
Abstract
Background:
The use of functional knee braces for returning to sports or during demanding activities following anterior cruciate ligament rupture is common; yet despite being commonly prescribed, its mechanism of action remains unknown.
Objectives:
To examine the effect of functional knee braces on mean muscle activity when performing lunge exercises.
Study design:
Pre-/post-test (within-subject research design).
Methods:
A total of 10 male participants with unilateral isolated anterior cruciate ligament deficiency participated. Electromyographic activities of six muscles around the knee were recorded during lunge exercises, with and without wearing a custom functional knee brace. The lunge cycle movement was subdivided into three phases: eccentric, isometric, and concentric.
Results:
The quadriceps and hamstrings were no different in the braced and unbraced conditions. When braced, the mean amplitude of the medial gastrocnemius was significantly lower throughout the whole movement (p = 0.01) and during the concentric (p = 0.006) and eccentric (p = 0.028) phases, but not within the isometric phase. The lateral gastrocnemius was found to have lower mean amplitude in the isometric phase (p = 0.044).
Conclusion:
With its origin on the medial femoral condyle, perhaps reduced medial gastrocnemius activity may better guide knee rotation and assist the joint achieving a healthier kinematic pattern.
Clinical relevance
Lower medial gastrocnemius activity may facilitate lower medial compartment contact pressure, for which greater loading is known to increase the risk of osteoarthritis in anterior cruciate ligament–deficient (ACLD) knees. However, further research is needed.
Background
Use of functional knee braces (FKBs) for returning to sports or during demanding activities following anterior cruciate ligament (ACL) rupture, despite being arguable, is common. 1 The financial cost of functional bracing for ACL injuries among the Americans and Scandinavians combined accounts for about US$65,000,000 annually. 2 While braces are prescribed to stabilize the injured knees, functional stability has been defined in a broader multifaceted context. It is known that ACL deficiency deprives the joint of the sensing function of mechanoreceptors that lie within the ligament, as well as the mechanical role of the ligament itself. 3 It is also well known that muscle activity is altered after ACL rupture, evident by increased hamstring activity, 4 decreased quadriceps activity, 5 reduced gastrocnemius activity during level walking, 6 and increased activity in ramp descent. 7 Some describe this as a protective mechanism (decreased quadriceps or gastrocnemius activity as ACL antagonists), while others suggest this as a knee stiffening mechanism (increased hamstring or gastrocnemius activity as ACL synergists).
Evidence suggests FKBs influence neuromuscular function during gait and sport activities. However the mechanisms behind that is, cutting, 8 jumping, 9 running, 10 and so on. But the mechanisms behind these adaptations remain unknown. Some suggest the brace acts mechanically to stabilize the knee, 11 whereas others suggest the brace acts proprioceptively. 9
No one, to our knowledge, has investigated the influence of functional knee bracing on neuromuscular function in ACL-deficient (ACLD) knee joints when performing lunge exercises. The lunge is a closed chain weight-bearing exercise that is usually part of rehabilitation programs for returning to sports. This exercise has been suggested as an appropriate test to discriminate knee function between copers and noncopers for ACL deficiency. 12 There is a belief that closed kinetic chain (CKC) exercises are safe for ACL, but recent reports claim that these types of exercises are not necessarily safer for patients with ACL deficiency.13,14
Therefore, the aim of this study was to examine the effect of FKBs on muscle activity when performing the lunge exercise. We hypothesize that wearing functional braces alters the neuromuscular function of the muscles about the knee during lunge exercise, thereby influencing stabilization. Considering the lunge exercise a safe or not so safe activity for ACLD knees, and understanding the effects of FKBs on neuromuscular control in ACLD knees perhaps will provide clinicians with more information that may lead to better decision-making process in this regard.
Methods
Participants
A total of 10 male participants with unilateral ACL injury were selected from a cohort of patients referred to a medical imaging center, and their magnetic resonance imaging (MRI) report confirmed ACL injury (convenient sampling). Their age ranged between 18 and 65 years, and they gave informed consent (approved by Ethics Committee of University of Welfare and Rehabilitation Sciences) to participate in the study. Inclusion criteria included diagnosis of unilateral ACL rupture confirmed by MRI and clinical examination by an orthopedic surgeon. Exclusion criteria were multiple ligamentous or meniscal injuries, pain, and effusion. Participants completed the Tegner Lysholm Knee Scoring Scale 15 regarding their level of activity before injury and at the time of the study.
FKB
A mold of the involved limb was obtained by tracing and exact measurement by a certified orthotist, from which custom type of braces was fabricated specific to each individual’s leg shape and alignment. Braces were manufactured with an anterior and posterior leg and thigh shell which consisted of thermoform plastic sheets that were shaped specific for each subject based on the tracings of the entire limb using precise measurements of the limb contours. The anatomical dimensions of the body segments were measured precisely, and a negative cylindrical cast of the subject’s shank was made to ensure a total shell-to-skin contact. The impression cast was shaped in non-weight-bearing sitting position, with the knee and ankle in the right angle, from standard rigid plaster. The orthotic knee joint was a standard polycentric hyper-extension controlling joint (17K48; Otto Bock, Duderstadt, Germany), with bars made from non-metallic materials. The straps of the brace were fastened for each subject to the maximum tolerable tension that was measured using a load cell to be within the range suggested in the literature. 16 Figure 1 shows a brace fabricated for one of the participants.

A custom-molded functional knee brace was manufactured for each participant.
Electromyography instrumentation
Electromyographic (EMG) activity was recorded using a Biometrics DataLog W4X8 (Biometrics Ltd, Newport, UK). Recordings were sampled at 1000 Hz and bandpass filtered between 20 and 450 Hz in the hardware. Prior to electrode placement, the skin was dry shaved, abraded, and cleaned with isopropyl alcohol to ensure low impedance. Pre-amplified bipolar surface electrodes (SX230; Biomectrics Ltd) with an interelectrode distance of 20 mm (gain: 1000, input impedance ≥10,000,000 MΩ, common mode rejection ratio (CMMR) at 60 Hz >96 db) were placed over vastus medialis and lateralis, medial and lateral hamstrings, and medial and lateral gastrocnemius in accordance with the methods described by Criswell. 17 Raw EMG data were transmitted to the eight multichannel data logger for differential amplification. A reference or ground electrode was placed over the wrist bony prominence to reduce electrical interference contaminating the signal. To avoid the influence of movement artifacts, electrodes and cables were taped to the subject. Palpation and isometric muscle testing were performed for each muscle in isolation to ensure correct electrode placement, to visually inspect the signal response and adjust the gains, and to record maximal voluntary isometric contractions (MVICs) necessary for normalization according to Konrad. 18 The two middle seconds of a 6-s contraction were recorded and averaged over three MVIC trials.
Two ports of the system were used for twin axis goniometers. Offline analysis of the signals was supported by DataLog analysis software (DataLog PC software version 7.50).
Test process
Subjects were asked to perform slow lunge exercises with their injured leg positioned (1) forward, (2) flex the knee and move down (eccentric phase), (3) remain stationary with the injured knee at maximum bent for a short period of time (isometric phase), and (4) then return back to the initial standing position (concentric phase). Figure 2 depicts a typical lunge cycle graph. Participants were required to keep the trunk upright throughout the maneuver while performing the lunge exercise with and without brace (three repetitions of each condition).
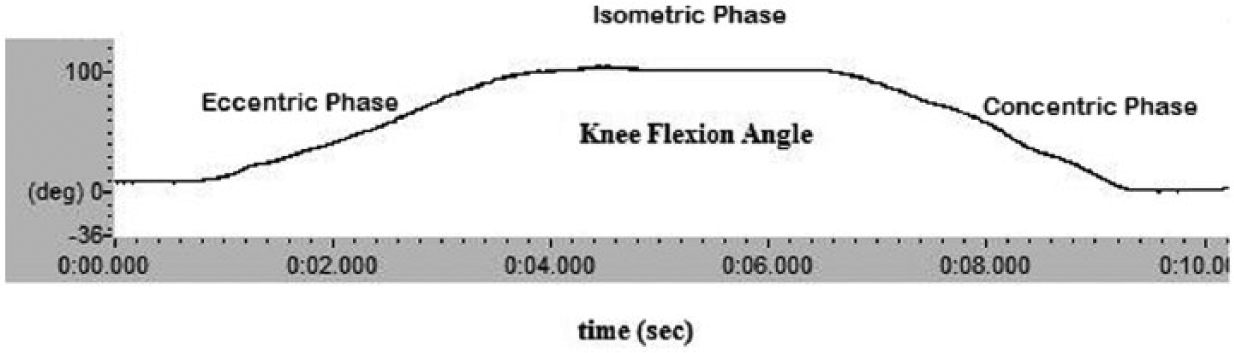
A typical lunge trial divided into three phases: eccentric, isometric, and concentric.
EMG processing
A root mean square (RMS) filter in the proprietary software set with a 50-ms 19 filter constant was used to process the EMG raw data. The start and end points of the cycles were considered a 5% threshold of the maximum amplitude on the knee sagittal range of motion graphs. The mean amplitude was recorded for the whole cycle in the marked area. The cycle itself was divided into three constituent parts: an eccentric or knee flexion phase, a concentric or knee extension phase, and isometric phase or plateau of the graph where mean and peak amplitudes were recorded for each phase separately and reported as percentage of MVIC.
Statistics
The braced and unbraced conditions were compared using a paired t-test. All the statistical tests were performed using SPSS (version 17; SPSS Inc., Chicago, IL), with the level of significance set at 0.05.
Results
Participants
Table 1 shows the general information of participants. All participants performed the lunge exercise without pain and difficulty. A representative cycle took 10.97 ± 5.05 s to complete without brace and 11.89 ± 5.69 s with brace (p = 0.035). By dividing the cycle into three phases, when wearing the brace participants took longer to complete the eccentric phase (4.31 ± 1.93 s without brace, 4.96 ± 2.25 s with brace; p = 0.008).
General information of the participants (n = 10).

SD: standard deviation.
Vasti
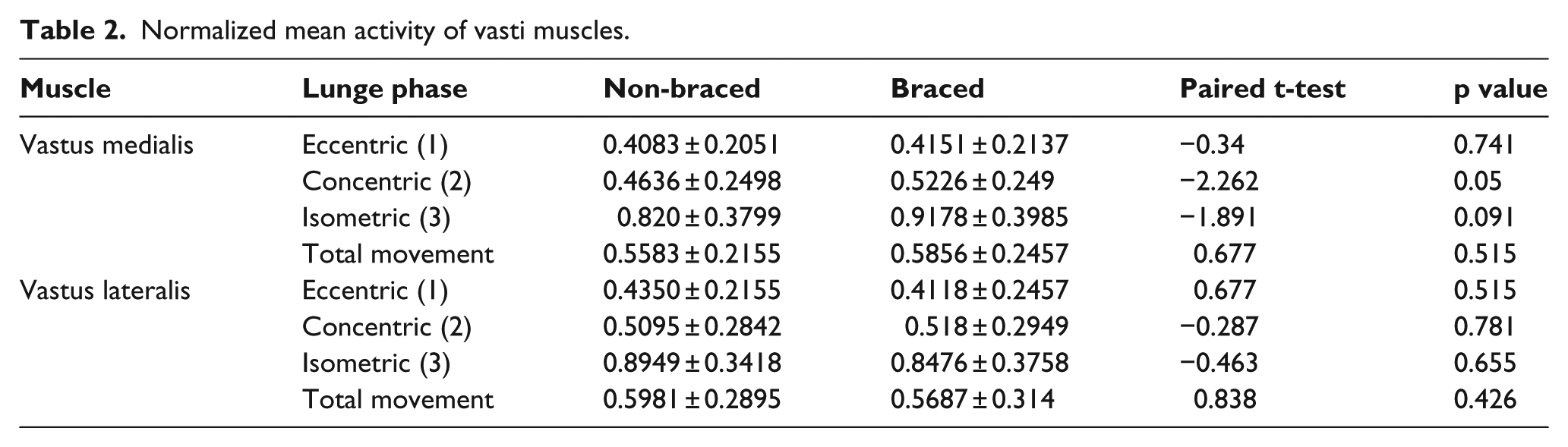
Figure 3 depicts a representative trial of raw EMG of all studied muscles including vastii activity during a single lunge trial with and without brace. Overall, no significant differences were seen in the mean activity of vastii muscles (Table 2).
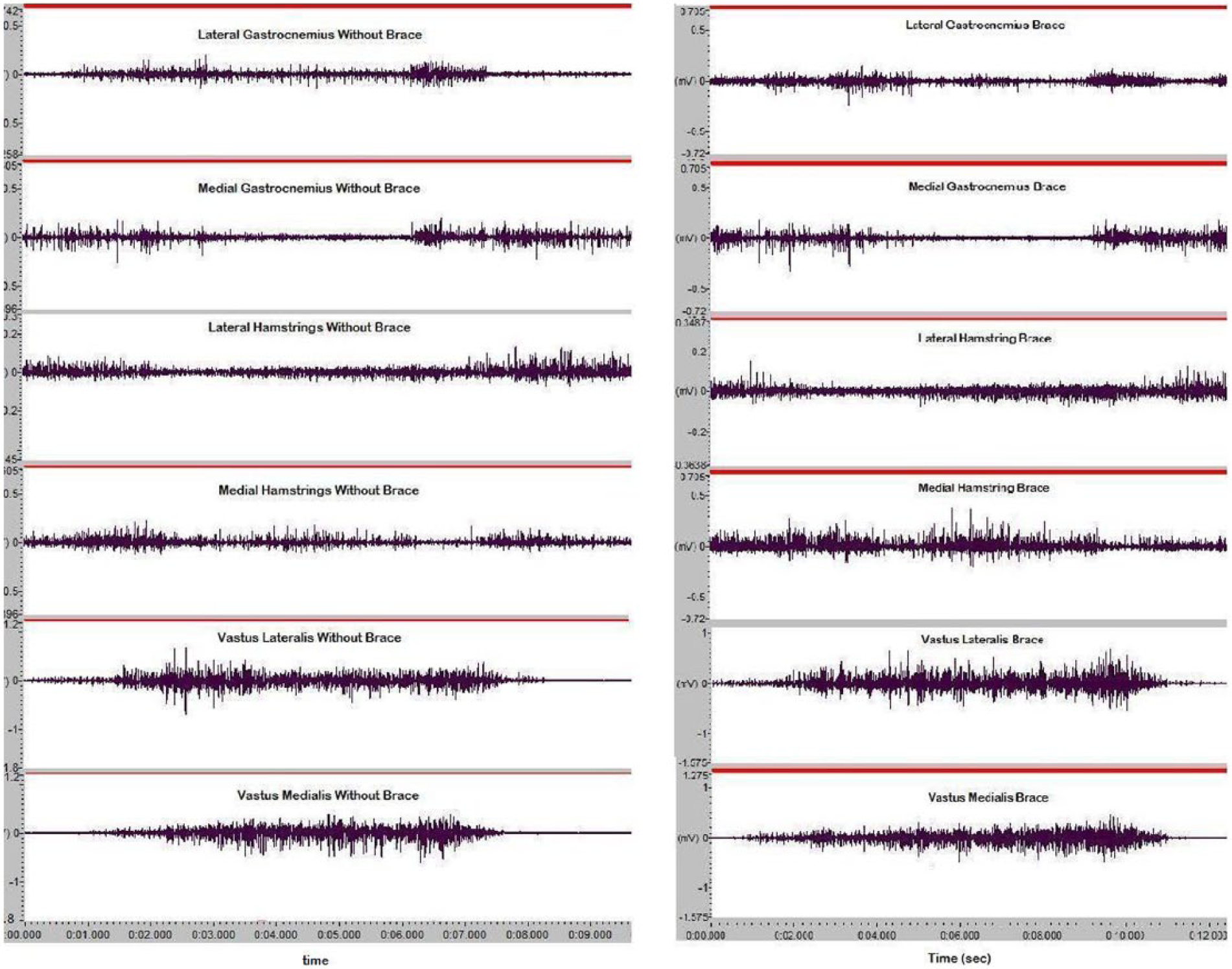
Raw EMG data of all muscles studied in unbraced (left) and braced (right) conditions during a lunge trial performed by one of the subjects. From up to down: lateral gastrocnemius, medial gastrocnemius, lateral hamstring, medial hamstring, vastus lateralis, and vastus medialis.
Normalized mean activity of vasti muscles.
Hamstrings
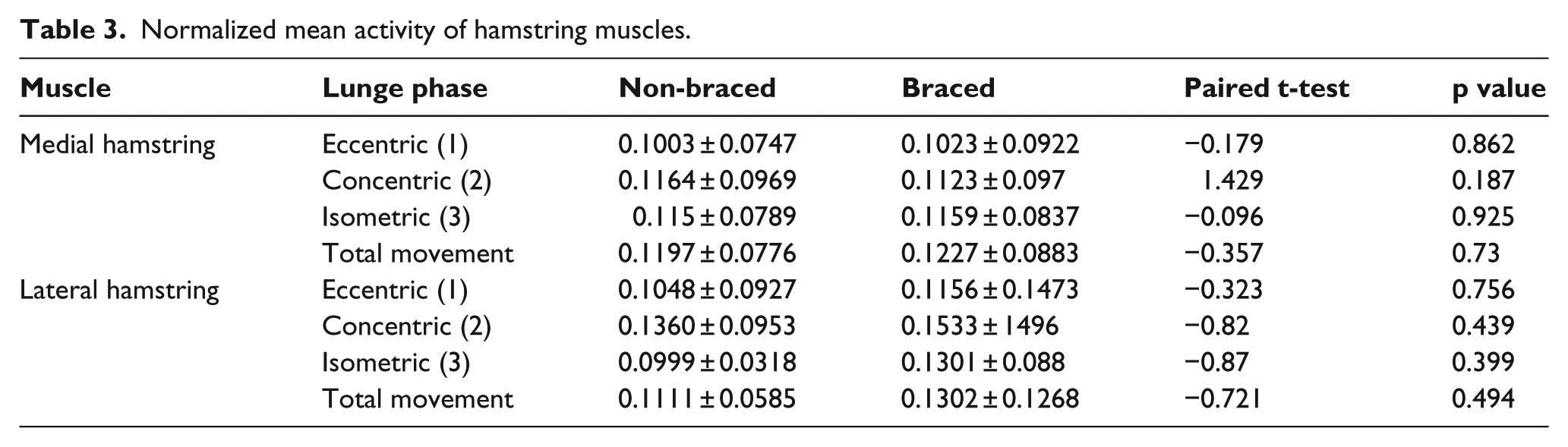
Bracing had no significant effect on the mean amplitude of hamstrings (Table 3).
Normalized mean activity of hamstring muscles.
Gastrocnemius
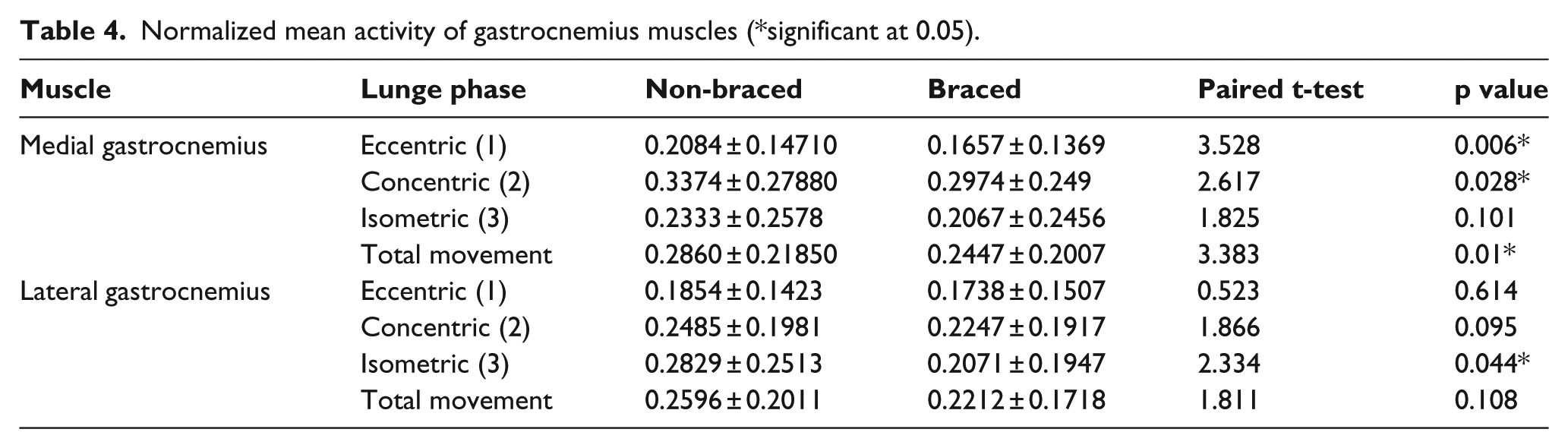
As a result of bracing, the mean medial gastrocnemius activity was altered (Table 4). In the braced condition, the mean amplitude was statistically lower over the whole maneuver (p = 0.01), including the concentric (p = 0.006) and eccentric (p = 0.028) phases but not during isometric phase. The lateral gastrocnemius exhibited statistically lower mean amplitude only in the isometric phase (p = 0.044).
Normalized mean activity of gastrocnemius muscles (*significant at 0.05).
Discussion
In this study, muscle activity about the knee was recorded during lunge exercises, with and without wearing an FKB which is worn for ACL deficiency. While brace wear did not negatively affect knee range of motion, the time to perform the lunge was (0.92 s) statistically longer when wearing the brace (p = 0.035). By dividing the lunge cycle into three discrete phases (eccentric, isometric, and concentric phases), difference in timing was evident, primarily in the first phase. No changes were noted in the remaining phases. While FKBs are designed to be worn during activity, there is always a concern that its influence may negatively impact performance and agility. Yet, the work by Rishiraj et al. 20 has shown that having worn braces for up to 12–14 h does not show performance deficits. However, the test condition utilized in our study was not challenging and the speed of movement was not high. Therefore, lack of any differences in knee range of motion between the braced and non-braced conditions is not unexpected. Knee bracing would produce a different impact on activities that are more ACL challenging, for example, open kinetic chain exercises, particularly if they are performed at higher speeds, with a lower level of neuromuscular control. Moreover, the difference in time of lunge performance may be resolved with longer wearing time, considering the fact that the adaptation time with brace was short in our study.
ACL injury has widely been acknowledged to affect neuromuscular function, perhaps leading to altered muscle activation patterns and reduced eccentric quadriceps control for the injured knee. 5 Some suggest this is evidenced by “Quadriceps avoidance,” which is a term to describe elimination of external knee flexor torque during the stance phase of gait. Others, however, call into question this phenomenon. 21 Williams et al. 5 described poor quadriceps control as failure to turn “off” the quadriceps at the appropriate time. Torry et al. 21 speculated changes in activation pattern and control mechanisms may be individual. For persons with ACL deficiency, prolonged hamstring activity with concomitant higher magnitudes has also been reported 21 or delays in hamstring reflex evident. 22 Shelburne et al. 23 suggested that hamstring facilitation pattern perhaps would be more effective in stabilizing the injured knees.
Whereby prescribing FKBs is thought to mediate improved functional stability after injury, the mechanism remains uncertain. Moreover, why performance is improved as reported by persons with ACL deficiency while wearing an FKB24–26 is also unclear.
Quadriceps and hamstrings
Smith et al. 22 reported that ACLD patients experience a better sense of stability with bracing. A delayed vastus lateralis muscle response was observed when donning the brace, whereas the hamstrings were activated earlier. Among active ACLD individuals, improved function with FKB and the task of study was hopping maneuver. Acierno et al. 11 found that quadriceps activity increased with concomitant reductions in hamstring activity while wearing the Pro Shifter Bledsoe knee brace during low activity among symptomatic subjects. Perhaps the results suggest bracing mediates a neuromuscular compensatory response favorable for persons with ACL deficiency. Other notable changes have been reported. Branch and Hunter 27 saw decreased quadriceps and hamstring activity (including the gastrocnemius) during side-step cutting perhaps refuting the notion of proprioception. Ramsey et al. 9 reported decreased contribution of the hamstrings and increased quadriceps activity with brace, despite no alteration in anterior tibial translation. The varied results suggest different theories of the protective role of bracing, that is, mechanical stabilizing role when agonists and antagonists both decreased activity and proprioceptive role when increased agonist or decreased antagonist and/or timing of the muscles show changes. Our findings demonstrate that bracing did not elicit any changes in the amplitude of these muscle groups. The results however should be looked at cautiously so as to not prejudice bracings’ positive effect moving forward.
Gastrocnemius
Despite the lack of significant changes in quadriceps and hamstring activity between the braced and unbraced condition, only the medial gastrocnemius exhibited significant changes with the brace as evidenced by lower activity during the eccentric (p = 0.006) and concentric (p = 0.028) phases of lunge cycle. Examining the cycle as a whole, decreased activity was evident with the brace (p = 0.01). However, the role the gastrocnemius plays in protecting the ACLD knee is convoluted. Fleming et al. 28 found that the gastrocnemius is able to increase anterior tibial translation. When examining the muscle as an ACL antagonist, decreased activity 29 may perhaps be considered a protective mechanism. Yet others suggest its role primarily as a stabilizer.30,31 In light of the fact that the gastrocnemius may act as an antagonist, perhaps the proprioceptive effect of the brace lowers its activity and thereby improves control. If the muscles’ role is stabilizing, any decrease in activity may be the result of mechanical properties of the brace in providing stability. If it can be confirmed by kinematic studies that anterior tibial translation is lowered as a result of bracing, this theory would be strengthened. The results from a two-dimensional (2D) digital fluoroscopy study showed no differences in anterior tibial translation during lunge exercise when wearing FKBs. 32 Lower gastrocnemius involvement perhaps may lead to reduced medial compartment contact pressure and may help lower the risk of osteoarthritis, with high loads detrimental to joint integrity for those with ACL deficiency. With its origin on the medial femoral condyle, perhaps reduced medial gastrocnemius activity may better guide knee rotation and assist the joint achieve healthier kinematic pattern.
Footnotes
Acknowledgements
The authors would like to thank Prof. J Richards (University of Central Lancashire, Preston, UK), Dr AA Jamshidi (Physical Therapy Department, Rehabilitation Faculty, Iran University of Medical Sciences), Dr A Shakouri Rad (Homaye Salamat Medical Imaging Center), Ms H Nabavi (Ergonomy Lab, University of Social Welfare and Rehabilitation Sciences), Dr Sh Shirvani, and Sports Medicine Federation for their help and support.
Author contribution
Jalali helped with conception and design, acquisition of data, data analysis and interpretation, and drafting and revising the article. Farahmand helped with conception and design, and drafting and revising the article. Rezaeian helped with acquisition of data, and data analysis and interpretation. Ramsey helped with data analysis and interpretation, and drafting and critical revision of the article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency.