
Abstract
Background:
After its success in restoring rotational stability and reducing failure rates in primary anterior cruciate ligament reconstruction (ACLR), lateral extra-articular tenodesis (LET) or anterolateral ligament reconstruction (ALLR) has been endorsed for use in revision ACLR surgery, where failure rates are historically higher.
Purpose:
To perform a systematic review and meta-analysis on whether the addition of a LET or ALLR results in superior clinical outcomes and stability compared with isolated revision ACLR (iACLR).
Study Design:
Meta-analysis; Level of evidence, 4.
Methods:
The Cochrane Controlled Register of Trials, PubMed, Medline, and Embase were used to perform a systematic review and meta-analysis of comparative studies using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) criteria with the following search terms: (“extra-articular” OR “tenodesis” OR “anterolateral ligament” OR “iliotibial”) AND (“anterior cruciate ligament”) AND (“revision” OR “re-operation”). Data pertaining to all patient-reported outcome measures (PROMs), rotational stability, and postoperative complications were extracted from each study.
Results:
After abstract and full-text screening, 10 clinical comparative studies were included. There were 793 patients, of whom 390 had an iACLR while 403 had an ACLR augmented with a LET or an ALLR (augmented ACLR [aACLR]). The mean time for assessment of PROMs was 35 months. The aACLR group had superior International Knee Documentation Committee (IKDC) scores (standardized mean difference [SMD], 0.27; 95% CI, 0.01 to 0.54; P = .04), rotational stability (odds ratio [OR], 2.77; 95% CI, 1.91 to 4.01; P < .00001), and lower side-to-side difference (OR, −0.53; 95% CI, −0.81 to −0.24; P = .0003) than those without the augmentation. Furthermore, they were less likely to fail (OR, 0.44; 95% CI, 0.24 to 0.80; P = .007). Subgroup analysis in the higher-grade laxity cohort (grade ≥2) revealed an even greater IKDC score (SMD, 0.51; 95% CI, 0.16 to 0.86; P = .005) and an improved Lysholm score (SMD, 0.45; 95% CI, 0.24 to 0.67; P < .0001) in the aACLR group.
Conclusion:
Revision aACLR with a LET or an ALLR can improve subjective IKDC scores, restore rotational stability, and reduce failure rates compared with iACLR. Although controversy remains on the necessity of augmenting all revision ACLRs, the present meta-analysis advocates adding a lateral procedure, particularly in those with a higher-grade pivot shift.
Keywords
The rate of success of anterior cruciate ligament (ACL) reconstruction (ACLR) ranges13,59 from 75% to 95%, with most patients returning to a desired performance level and regaining knee stability. However, as the incidence of ACLR procedures has increased, the number of revision surgeries has concurrently risen. 29 A residual positive pivot shift has been described as a significant negative predictive factor and is associated with failure in patients undergoing ACLR,4,24,26,57 a phenomenon that mandates revision surgery. 8
Several technical factors—such as optimal tunnel placement and aperture fixation—as well as graft considerations—such as double-bundle and anatomic single-bundle reconstructions—have been explored as means to prevent the failure of ACL reconstruction.6,8,36,46,47
There has been a renewed interest in the anterolateral complex of the knee, with many biomechanical studies stressing its importance as a secondary restraint to anterior displacement and internal rotation of the tibia.10,17,21,32,33 If the anterolateral complex is disrupted, a higher-grade pivot shift and marked anterolateral laxity can occur.19,39,44
After its success in restoring rotational stability and reducing failure rates in primary ACLR for high-risk patients,31,41,50 the use of lateral extra-articular tenodesis (LET) or anterolateral ligament (ALL) reconstruction (ALLR) for revision surgery, where failure rates have historically been higher than primary procedures, has been endorsed by authors.37,42 In addition, its load-sharing effects can provide a protective element from undesired stresses during the early phases of rehabilitation.7,12 A recent consensus meeting of leading experts suggests that LET or ALLR should be considered when performing ACLR revision, particularly in patients with clinical rotatory instability. 40
Whether the addition of a LET or ALLR is truly superior to isolated revision ACLR is unclear. A recent qualitative synthesis supported the use of LET/ALLR. 14 However, this was predominantly evaluating case series, as not enough comparative studies were present at the time to support the technique.
We therefore performed a systematic review and meta-analysis on clinical comparative studies to investigate whether ACLR revision augmented with LET/ALLR (aACLR) had superior clinical outcomes and rotational stability compared with isolated revision of ACLR (iACLR).
Methods
Literature Review
A systematic review and meta-analysis was performed and reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 30 The Cochrane Controlled Register of Trials, PubMed, Medline, and Embase were searched from the inception of the databases to August 2, 2022. The search terms included “extra-articular” OR “tenodesis” OR “anterolateral ligament” OR “iliotibial” AND “anterior cruciate ligament” AND “revision” OR “re-operation.” No restriction was made on language, and efforts were made to obtain translated versions of all included studies. No restrictions were placed on the date of publication or the impact factor of the journal. All relevant articles and reviews were examined for further relevant citations that could be included in the analysis.
Eligibility Criteria
Each identified study was reviewed and included if it was a clinical comparative study between revision ACLR surgery by aACLR with LET/ALLR or iACLR. Articles were excluded if they were primary reconstructions, nonhuman studies, purely biomechanical evaluations, case reports, expert opinions, technical tips, and publications pertaining to surgical techniques. All forms of patient-reported outcome measures (PROMs), return to pre-injury level, post-operative rotational stability, failure, and complications were included.
Study Selection and Quality of Studies Assessment
Two authors (K.B. and H.H.C.) independently reviewed the titles and abstracts from the search results. Each author independently reviewed potentially suitable papers, and any discrepancies regarding the eligibility criteria of the papers were resolved by consensus from the senior authors (R.A. and N.S.).
The same 2 authors (K.B. and H.H.C.) assessed the quality of the studies. This was undertaken using the Modified Coleman Methodological Score (MCMS), modified to account for the subject matter 5 (Table 1). The MCMS is based on a scale ranging from 0 to 100, where a score of 85 to 100 is considered excellent, 70 to 84 good, 55 to 69 fair, and <55 poor.
The MCMS Criteria Used for the Quality of Studies Assessment a
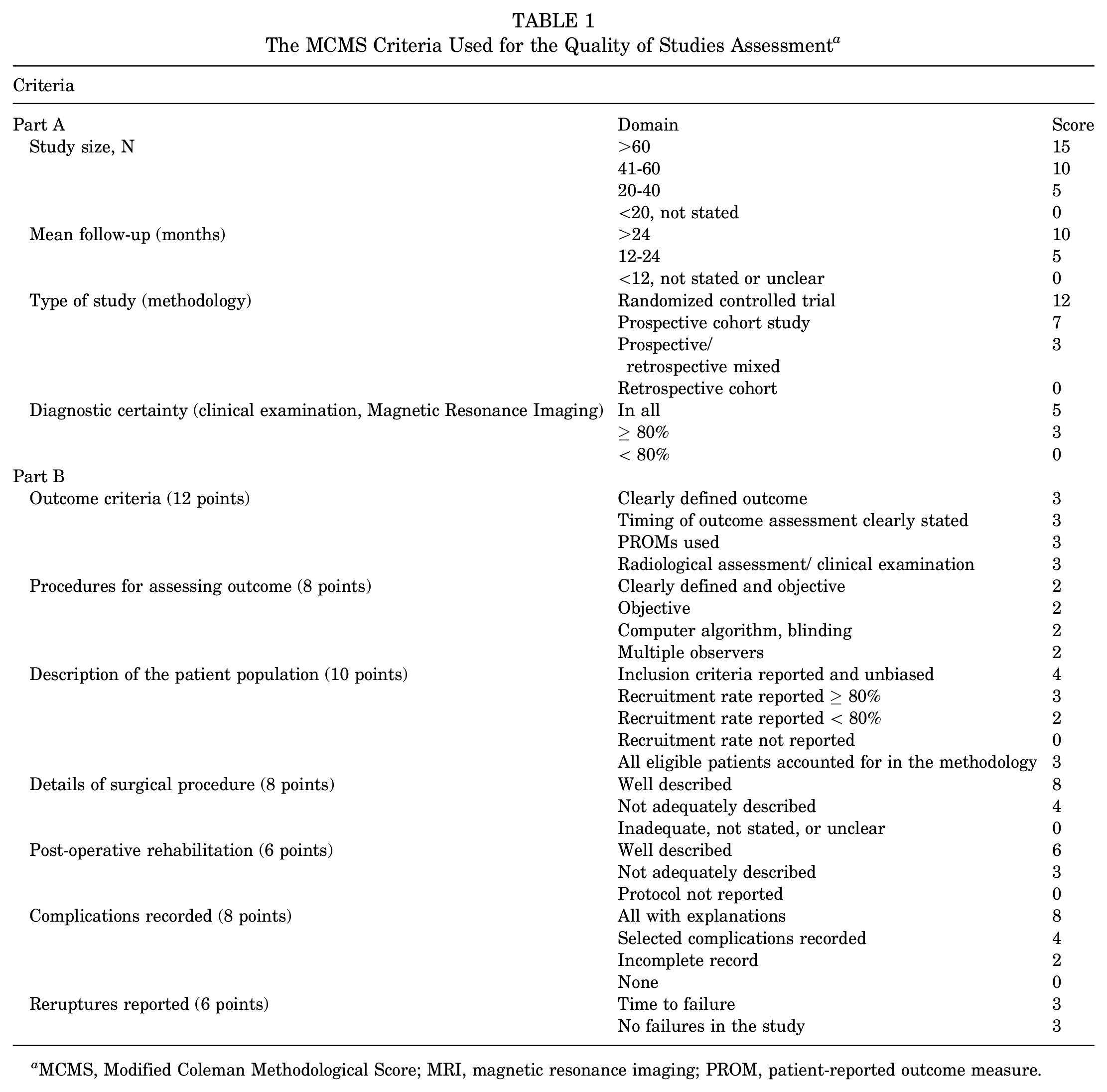
MCMS, Modified Coleman Methodological Score; MRI, magnetic resonance imaging; PROM, patient-reported outcome measure.
The risk of bias in the included studies was assessed and reported in accordance with the Risk of Bias In Non-randomized Studies of Interventions tool. 55 Each item was judged according to high, moderate, low, or unclear risk of bias. Studies were deemed to have the highest risk of bias if they scored a high or unclear risk of bias.
Data Synthesis and Statistical Analysis
Review Manager 5.4 software was used for data synthesis. Odds ratios (ORs) were used for all dichotomous variables and standard mean differences for continuous parameters. Statistical heterogeneity was assessed using the I2 and the chi-square result. A P < .1 and an I2 > 50% were considered suggestive of statistical heterogeneity, prompting a random-effects model. Otherwise, a fixed-effects model was used.
Results
The electronic search yielded 581 studies. After removing 157 duplicates, 424 studies remained, of which 380 were excluded after reviewing the abstracts. An additional 34 studies were excluded based on the aforementioned inclusion and exclusion criteria. This left 10 studies for final qualitative and quantitative analyses (Figure 1). §
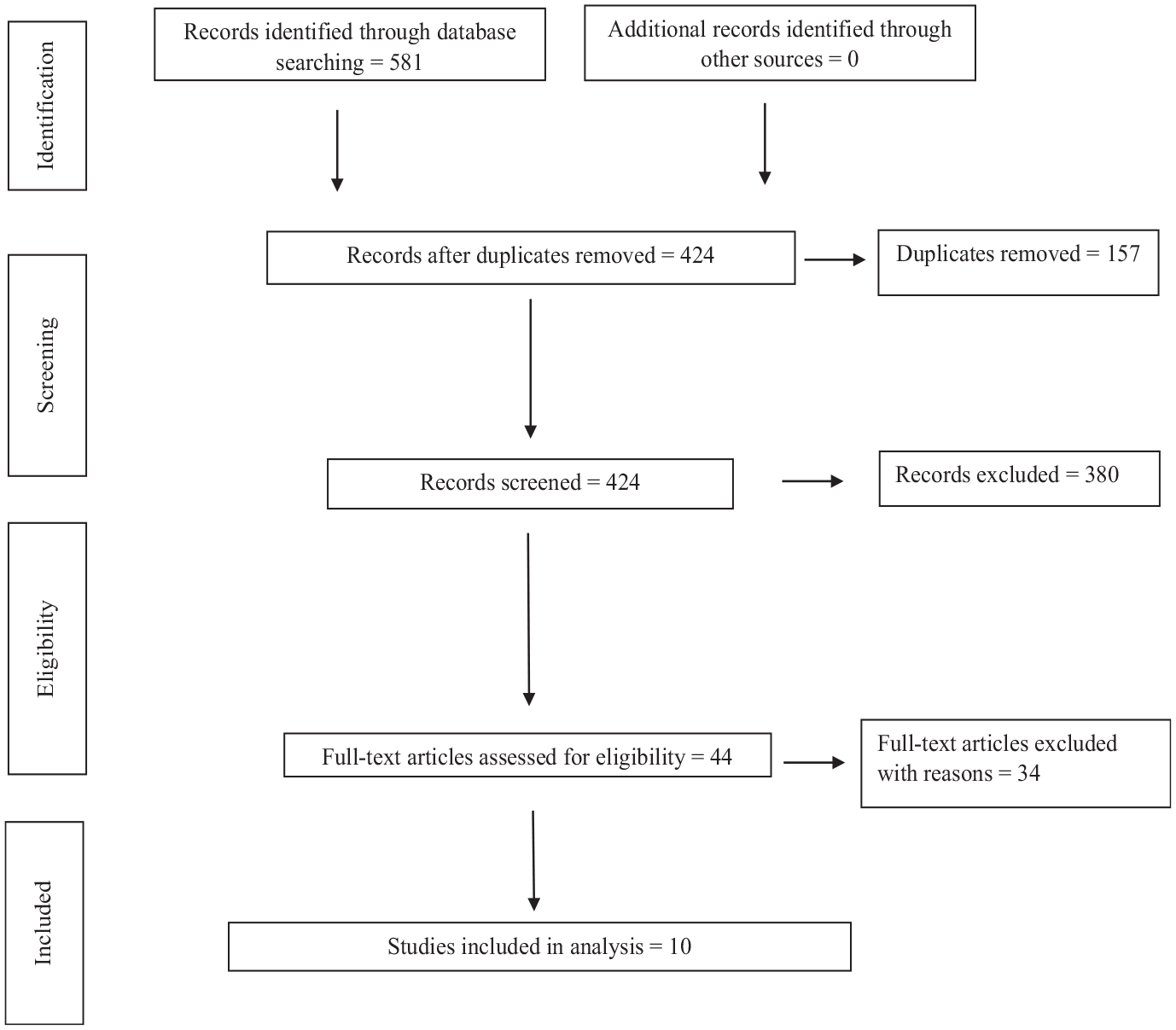
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for study selection.
Methodological Quality of Included Studies
Regarding the MCMS of the 10 included studies, there were a mixture of good-,2,18,27 fair-,9,28,48,56,61 and poor-quality studies.25,58 The overall quality of the studies was fair (mean score, 63.2). The baseline characteristics and surgical techniques of these studies are provided in Tables 2 and 3, respectively.
Baseline Characteristics of the Included Studies a
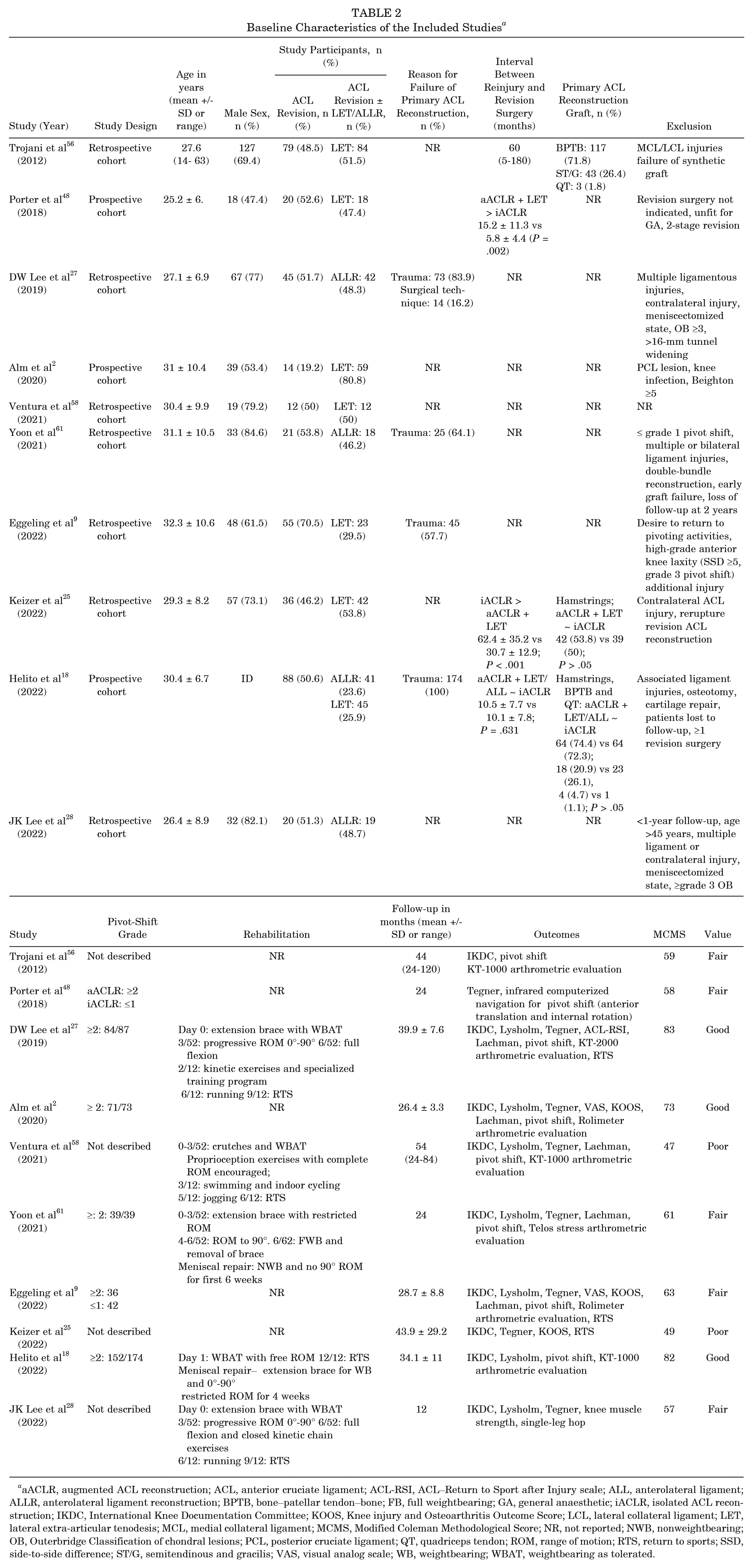
aACLR, augmented ACL reconstruction; ACL, anterior cruciate ligament; ACL-RSI, ACL–Return to Sport after Injury scale; ALL, anterolateral ligament; ALLR, anterolateral ligament reconstruction; BPTB, bone–patellar tendon–bone; FB, full weightbearing; GA, general anaesthetic; iACLR, isolated ACL reconstruction; ID, inadequate description; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LCL, lateral collateral ligament; LET, lateral extra-articular tenodesis; MCL, medial collateral ligament; MCMS, Modified Coleman Methodological Score; NR, not reported; NWB, nonweightbearing; OB, Outerbridge; PCL, posterior cruciate ligament; QT, quadriceps tendon; ROM, range of motion; RTS, return to sports; SSD, side-to-side difference; ST/G, semitendinous and gracilis; VAS, visual analog scale; WB, weightbearing; WBAT, weightbearing as tolerated.
Baseline Characteristics
In total, there were 793 patients, of whom 390 had an iACLR while 403 had an aACLR with either a LET or an ALLR. The mean age and time for assessment of PROMs were 29.2 years and 35 months, respectively. Where described, trauma was the common cause for failure of the primary ACL graft.9,18,27,61 Three studies described the initial primary graft,18,25,56 of which the hamstring autograft was the most common in 2 studies.18,25 Six studies described the extent of knee laxity before revision,2,9,18,27,48,61 with 4 studies primarily investigating higher-grade (≥2) pivot shift.2,18,27,61
Five studies reported on their rehabilitation protocol.18,27,28,58,61 All studies differed from each other in regard to full weightbearing, degree of knee motion, and return to sport (RTS).
To conduct a meta-analysis, we ensured certain outcomes were measured in ≥ 4 studies with precise means and similar metrics.
The most common PROMs measured were the International Knee Documentation Committee (IKDC), Tegner, and Lysholm scores, with ≥7 studies for each. Three studies looked at the Knee injury and Osteoarthritis Outcome Score (KOOS) and RTS at the same level.9,25,27 In regard to postoperative stability, the grade of the pivot shift and the side-to-side difference (SSD) was measured in the majority of studies, with only 5 studies measuring anterior laxity with Lachman.2,9,27,58,61
Description of Surgical Techniques by Author a
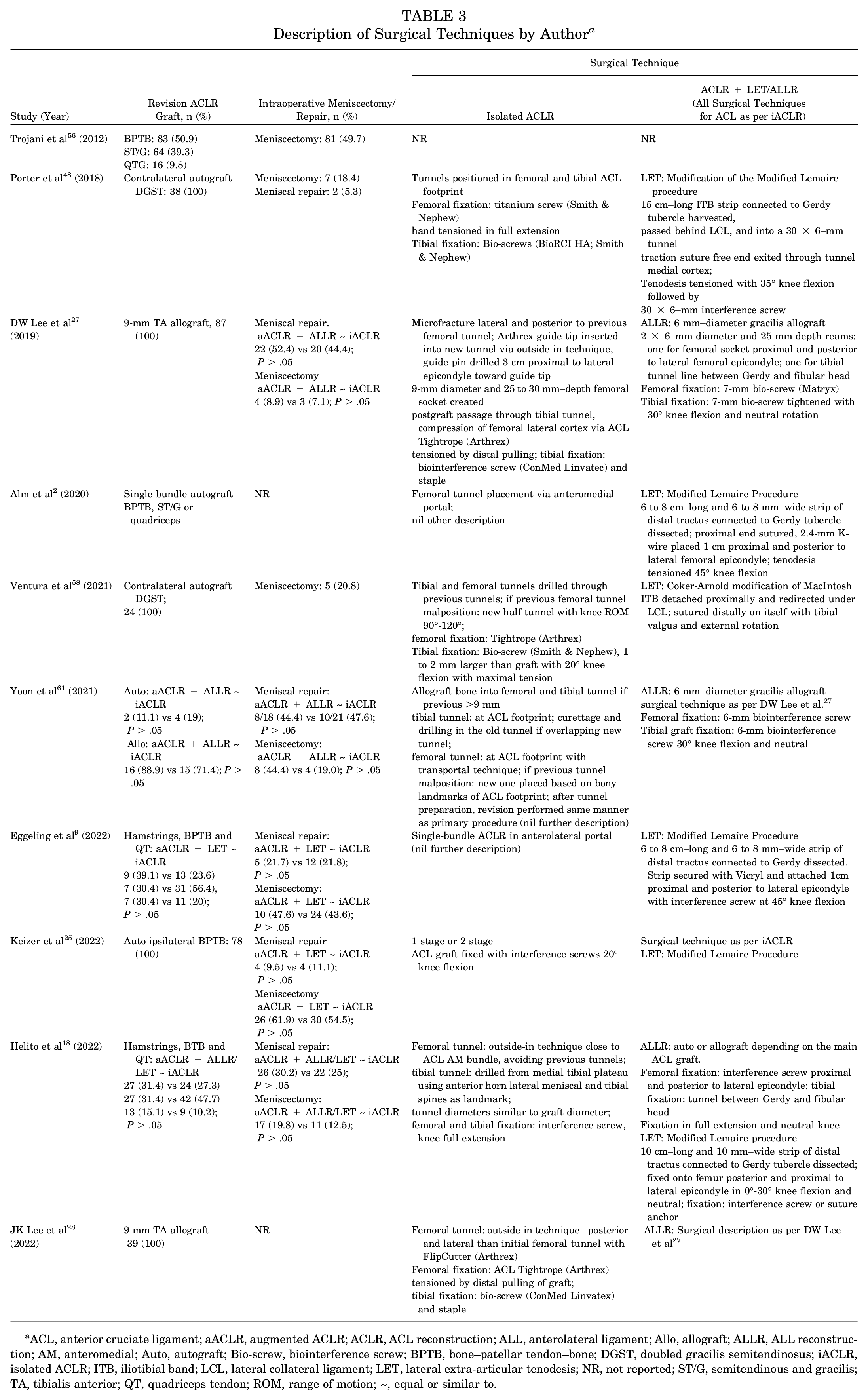
ACL, anterior cruciate ligament; aACLR, augmented ACLR; ACLR, ACL reconstruction; ALL, anterolateral ligament; Allo, allograft; ALLR, ALL reconstruction; AM, anteromedial; Auto, autograft; Bio-screw, biointerference screw; BPTB, bone–patellar tendon–bone; DGST, doubled gracilis semitendinosus; iACLR, isolated ACLR; ITB, iliotibial band; LCL, lateral collateral ligament; LET, lateral extra-articular tenodesis; NR, not reported; ST/G, semitendinous and gracilis; TA, tibialis anterior; QT, quadriceps tendon; ROM, range of motion; ~, equal or similar to.
Surgical Characteristics (Table 3)
Six studies compared iACLR ± LET augmentation,2,9,25,48,56,58 3 ± ALLR,27,28,61 and 1 ± LET or ALLR. 18 In 5 studies, there were different harvesting options,2,9,18,56,61 and in the cases where they were described, they were similarly distributed between groups.9,18,61 Two studies used contralateral hamstring autograft,48,58 1 ipsilateral bone–patellar tendon–bone (BPTB) autograft, 25 and 2 tibialis anterior allograft.27,28
Eight studies described intraoperative meniscal lesions,9,18,25,27,48,56,58,61 but only 5 directly compared this between groups.9,18,25,27,61 The distribution of meniscal repair and meniscectomy were similar. Although there were variations between studies in the techniques for revising the ACL, all studies ensured the ACL construct was stabilized in the same way for the group that also underwent anterolateral complex augmentation.
The modified Lemaire procedure was performed in all but 1 study using LET,2,9,18,25,48 with the remaining study undertaking the Coker-Arnold modification of MacIntosh. 58 ALLR was similarly performed in 3 studies,27,28,61 where the gracilis allograft was fixed into a tibial and femoral socket at 30° of knee flexion and neutral. The remaining study fixed the graft in extension. 18
Study Risk of Bias Assessment
Given the nonrandomized design of all included studies, the risk of selection bias was moderate to high. The risk of all other bias, particularly attrition bias, was generally low. Based on this, we thought the overall risk of bias was moderate to high. The Cochrane risk of bias graph is shown in Figure 2 and the summary in Table 4.
Risk of Bias Summary a
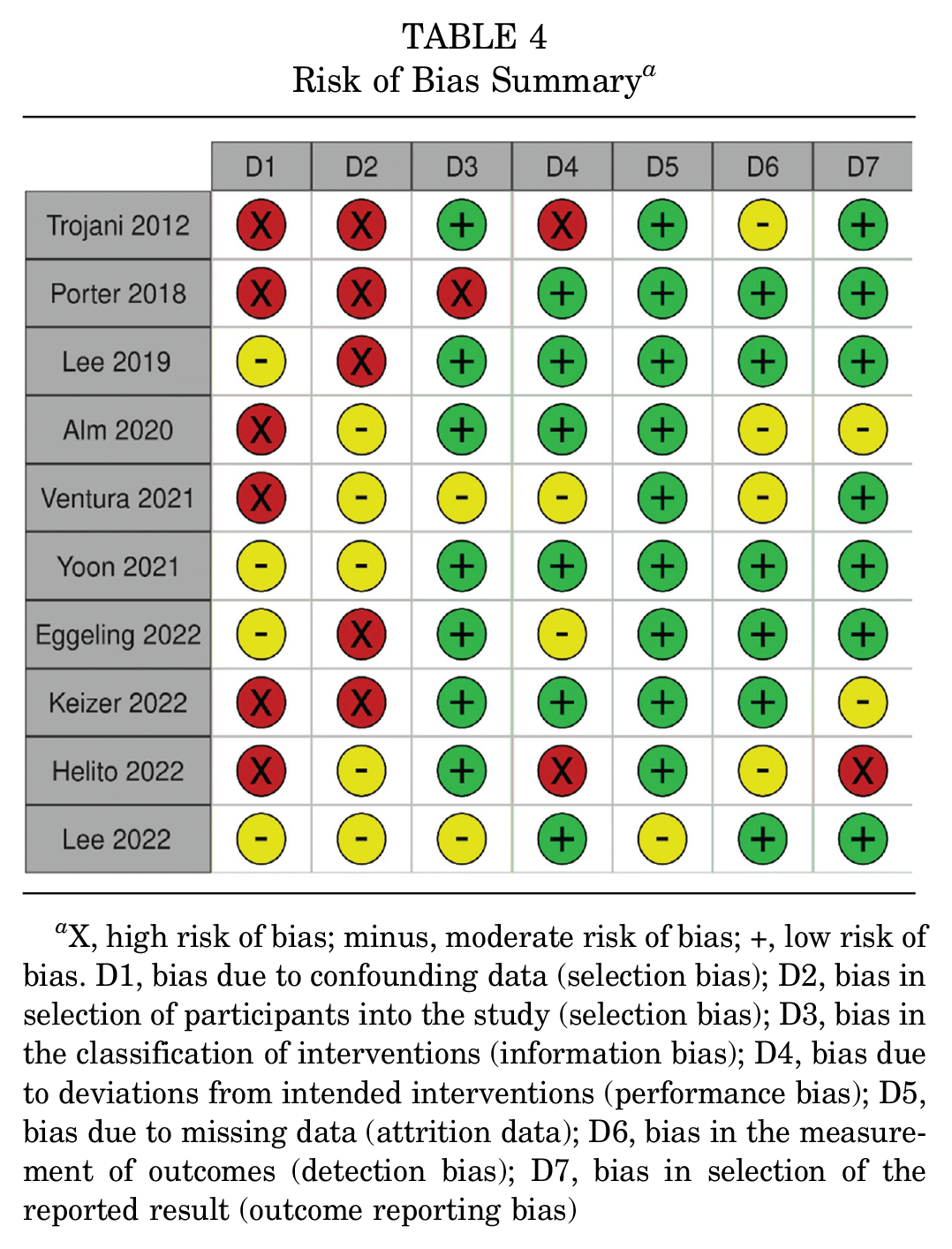
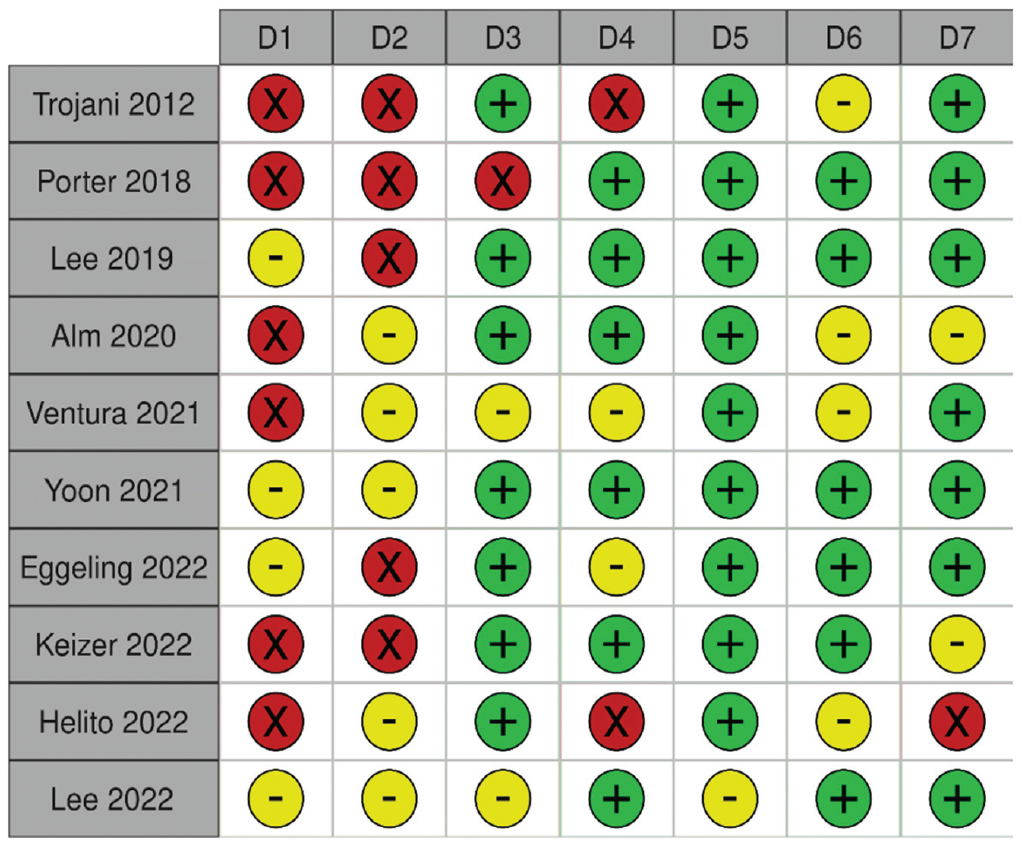
X, high risk of bias; minus, moderate risk of bias; +, low risk of bias. D1, bias due to confounding data (selection bias); D2, bias in selection of participants into the study (selection bias); D3, bias in the classification of interventions (information bias); D4, bias due to deviations from intended interventions (performance bias); D5, bias due to missing data (attrition data); D6, bias in the measurement of outcomes (detection bias); D7, bias in selection of the reported result (outcome reporting bias)
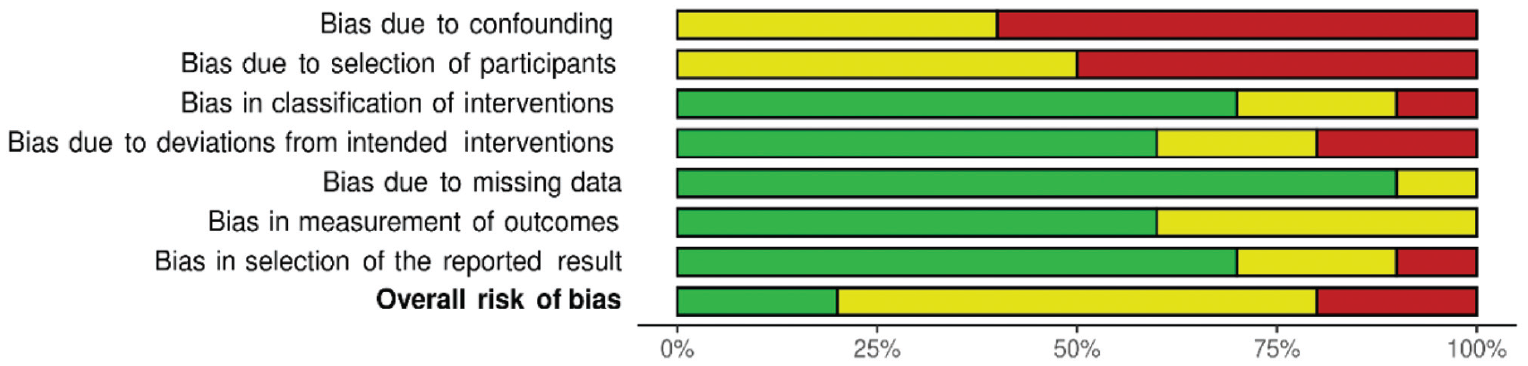
Risk of bias graph.
Clinical Outcomes
A qualitative synthesis of the data is presented in Table 5.
PROMs of Revision of ACLR With and Without Lateral Extra-articular Augmentation a
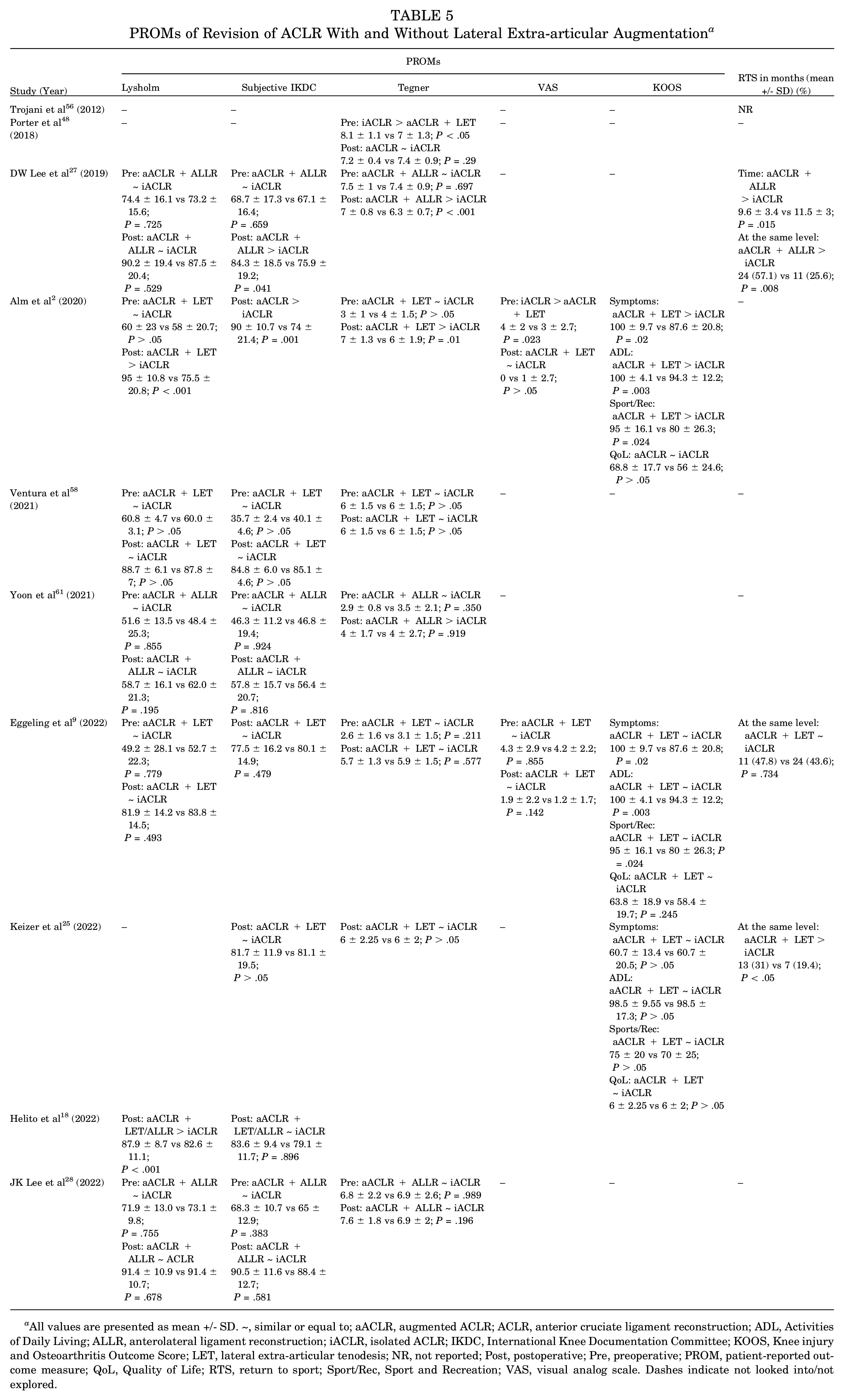
All values are presented as mean +/− SD. ~, similar or equal to; aACLR, augmented ACLR; ACLR, anterior cruciate ligament reconstruction; ADL, Activities of Daily Living; ALLR, anterolateral ligament reconstruction; iACLR, isolated ACLR; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LET, lateral extra-articular tenodesis; NR, not reported; Post, postoperative; Pre, preoperative; PROM, patient-reported outcome measure; QoL, Quality of Life; RTS, return to sport; Sport/Rec, Sport and Recreation; VAS, visual analog scale. Dashes indicate not looked into/not explored.
Lysholm Score
There were no differences between the 2 groups pre- and postoperatively (preoperative standardized mean difference [SMD], 0.03; 95% CI, −0.20 to 0.25; P = .82. postoperative SMD, 0.28; 95% CI, −0.09 to 0.66; P = .14) (Figure 3, A and B).
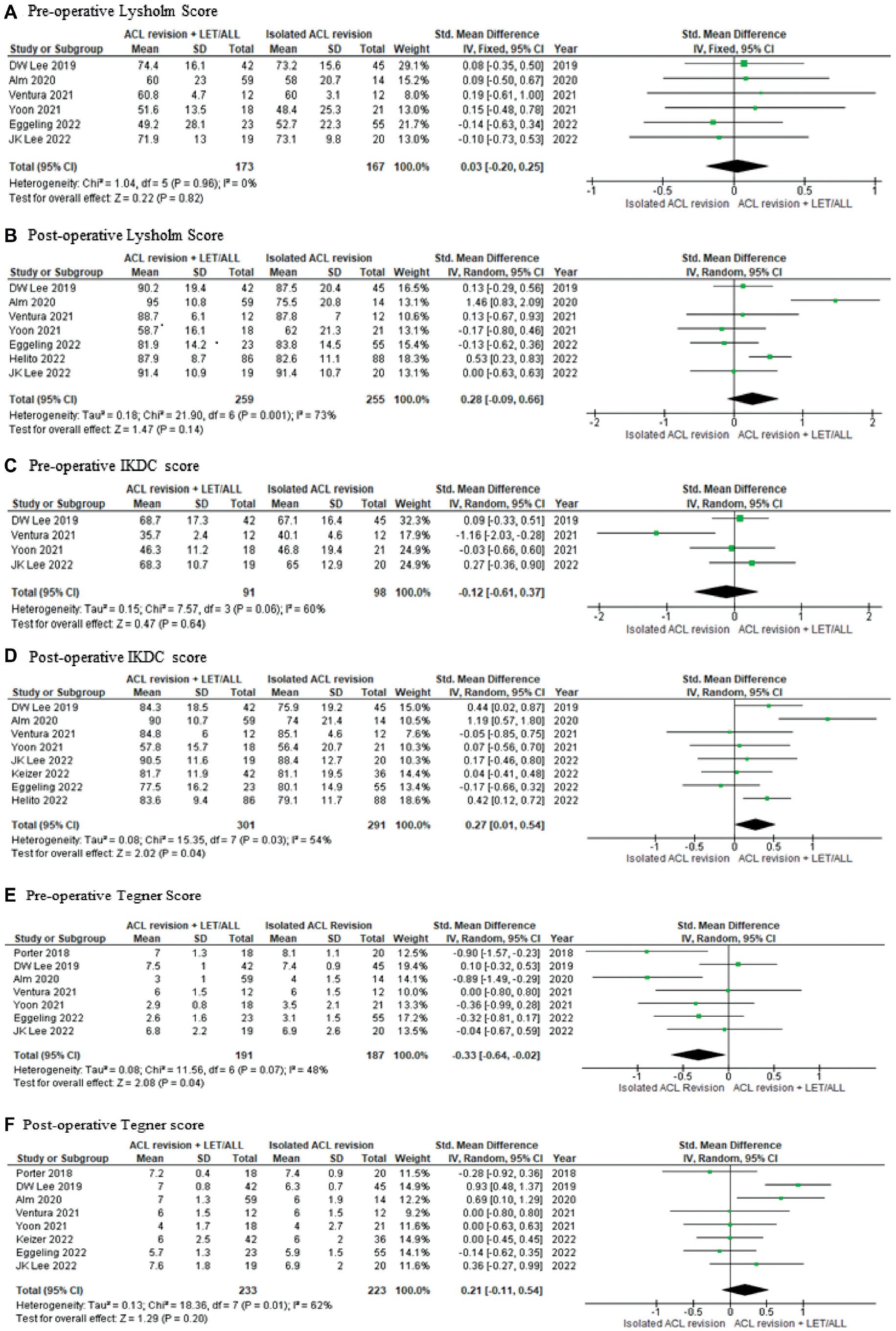
Forest plots of the comparison between groups for Lysholm, IKDC, and Tegner scores. ACL, anterior cruciate ligament; ALL, anterolateral ligament; IKDC, International Knee Documentation Committee; IV, inverse variance; LET, lateral extra-articular tenodesis.
Subjective IKDC Score
Preoperatively, there were no differences between the 2 groups (SMD, −0.12; 95% CI, −0.16 to 0.37; P = .64) (Figure 3C). Postoperatively, those patients who had a LET/ALLR augmentation in addition to the revision of the ACL construct had better IKDC scores than those without the augmentation (SMD, 0.27; 95% CI, 0.01 to 0.54; P = .04) (Figure 3D).
Tegner Score
Preoperatively, those without LET/ALLR augmentation had better Tegner scores (SMD, −0.33; 95% CI, −0.64 to −0.02; P = .04) (Figure 3E). However, the scores were similar between both groups postoperatively (SMD, 0.21; 95% CI, −0.11 to 0.54; P = .20) (Figure 3F).
All Other PROMs
Two of the 3 studies showed significant improvement in KOOS scores,2,9 particularly on Symptoms, Activities of Daily Living, and Sport and Recreation function when there was a LET/ALLR augmentation to the revised ACL construct. The remaining study showed similar scores between the groups. 25
Furthermore, 2 of 3 studies showed that adding a LET/ALLR augmentation led to a significantly higher proportion of athletes returning to the same level of sports compared with those without this added augmentation.25,27 The remaining study showed no difference. 9
Visual analog scale scores were similar between both groups.2,9
Subgroup Analysis: Preoperative High-Grade Knee Laxity
The majority of patients in 4 studies,2,18,27,61 had preoperative high-grade knee laxity ≥2 (100%, 97.3%, 97%, and 87.4%, respectively).
When performing a meta-analysis on these studies, an even greater IKDC score in the ALLR/LET augmentation group was observed (SMD, 0.51; 95% CI, 0.16-0.86; P = .005) (Figure 4A). The Lysholm score was better in this group compared with those without the additional construct (SMD, 0.45; 95% CI, 0.24-0.67; P < .0001) (Figure 4B).
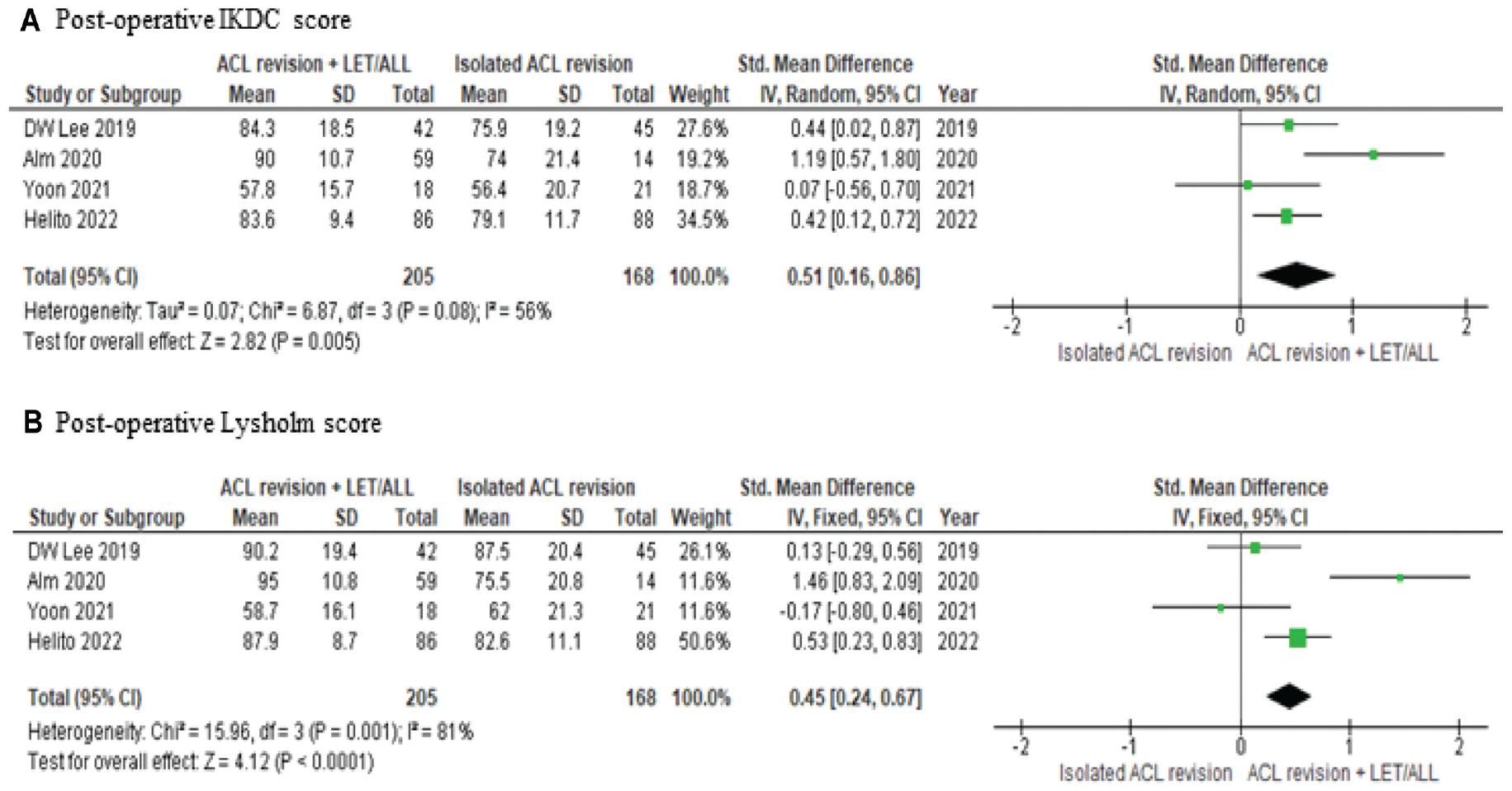
Forest plot of subgroup analysis for preoperative high-grade knee laxity. ACL, anterior cruciate ligament; ALL, anterolateral ligament; IKDC, International Knee Documentation Committee; IV, inverse variance; LET, lateral extra-articular tenodesis.
Postoperative Stability and Failure
A qualitative synthesis of the data is presented in Table 6.
Postoperative Stability, Failure Rates, and Complications Between the 2 Groups a
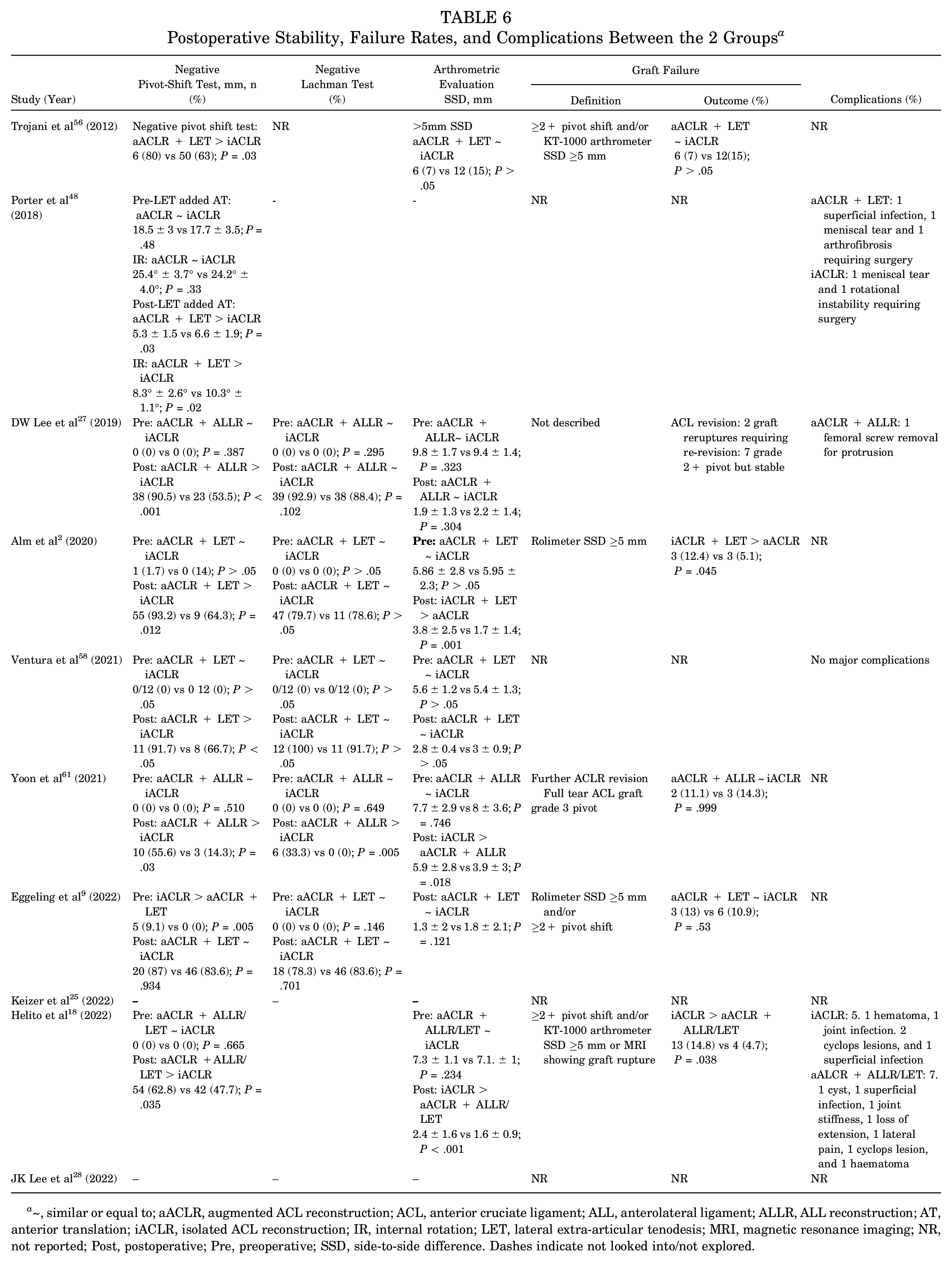
~, similar or equal to; aACLR, augmented ACL reconstruction; ACL, anterior cruciate ligament; ALL, anterolateral ligament; ALLR, ALL reconstruction; AT, anterior translation; iACLR, isolated ACL reconstruction; IR, internal rotation; LET, lateral extra-articular tenodesis; MRI, magnetic resonance imaging; NR, not reported; Post, postoperative; Pre, preoperative; SSD, side-to-side difference. Dashes indicate not looked into/not explored.
There was significant improvement in rotational stability in the aACLR group compared with the iACLR group (OR, 2.77; 95% CI, 1.91 to 4.01; P < .00001) (Figure 5A). Both groups had similar restoration in anterior laxity (OR, 1.61; 95% CI, 0.81 to 3.21; P = .17) (Figure 5B). Preoperatively, there was no difference in the SSD between the 2 groups (OR, 0.15; 95% CI, −0.06 to 0.35; P = .16) (Figure 5C). However, postoperatively, this was significantly elevated in the iACLR group (OR, −0.53; 95% CI, −0.81 to −0.24; P = .0003) (Figure 5D).
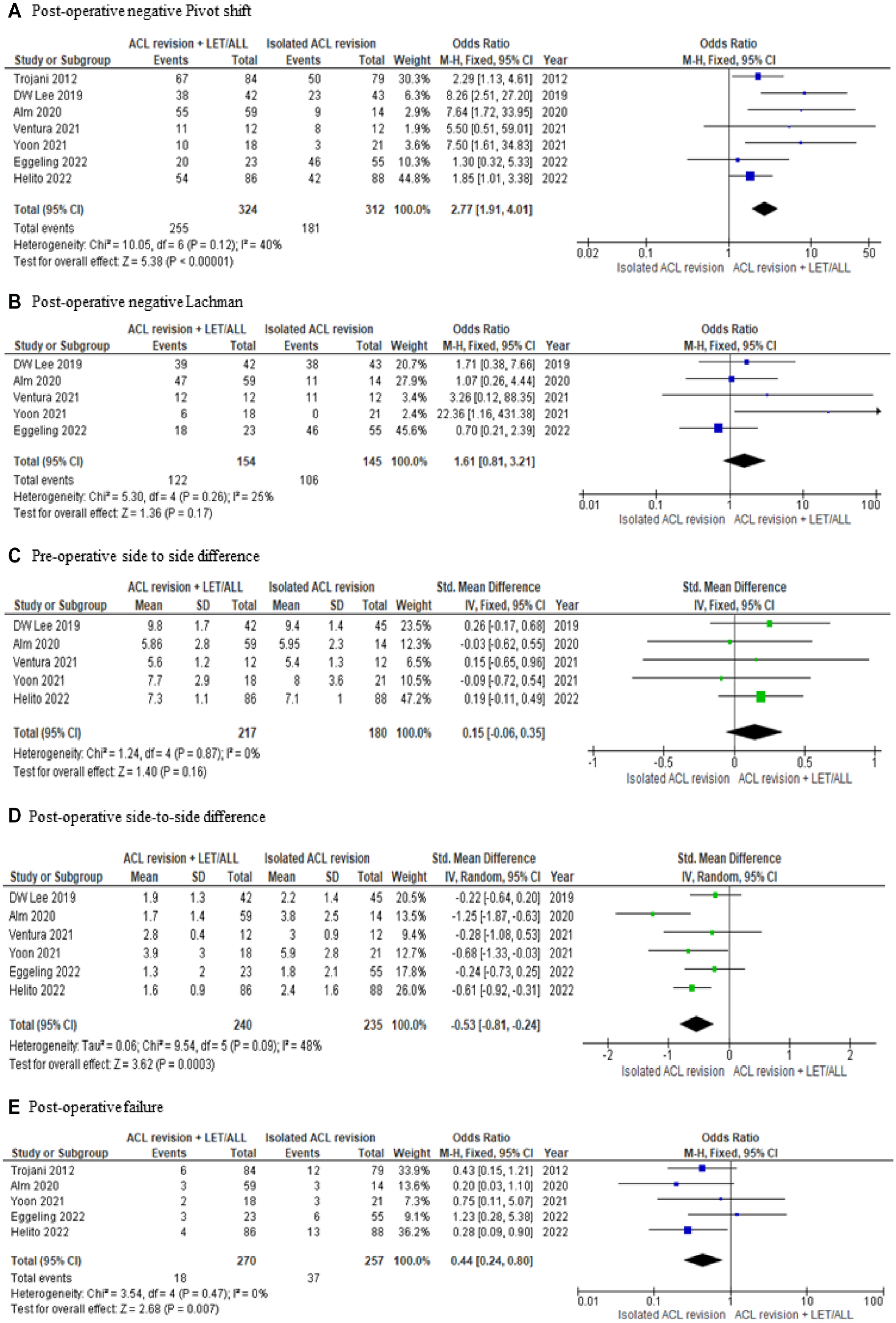
Forest plot of postoperative stability and failure between both groups, along with comparison of preoperative to postoperative side-to-side difference. ACL, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; LET, lateral extra-articular tenodesis; M-H, Mantel-Haenszel.
Five studies defined graft failure after revision.2,9,18,56,61 All but 1 study had similar definitions, 61 which included a grade ≥2+ pivot shift and/or SSD ≥5 mm. Failure was less likely to occur with aACLR (OR, 0.44; 95% CI, 0.24-0.80; P = .007) (Figure 5e).
Complications
Four studies reported complications,18,27,48,58 although only 3 provided adequate descriptions.18,27,48 There were very few complications, with hematoma formation, cyclops lesion, and superficial infection being the most common.
Discussion
Revision of an ACLR with an extra-articular augmentation leads to better subjective postoperative IKDC scores, a lower incidence of rotational laxity, greater stability in the SSD in stress radiographs, and a lower failure rate compared with those without an augmentation.
Although the Lysholm and Tegner scores were similar, the importance of the favorable subjective IKDC scores in the augmented group should not be underestimated. It is a point-based calculation system, which minimizes confounding patient factors such as age or sex, as it takes various knee-related problems into account.34,45,49 This is in contrast to the Lysholm score, with concerns of its greater ceiling effects that need to be addressed when assessing the knee function postoperatively. 49
One explanation regarding the insignificant Tegner scores is that the preoperative activity scores were higher in the group without augmentation. This would favor this cohort rather than the LET/ALLR group in regard to final scores, which were similar in both groups.
A correlation between cartilage damage and meniscal injuries and the clinical outcomes of revision surgery has previously been demonstrated.11,23,43 However, this is unlikely to have contributed to the lower IKDC scores in the iACLR group, as such pathology and its treatment, where described, were equally distributed among both cohorts.
Revision ACL is often not expected to yield the same results as primary ACLR and should be considered a salvage procedure with limited goals, such as restoring stability to allow work, activities of daily living, and light recreational sports. 15 As several reports have shown its inferior functional outcomes compared with primary surgery, closer attention should be paid to the cause of failure and the presenting symptoms.1,16 Based on extensive research, the primary reason for ACLR revision is an unrecognized anterolateral complex injury.39,51 This can cause persistent rotational instability, 3 and the pivot shift is the most clinically useful test in detecting such pathology. 38 The significantly lower incidence of rotational laxity and side-to-side difference in this meta-analysis after augmentation of the ACLR, with either LET or ALLR, supports the role of the anterolateral complex as an important stabilizer of the knee. In addition, there is the added benefit of protecting the ACL graft from excessive stresses, particularly in the early postoperative period. 28
The augmented ACLR could explain the lower incidence of graft failure, as the shared distribution of load minimizes micromovement of the graft in the tunnel, enabling a successful bone-tendon healing interface, and a satisfactory RTS.53,54,60 The latter is qualitatively supported by 2 of the 3 included studies reporting RTS25,27, both of which had a larger LET/ALLR cohort, and showed a higher incidence of returning to the same level of sporting activity in the augmentation group. Despite no differences in the remaining study, the authors did show that lateral extra-articular augmentation led to a more functional knee when performing sports in the KOOS questionnaire. 9
There are concerns that the extra-articular procedure may result in the overconstraint of the knee with potential adverse effects, including lateral knee pain and reduced range of motion.10,20,35 The challenge for the orthopaedic surgeon, therefore, is how to select those patients undergoing revision ACLR who would benefit from the addition of an anterolateral procedure. One potential subgroup of patients is those who present with a persistent pivot shift, particularly a high-grade (≥2) laxity, in the revision setting. 8 Subgroup analysis of the studies reporting high-grade pivot shift revealed an even greater postoperative IKDC score in the augmentation group as well as a significantly improved Lysholm score.2,18,27,61 This suggests that the extent of preoperative anterior knee laxity may be an important, previously underestimated risk factor for revision ACLR failure. Additionally, a low-grade pivot shift (<2) could indicate intact anterolateral structures, thus rendering the additional ALLR/LET procedure ineffective, 9 and unnecessarily overconstraining an already well-preserved anterolateral side of the knee. Due to the inclusion of patients with lower-grade pivot shift preoperatively, the beneficial effects of the extra-articular augmentation may have been underestimated and may provide an alternative explanation for the similar results in most of the PROMs when all studies were analyzed. 9
Graft choice may have potentially confounded the results of the present study. However, of the 5 studies in which different graft types were used, 4 showed no differences between the groups,9,18,56,61 thereby enabling comparability. Data were lacking in the final study, 2 but the remaining 5 studies used the same graft construct for all patients. A recent meta-analysis has shown no difference between BPTB and hamstring grafts for ACL revision, although hamstring grafts are the preferred option because of lower donor-site morbidity. 52 In the revision setting, graft standardization is generally not feasible. This is due to the multifactorial nature of revision ACLR surgery taking into account the previous harvested grafts, the type of primary reconstruction used, the size and position of existing tunnels, tunnel widening, and multiple patient factors. The strength of this study includes being the first systematic review to specifically compare the clinical outcomes of revision surgery of the ACL with or without an extra-articular augmentation.
There are some limitations in this study. First, selection bias due to the retrospective, nonrandomized design of the majority of studies may have influenced the results. To date, no prospective randomized study has been performed addressing this question. Only 1 study 56 evaluated degenerative changes with radiographic follow-up. The mean follow-up of 35 months is not long enough to comment on any association with osteoarthritis or the concern that anterolateral augmentation may lead to over constraint and degenerative changes. The wide age range included in the studies may influence the correlation between the study findings and all population groups, including the pediatric and adolescent cohorts. Only 1 study used equipment to enable objective measurement of the pivot shift. 48 The fixation angle and tension of the augmented graft should be adapted according to the amount of rotatory laxity and the type of augmentation procedure performed. 22 This will provide better accuracy in the ability to correct the residual pivot shift and restore function to normal without overconstraining the knee. We recommend the use of equipment that can objectively assess pivot shift in future research on this topic.
Although there were differences in rehabilitation between studies, all studies included a postoperative regimen that was identical between both constructs, limiting its potential as a confounder.
Many factors need to be considered before revision. This includes preoperative factors such as radiographic evaluation, bone tunnel defects, previous femoral tunnel malposition, and graft diameter. Potentially important intraoperative findings and patient-related factors that could affect the outcomes of surgery were compared, although they were not consistent throughout the studies. In the majority of studies, there was no significant difference between the 2 cohorts, enabling comparability between the groups. One potential confounder was the graft positioning during the revision ACLR, particularly if placed in a nonanatomic position. Three studies positioned the graft anatomically,48,58,61 three nonanatomic,18,27,28 and the rest did not provide sufficient details.2,9,25,56 Despite few complications, graft positioning was unreported in 6 studies.2,9,14,56,58,61 It is important for future research to delve further into this to ensure that morbidity postaugmentation is kept minimal.
Conclusion
Despite the limitations, this meta-analysis provides useful information for clinicians. Lateral extra-articular augmentation to a revision ACLR improved subjective IKDC scores, rotational stability, and reduced failure rates compared with isolated ACLR revision. Although there remains controversy on the necessity of augmenting all revision ACLRs, the present meta-analysis advocates adding a lateral extra-articular procedure in those with a higher-grade pivot shift.
Footnotes
Submitted August 22, 2022; accepted December 3, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.