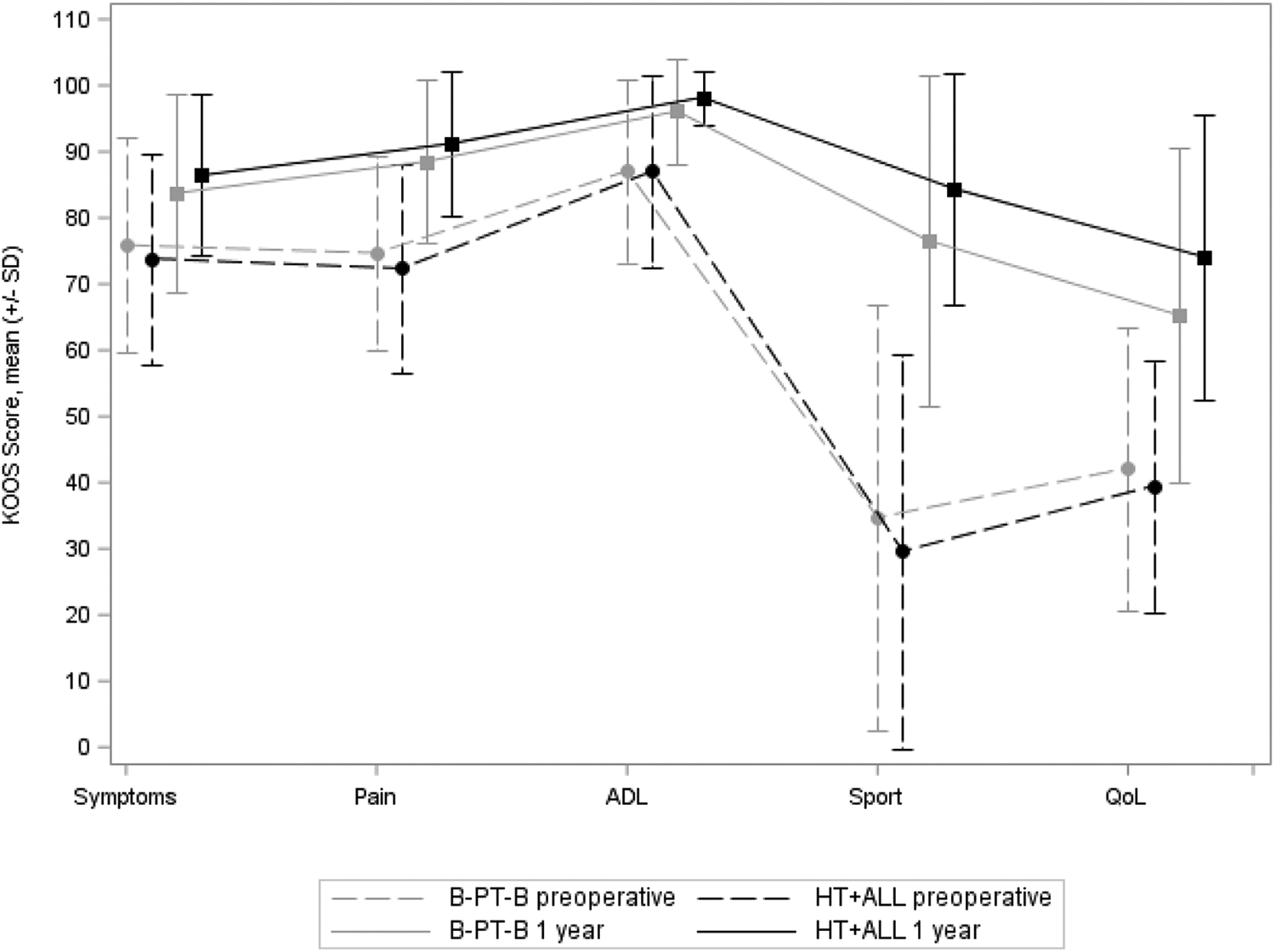
Knee injury and Osteoarthritis Outcome Score (KOOS) values at baseline and 1 year postoperatively. ADL, Activities of Daily Living subscale; B-PT-B, isolated anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft; HT+ALL, combined anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft; QoL, Quality of Life subscale.

Lysholm scores at baseline and 1 year postoperatively. B-PT-B, isolated anterior cruciate ligament reconstruction with bone–patellar tendon–bone autograft; HT+ALL, combined anterior cruciate ligament and anterolateral ligament reconstruction with hamstring tendon autograft.
Discussion
The main finding of this study was that there was no evidence of an increased risk of complications or reoperations with the combined ACL + ALLR procedure when compared with isolated ACLR. No cases of infection, arthrofibrosis, or venous thromboembolism were noted in either group. At 12-month follow-up, there were no significant differences between groups with respect to persistent pain, range of motion deficits, or the rate of reoperation for secondary meniscal procedures. In fact, the only adverse outcome that occurred with a significantly different rate between groups was reoperation for cyclops lesion. Specifically, there were no cases of cyclops lesion in the combined ACL + ALLR group, but the rate in the isolated ACLR group was 8.9% (P = .0012). On that basis, it can be stated that the results of the interim analysis of this RCT provide no evidence to support concerns that the high rates of adverse events reported after historical lateral extra-articular procedures 3,33,35,44 also manifest after the ALL reconstruction technique used in this study.
Potential factors that explain this dissimilitude with historical results include important differences between the surgical techniques and rehabilitation. The procedures that were historically widely abandoned (including Lemaire and McIntosh) used graft harvest from the iliotibial band (an important secondary stabilizer), were nonanatomic, and were often associated with prolonged periods of immobilization in extension. 14 In contrast, combined ACL + ALLR uses a percutaneous technique that avoids the morbidity of a large lateral incision and violation of the iliotibial band. The procedure is anatomically based, and the rehabilitation is unchanged from a standard contemporary program. 41
The results of this study are consistent with previous work. 14,30,43,45 Thaunat et al 45 reported clinical outcomes of combined ACL + ALLR in 548 patients with a mean follow-up of 35.5 months (range, 24-54 months). To our knowledge, the Thaunat et al study is the largest published series of any type of lateral extra-articular procedure and the only previously published study that specifically focuses on reoperation rates and complications. Thaunat et al reported that the combined procedure was associated with a very low rate of specific complications (0.5%) and a reoperation rate of 13.1%. 45 The much lower reoperation rate in the current study is likely to be a reflection of the considerably shorter follow-up period. Although direct comparisons could not be made with other studies, Thaunat et al 45 highlighted that in large series of isolated ACLRs with similar durations of follow-up, reported rates of reoperation have varied between 18.9% and 26.7%. 20,24
Although the main focus of this study was early identification of any increased risk of adverse outcomes of combined ACL + ALLR, it is also appropriate to comment on whether the outcomes are consistent with expectations and the previous literature. 1 Based on previous reports, 14,29,30,43 there was an expected trend toward a lower graft rupture rate with combined ACL + ALLR (0.9%) compared with isolated ACLR with BPTB autograft (5.4%; P = .1191) and significantly improved subjective IKDC, Lysholm, and KOOS (Quality of Life and Activities of Daily Living subscale) scores.
It is interesting to note that the rate of reoperation for cyclops lesions was significantly higher in the isolated ACLR group. Numerous reports, including meta-analyses, indicate that ACLR with a BPTB graft is associated with a significantly higher risk of extension deficit, 2,4,13,27,31,38,47 although this is not a universal finding. It is also of note that early extension deficit after ACLR is a recognized risk factor for cyclops lesion, 36 and this may explain the findings of the current study.
The main limitation of this study, due to the inherent nature of an interim analysis, is that the requirements of the sample size calculation have not been met, and recruitment is ongoing. However, there is a need to publish these preliminary results in view of the resurgence in popularity of lateral extra-articular procedures and the counterpoise with historical concerns regarding adverse outcomes. Although the possibility of underpowering of this study exists, the sample size calculation was based on a primary outcome measure of graft rupture and not the main outcomes of interest (adverse events) of this interim analysis. Some readers may question the choice of different grafts for the isolated and combined procedures. As several important studies have demonstrated a lower failure rate with isolated bone-patellar tendon-bone grafts than with isolated hamstring grafts, we wanted to compare the ACL + ALLR technique to this higher gold standard. Further limitations of this study include the lack of blinding and the relatively short minimum follow-up period of 1 year. This duration of follow-up was specifically chosen as part of the safety monitoring of this RCT. However, it is clear that the risk of reoperation after ACLR increases with the passage of time, and this study would have been able to reliably capture only early complications (occurring within 12 months after surgery). Furthermore, it is widely accepted that some outcomes such as return-to-sport rates and patient-reported outcome measures are best evaluated with a minimum follow-up of 2 years.
Conclusion
This study demonstrates no evidence of an increased risk of adverse events after combined ACL + ALLR when compared with isolated ACLR with a BPTB graft in the first year following surgery.
Footnotes
Final revision submitted November 26, 2019; accepted December 17, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.-C. has received research support, consulting fees, speaking fees, and royalties from Arthrex. J.-M.F. has received research support, consulting fees, and speaking fees from Arthrex. M.T. has received research support, consulting fees, and speaking fees from Arthrex. A.S. has received consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the CPP Sud-Est III Comite de Protection des Personnes (Research ethics committee approval No. 2016-007B).