
Abstract
Background:
A preoperative high-grade pivot-shift phenomenon (2+ and 3+) is often a predictor of inferior knee rotational stability and excessive anterior tibial translation of the lateral compartment (L-ATT) after an anterior cruciate ligament (ACL) injury. Lateral extra-articular tenodesis (LET) has been reported to reduce failure rates and improve knee stability in patients with an ACL injury. However, the effect of LET on knee rotational stability and L-ATT is still not entirely clear in patients with an ACL injury and a high-grade pivot-shift phenomenon.
Purpose:
To explore the effect of LET on knee rotational stability and L-ATT in patients with an ACL injury and a high-grade pivot-shift phenomenon.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 254 patients who underwent ACL reconstruction (ACLR) between January 2019 and December 2020 were retrospectively reviewed, and 71 patients (43 male and 28 female) with a preoperative high-grade pivot-shift phenomenon were included. Of these, 24 patients who underwent ACLR combined with LET and 47 patients who underwent ACLR alone were categorized as the study and control groups, respectively. Knee stability was evaluated by the KT-1000 arthrometer side-to-side difference and the pivot-shift test, and L-ATT was measured on magnetic resonance imaging. Baseline patient characteristics, preoperative and postoperative knee stability, and preoperative and postoperative L-ATT were compared between the 2 groups. Moreover, the relative risk of a residual pivot-shift phenomenon after ACLR combined with LET versus ACLR alone was calculated.
Results:
The mean time from injury to surgery in the study group was significantly longer than that in the control group (29.9 ± 54.7 vs 10.1 ± 23.1 months, respectively; P = .035). Other baseline patient characteristics, preoperative knee stability, and preoperative L-ATT showed no significant differences between the groups. At the final follow-up (26.4 ± 4.7 and 28.1 ± 11.0 months for study and control groups, respectively), knee rotational stability (residual pivot-shift phenomenon: 2/24 vs 16/47, respectively; P = .018) and L-ATT (4.6 ± 2.6 vs 6.3 ± 2.6 mm, respectively; P = .010) were superior in the study group compared with the control group. Furthermore, the relative risk of a residual pivot-shift phenomenon was significantly lower in the study group (0.176 [95% CI, 0.037-0.845]; P = .030).
Conclusion:
ACLR combined with LET was an effective treatment strategy for ACL injuries with a high-grade pivot-shift phenomenon, associated with satisfactory clinical outcomes, significantly improved rotational stability, and reduced L-ATT.
Keywords
Recent increases in the understanding of knee anatomy and biomechanical mechanisms have led to satisfactory clinical outcomes after anterior cruciate ligament (ACL) reconstruction (ACLR).11,26 Nevertheless, persistent knee instability and excessive anterior tibial translation (ATT) continue to pose significant challenges, hindering athletes from achieving preinjury levels of sports performance.13,24 Previous studies have shown that residual knee instability after ACLR not only damages knee function but also leads to cartilage and meniscus degeneration or even graft failure.4,13
The pivot-shift test is a common physical maneuver to assess knee rotational stability in clinical practice. The presence of a high-grade pivot-shift phenomenon (2+ and 3+) indicates inferior knee rotational stability and potential injuries to secondary stable structures in the knee joint.23,29 Unlike physical measures of dynamic laxity such as ligament arthrometry and the pivot-shift test, ATT has been used to evaluate the pathological static tibiofemoral relationship in the context of ACL deficiency. 1 Previous research has identified that this aberrant tibiofemoral alignment is particularly pronounced in the lateral compartment, often leading to knee rotational instability, impingement of the ACL graft, and, in some cases, graft failure after ACLR.14,19,32 Thus, the above findings raise concerns about how to manage ACL injures along with a preoperative high-grade pivot-shift phenomenon and excessive ATT of the lateral compartment (L-ATT) using other combined surgical procedures.
Recent studies have noted that anterolateral ligament (ALL) injuries are common in patients with ACL injuries.23,27,33 Therefore, ALL reconstruction and lateral extra-articular tenodesis (LET) procedures have been increasingly applied in clinical practice during ACLR.10,20 According to anatomic and biomechanical studies, the ALL plays an important role in assisting the ACL in maintaining anterolateral rotational stability.6,12 For patients with ACL injuries combined with a preoperative high-grade pivot-shift phenomenon, expected postoperative clinical outcomes are inferior to those without. 15 However, the effect of LET on knee rotational stability and L-ATT remains unclear for this special subset of patients.
Thus, the aim of this study was to explore the effect of LET on knee rotational stability and L-ATT in patients with an ACL injury with a preoperative high-grade pivot-shift phenomenon. It was hypothesized that ACLR plus LET would significantly reduce the rate of a residual pivot-shift phenomenon and L-ATT compared with ACLR alone.
Methods
Patient Selection
A consecutive sample of 254 patients with a clinically diagnosed ACL injury in our department between January 2019 and December 2020 were retrospectively reviewed. Patients were included if they met the following criteria: (1) had a noncontact ACL rupture confirmed by history, magnetic resonance imaging, and a physical examination; (2) underwent single-bundle ACLR with a hamstring tendon autograft; and (3) had a combined high-grade (2+ and 3+) pivot-shift phenomenon assessed intraoperatively under anesthesia. Patients were excluded if they (1) had multiple ligament injuries requiring surgical treatment, (2) underwent revision ACLR, (3) had a history of surgery on the ipsilateral knee joint, (4) had open epiphyseal plates, or (5) were lost to follow-up within 2 years.
The application of the above criteria left 71 patients; 24 patients who underwent ACLR combined with LET were regarded as the study group, and 47 patients who underwent ACLR alone were allocated to the control group (Figure 1). This study was approved by our hospital’s ethics board (No. JST 202 306 08), and informed consent was obtained from all participants.
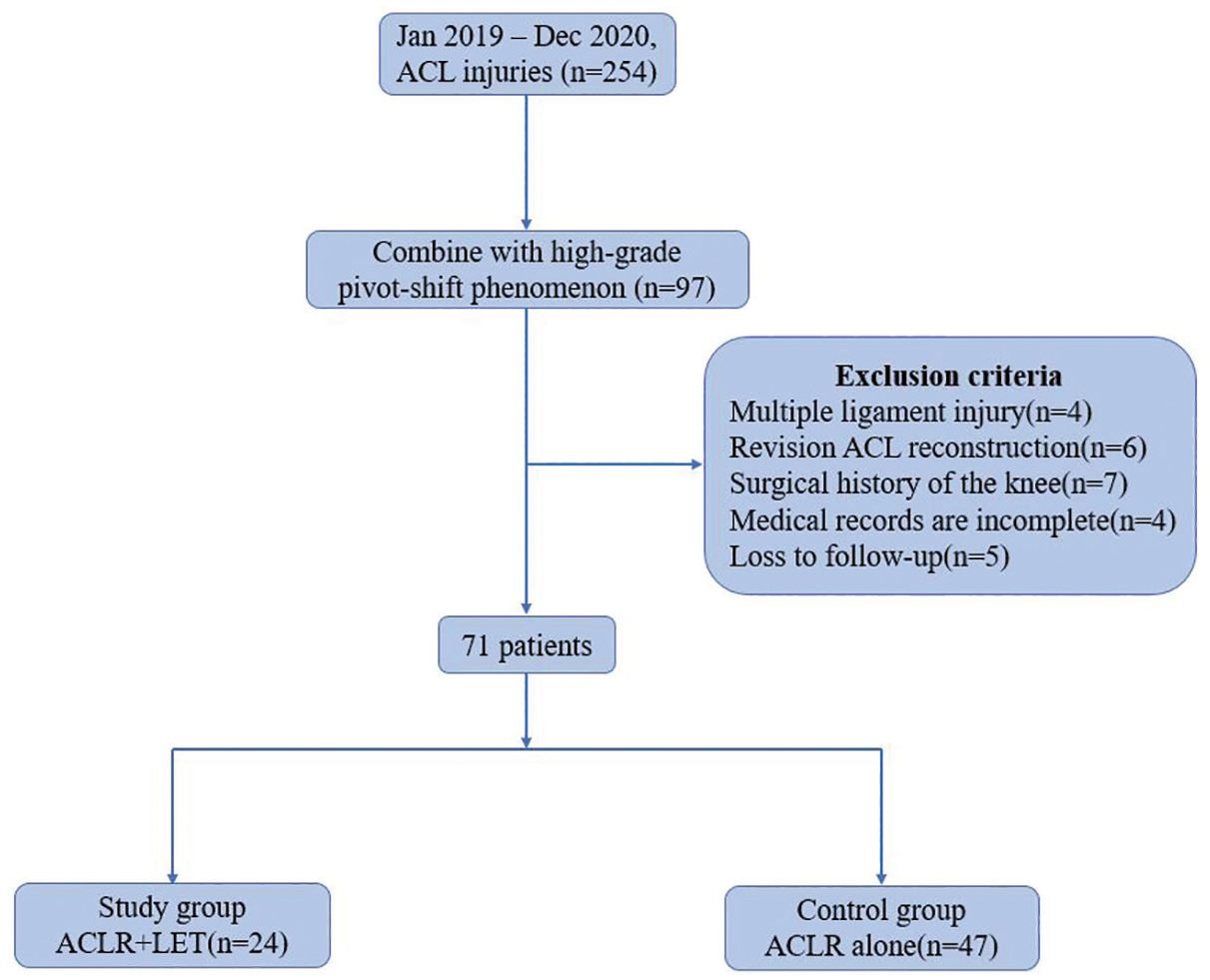
Flowchart of the study. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; LET, lateral extra-articular tenodesis.
Data Collection
Age, sex, body mass index, side of injury, and side of meniscal injury were retrospectively reviewed form medical records. The time from injury to surgery was determined as the interval from the initial ACL injury to ACLR, and follow-up time was calculated from surgery to the last follow-up. Also, the posterior tibial slope was measured on whole-leg radiography using a previously reported method. 19
Physical Examination
Senior physicians (H.Z. and L.G.) with over 20 years of clinical orthopaedic experience conducted knee stability examinations. The KT-1000 arthrometer side-to-side difference (SSD; assessing anterior-posterior stability) and the pivot-shift test (assessing rotational stability) were performed during the physical examination. Both evaluations were performed with the patients under anesthesia, and the first and second evaluations were performed immediately before ACLR and hardware removal surgery, respectively.
KT-1000 Arthrometer SSD
After the patients were placed in the supine position with the knee flexed at 30°, the KT-1000 arthrometer (MEDmetric) was utilized with maximal manual anterior forces, and the SSD was recorded.
Pivot-Shift Test
The pivot-shift test was utilized to mimic the process from anterior subluxation to restoration of the proximal tibia, and the result was graded as 0 (negative), 1+ (glide), 2+ (clunk), and 3+ (locking), which were further categorized as low grade (0 and 1+) and high grade (2+ and 3+). 30
L-ATT Measurement
L-ATT measurements were completed by a single observer (J.-T.L.), who was blinded to the patients’ grouping. The measurement was performed on sagittal magnetic resonance imaging using the technique described by a previous study. 30 The scan showing the most medial cut of the fibula at the tibiofibular joint was selected to perform measurements. First, a best-fit circle was drawn over the posterior femoral condyle at the subchondral bone, and then, a line tangent to the lateral tibial plateau was confirmed. Next, the distance between 2 parallel lines perpendicular to the tibial plateau, which were drawn tangent to the posterior margin of the circle and the tibial plateau, respectively, determined the amount of L-ATT (Figure 2).
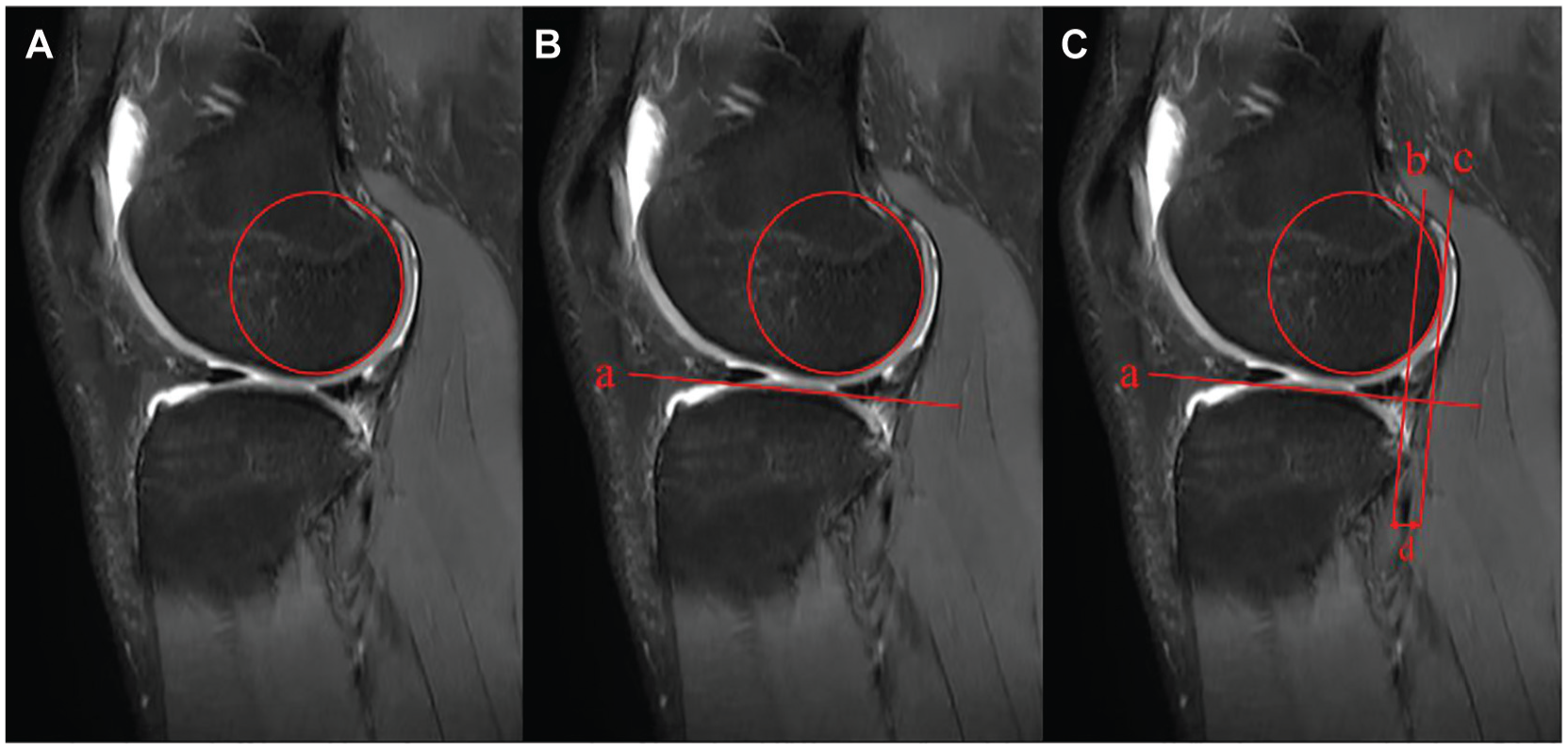
Measurement technique of anterior tibial translation of the lateral compartment (L-ATT). (A) A best-fit circle was drawn over the posterior femoral condyle at the subchondral bone. (B) A line tangent to the lateral tibial plateau was confirmed (line a). (C) The distance between 2 parallel lines (lines b and c) perpendicular to the tibial plateau, which were drawn tangent to the posterior margin of the circle and the tibial plateau, respectively, determined the amount of L-ATT (d).
Surgical Technique
All the patients in this study underwent primary single-bundle ACLR with a 4- to 6-strand hamstring tendon autograft (graft diameter of at least 8.0 mm). The surgical procedures were performed by 2 senior surgeons (H.Z. and L.G.) with the patients under lumbar anesthesia. The femoral tunnel was drilled with an inside-out technique, and the location was determined using the quadrant method intraoperatively with true lateral radiography. 3 The tibial tunnel was positioned at the center of the native ACL footprint and drilled with an outside-in technique. During ACLR, the meniscal injury was repaired or partially excised according to the type of the tear, location of the tear, and quality of the meniscus. The XO Button (ConMed) and IntraFix tibial system (DePuy Synthes) were used for femoral- and tibial-side fixation, respectively. In addition to the IntraFix tibial system, an extra screw was added on the tibial side for double fixation to improve fixation strength and accelerate recovery. At 2 years after ACLR, the screw could be removed at the request of patients, and the follow-up physical examination could be performed at the same time.
As of yet, there exists no consensus regarding the appropriate indications for LET in surgical practice. In the context of this study, the decision to utilize the LET procedure was guided by specific criteria, which were applied in patients with an ACL injury exhibiting a high-grade pivot-shift phenomenon preoperatively. These criteria included the following: (1) young patients who participated in demanding sports that involved the pivot mechanism; (2) professional athletes who aspired to continue their sports career; (3) cases in which the pivot-shift test result remained positive after the ACL graft was stretched tight, with no injury in the posterior horn of the lateral meniscus, or if the tear had been effectively repaired; and (4) patients with knee hyperextension >10° or those demonstrating laxity in multiple joints. The study’s use of these criteria aimed to clarify the scenarios in which the LET procedure would be most advantageous, enhancing the precise role of the technique in surgery.
The detailed steps of LET are as follows. First, the iliotibial band was exposed after a curved incision was made from the Gerdy tubercle to the lateral femoral condyle. An approximately 10 mm–wide and 10 cm–long iliotibial band was prepared with the Gerdy tubercle connection reserved (Figure 3A), and then, the iliotibial band strip was whipstitched and passed beneath the lateral collateral ligament (LCL) (Figure 3B). In place of the lateral femoral condyle, the femoral insertion of the LCL was exposed, and then, a K-wire was drilled approximately 1 cm from the femoral insertion of the LCL posteriorly and proximally. Next, the woven iliotibial band strip was entangled in the K-wire for isometric testing during knee flexion and extension. Finally, a tunnel with a diameter of 6 or 7 mm was drilled after the isometric point was identified (Figure 3C), and then, the woven iliotibial band strip was pulled into the tunnel and fixed with an interference screw (Figure 3D).

Steps of the lateral extra-articular tenodesis technique. (A) A 10 mm–wide and 10 cm–long iliotibial band (white arrow) was prepared with the Gerdy tubercle connection reserved. (B) The iliotibial band strip was whipstitched and passed beneath the lateral collateral ligament (black arrow). (C) A tunnel was drilled after the isometric point (red arrow) was identified. (D) The woven iliotibial band strip was pulled into the tunnel and fixed.
Rehabilitation Protocol
All patients in this study followed the same rehabilitation protocol. A hinged knee brace was used immediately after surgery; the brace was opened to allow passive range of motion from 0° to 90°, free from weightbearing, for the first 2 weeks. Partial weightbearing was started at 2 weeks postoperatively with the protection of the brace, and active and passive knee flexion and extension were allowed from 0° to 120°. From 4 to 8 weeks, full weightbearing and active full range of motion were permitted; after that, the knee brace could be removed, and daily activities were encouraged. The preinjury level of sports was not allowed until 9 to 12 months after surgery.
Statistical Analysis
Statistical analyses were conducted with SPSS software (Version 25.0; IBM). Descriptive statistics were calculated for patient characteristics and physical examination results. For comparative analyses within and between groups, the chi-square test or Fisher exact test was utilized for categorical variables, and the Student t test or Mann-Whitney U test was used for continuous variables according to the assumption of normality and homoscedasticity. Moreover, the relative risk (RR) of a residual pivot-shift phenomenon after ACLR combined with LET versus ACLR alone was calculated. Statistical significance was set at P < .05.
Results
Patient Characteristics
According to the inclusion and exclusion criteria, a total of 71 patients (43 men and 28 women) were enrolled in this study. There were 24 patients (16 men and 8 women) allocated to the study group, and the other 47 patients (27 men and 20 women) were allocated to the control group. The study group had a significantly longer mean time from injury to surgery than the control group (29.9 ± 54.7 vs 10.1 ± 23.1 months, respectively; P = .035). No significant differences were found between the groups in terms of age, sex, body mass index, side of injury, side of meniscal injury, follow-up time, posterior tibial slope, and preoperative L-ATT. Moreover, there was no significant difference between the groups in regard to preoperative anterior-posterior and rotational stability evaluated with the KT-1000 arthrometer SSD and pivot-shift test, respectively (Table 1).
Baseline Characteristics of Patients a

Data are presented as No. or mean ± SD. L-ATT, anterior tibial translation of lateral compartment; SSD, side-to-side difference. Bold denotes statistical significance.
Knee Stability
There was no statistically significant difference in preoperative knee stability (evaluated by the KT-1000 arthrometer SSD and pivot-shift test) between the 2 groups. At the final follow-up, anterior-posterior and rotational stability were both improved compared with preoperatively (both P < .001). Moreover, the study group demonstrated superior knee rotational stability compared with the control group (residual pivot-shift phenomenon: 2/24 vs 16/47, respectively; P = .018) (Table 2). However, although the mean KT-1000 arthrometer SSD in the study group was smaller than that in the control group, the difference between the 2 groups was still not significant (1.1 ± 1.7 vs 2.1 ± 2.3 mm, respectively) (Table 2).
Preoperative and Postoperative Physical Examination Results a
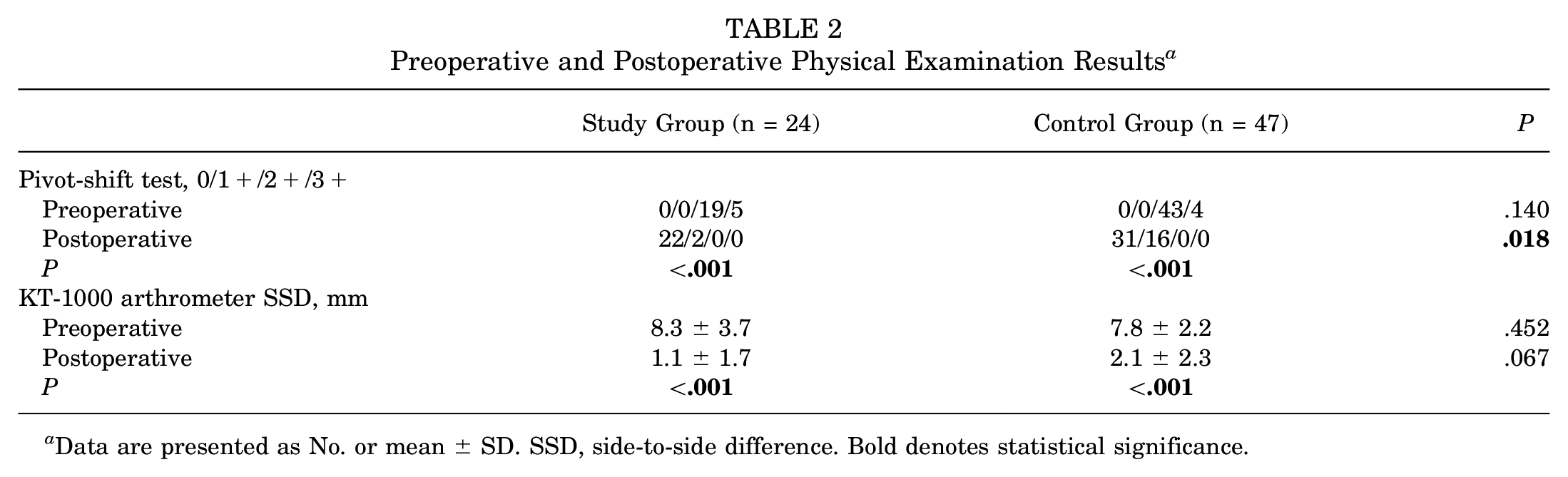
Data are presented as No. or mean ± SD. SSD, side-to-side difference. Bold denotes statistical significance.
L-ATT Measurement
Compared with preoperatively, the postoperative L-ATT was significantly reduced in both the study and control groups (P < .001 and P = .005, respectively). Furthermore, the mean postoperative L-ATT in the study group was significantly smaller than that in the control group (4.6 ± 2.6 vs 6.3 ± 2.6 mm, respectively; P = .010), despite no significant difference between the groups preoperatively (8.1 ± 2.7 vs 7.0 ± 2.6 mm, respectively) (Table 3).
Preoperative and Postoperative L-ATT Measurements a

Data are presented as mean ± SD. L-ATT, anterior tibial translation of lateral compartment. Bold denotes statistical significance.
Further Analysis of RR Value
To evaluate the effect of LET on reducing the rate of a residual pivot-shift phenomenon, the RR of a residual pivot-shift phenomenon after ACLR combined with LET versus ACLR alone was calculated. Analysis showed that the RR of a residual pivot-shift phenomenon in the study group was significantly lower than in the control group (RR, 0.176 [95% CI, 0.037-0.845]; P = .030).
Discussion
The principal finding of this study is that for patients with an ACL injury with a preoperative high-grade pivot-shift phenomenon, combined ACLR and LET was associated with superior knee rotational stability and significantly reduced the rate of a residual pivot-shift phenomenon and L-ATT compared with ACLR alone.
ACLR is one of the most common and effective procedures in the sports medicine field.8,26 However, it cannot be denied that some patients with ACL injuries have residual knee instability, especially rotational instability evaluated with the pivot-shift test. Previous studies have reported that the incidence of a residual pivot-shift phenomenon is approximately 30% after ACLR.10,22 Patients not only exhibit reduced knee functional scores but also face significant challenges in returning to their preinjury sports levels because of compromised knee stability. Furthermore, they are at an increased risk of experiencing ACL graft failure or other associated complications. In the present study, the incidence of a residual pivot-shift phenomenon in the control group was 34.0% (16/47), a figure that is slightly elevated compared with previous findings.10,22 This discrepancy can be attributed to our study’s inclusion criteria, which specifically targeted patients with a high-grade pivot-shift phenomenon resulting from ACL injuries. A preoperative high-grade pivot-shift phenomenon is often associated with damage to secondary stabilizing structures of the knee.23,29 Consequently, this population is more likely to exhibit a higher rate of residual knee instability after ACLR.
ATT refers to anterior subluxation of the proximal tibia relative to the femoral condyle, 1 which has become a growing concern in recent years, as an altered tibiofemoral relationship can adversely affect the restoration of normal knee kinematics.7,24 Previous studies have demonstrated that excessive ATT is correlated to diminished knee stability and, in some cases, ACL graft failure.19,24,32 Furthermore, it has been observed that ACLR alone may not fully restore ATT to its preinjury state. 28
Considering the ongoing issue of a residual pivot-shift phenomenon and unaddressed ATT after ACLR, the identification of risk factors contributing to residual knee instability after ACLR is imperative for the refinement of surgical techniques and the enhancement of clinical outcomes, presenting an urgent problem that requires a timely solution. Some previous research has shown that ACLR combined with ALL reconstruction/LET could reduce the failure rate and restore knee kinematics with improved knee rotational stability and decreased ATT.5,9,17,18,20,21,31 Onggo et al 20 conducted a meta-analysis and systematic review of randomized controlled trials (RCTs) to directly compare ACLR with LET and ACLR alone in terms of clinical outcomes and complications. A total of 517 LET and 589 non-LET cases were included in 7 RCTs with level 1 evidence; the results showed that the LET group had significantly improved anterolateral knee stability (residual pivot-shift phenomenon: RR = 0.59) and a reduced graft rerupture rate (RR = 0.31) after primary ACLR. Similarly, Getgood et al 6 conducted a multicenter, prospective RCT to explore whether LET could reduce the risk of ACLR failure in young, active patients. A total of 589 patients completed 2 years of follow-up; they found that the addition of LET to ACLR resulted in a statistically significant, clinically relevant reduction in graft ruptures (4% vs 11%, respectively; RR = 0.67) and persistent rotary laxity (25% vs 40%, respectively; RR = 0.38) at 2 years after surgery compared with ACLR alone. In the current study, the rate of a residual positive pivot-shift test result in the study group was 8.3% (2/24), which is a statistically significant reduction compared with the control group (34.0% [16/47]). Additionally, the mean postoperative L-ATT in the study group was markedly reduced relative to that in the control group (4.6 ± 2.6 vs 6.3 ± 2.6 mm, respectively; P = .010), despite comparable preoperative L-ATT values (8.1 ± 2.7 vs 7.0 ± 2.6 mm, respectively; not significant). These results suggest that the LET procedure can significantly enhance knee rotational stability as assessed by the pivot-shift test and effectively diminish L-ATT in patients with an ACL injury presenting with a preoperative high-grade pivot-shift phenomenon, which is consistent with findings observed in previous studies.
The RR of a residual pivot-shift phenomenon after ACLR combined with LET was 0.176 (95% CI, 0.037-0.845; P = .030). This indicates that the rate of a residual positive pivot-shift test result could be reduced, on average, by 82.4% when the LET procedure is performed concurrently with ACLR. These findings are encouraging and underscore the critical role of the LET procedure in enhancing knee rotational stability during ACLR, aligning with the outcomes of previous clinical and biomechanical studies.5,21,31 Among those studies, Xu et al 31 performed a meta-analysis with a high evidence level (only level 1 and 2 clinical studies included) to explore the effect of combined ALL reconstruction and ACLR on reducing the pivot-shift rate. Their findings revealed that patients who underwent combined ACLR and ALL reconstruction exhibited a significantly lower rate of a positive pivot-shift test result compared with those who underwent isolated ACLR (odds ratio, 0.46 [95% CI, 0.23-0.92; P = .03). Those clinical and biomechanical studies showed that combined LET and ACLR could significantly reduce residual rotary instability and help to restore normal kinematics of the knee.
Several different ALL reconstruction/LET techniques have been proposed and applied in clinical practice, and the modified Lemaire technique was utilized in this study. A recently published meta-analysis included 28 studies with a total of 2990 patients; it demonstrated that ACLR + the Coker-Arnold technique, the Lemaire technique, and ALL reconstruction resulted in a significantly lower ACL rerupture rate and a reduced rate of a residual pivot-shift phenomenon. 9 However, there is still no consensus about the indications for the application of ALL reconstruction/LET in clinical practice. In the study by Mahmoud et al, 16 the indications were grade 1 or 2 lateral laxity, hyperextension laxity, and/or increased rotational laxity of 5° to 10°. Ariel de Lima et al 2 suggested that the surgical indications for LET should be the following: revision ACLR, grade 2+ or 3+ pivot-shift test result, practice of sports with a pivot mechanism and/or a high mechanism level, chronic ACL injury, ligament laxity, and Segond fracture. Meanwhile, the indications for ALL reconstruction established by Sonnery-Cottet et al 25 were revision ACLR, high-grade pivot-shift test result, chronic ACL rupture, young patients, pivoting activities, and patients undergoing medial meniscal repair. It is obvious that further research is needed to determine the appropriate indications for the application of ALL reconstruction or LET. In the present study, previous literature was referenced, and actual situations were considered. Finally, the indications for LET were determined as mentioned in the Methods section.
Several limitations of this study warrant acknowledgment. First, the retrospective nature of this research introduces potential confounding biases that cannot be entirely mitigated. Second, the modest sample size and brief follow-up period employed in this study may limit the generalizability of the findings; an expanded sample size and extended follow-up duration would bolster the robustness and credibility of the conclusions. Furthermore, the pivot-shift test is a subjective physical maneuver that was used based on the experience of the researchers, and the examinations in this study were conducted by the same senior surgeons; thus, the results are credible.
Conclusion
LET was an effective technique, combined with ACLR, for patients with ACL injuries and a preoperative high-grade pivot-shift phenomenon, which significantly enhanced knee rotational stability as measured by the pivot-shift test and effectively decreased L-ATT of the knee.
Footnotes
Final revision submitted September 17, 2024; accepted November 6, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.Z. has received funding from the National Natural Science Foundation of China (82172514) and the Beijing Municipal Science & Technology Commission (Z211100002921043 and Z221100007422004). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the review board of the Beijing Jishuitan Hospital (No. JST 202 306 08).