
Abstract
Background:
There has been renewed interest in nonoperative treatment of anterior cruciate ligament (ACL) rupture following research suggesting that some ACL ruptures can heal naturally. However, the research is based on magnetic resonance imaging grading of ACL injuries rather than clinical signs, and the accuracy of the grading system is unknown. Nonoperative treatment of ACL ruptures has been associated with a higher risk of meniscal tears and recurrent instability, both of which may have long-term implications for the knee in terms of degeneration and the need for more complex stabilization surgery. More research into the nonoperative management of clinically significant ACL injuries is indicated before consideration for use in clinical practice.
Hypothesis:
Operative management of ACL rupture improves clinical outcome relative to nonoperative management.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The Covid-19 pandemic temporarily stopped elective surgery during 2020. For 2 months, those patients with isolated ACL ruptures underwent nonoperative treatment with bracing and physical therapy (Nonop group) were compared with a matched cohort undergoing ACL reconstruction (ACLR group) immediately before this period. Groups were compared at baseline with regard to age, gender, body mass index (BMI), lateral posterior tibial slope (LPTS), and the following patient-reported outcome measures (PROMs)—Tegner Activity Scale (TAS), International Knee Documentation Committee (IKDC), Sport and Recreation subscale (Sport/Rec) of the Knee injury and Osteoarthritis Outcome Score (KOOS), Knee Related Quality of Life (KR QoL) subscale of the KOOS, and Lysholm Knee Score (LKS)—as well as recurrent instability and meniscal tears, over a period of 3 years. Pearson chi-square test and analysis of variance were used for baseline characteristics, generalized linear models and multivariate tests for changes in PROMs, and chi-square tests for meniscal tears and recurrent instability. Statistical significance was accepted at P < .05.
Results:
A total of 82 patients were recruited, 41 in each group. The ACLR group and the Nonop group were similar with regard to all baseline variables, with the following mean ± SD values, respectively: age in years (22.1 ± 3.8 vs 21.3 ± 3.4; P = .23), BMI in kg/m2 (21.0 ± 2.0 vs 20.4 ± 2.5; P = .39), LPTS (8.1° ± 1.3° vs 7.9° ± 2.0°; P = .65), and preinjury TAS (8.2 ± 1.1 vs 8.7 ± 1.0; P = .33). The male:female ratio was 15:26 vs 17:24 (P = .71), respectively. At 3-year follow-up, the ACLR group had greater improvement in all PROMs than the Nonop group: TAS, 8.0 ± 1.0 vs 5.5 ± 0.9; IKDC, 90.9 ± 3.8 vs 65.0 ± 8.1; Sport/Rec, 92.4 ± 7.6 vs 66.6 ± 6.1; KR QoL, 91.1 ± 5.5 vs 74.3 ± 6.6; and LKS, 92.2 ± 4.9 vs 66.9 ± 6.1, respectively (all P < .001). There was a lower risk of both recurrent instability (5% vs 88%; P < .001) and medial meniscal tears (5% vs 63%; P < .001).
Conclusion:
ACLR results in a highly statistically significantly better clinical outcome than nonoperative management of ACL rupture in terms of PROMs, as well as a lower risk of both recurrent instability and meniscal tears, over a period of 3 years.
There are conflicting data in the literature with regard to the efficacy of nonoperative treatment of anterior cruciate ligament (ACL) rupture, and a variety of protocols have been used.2,3,10,27 Although 14% of ACL injuries have been reported to heal without surgery, this refers to partial tears diagnosed on magnetic resonance imaging (MRI) rather than clinical assessment, and some of these may be false positive diagnoses.2,3,33 There was increased interest in nonoperative management of ACL ruptures following the publication of a randomized controlled trial (RCT) in 2010, which concluded that an initial trial of nonoperative treatment was indicated. 10 However, subsequent RCTs in the literature found the opposite results with better outcomes following the reconstruction of both acute and chronic ACL ruptures relative to nonoperative treatment.2,26 Systematic reviews are unable to compensate for the poor level of scientific evidence available for the pooling of the results, but one such attempt has also been used to promote the nonoperative treatment of ACL rupture and was published in 2015. 7 More recently, an article published in the British Journal of Sports Medicine (BJSM) in 2023 claimed a 90% healing rate with a novel bracing protocol, and this has resulted in renewed interest in nonoperative treatment. 8
There are multiple different surgical techniques described in the literature, but prospective studies have demonstrated that failure rates of <2% per year are possible with a return-to-sport rate in excess of 90% when the reconstructive procedure corrects the anterolateral rotatory instability in the ACL-deficient knee.21,22,24 However, other factors unrelated to surgical technique influence the decision as to whether or not an athlete returns to competition. 1 Attempting to perform an RCT decades after the introduction of surgical treatment for ACL ruptures is challenging, as the position of clinical equipoise has been lost. The Covid-19 pandemic resulted in the closure of elective operating theaters across Australia in 2020 for a period of approximately 2 months. During that period, it was not possible to perform ACL reconstructions (ACLRs) unless there was another surgical indication. This provided the opportunity for the main author (M.D.P.) to allocate such patients to the nonoperative arm of a prospective cohort study. Although not an RCT, the timing of the commencement and duration of this shutdown period was random and beyond the influence of the surgeon or patient and therefore allocation of patients to treatment groups was, to some extent, random.
The objective of this study was to compare the clinical outcome in those patients presenting to the main author with an isolated ACL rupture and treated with bracing and physical therapy (Nonop group), relative to those treated with surgical stabilization (ACLR group). Our study hypothesis was that surgical stabilization would result in improved clinical outcomes relative to nonoperative treatment.
Methods
Patients presenting to the main author, a private subspecialist sports orthopaedic surgeon, during the Covid-19 induced shutdown of elective surgery (from March 16, 2020, to May 10, 2020) who met the study inclusion criteria (Table 1) were invited to take part in the study. They were referred for physical therapy to follow a standard protocol, similar to that used in the RCT performed by Frobell et al, 10 which reported successful outcomes with nonoperative treatment. Patients were informed that should their knee remain functionally unstable, and/or they developed meniscal tears, they would be able to undergo an ACLR if and when the lockdown period came to an end. These patients were allocated to the Nonop group.
Inclusion and Exclusion Criteria for Patient Recruitment a
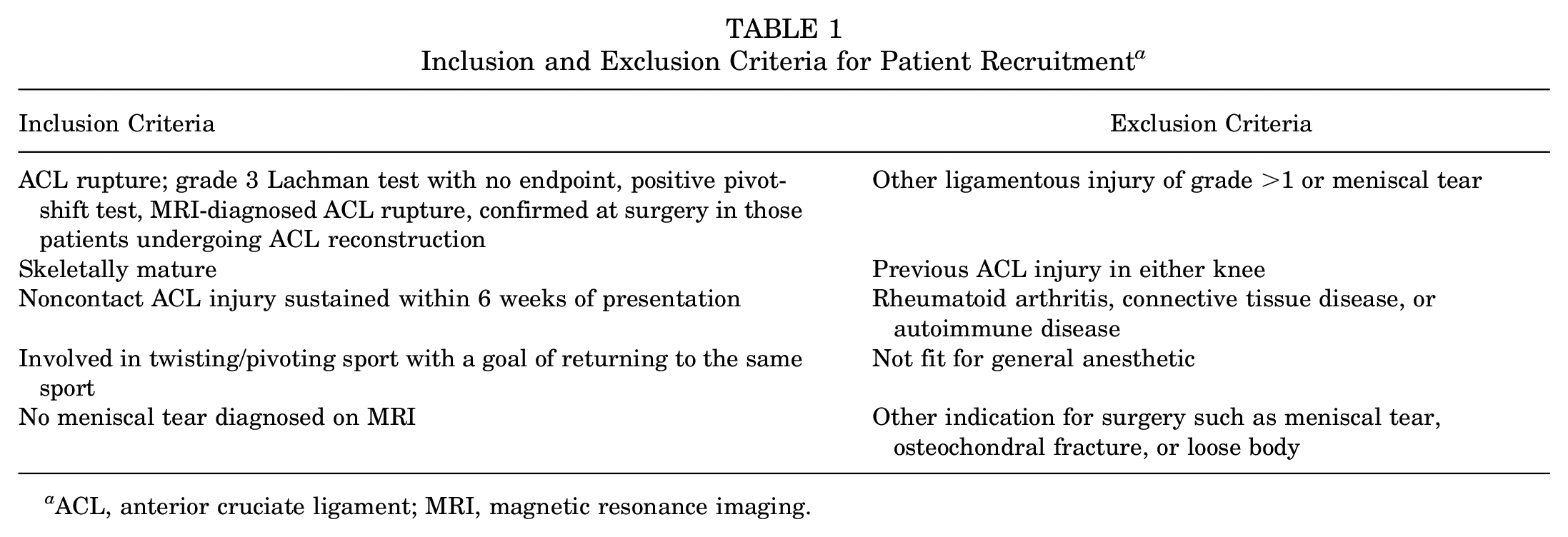
ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
The inclusion criteria used are detailed in Table 1. The clinical diagnostic signs for an ACL rupture were a grade 3 Lachman test with no endpoint to testing, as well as a pivot shift of ≥1 grade higher than the contralateral uninjured knee. These findings have been shown to have an accuracy of 93% using arthroscopy as the gold standard, with a kappa score of 72%.14,17,20 The pivot shift was performed in the standard manner, graded as 0 (none), 1 (glide), 2 (clunk), or 3 (gross). 13
The presence of a meniscal tear on the MRI was an exclusion criterion. The criteria used to diagnose a meniscal tear were a displaced meniscal fragment or tear visible on the MRI that communicated with a surface of the meniscus. Although MRI is not 100% accurate for diagnosis of ACL ruptures or meniscal tears, the same 3T MRI machine (Siemens) was used for all patients, and images were reported on by radiologists with a subspecialist interest in musculoskeletal medicine in an attempt to reduce potential bias or confounding. All MRIs were performed with standard sequences, and the criteria used to diagnose an ACL rupture were full disruption of the continuity of the fibers and edema of the ligament. These criteria have been shown to have a sensitivity of 0.77 and 0.83, and specificity of 0.83 and 0.92, respectively. 18
An increased lateral posterior tibial slope has been shown to be associated with an increased risk of recurrent ACL rupture in some studies and therefore is a potential confounding factor.6,34 For this reason, the lateral posterior tibial slope was measured on the MRI in all patients as described by Hashemi et al. 12 The measurement is described in detail in their article but, in summary, the posterior slope is defined as the angle between the slope of the lateral tibial plateau and a line perpendicular to the diaphyseal axis of the tibia in the sagittal plane.
Nonoperative Protocol
Patients were placed in an ACL-specific brace, found to be able to hold the tibia reduced on the femur and to reduce the strain on the ACL, as well as to protect the knee from ACL injury.9,11 The brace was locked at 30° of flexion for 2 weeks. After this, the patients followed the protocol described by Frobell et al, 10 while wearing the ACL-specific brace. The protocol is detailed in Table 2. The entire protocol was supervised by a physical therapist, not involved in the study, who was instructed to inform the treating surgeon of any noncompliance with the protocol. Depending on the specific Covid restrictions at the time of treatment, patients either attended physical therapy for treatment in person, or it was supervised via an online video link. The protocol was divided into 4 weekly intervals or levels, over a period of 4 months. Patients were only allowed to progress to the next level if the predetermined goals were met for range of motion, muscle function, and functional performance as determined by the treating physical therapist. The duration of the lockdown period was shorter than the rehabilitation program, and thus all patients in the Nonop group were reviewed in person by the treating physical therapist before completion of the program.
Nonoperative Protocol a
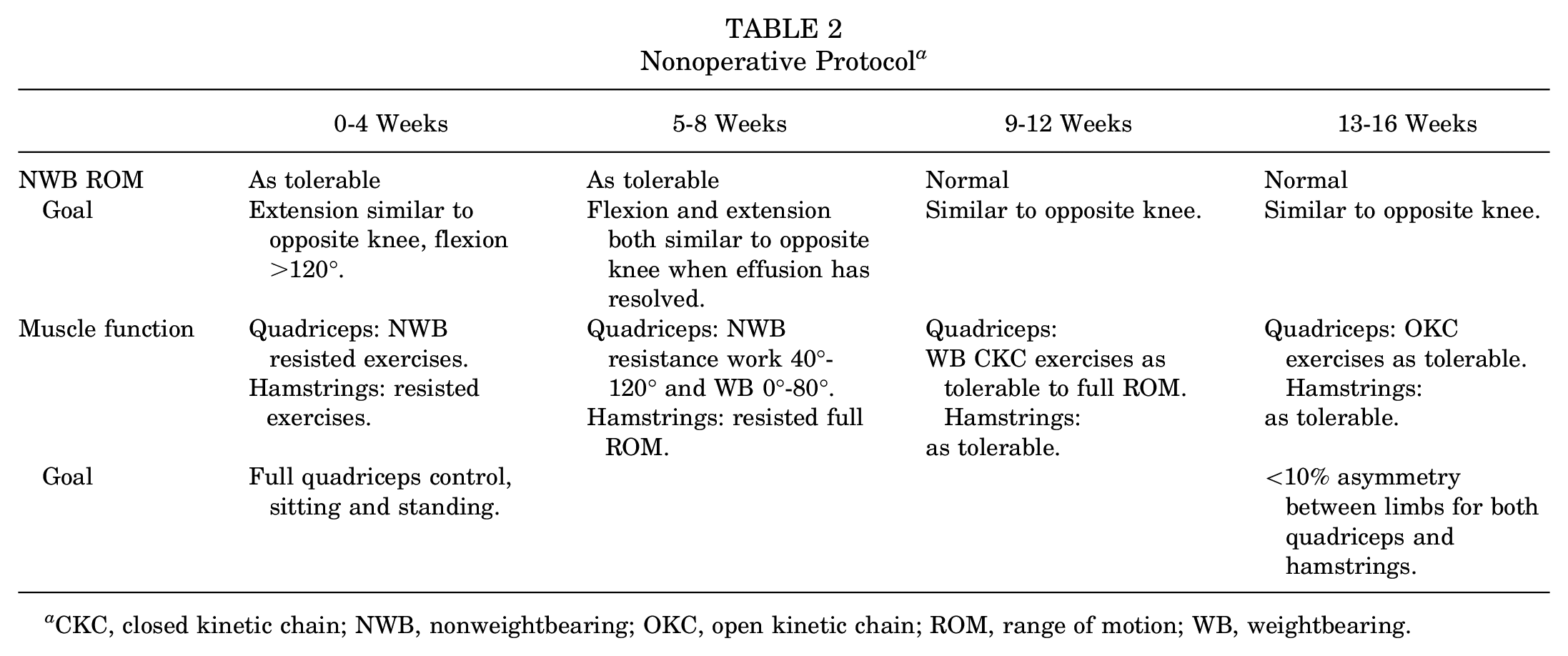
CKC, closed kinetic chain; NWB, nonweightbearing; OKC, open kinetic chain; ROM, range of motion; WB, weightbearing.
The control cohort, the ACLR group, comprised exactly the same number of patients who had been operated on immediately before the shutdown period and who satisfied the same inclusion criteria (Table 1). As is standard practice for the main author, they were consented to undergo surgical correction of the anterolateral rotatory instability of their knee. They were informed that this would be done using an ACLR, along with modified iliotibial band (ITB) tenodesis, if indicated. 24 The same surgeon performed all surgical procedures. ACLR was performed using a quadrupled hamstring tendon autograft. Graft positioning was in the manner described in the literature to correct the pivot shift in an ACL-deficient knee. 21 Aperture fixation was used in both bone tunnels to maximize correction of the pivot shift. 22 If there was a residual pivot shift ≥1 grade higher than the contralateral uninjured knee, a modified ITB tenodesis (MITBT) was added.24,25 The MITBT was performed as described in the literature with tensioning to the point that it corrected the pivot shift.24,25
Those patients in whom the ACL was found to be macroscopically intact during arthroscopy but diagnosed as ruptured on MRI (ie, false positive MRI diagnoses) underwent an ACL repair rather than a reconstruction. These patients were not included in the study.
The baseline data and outcomes of interest in the study design were routinely collected by the main author and stored on a secure database. All patients provided written informed consent to take part in the study and for their anonymous data to be included in the analysis.
Outcomes of Interest
Following are the validated accurate patient-reported outcome measures (PROMs) used, with their minimal clinically important difference (MCID) values.
Tegner Activity Scale (TAS): 1 point4,32 Subjective International Knee Documentation Committee: 5 points16,19 Knee Osteoarthritis Outcome Score (KOOS) Sport and Recreation subscale (Sport/Rec) & KOOS Knee Related Quality of Life subscale (KR QoL): 10 points
28
The PROMs were completed at baseline and repeated 12, 24, and 36 months after injury. Patients were re-examined at 12, 24, and 36 months after surgery, with their Lachman and pivot-shift scores recorded. Patients were also asked to report any recurrent instability and/or occurrence of mechanical symptoms such as locking, catching, pain, or swelling in either knee. If patients developed these symptoms, the MRI was repeated and the presence of a meniscal tear and/or ACL graft rupture diagnosed using the same MRI criteria as described above. TAS at baseline referred to their level of activity before the injury. All data were stored on the surgeon’s private database.
Power Analysis and Sample Size
Based on previous research performed by the authors using these PROMs after ACLR and a power analysis calculation, a minimum study size of 42 was required to achieve a power of 80% and a risk of type 1 error of 5% using the MCID values above.23,24
Statistical Analysis
The baseline characteristics of the 2 groups were compared using the Pearson chi-square test and analysis of variance, generalized linear models and multivariate tests were utilized for changes in PROMs, and chi-square tests for the risk of meniscal tears and recurrent instability. The analysis was performed at 1, 2, and 3 years after commencement of treatment. P < .05 was used as the level of statistical significance. The analysis was performed using SPSS Version 26 software.
Results
During the 2-month lockdown period, 61 patients presented with an ACL rupture diagnosed on both MRI and clinical assessment. Twenty of these patients were excluded from the study. Nine had MCL injuries of grade 2 or 3 severity, and 11 had meniscal tears (7 lateral and 4 medial). The remaining 41 patients satisfied all the study criteria and agreed to participate in the study, comprising the Nonop group.
The 41 patients presenting immediately prior to the theatre shut down with an ACL rupture and satisfying the study criteria comprised the ACLR group. Of 7 patients presenting with an MRI diagnosis of ACL rupture, 18 were found to have a macroscopically intact ACL, albeit lax at arthroscopy. These false positive MRI diagnoses (24%) were treated with an ACL repair and were not included in the study. Of the 58 patients with ACL rupture confirmed at arthroscopy, 17 were excluded from the study, 12 due to the presence of a meniscal tear (8 lateral and 4 medial) and 5 due to the presence of a medial collateral ligament (MCL) tear treated with bracing (2 patients) or MCL repair (3 patients). The remaining 41 patients comprised the ACLR group. Of these patients, 5 had an MITBT added to their ACLR.
All patients provided written consent to take part in the study and agreed to have their anonymous data included in the study. No patient refused to take part in the study. The study was approved by the ethics committee at the hospital where the ACLRs were performed, and regional ethics approval was deemed not to be necessary.
Baseline Characteristics
As seen in Table 3, the 2 groups were similar with regard to the potential confounding factors of male-to-female ratio, age, body mass index, lateral posterior tibial slope measurements, dominance of the injured side, and TAS scores.
Baseline Data a

Data are presented as mean ± SD unless otherwise indicated. Sex and knee dominance were compared using cross-tabulation (Pearson chi-square test) and analysis of variance was used for age, BMI, LPTS, and TAS before injury. BMI, body mass index; F, female; LPTS, lateral posterior tibial slope; M, male; TAS, Tegner Activity Scale.
Sports Participation
Patients were asked to record the sports to which they wished to return. In the ACLR group, there were 23 rugby players, 12 soccer players, 3 touch football, and 3 netball. In the Nonop group, there were 20 rugby players, 9 soccer, 8 touch football, and 4 netball.
Recurrent Instability
The incidence of recurrent instability over the 3-year follow-up was higher in the Nonop group than the ACLR group (P < .001).
In the ACLR group, 2 patients (<5%) experienced recurrent instability of the knee and were diagnosed with ACL graft rupture on both clinical assessment and MRI, occurring 16 months and 20 months after ACLR surgery. Both were managed with a revision ACLR.
In the Nonop group, 36 of 41 patients (88%) developed ongoing instability over the 3-year follow-up, and these patients all requested an ACLR. Eight patients experienced instability within the first year (20%), 12 within the second year (29%), and 16 during the third year (39%). PROM data were only included in the statistical analysis until the knee experienced recurrent instability. Including data after this would have disadvantaged the Nonop group on account of the precipitous fall in scores after reinjury.
Meniscal Tears
Over the 3-year period, the Nonop group had a higher risk of medial meniscal tear than the ACLR group (53.7% vs 2.4%; P < .001). The incidence of lateral meniscal tears was also higher in the Nonop group but did not reach statistical significance (9.8% vs 2.4%; P = .17).
Patient-Reported Outcomes
The ACLR group had greater improvement in all PROMs, and the results are summarized in Table 4.
Comparison of PROMs, Recurrent Instability, Contralateral ACL Rupture, and Meniscal Tear in Both Groups at Baseline and Over the 3-Year Follow-up a

Data are presented as mean ± SD or n (%). ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; KR QoL, Knee Related Quality of Life; LKS, Lysholm Knee Score; LM, lateral meniscus; MM, medial meniscus; PROM, patient-reported outcome measure; Sport/Rec, Sport and Recreation; TAS, Tegner Activity Scale. Multivariate tests using generalized linear models were used to compare the PROMs. The chi-square test with Yates correction was used to compare rates of recurrent instability, meniscal tears, and contralateral ACL rupture.
Other Outcomes
The number of contralateral ACL ruptures was 3 in the ACLR group and 1 in the Nonop group (P = .31). There were no significant complications in the ACLR group, while 2 patients in the Nonop group developed deep venous thrombosis and were treated with oral anticoagulation.
On examination of the injured knee at 3-year follow-up, there were 22 patients in the Nonop group who had a pivot shift of ≥1 grade higher than at baseline and none had a reduced pivot shift. In the ACLR group, all patients had a negative pivot shift at 3-year follow-up.
Summary of the Analysis
ACLR group patients had a lower risk of recurrent instability, lower risk of medial meniscal tears, and higher PROMs, with a similar risk of complications when compared with the Nonop group. Figure 1 demonstrates the changes in these outcomes over time in the 2 treatment groups.

TAS (Tegner Activity Scale), IKDC (International Knee Documentation Committee), Sport/Rec (Sport and Recreation), KR QoL (Knee Related Quality of Life), and LKS (Lysholm Knee Score), and incidence of recurrent instability as a percentage of total, in Groups A (ACLR) and B (Nonop), plotted against time.
Discussion
The results of this study suggest that patients with an isolated ACL rupture participating in pivoting sports, treated with a combination of bracing and physical therapy, have a highly significantly increased risk of recurrent instability and meniscal tear relative to those undergoing a surgical correction of their anterolateral rotatory instability. Those patients undergoing reconstruction recorded higher PROMs, and there was no evidence of an increased complication rate in the group managed with surgery. Therefore, we accepted the study hypothesis.
Although there remains interest in the nonoperative management of ACL injuries, there are few new data to support this approach. Frobell et al 10 performed an RCT in 2010 (the “KANON study”) comparing operative treatment with nonoperative treatment and the option to have surgery subsequently if required. In practice, those patients undergoing nonoperative treatment who remain unstable represent failures of nonoperative treatment from the patient’s perspective. In that study, they found that the risk of recurrent instability in the nonoperative group was 39% within 2 years versus 3% in the operative group (13 times higher), and the risk of meniscal tears was 22% versus 1.5% (15 times higher). Although the conclusions drawn by the researchers were that attempting rehabilitation with these high failure rates was acceptable in their opinion, from the patient’s perspective it is less likely to be acceptable. For some patients, the delay in recovery and return to competitive sport incurred by attempting nonoperative treatment only to undergo surgery at a later date may also be unacceptable for career, financial, social, or personal reasons. The KANON study excluded patients with a TAS score of 10, and the exclusion of these patients competing at an international level would be likely to bias the study in favor of nonoperative treatment. In our study, a preinjury TAS score of 10 did not exclude patients from the study and this may have contributed to the higher rate of recurrent instability we found in the Nonop group.
Other RCTs have shown contrasting results to those from the KANON study with regard to the treatment of acute ACL ruptures. The “COMPARE” study was an RCT of similar size to the KANON study, and it also compared early ACLR with rehabilitation followed by optional delayed ACLR. 26 Approximately 50% of the patients in the rehabilitation group failed to regain stability and required ACLR. Those patients randomized to undergo reconstruction were found to have a higher level of knee function and sports participation.
Another larger multicenter RCT, 2 in which patients with chronic ACL deficiency and functional instability were randomized to either early ACLR (156 patients) or rehabilitation (160 patients), found that reconstruction resulted in a greater improvement in PROMs (KOOS subscales) and was more cost-effective in terms of quality of life years than rehabilitation. The rehabilitation group had a failure rate of 41% requiring surgical stabilization within a period of 18 months.
Although a recent publication by Filbay et al 8 has been used to promote nonoperative treatment with brace for ACL ruptures, that study was an uncontrolled cohort study of 80 patients, without any blinding. The diagnosis of both the ACL rupture and its healing was based solely on MRI imaging, using a grading system not validated for the grading of the ACL injury itself, with a follow-up period of only 12 months. MRI has been shown to be no more accurate than clinical assessment and has limited value as a research tool.18,20,33 The number of false positive MRI diagnoses in their study is unknown, but in our study it was 24%. The bracing protocol they used was not free of complications. It involved a period of immobilization with the knee flexed to 90° and was associated with an increased risk of deep venous thrombosis. The authors stated that “longer term follow-up and clinical trials are needed to inform clinical practice.” Unfortunately, the publication of an uncontrolled, short duration, unblinded, and low level of evidence study is likely to violate the position of clinical equipose and may result in a volunteer bias in all future studies involving the use of that bracing protocol. We suggest that RCTs be indicated for comparing the novel bracing protocol with current bracing protocols, using clinical assessment and MRI for diagnosis of the ACL rupture, and then RCT comparing ACL repair with the use of nonoperative treatment in those patients for whom this may be appropriate. We would advise that patients be informed that the recommendation of this protocol as a reasonable treatment option is premature, lacking in evidence, and associated with a risk of thromboembolic phenomena.
In our study, there was a 13-fold higher incidence of meniscal tears in the patients undergoing rehabilitation rather than surgery. Despite the initial optimism with regard to the outcome after rehabilitation quoted in the KANON study above, when Snoeker et al 30 reviewed the same patients from that study at 5 years, they found that patients who underwent ACLR had a lower risk of medial meniscal tears and a lower risk of progression of the meniscal tears seen on MRI. The cause of the medial meniscal tears may be the ongoing anterolateral rotatory instability and possible progression in the severity of this instability. Other research has reported an increased risk of developing meniscal damage after ACL injury, with this used as a rationale for performing early ACLR. 31 In vivo studies had found an association between length of time between ACL rupture and surgical stabilization, and the degree of both sagittal plane and coronal plane laxity found at surgery. 29 Other studies have also suggested that there may be progression of the anterolateral rotatory instability seen in ACL-deficient knees over time due to chronic attenuation of secondary stabilizers of the knee, including the anterolateral complex, as they take over the role of the deficient ACL.25,29 There was some evidence of this in the current study, as half of all patients treated nonoperatively demonstrated a progression of the grade of the pivot shift over the 3 years, which did not occur in the surgically treated group. However, our study was not sufficiently powered to determine if this was statistically significant. Interestingly, there was a higher risk of contralateral ACL rupture in the operative group (7% versus 2%), but this is likely related to the higher rate of return to pivoting sports in the operative (ACLR) group and the high rate of failure to recover sufficiently to return to sport in the Nonop group.
In each of the 3 RCTs referred to above,2,10,26 there was a higher frequency of recurrent instability in the Nonop group, and being a time-dependent figure, the magnitude of the difference, or the relative risk of recurrent instability, will increase with the duration of follow-up. In our study, the cumulative percentage of patients experiencing failure of treatment in the physical therapy group was 20%, 49%, and 88%, at 1, 2, and 3 years of follow-up, respectively. The follow-up period of only 12 months in one published cohort study 8 is too short with regard to clinical outcome and unlikely to appreciate any progressive deterioration in instability associated with an attempt to return to pivoting activities.
A paper published in the BJSM by Filbay et al, 7 described as a “meta-analysis,” was a systematic review of predominantly level 3 and 4 studies. The single RCT included in this systematic review was the KANON study, and the pooling of this single RCT with cohort studies comparing operative and rehabilitation treatment would appear inappropriate. The systematic review should have concluded that there were insufficient data available to perform a useful meta-analysis.
As our knowledge with regard to the anatomy and function of the ACL has improved, as well as its central role in the more complex phenomenon of anterolateral rotatory instability to which other injuries may contribute, so too have the surgical techniques to correct this. The surgical goal of the main author was to correct the pivot shift, using an ACLR and added MITBT only if indicated to correct a residual pivot shift. The MITBT has been shown to be more effective in its ability to reduce the risk of recurrent instability when compared with lateral extra-articular tenodesis (LET). 23 This may be related to the more precise intraoperative adjustment of the tension in the MITBT procedure to the point that it corrects the pivot shift, instead of the relatively arbitrary “hand tensioning” of the LET. It is for this reason that the ACLR group included patients both with and without the MITBT, as the endpoint of the surgical stabilization was correction of the pathological pivot shift, rather than the use of preoperative criteria to determine if the tenodesis was indicated.
Nonoperative management techniques have also improved. The improved understanding has resulted in the categorization of patients as potential copers or noncopers, along with those patients who adapt their lifestyle to live within the envelope of stability they retain. 5 However, the challenge remains how to accurately predict which category a patient will fall into.
There is some debate with regard to what value is a meaningful change in the KOOS in patients after an ACL injury. Ingelsrud et al 15 have recommended the use of subscale specific values for the KOOS, with 12.1 for the Sport/Rec subscale and 18.3 for the KR QoL subscale. Those researchers used a predictive modeling method based on retrospective data, which was incomplete for >50% of the patients, and thus there is an inherent degree of inaccuracy in the conclusion. However, even the use of their larger values as subscale MCIDs would not alter the results of our statistical analysis, and the study hypothesis would still be accepted.
Limitations
The limitations of our study include the relatively small sample size; however, it was adequately powered to compare the outcomes of interest and to test the study hypothesis. The study was not an RCT, yet there was no bias with regard to group allocation, as all patients evaluated during the shutdown period had no choice but to undergo nonoperative treatment, and all agreed to take part in the study. The surgeon had no prior knowledge with regard to either the date of the commencement of the shutdown period or its duration. Therefore, although not providing evidence as strong as that from an RCT, there was also no volunteer bias, which was seen to a certain degree in the 3 RCTs referred to above. All the data collected and included in the study are a routine component of the main author’s standard patient follow-up; and although it is a retrospective study, the data were collected prospectively. All procedures were performed by a single subspecialist orthopaedic surgeon, and this limits the external validity of the findings. Although patients in the Nonop group may not have attended physical therapy in person for part of their treatment, all were supervised, albeit partially via video link, and most patients would have had more time at their disposal to dedicate to their rehabilitation exercises.
Conclusion
With these limitations in mind, we conclude that patients with an isolated ACL rupture sustained in a noncontact injury during sports participation, diagnosed on clinical assessment and MRI, have a lower risk of recurrent instability and meniscal tear if treated with surgical stabilization rather than bracing and rehabilitation, as well as improved clinical outcomes in terms of validated PROMs.
Footnotes
Final revision submitted August 29, 2024; accepted October 4, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Barton Private Hospital.