
Abstract
Background:
Postoperative laxity correlates with negative clinical outcomes after anterior cruciate ligament reconstruction (ACLR). The influence of lateral extra-articular tenodesis (LET) on anteroposterior translation is unclear.
Purpose/Hypothesis:
This study aimed to evaluate the reduction in radiographic static anterior tibial translation (SATT) and dynamic anterior tibial translation (DATT) after LET as an adjunctive procedure to ACLR. It was hypothesized that adding a LET procedure would have no effect on postoperative SATT and DATT.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent primary ACLR with hamstring tendon autografts between 2020 and 2022 were reviewed, and those who underwent ACLR and LET as an anterolateral associate procedure were paired 1 to 1 with those who underwent isolated ACLR (control) based on age, sex, preoperative SATT, and posterior tibial slope (PTS). The indications for LET were age <18 years and anterolateral rotary instability (grade ≥2 pivot shift). A previously validated technique was used to measure SATT, DATT, and PTS on lateral weightbearing and lateral stress knee radiographs. Preoperative and 9-month postoperative radiographs were compared between the 2 groups.
Results:
A total of 72 patients were included in the analysis (n = 36 patients in each group). The inter- and intraobserver reliability of the SATT, DATT, and PTS measurements was excellent (intraclass correlation coefficients, 0.88-0.99). The mean pre- and postoperative SATT in the ACLR+LET group was 2.44 ± 2.90 mm and 2.44 ± 2.38 mm, respectively, compared with 2.60 ± 2.99 mm and 2.12 ± 2.74 mm, respectively, in the control group. The mean pre- and postoperative reduction in side-to-side DATT in the ACLR+LET group was 5.44 ± 4.65 mm and 1.13 ± 2.95 mm, respectively, compared with 5.03 ± 3.66 mm and 2 ± 3.12 mm, respectively, in the control group. There was no pre- to postoperative difference in SATT (P = .51). However, the side-to-side DATT was reduced by 3.66 ± 3.37 mm postoperatively (P < .001), without significant differences between groups (P = .24).
Conclusion:
Including a LET procedure for patients undergoing ACLR did not reduce SATT; that is, it did not decrease the amount of tibial translation due to physiological axial load.
Keywords
Anterior cruciate ligament (ACL) tear is one of the most common injuries in young pivoting sports athletes, often resulting in ACL reconstruction (ACLR). Despite a high rate of good functional outcomes and return to sports (RTS), 26 the literature reports a rerupture rate of up to 17%; thus, there is a need to improve outcomes.5,43
Increased postoperative laxity results in negative clinical outcomes, including reduced psychological readiness for RTS, higher graft failure rates, diminished patient-reported outcomes, and an increased risk of long-term osteoarthritis.16,17,30,50,51 Therefore, quantifying laxity after ACLR is important in clinical practice.
ACLR aims to address anterior tibial translation and control rotational instability. Laxity in ACL surgery can be assessed by the response to translational force, axial load, and excessive internal rotation. Translational forces are clinically assessed with Lachman and anterior drawer tests and can be measured via a KT-1000 arthrometer and Telos stress radiography.28,36,48,52 Internal rotation is best evaluated via the pivot-shift test; nonetheless, it is not easy to objectively quantify.1,31-33,36,37,38,50,52 Static anterior tibial translation (SATT) is a radiographic measure of the amount of tibial translation in response to the physiological axial load during a single-leg stance, which is affected by a combination of muscle activation, bone morphology, and ACL status. 34 The relationship between slope and anterior translation has been confirmed in biomechanical studies on gait analysis, 2 which have demonstrated a direct effect of increased anterior tibial translation and resultant increased ACL force associated with the increasing posterior tibial slope (PTS). This is most pronounced during midstance. This supports the clinical validity of SATT as an in vivo measure of ACLR graft stress.29,31,45,46 Dynamic anterior tibial translation (DATT) is a radiographic measure of the amount of tibial translation in response to applied femoral (posterior) and tibial (anterior) loads to stress the ACL/graft. Compared with SATT, which represents translation in the axially loaded state, DATT represents soft tissue constraint in the axially unloaded state.
The addition of an anterior lateral ligament reconstruction 49 or lateral extra-articular tenodesis (LET) 21 has been proposed to reduce ACLR failure in high-risk patients. This has led to a push to use it alongside all ACLR procedures by some surgeons, with a number needed to treat of 14 to prevent 1 rerupture. 21 Biomechanical and clinical data indicate that LET reduces the pivot-shift phenomenon by reducing the amount of internal rotation. A recent systematic review reported a significant reduction in the prevalence of residual pivot shift using LET associated with ACLR, without significant differences in the RTS rate or patient-reported outcomes. 27 This results in less rotation of the knee, assessed via decreased anterior tibial translation in the lateral compartment, reducing ACLR graft stress with pivoting maneuvers. 11 Another systematic review suggested that in primary ACLR, there is no benefit in lowering anterior laxity in the medial compartment according to radiographic stress testing or KT-1000/2000 arthrometer testing. 15 These studies suggest that LET works not via decreased anteroposterior laxity but via decreasing the rotational component of the laxity. The response to axial load has not been assessed.
The amount of anterior tibial translation under axial load can be radiographically quantified with single-leg stance radiographs using the SATT method. 13 Increased PTS has been correlated with increased SATT. Furthermore, increased preoperative SATT has recently been associated with increased graft failure risk. 38 The effect of an extra-articular procedure on SATT has not been measured. Despite the addition of a LET, the Stability Study showed that the relative risk of graft failure remained elevated in patients with increased PTS. However, the authors advocated for a LET in patients with high PTS. 18 Given that the tibial slope mainly affects (increases) anterior tibial translation with an axial load but the LET procedure works via rotational control, the influence of the LET on SATT needs to be evaluated.
The primary objective of our study was to evaluate whether there was an effect (reduction) of the radiographic SATT with the addition of a lateral extra-articular adjuvant procedure in patients with ACLR. The secondary objective was to evaluate the radiographic DATT in the same cohort. We hypothesized that adding a LET procedure would have no effect on postoperative SATT or DATT.
Methods
Study Design
The protocol for this study received ethics committee approval, and all included patients provided informed consent for the use of their data for research. A retrospective consecutive series of patients who underwent ACLR using hamstring tendon autografts and LET (modified Lemaire) between 2020 and 2022 was paired 1 to 1 to a cohort of patients who underwent ACLR using isolated hamstring tendon autografts from the same period based on age, sex, preoperative SATT, and PTS to act as a control group. The indications for LET during this period were as follows: patients <18 years old, anterolateral rotary instability defined as a grade ≥2 pivot shift, and a recurvatum of >10°.
The study inclusion criteria were the availability of pre- and postoperative lateral knee monopodal weightbearing radiographs and Telos stress radiographs. The exclusion criteria were age <15 years, grafts other than hamstring tendon autografts, associated meniscal injury, associated bony procedures, multiligamentous injuries, and revision cases. Patients with radiographs from another institution or without adequate lateral knee radiographs were excluded from this study. An adequate radiograph was defined as posterior femoral condyles superimposition, knee flexion between 15° and 30°, and a minimum of 15 cm of proximal tibia visible. 14
All ACLR procedures were performed by a single senior surgeon (D.H.D.) using an outside-in technique with femoral and tibial bioabsorbable interference screw fixation (Ligafix; SBM). LET was used as an anterolateral associate procedure in the study group. The modified Lemaire procedure involves harvesting a strip of the posterior part of the iliotibial band (1 cm wide and 9 cm long), maintaining the distal attachment at the Gerdy tubercle.12,39 After ACL fixation, the iliotibial band graft was passed under the lateral collateral ligament and fixed with an interference screw (Ligafix) in a tunnel placed proximal and posterior to the femoral LCL insertion at 80° of knee flexion and neutral rotation.
Postoperatively, all patients participated in the same rehabilitation program regardless of the surgical technique. The rehabilitation protocol consisted of partial to full weightbearing with crutches and physical therapy starting on the day of surgery. Noncontact pivoting activities were allowed at 6 months, and the patients were able to return to full sports activities if isokinetic testing demonstrated a <10% difference in the quadriceps/hamstrings ratio between the operated and contralateral leg at 9 months.
Images and Measurements
Lateral monopodal weightbearing knee radiographs were performed at 20° of knee flexion. Telos stress radiographs were performed with a 150-N anteriorly directed force to the posterior tibia. Preoperative radiographs were performed 1 week before surgery. All patients in our institution have preoperative physical therapy to ensure a nonpainful knee with a full range of motion and good quadriceps and hamstring activation before surgery. Postoperative images were taken at the 9-month follow-up.
All measurements were performed on deidentified radiographs by 2 independent examiners (N.C. and T.P.) using Horos DICOM viewer software Version 3.3.6 (Horos Project). Each reviewer performed all the measurements twice to calculate inter- and intraobserver reliability.
The PTS was measured by calculating the angle between a line perpendicular to the tibial diaphysis and the medial tibial plateau (Figure 1).4,7,8,13 The anterior tibial translation distance was defined as the distance between 2 lines parallel to the posterior tibial cortex—the first line tangent to the posterior aspect of the medial tibial plateau and the second line tangent to the posterior femoral condyles (Figure 2).7,8,13

A lateral right knee radiograph demonstrating measurement of the PTS on a monopodal weightbearing radiograph. The PTS is the angle a, formed between line B, perpendicular to the tibial diaphyseal axis (line A), and line C, tangent to the most superior points at the anterior and posterior edges of the medial plateau. PTS, posterior tibial slope. Line A is defined by the line passing through the center of the two circles. The circles are placed 5 and 15cm from the joint surface.

(A) A lateral left knee radiograph demonstrating SATT measurement on a monopodal weightbearing radiograph. The posterior tibial cortex is the reference (line A). Two lines are traced parallel to line A and tangent to the posterior part of the medial plateau (line B) and the medial femoral condyle (line C). The SATT is the distance between lines B and C. (B) A lateral knee radiograph demonstrating measurement of DATT on Telos stress radiograph using 150 N of force applied on the femur (arrow 1) and the tibia (arrow 2) in opposite directions. The posterior tibial cortex is the reference (line a). Two lines are traced parallel to line a and tangent to the posterior part of the medial plateau (line b) and the medial femoral condyle (line c). The DATT is the distance between lines b and c. DATT, dynamic anterior tibial translation; SATT, static anterior tibial translation.
Statistical Analysis
The inter- and intraobserver reliability of the radiographic measurements was calculated using the intraclass correlation coefficient (ICC). Regarding the patient and radiographic data, continuous variables were reported as means ± standard deviation where appropriate, while dichotomous variables were reported as the number and percentage of patients. The Shapiro-Wilk normality test was used to assess the normality of distributions. A paired-samples Student t test was performed to determine the difference between SATT on pre- versus postoperative Telos stress radiographs in the isolated ACLR and ACLR+LET cohorts. A 2-tailed Student t test for independent samples was used to compare the SATT values between the 2 cohorts. The difference (Δ) in DATT values between the operated and contralateral knee (side-to-side DATT) was compared at both the pre- and postoperative time points between the cohorts. Finally, the pre- to postoperative SATT and side-to-side DATT differences were compared between cohorts. SPSS Version 25 (IBM) was used to perform all statistical analyses. Statistical significance was set at P < .05.
A post hoc power analysis was performed. With a total sample size of 72 participants (n = 36 in each group), the study was 80% powered to detect a mean difference of 1.8 mm in SATT, a significant difference between the groups with a 95% confidence level, given the standard deviations for SATT difference in our groups.
Results
There was excellent inter- and intraobserver reliability for the SATT, DATT, and PTS measurements (ICCs, 0.88-0.99). A total of 72 patients were included in the statistical analysis, with 36 patients in each group. Table 1 reports the patient characteristics and radiographic data. As expected by the indications for LET, a statistically significant difference was found in the incidence of high-grade pivot shift (defined as grade ≥2) in the ACLR+LET group compared with the isolated ACLR group (91% vs 0%, respectively). Otherwise, no group differences were identified with regard to side, sex, age, tibial slope, or graft diameter.
Demographic and Radiographic Data by Study Group a
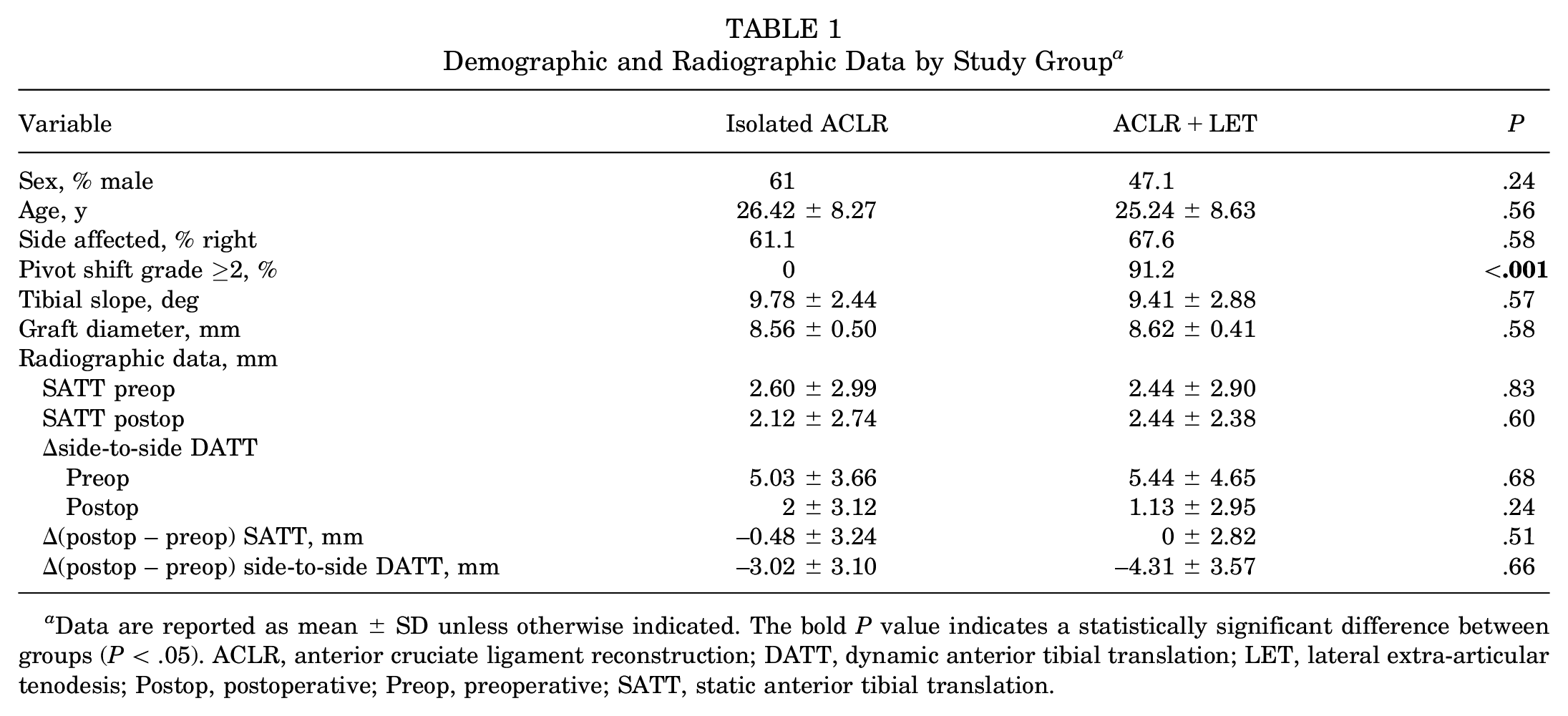
Data are reported as mean ± SD unless otherwise indicated. The bold P value indicates a statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; DATT, dynamic anterior tibial translation; LET, lateral extra-articular tenodesis; Postop, postoperative; Preop, preoperative; SATT, static anterior tibial translation.
In both groups, there was a significant pre- to postoperative reduction in side-to-side DATT (isolated ACLR: from 5.03 to 2 mm; ACLR+LET: from 5.44 to 1.13 mm; P < .001 for both), without any significant differences between the groups (P = .24). However, no significant changes in pre- to postoperative SATT were observed in either group (isolated ACLR: from 2.60 to 2.12 mm; ACLR+LET: from 2.44 to 2.44 mm; P = .51).
Although this was a radiographic rather than a clinical study, some clinical outcomes were noted. First, no complications were recorded in either group. Second, all patients had a grade 0 pivot shift, and no graft failures were reported at the final follow-up. Third, all patients returned to sports according to the rehabilitation protocol, allowing for a return to contact-pivoting sports after 9 months of rehabilitation .
Discussion
The most important finding of the present study was the absence of an effect of a concomitant LET procedure on both SATT and DATT reduction in patients with ACLR.
The anterior translation of the tibia plays an important role in the clinical assessment of knee stability, specifically in the context of postoperative outcomes. Increased anterior knee laxity has been identified as a parameter to define clinical failure after ACLR.16,30,51 In a systematic review, Grassi et al 23 found a clinical failure rate of up to 32% after ACLR when considering clinical anterior tibial translation. Moreover, increased manual knee laxity 2 years after ACLR has been associated with poorer clinical outcomes. 51 These findings highlight the importance of accurately assessing and addressing anterior knee laxity for optimizing patient outcomes.
Chronic anterior laxity has been considered a potential risk factor for ACLR failure 38 and an indication for primary lateral extra-articular procedures.20,37,38 Although a specific threshold has not been defined in the literature, Ni et al 38 suggested in a 2020 study that an SATT of >6 mm significantly increases the rate of graft rerupture, thus emphasizing the importance of interventions aimed at restoring normal SATT values.
Biomechanical studies have shown that an isolated LET procedure does not return normal anterior stability to the ACL-deficient knee. 47 However, in association with ACLR, LET procedures can significantly reduce anterior tibial translation and the forces on an intra-articular graft when applying an anteriorly directed force. However, these assessments were performed in the axially unloaded limb; therefore, these studies are not representative of the amount of anterior translation in response to an axial load, as can be measured by SATT.19,50
Both LET and tibial deflection osteotomy (TDO) have been proven to reduce ACLR graft strain and failure rates by different mechanisms.10,21,25,41 The LET procedure has been proven to reduce graft forces by controlling anterolateral rotatory instability.24,35,47 The PTS was found to have a linear relationship with the tensile force on the ACL in a biomechanical study, 2 and an increased PTS has been associated with a higher pivot shift. 3 An increased PTS increases anterior translation under axial load in gait analysis,43-45 which is reflected radiographically with increased SATT with increased PTS. 13 By decreasing the slope, TDO can decrease graft tension, recenter the tibia under the femur, and decrease SATT.10,41 It can also increase the effect on axial load2,22,44 and decrease the rotational instability by decreasing the PTS. The correction of the tibial slope appears to have a global effect on knee laxity, both anteroposterior and rotational.
SATT is a radiographic measure of the amount of tibial translation in response to a physiological axial load during a single-leg stance, which is affected by a combination of muscle activation, bone morphology, and ACL status. Previous studies have demonstrated that it is influenced by ACL status, chronicity of rupture, and meniscal pathology and it is linearly correlated with increased tibial slope.8,9 ACLR has not been shown to improve SATT 9 ; if SATT is increased without elevated tibial slope in the primary setting, this should elevate the surgeon's suspicion for identifying and addressing meniscal pathology. 8 In revision ACLR with a high tibial slope, TDO can reduce the SATT. The SATT was reduced from 8.5 to 3.6 mm in the setting of primary and secondary revision ACLR when combined with a TDO 53 and from 11.7 ± 5.2 mm to 4.3 ± 2.5 mm in secondary revision ACLR when combined with a TDO, 10 and a small number of cases demonstrated increased tibial slope and SATT in the primary TDO and ACLR setting. 6 The present study reports an important negative finding—LET did not influence SATT.
Our study provides evidence to support that the protective effect of LET is not due to anterior tibial translation reduction under axial load, restricting its role in rotational stability control.24,35,47 This is contrary to the TDO technique, which has proven to reduce anterior tibial translation,21,54 in line with what was previously published in retrospective clinical studies, where combining ACLR with TDO in ACL revision cases with increased PTS demonstrated excellent functional results, with negative Lachman and pivot-shift tests at long-term follow-ups.10,41
Because of its relative risk reduction for graft rupture, certain studies 40 advocate for the universal addition of anterolateral ligament reconstruction or LET in patients undergoing ACLR. We emphasize the importance of a more selective, “a la carte” approach guided by strict criteria. The goal of ACLR is to reduce anterior translation and rotational instability. An ACLR is efficient for controlling DATT due to translational forces, such as during the Lachman test; however, it does not decrease SATT, that is, the amount of tibial translation that occurs with axial load. LET will improve rotational laxity but not directly influence SATT. A slope-decreasing TDO will reduce the tibial slope and, subsequently, SATT.10,41 The selection of an appropriate strategy is essential for achieving optimal outcomes. Our findings provide further evidence that LET alone does not effectively address the increased SATT observed in cases with a steep tibial slope. Consequently, we advocate considering bony procedures to restore sagittal stability in such cases.
The choice of an associated procedure for ACLR should be based on a comprehensive clinical and radiographic assessment. LET may be suitable for cases with a high pivot shift, while TDO should be considered in patients with elevated SATT and increased tibial slope. However, further studies are required to determine whether TDO improves functional outcomes—an effect not shown with LET.42,49
Strengths and Limitations
The strengths of our study lie in several key aspects. First, we employed 2 validated methods for measuring SATT and DATT.7,13 In addition, we minimized the potential confounding effects associated with different grafts by excluding patients with graft types other than hamstrings. Moreover, all surgeries were performed by a single experienced ACLR surgeon (D.H.D.), enhancing consistency and reducing variability in our results.
As an initial limitation, the retrospective design of the study introduced inherent biases associated with observational studies. This was a radiographic study; therefore, it lacked an association with clinical outcomes, including failure rates. Our study had a relatively small sample size. Nonetheless, a post hoc power analysis using our standard deviation and sample size indicated that the study had 80% power to detect a difference in SATT of 1.8 mm between the groups but would have required a sample size of 444 patients in each group to detect a mean difference of 0.52 mm with 80% power. Given that Ni et al 38 provided an SATT threshold of 6 mm for an increased odds ratio of 9.9 for ACLR rerupture, we do not feel that increasing our sample size to detect a difference of 0.52 mm would be of clinical significance. With regard to DATT, a post hoc power analysis using our standard deviation and sample size indicated that the study had 80% power to detect a difference in DATT of 2.5 mm between the groups but would have required a sample size of 270 patients in each group to detect a mean difference of 1.29 mm with 80% power. Also, the 9-month follow-up may miss an attritional/fatigue benefit to LET on anterior translation. LET could provide indirect benefits over time if rotational biomechanics repeatedly stressed the graft, which would be reduced by a LET. A LET may result in a more compliant construct with a diminished ability to constrain both anterior tibial translation and internal tibial rotation. A longer follow-up would likely be needed to detect a difference attributable to this speculated mechanism. These limitations should be considered when interpreting our study results.
Conclusion
The findings of our study suggest that including a LET procedure in patients undergoing ACLR does not reduce SATT. It is crucial to consider the evaluation of this parameter before recommending an associated LET procedure in ACLR, particularly in patients with an increased tibial slope. Adding a TDO may be more appropriate to reduce the SATT in patients with increased tibial slope and associated increased static anterior tibial translation.
Footnotes
Final revision submitted October 24, 2023; accepted October 26, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ramsay Santé Recherche & Enseignement (ref No. IRB0010835).