
Abstract
Background:
Successful return to sport is an important outcome measure after anterior cruciate ligament (ACL) reconstruction and a reason for patients’ decisions to elect surgery. Rehabilitation programs supervised by physical therapists are routinely prescribed after ACL reconstruction surgery. However, the added advantage of supervised physical therapy after ACL reconstruction is still debatable.
Hypothesis:
Attending more supervised physical therapy sessions after arthroscopic ACL reconstruction in recreational athletes increases their chance of successful return to sport.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors analyzed 93 recreational athletes who underwent arthroscopic ACL reconstruction. After arthroscopic single-bundle ACL reconstruction, patients were advised to attend 20 supervised physical therapy sessions. Patients’ demographics, surgical details, and outcome measures (Knee injury and Osteoarthritis Outcome Score [KOOS], Lysholm scale, and Short Form–36 Health Survey [SF-36]) were recorded presurgery and at 1-year follow-up. Ability to return to sports was documented through patients’ self-report. The attendance at physical therapy by each patient was obtained by examining database records and assessed as fully compliant (>15 sessions), moderately compliant (6-15 sessions), or noncompliant (<6 sessions).
Results:
Patients in the fully compliant group had significantly greater odds (odds ratio [OR], 18.5; 95% CI, 1.9-184.5; P = .013) of a successful return to sport as compared with the noncompliant group. Patients in the moderately compliant group also had greater odds of returning to sport as compared with the noncompliant group (OR, 4.2; 95% CI, 1.0-16.6; P = .043). Patients in the fully compliant group had significantly greater scores on the Lysholm (P < .001), KOOS Sports and Recreation subscale (P = .021), KOOS Symptoms subscale (P = .040), and SF-36 physical component summary (PCS) (P = .012) as compared with the noncompliant group. Moderately compliant patients had significantly greater scores on the Lysholm (P = .004), KOOS Sports and Recreation (P = .026), KOOS Symptoms (P = .041), KOOS Quality of Life (P = .022), and SF-36 PCS (P = .004) as compared with noncompliant patients.
Conclusion:
In recreational athletes, moderate to full compliance with a supervised physical therapy program predicts improved knee function and a greater chance of returning to sport 1 year after ACL reconstruction.
Keywords
Anterior cruciate ligament (ACL) tears are the most commonly reported knee injury in athletes, with nearly 300,000 ACL ruptures and 100,000 ACL reconstructions performed yearly in the United States. 8,22 Despite limited well-designed epidemiological studies in the Asian context, it has been reported that more than 60% of patients who undergo ACL reconstruction are recreational athletes (or sports persons). 19 Supervised physical therapy is routinely prescribed after ACL reconstruction, aiming at restoring motion, improving neuromuscular coordination, and improving quadriceps muscle function and activation. 13 The importance of physical therapy programs in improving knee function has been emphasized in previous studies, 1,3,19 though the competitive advantage of regular supervised physical therapy sessions in comparison with home-based exercises is unclear in empirical research. Studies have demonstrated patients achieved satisfactory outcomes with more home-based rehabilitation and a lesser number of supervised physical therapy sessions. 6,11,14,24 On the other hand, studies have demonstrated that infrequent physical therapy attendance is associated with a poor outcome while extended ambulatory physical therapy leads to improved functional ability and quicker return to work. 16,26
Return to sport is one of the most important outcome measures after ACL reconstruction and an important reason behind patients’ decisions to elect surgery. 21 Return to sport after ACL reconstruction remains challenging for patients, and possibly for the primary care team, due to fear of reinjury and personality and changing perspective in patients after ACL reconstruction. 3,5,12,18,21,22,25,26 A recent meta-analysis by Ardern et al 1 reported return to sport as a primary outcome, highlighting that only 65% of individuals returned to their preinjury level of sports participation and 55% returned to competitive level sports. This study only showed a marginal improvement in these figures compared with an earlier study by Ardern et al. 3 Despite surgery, the rate of returning to sport is not optimal. Understanding the variables that would improve patients’ abilities to return to sport is essential.
Previous studies have assessed the benefit of supervised rehabilitation in terms of self-reported quality of life and functional outcome scores. None have looked at its effect on return to sport. We aimed to assess the association of compliance with physical therapy and returning to sports. Thus, the research questions for this study were the following: (1) Does compliance to a supervised rehabilitation program predict a higher likelihood of successful return to sports? (2) Does compliance to a supervised rehabilitation program predict better functional outcomes?
Methods
Study Design
This was a retrospective research study, utilizing our center’s sports registry database. This study was approved by the local ethical review committee.
Patient Selection
Patients undergoing ACL reconstruction were found through the institute’s registry, and written informed consent was obtained from each patient. Research coordinator nurses, who have been purposefully trained, collected all data at baseline (presurgery) and at 12-month follow-up with the primary care team. Data from 2011 to 2012 were selected to allow at least 1-year follow-up for all patients.
Patients who underwent arthroscopic ACL reconstruction in 2011 and 2012, had postoperative physical therapy in this setup, self-identified as recreational athletes, and completed 12-month follow-up were included in this study. Patients who had previous surgery/fracture of the affected knee, osteoarthritis, inflammatory arthritis, peripheral vascular disease, and significant concomitant injury/surgical procedure (eg, full-thickness chondral damage, meniscal repair, or posterior cruciate ligament or collateral ligament reconstruction/repair) were excluded.
Surgical Intervention
All patients had clinical signs of ACL tear, and magnetic resonance images (MRIs) were used to confirm the clinical diagnosis prior to surgery. Furthermore, patients were evaluated under anesthesia for knee instability. Arthroscopic surgery was performed under general anesthesia in all cases, with administration of prophylactic intravenous antibiotics at induction and for a further 24 hours. Arthroscopic single-bundle ACL reconstruction using autogenous semitendinosus and gracilis tendon grafts was performed using standard portals in all cases. Anteromedial working and anterolateral viewing arthroscopic portals were made. An additional incision was made at the medial proximal tibia for harvesting of the hamstring tendons and transtibial drilling. Femoral drilling was performed via the anteromedial working portal. The femoral and tibial anatomic footprints were used for reconstruction. Suspensory fixation was used on the femoral side, and interference screw fixation was used on the tibial side.
Physical Therapy Intervention
All patients were referred to a postoperative physical therapy program immediately after surgery. Patients were seen in the day surgery ward for full weightbearing (as tolerated) mobilization with axillary crutches and taught home exercises before discharge. Cryotherapy was advocated during the first few postoperative days at home for 20 minutes, 3 to 5 times a day. 27 All patients were advised to attend 20 physical therapy outpatient appointments (once a week for the first 6 weeks [6 sessions], once every 2 weeks for the next 20 weeks [10 sessions], and once every 3 weeks for the next 12 weeks [4 sessions]) over 9 months. Overall, the physical therapy program for a recreational athlete emphasizes early restoration of knee range of motion and quadriceps function, progressive strengthening, neuromuscular training, and return to sport. Additionally, all patients were encouraged to continue exercises in their own gym throughout the physical therapy program.
The physical therapy outpatient program guideline included baseline detailed assessment of the physical and functional parameters and job- and sports-related needs for each patient. Clinic-based treatments targeted full knee extension, maximal knee flexion, and gait retraining in the early phase. Functional electrical stimulation was applied for 20 minutes in the presence of an extension lag of more than 10° during the physical therapy sessions until the lag resolved. 27 Closed kinetic chain quadriceps exercises were initiated after 3 weeks, and open kinetic chain exercises were initiated 4 weeks after surgery. Hip and core muscle exercises were added as part of the program as required. 27 Static cycling was used for flexibility and aerobic training from the third postoperative week. Neuromuscular training was introduced after 1 month. 23 Outdoor cycling and swimming were allowed after 2 months, and outdoor jogging was allowed at 3 months. 27 Agility training was initiated after 4 months, and sports-specific drills were encouraged at 5 to 6 months. At the end of 6 months, patients were allowed to return to sport if there was no/minimal pain and swelling, good quadriceps and hamstring strength (>85% of the unaffected leg), good symmetry on hop tests (>85% of the unaffected leg), and good agility in previous maximum intensity training. 7,23 Treating physical therapists in the setup had at least more than 7 years postqualification experience and further postgraduate training (eg, master’s degree, postgraduate certificate).
Outcome Measures
The number of physical therapy outpatient sessions attended in the first 9 months after arthroscopic ACL reconstruction was collected from the patients’ records as documented by physical therapists. For the purposes of the study, compliance with outpatient physical therapy was defined based on the number of sessions out of a recommended 20 sessions attended by patients in the first 9 months postoperatively. Patients were considered fully compliant if they attended 16 or more sessions (>75% of 20 sessions), moderately compliant if they attended 6 to 15 sessions (25%-75%), and noncompliant if they attended less than 6 sessions (<25%).
Subjects were evaluated at the presurgery assessment and on a routine follow-up at 12 months postoperative using the Lysholm knee score, Knee injury and Osteoarthritis Outcome Score (KOOS), and Short Form–36 Health Survey (SF-36) physical component summary (PCS) and mental component summary (MCS). Ability to return to sport was also documented through patients’ self-report. 4,20
Moreover, the type of sports and frequency of participation as documented at the presurgery assessment in the registry were divided into 3 types in keeping with the Cincinnati sports activity scale 5 : type 1 sports involve jumping, hard pivoting, and cutting activities (eg, basketball, volleyball, football, soccer, gymnastics); type 2 sports include running, twisting, and turning activities (eg, racquet sports, baseball, hockey, skiing, wrestling); and type 3 sports do not involve running, twisting, or jumping (eg, cycling and swimming).
Data Analysis
Descriptive statistics were used for summarizing the patients’ characteristics (age, sex, race, body mass index, surgical site, preinjury types of sports played, and sports activity level), Lysholm knee score, KOOS, SF-36 PCS, and SF-36 MCS. Difference in the means of the demographics and other secondary outcomes in the 3 compliance groups were tested using 1-way analysis of variance with Bonferroni correction to control for the inflated type I error resulting from multiple comparisons. For difference in portions, a chi-square test was utilized when needed. Bivariate correlations were tested using Pearson correlations for the continuous dependent variables. Logistic regression adjusting for baseline patients’ characteristics and scores was performed to analyze the predictors of successful return to sport and better functional outcomes. Statistical analyses were performed using SPSS version 22 (IBM Corp), and significance was set at P < .05.
Results
A total of 239 patients’ records from the registry in 2011 and 2012 were screened in keeping with the study selection criteria to include 93 patients in this study (Figure 1 and Table 1). At the presurgery assessment, patients’ characteristics (age, sex, race, body mass index [BMI], site of operation, preinjury type of sports, and sports activity level) and presurgery outcome scores (Lysholm, PCS, MCS, and all KOOS subscale scores: Symptoms, Pain, Activities of Daily Living [ADL], Sports and Recreation [Sport/Rec], and Quality of Life [QoL]) were not significantly different among noncompliant, moderately compliant, and fully compliant outpatient physical therapy session groups, indicating that the groups were well matched.

Patient selection.
Patient Characteristics at Presurgery Assessment a
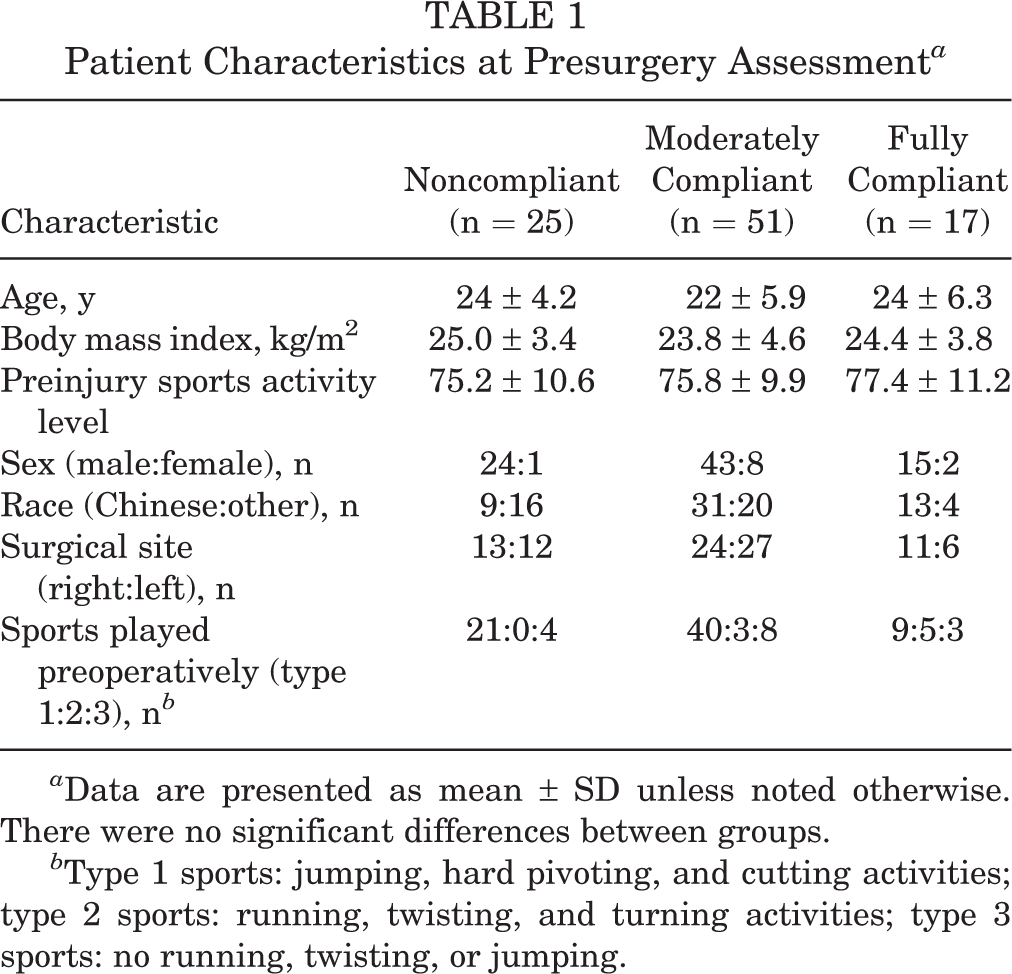
a Data are presented as mean ± SD unless noted otherwise. There were no significant differences between groups.
b Type 1 sports: jumping, hard pivoting, and cutting activities; type 2 sports: running, twisting, and turning activities; type 3 sports: no running, twisting, or jumping.
Outcome Scores
Patients in the noncompliant group attended on average 3.6 (range, 1-5) sessions, in the moderately compliant group attended on average 10.7 (range, 6-15) sessions, and in the fully compliant group attended on average 17.1 (range, 16-19) outpatient physical therapy sessions. All the participants were given the same regular physical therapy sessions but some elected not to attend regularly on their own accord. None of these patients had any postoperative complications that necessitated revision surgery within 1 year. The differences in functional outcome scores across the 3 groups are summarized in Table 2. There was significant improvement in all outcome scores at 1 year postsurgery compared with presurgery in all 3 groups (Table 2).
Outcome Measures at Presurgery Assessment and at 1-Year Follow-up a
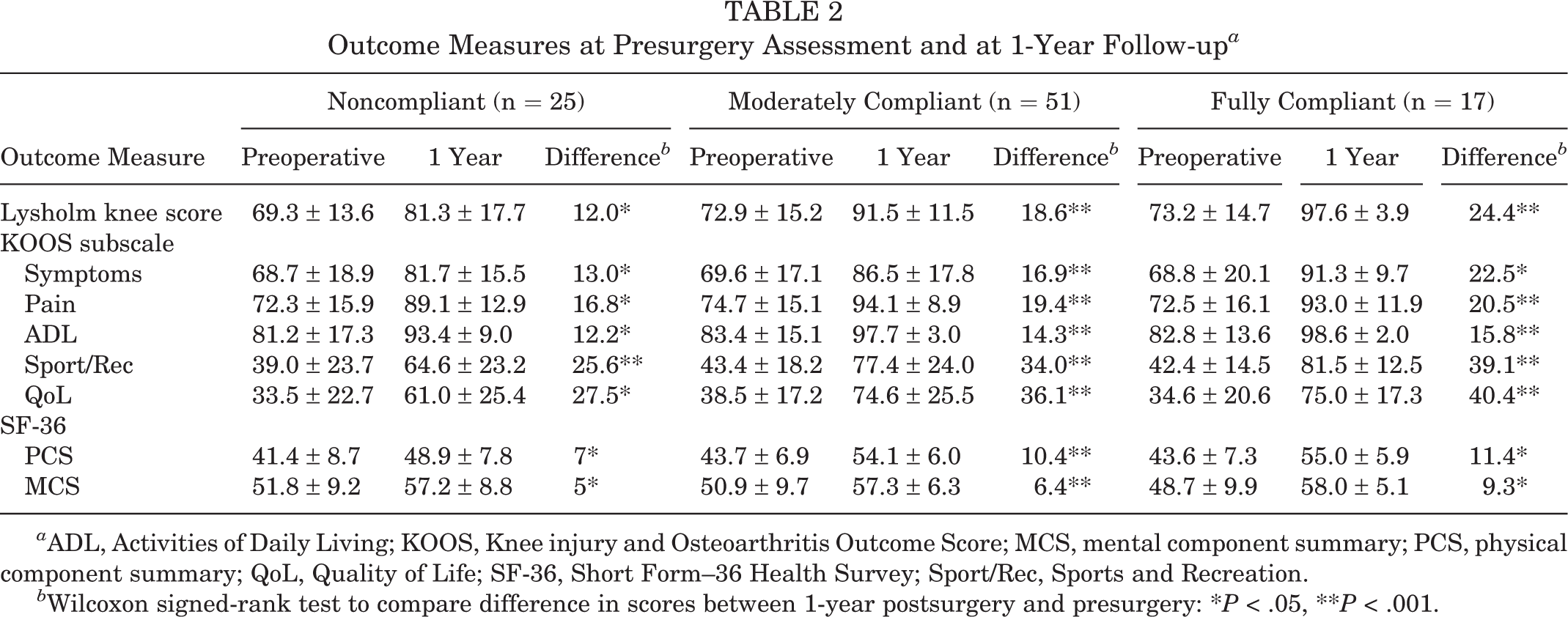
a ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MCS, mental component summary; PCS, physical component summary; QoL, Quality of Life; SF-36, Short Form–36 Health Survey; Sport/Rec, Sports and Recreation.
b Wilcoxon signed-rank test to compare difference in scores between 1-year postsurgery and presurgery: *P < .05, **P < .001.
There were no significant correlations regarding age and preoperative sports activity level for Lysholm knee score, all KOOS subscales, SF-36 PCS, and SF-36 MCS at 1 year postsurgery. There were no significant differences in the outcome scores between different sexes, races, sites of operation, or preinjury types of sports. Patients who underwent more physical therapy sessions were correlated with better scores on the Lysholm (r = 0.226, P = .029) and KOOS ADL subscale (r = 0.214, P = .040), but not the PCS (r = 0.126, P = .229) or MCS (r = –0.026, P = .808) or the KOOS Symptoms (r = 0.121, P = .247), Pain (r = 0.132, P = .208), Sport/Rec (r = 0.158, P = .132), or QoL subscales (r = 0.084, P = .422).
The mean differences in the outcome scores between the 3 groups for compliance to physical therapy are summarized in Table 3. Regression analysis adjusting for baseline patients’ characteristics and scores confirmed that patients in the fully compliant group had significantly higher scores on the Lysholm (P < .001), KOOS Sport/Rec (P = .021), KOOS Symptoms (P = .040), and SF-36 PCS (P = .012) as compared with noncompliant patients. Moderately compliant patients had significantly higher scores on the Lysholm (P = .004), KOOS Sport/Rec (P = .026), KOOS Symptoms (P = .041), KOOS QoL (P = .022), and SF-36 PCS (P = .004) as compared with noncompliant patients. There were no significant differences in the Lysholm knee score, all KOOS subscales, and SF-36 PCS or MCS between the fully compliant and moderately compliant groups.
Mean Differences in Outcome Scores at 1-Year Follow-up in the 3 Groups a

a ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MCS, mental component summary; PCS, physical component summary; QoL, Quality of Life; SF-36, Short Form–36 Health Survey; Sport/Rec, Sports and Recreation. Significant difference: *P < .05, **P < .001.
Return to Sport
Sixty-two (66.7%) subjects could return to their preinjury level of sports. There were no significant correlations for age, BMI, or preinjury sports activity level to successful return to sport. There were no significant differences regarding successful return to sport between different sexes, races, sites of operation, or preinjury types of sports.
Compliance to physical therapy was a significant factor in determining the ability to return to sport. Regression analysis adjusting for baseline patients’ characteristics and scores confirmed that patients in the fully compliant group had significantly greater odds (odds ratio [OR], 18.5; 95% CI, 1.9-184.5; P = .013) of return to sport as compared with those in the noncompliant group. Patients in the moderately compliant cohort also had greater odds (OR, 4.2; 95% CI, 1.0-16.6; P = .043) of returning to sport as compared with those in the noncompliant group.
There were no significant differences in outcomes scores between patients who participated in jumping, pivoting, and cutting activities in type 1 sports versus patients who did not (type 2 and 3 sports). However, the type of sports affected the chance of successful return to sport. Patients who participated in sports that did not require jumping, hard pivoting, and cutting activities had a greater chance of successfully returning to preinjury sports (87.0%) as compared with patients who participated (61.4%) in jumping, hard pivoting, and cutting activities, although these results were not statistically significant (P = .076).
Higher Lysholm knee score, all KOOS subscales, and SF-36 PCS were associated with a greater success rate of returning to sport (Table 4).
Association of Outcomes Scores With Successful Return to Sport a

a Data are reported as percentages. ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MCS, mental component summary; PCS, physical component summary; QoL, Quality of Life; SF-36, Short Form–36 Health Survey; Sport/Rec, Sports and Recreation.
Discussion
The results of this retrospective study indicate that compliance with a supervised rehabilitation program predicts a greater likelihood of successful return to sports and better functional outcome scores. This correlation could be the result of physical therapy leading to quicker return of strength, range of motion, stability, and neuromuscular function. Compliant patients may be more driven to regain function and return to sports, hence putting in more effort to participate in both supervised and home physical therapy. Poorly compliant patients may not put in effort in supervised physical therapy as well as a home/gym program and may also have possible psychological or social factors that affect outcomes.
A systematic review and meta-analysis done in 2014 1 showed that 81% of patients post–ACL reconstruction returned to any sport, while 65% attained their preinjury level of competition. Only 55% returned to competitive level sport after surgery. Even though the rate of return to sport was low, 90% of patients achieved near normal knee function postsurgery. 3 The low percentage of patients returning to their preinjury level of sport prompted researchers to analyze the variables influencing this factor, with fear of movement and reinjury (or kinesiophobia) 3,10,17 –20 as frequently cited reasons in 20% to 24% of patients. 18,19 Other variables include impaired knee function, 10,18 instability, 19,20 pain, 17,20 social reasons, 19 low self-motivation, 18 effusion, 20 muscle weakness, 10,20 and knee extension deficit. 17 Despite attributes such as impaired knee function, instability, muscle weakness, and knee extension deficit, which can potentially be improved by supervised physical therapy, several studies have demonstrated patients achieving satisfactory outcomes with fewer physical therapy sessions and with the lessened physical therapy supervision of exercise programs. 6,11,14,24
The review by Treacy et al 26 of 39 patients demonstrated that infrequent physical therapy attendance was associated with poorer outcomes in terms of Lysholm knee score, poorer patient satisfaction, and a delayed return to previous activity level. They recommended a general reduction in the number of physical therapy visits but concluded that a certain level of supervision was still necessary. This recommendation was included in our study: Athletes only need to complete 20 sessions of physical therapy. This appears to be an optimal number, as extensive supervised rehabilitation does not necessarily confer better outcomes and might not be cost- and time-effective, as shown in the previous study. 26 That study showed that athletes compliant with 60 visits over 6 months did not perform significantly better than those who were moderately compliant with 5 to 24 sessions over 6 months. Our protocol of having a supervised program of 16 to 20 sessions (fully compliant) or 6 to 15 sessions (moderately compliant) over 9 months has shown satisfactory results in terms of outcome scores as well as return to sport. It may be that 10 supervised therapy sessions are as effective as 20, with a 50% reduction in cost.
Frosch et al 16 emphasized the importance of compliance to physical therapy. Their study of 35 patients after ACL reconstruction showed that as compared with patients treated with regular physical therapy (2-3 times per week for 30 minutes), patients who had undergone an extended ambulatory physical therapy program (3-5 times per week for 2.5 hours) gained a significantly greater degree of functionality in the Lysholm knee and Tegner scores and displayed better results in the proprioceptive capability test and KT-1000 ventral tibial stability. Importantly, functional improvement was correlated with earlier return to work activities.
In our study on recreational athletes, patients with higher SF-36 PCS, Lysholm knee score, and KOOS subscales had an increased chance of returning to their preinjury sporting activity. These findings support the notion by Ericsson et al 12 that patients need to achieve a sufficient level of physical functioning to enable optimal performance of sport-specific tasks. Kinesiophobia, which is an important factor determining successful return to sport, 2 has also been shown to decline during rehabilitation. 9 Current literature suggests that factors other than knee function such as fear of reinjury, kinesiophobia, shifts in priority, and individual personalities will affect chances of returning to sport. 3,5,12,18,21,22,25,26 These studies involved an unknown mixture of competitive as well as recreational athletes. Kinesiophobia and fear of reinjury could be more important in competitive athletes as a higher level of aggressiveness and neglect of safety during training as well as competition could be involved, predisposing to higher risk profiles for injury. The results in our study seem to suggest that recreational athletes who do not participate in competitive sports tend to be able to return to preinjury sports once they have achieved an adequate level of knee function.
In contrast to our present study, Feller et al 14 found that patients who chose to attend physical therapy on a very limited basis after ACL reconstruction could achieve satisfactory if not better outcomes than patients who attended physical therapy regularly. Noncompliant patients in our study had poorer SF-36 PCS, Lysholm knee score, and KOOS scores and significantly less likelihood of returning to preinjury sporting activity as compared with patients who were moderately or fully compliant. The findings of the study by Feller et al 14 could be clearly interpreted if the details about the surgical technique and the types of implants used, which may cause said difference, were reported. In relation to this argument, all surgeries in the present study were performed via anatomic ACL reconstruction using autogenous hamstring tendon grafts, limiting surgical factor as a potential source of bias. It was also noted that there were only 10 patients in the minimal attendance group that were matched with 10 patients from the regular physical therapy group. During critical interpretation, lack of adequate sample size is always a concern about the robustness of any pilot study findings.
Schenck et al 24 compared 2 rehabilitation programs (clinic-based with an average clinic visit of 14.2 vs physical therapist–directed home-based with an average visit of 2.85) after a mid-third patellar autograft reconstruction of the ACL. There were no differences in functional or subjective outcomes in the different postoperative rehabilitation regimens. Interpreting the results of Schenck et al 24 and the current study suggest that patients need to be trained and guided by physical therapists in the clinic on the exercise regimen before patients can get optimal results from their home therapy. Better outcomes could be obtained in patients with home-based therapy if they were guided, compliant, and determined. In our study population, the subjects were all recreational athletes. Although they were encouraged to continue the exercises in their own gym throughout the physical therapy program, compliance with home-based exercise was not determined.
Furthermore, our results suggest that patients who participated in sports that did not require jumping, hard pivoting, and cutting activities had a greater chance of successfully returning to preinjury sports (87.0%) as compared with patients who participated (61.4%) in jumping, hard pivoting, and cutting activities, although the results were not statistically significant (P = .076). This may be due to less fear of reinjury as compared with sports that require pivoting and cutting maneuvers.
Contextual factors such as sex, age, and preinjury sports are nonmodifiable. Other than psychological factors, postsurgery rehabilitation is probably the most important modifiable factor that can be addressed to achieve greater postsurgery function as well as successful return to sport. 27 Modifiable factors such as neuromuscular strength and proprioception that have been associated with return to sport should be identified and acted on. 19,20 Our study indicates that moderate to full compliance with an evidence-based, structured, and supervised physical therapy program significantly improves knee function and increases the rate of return to preinjury sporting activity. Patients should therefore be actively counseled to comply with their postoperative physical therapy program.
The strengths of this study include the fact that all patients were followed up with and the outcomes studied by investigators who were not directly involved in the initial management of the patients, which minimizes risk of bias. We have excluded confounding factors that may affect the outcomes of surgery, such as the presence of meniscus surgery, graft type, fixation, and other surgical techniques. As the study patients had their surgery done using hamstring tendon autogenous grafts, risk of bias due to graft choice was minimized. 1 The patient group consisted only of recreational athletes, which was believed to create a more homogenous cohort by reducing potential differences in patients’ motivation levels and postsurgical expectations.
The major limitation of this study is its retrospective design. It also did not capture the frequency and intensity of home exercises, which could have influenced the findings. Indeed compliance with physical therapy visits could reflect the underlying motivation to participate in the rehabilitation process, which may be more important than supervision by a physical therapist.
We also did not specifically assess patients’ fear of reinjury. Again, due to the retrospective design, randomization was not used, and this may have increased the risk of bias in the results. Although patients were followed for 1 year regarding successful return to sport, the results could be more robust with a longer follow-up of up to 2 years. The noncompliant group of patients may have just been slow to return to sport, and outcome measures may have continued to improve with more time. However, clinical guidelines suggest that patients should be expected to return to sport by 9 months postsurgery. 4 Furthermore, a recent randomized clinical trial has found no difference in knee function, health status, and rate of return to preinjury activity level/sport between the second and fifth year of follow-up after ACL reconstruction. 15
The authors advocate for a prospective randomized study to be performed to address some limitations in this study. Future research may be done to assess the optimal number of physical therapy sessions, the effect of compliance with physical therapy on longer term outcome, and the facilitation of home-based rehabilitation with Internet-based tele-rehabilitation.
Conclusion
Increased compliance with a well-designed, progressive, and supervised physical therapy program improves knee function and correlates with a greater chance of return to sport in recreational athletes after arthroscopic ACL reconstruction with autogenous hamstring graft. Future research on physical therapy compliance after ACL reconstruction should investigate the similar question in a rigorous prospective study with adequate sample size and 2-year follow-up.
Footnotes
Acknowledgment
The authors thank Miss Toh Shi Jie (research coordinator), Miss Rajar Rajaswari (therapy assistant), and Mr Chinnasamy Duraimurugan (principal physical therapist and workgroup leader, Sports Centre) and their teams for assistance with this study.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.