
Abstract
Background:
Several procedures for combined rupture of both anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) in multiple-ligament knee injuries (MLKIs) have been reported. However, the clinical outcome of these treatments remains controversial.
Hypothesis:
Postoperative knee stability and clinical outcomes in patients who underwent simultaneous bicruciate reconstruction would be comparable with those that underwent bicruciate reconstruction with collateral ligament surgery.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective study was conducted with 41 patients (41 knees) who sustained unilateral MLKI with combined ACL and PCL rupture. Fifteen cases required simultaneous ACL and PCL reconstruction, and the others had additional surgical treatment as follows: At the time of cruciate ligament reconstruction, 14 cases required posteromedial corner (PMC) reconstruction and 8 cases required posterolateral corner (PLC) reconstruction. Five cases were treated with an initial PMC or PLC before the cruciate ligament reconstruction. One of these underwent PMC reconstruction at the second stage for residual valgus laxity. Then, the authors divided the cases into 2 groups based on surgical procedure: in group 1, 15 patients underwent only bicruciate reconstruction. In group 2, 26 patients underwent bicruciate and PMC or PLC reconstruction/repair. The patients were examined at ≥2 years after surgery.
Results:
The side-to-side difference in the total anteroposterior translation, and the relative position on the anterior and posterior stress radiographs significantly improved postoperatively in both groups (group 1: P = .0115, P = .0007; group 2: P = .0004, P < .0001). In the valgus and varus stress tests, the medial and lateral joint opening significantly improved postoperatively in group 2 (P < .0001; P = .0093). Anterior, posterior, valgus, and varus stress radiographs showed no significant differences in comparison with that in the uninjured knee. There were no significant differences in the postoperative anteroposterior laxity and the medial and lateral joint opening between the groups. The Lysholm score, the International Knee Documentation Committee evaluation, all subscales of the Knee injury and Osteoarthritis Outcome Score, the Tegner score, and the isokinetic peak torque of quadriceps and hamstring muscles significantly improved postoperatively in both groups (P < .0003). Each clinical parameter did not differ between the 2 groups.
Conclusion:
There were no significant differences in the knee stability and clinical results after bicruciate reconstruction between those with and those without collateral ligament surgery. Reconstruction of bicruciate MLKIs with repair or reconstruction of associated collateral ligament injuries improves clinical outcomes.
Multiple-ligament knee (MLK) injuries (MLKIs) and knee dislocations are severe traumas that involve intra- and extra-articular ligament tears, often with concomitant vascular and nerve injuries and a fracture around the knee. MLKIs, however, are uncommon, which means that minimal evidence is available, resulting in a lack of consensus regarding the most effective treatment. 4 In particular, MLKIs with both anterior and posterior cruciate ligament (ACL and PCL) tears often result in significant functional disability and require surgical treatment.9,49 Although nonsurgical and surgical treatments have been reported in MLKIs, surgical interventions have generally been recommended because of poor outcomes after nonsurgical treatment.27,40
With advancements in arthroscopic reconstructive surgery, recent studies have reported the effectiveness and safety of reconstruction of both cruciate ligaments.11,25,34,36,61 However, controversies remain, including knee stability and clinical outcomes when there are associated collateral ligament injuries because the achievement of normal laxity and normal range of knee motion is often difficult to obtain.
It is well known that combined lesions in MLKIs cause severe functional impairment. 15 Biomechanical studies have established that injuries to the posterolateral corner (PLC) of the knee worsen the deleterious effects of tears in one or both cruciate ligaments. 51 Race and Amis 48 reported that the PLC injury promote the functional disability of the PCL insufficiency. Harner et al 19 also reported that the PLC deficiency provides high forces to the PCL, which may cause an elongation of a PCL graft. Barrett et al 1 showed that for MLKIs requiring a medial collateral ligament (MCL) reconstruction, the outcomes were significantly worse for those with higher Schenck classification grade.53,62 King et al 30 and Tardy et al 58 compared MLKIs in patients with PLC or posteromedial corner (PMC) injuries and no difference in functional results after surgery was shown. Previous studies reporting on clinical outcomes after bicruciate and PMC or PLC reconstruction continue to vary widely, with patients often experiencing chronic pain, stiffness, loss of range of knee motion, instability, and failure to return to work or sports.11,60
Based on the previous studies, the purpose of the present study is to evaluate the clinical results of MLKI after undergoing simultaneous ACL and PCL reconstruction with an associated collateral ligament repair/reconstruction when needed. We have proposed the following hypothesis: postoperative knee stability and clinical outcomes in patients who underwent simultaneous bicruciate reconstruction would be comparable with those that underwent bicruciate reconstruction with collateral ligament surgery.
Methods
Study Design
A retrospective study was conducted in patients who underwent both ACL and PCL reconstruction for unilateral MLKI between 2010 and 2020 at the Hokkaido University hospital. According to anatomic MLKI classification, 47 MLK 2 (complete tears of the ACL and PCL without injury to the superficial MCL [sMCL], PMC, lateral collateral ligament [LCL] or PLC) and MLK 3 (complete tears of the ACL and PCL with complete tear of the sMCL and/or PMC or the LCL and/or PLC) were enrolled in this study. The MLKI classification based on the injury patterns described by Schenck in the knee dislocation classification53,62 was assigned on the basis of all ligaments that had a grade III (complete) tear or were deemed clinically incompetent and required surgical repair or reconstruction. Surgical strategy for combined rupture of both ACL and PCL in MLKI was as follows 20 : in the acute cases (<3 weeks after injury), we performed repair of the grade III PMC or PLC injuries in the first stage. 24 Simultaneous ACL and PCL reconstructions were performed in the second stage. 70 In the chronic cases (≥3 weeks after injury), we performed a single-stage ACL and PCL reconstruction and/or collateral ligament reconstruction.32,34 Two senior orthopaedic surgeons (K.Y. and E.K.), who were sufficiently trained concerning this surgery, performed all operations using the same procedure. After surgery, all patients underwent postoperative management using the same rehabilitation protocol as reported previously.20,70 To test the study hypotheses, we divided the patients into 2 groups: (1) group 1, in which only bicruciate reconstruction was performed after injury; and (2) group 2, in which bicruciate reconstruction with PMC or PLC reconstruction/repair was carried out. All the patients were clinically and radiologically evaluated at ≥2 years after surgery. This retrospective study design using patient data was approved by the institutional review board of the hospital and all patients provided informed consent.
Patient Demographics
All 44 initial consecutive patients (44 knees) who sustained unilateral MLKI with both ACL and PCL tears (anatomic MLKI classification 47 ; MLK 2 or MLK 3) were enrolled in this study. The diagnosis of injured ligaments was made based on a detailed history of the knee injury, a physical examination of pathological status and abnormal laxity, routinely performed plain radiographs, magnetic resonance imaging (MRI) scans, computed tomography (CT), and findings at the time of surgery. Patients with any previous surgery for ligamentous injuries, a concurrent fracture, or osteoarthritis (Kellgren and Lawrence classification > grade 2) were excluded. Three patients (group 1, n = 1; group 2, n = 2) were lost to follow-up and thus excluded from analysis.
Ultimately, 41 patients (37 men and 4 women), with a mean age of 31.1 years (range, 16-60 years), were registered for evaluation (Table 1). In groups 1 and 2, there were 15 and 26 patients, respectively. Seven patients in group 1 sustained a collateral ligament injury (6 sMCL injuries and 1 PLC injury) (≤ grade II) that healed with nonoperative treatment before the bicruciate reconstruction. The mean interval from the time of injury to surgery was 7.4 months (range, 3-22 months) in group 1 and 7.7 months (0-23 months) in group 2. The mean follow-up period was 31.8 months (range, 24-42 months). The cause of injury included 22 sports-related injuries, 12 motor vehicle accidents, and 7 work-related injuries.
Patient Characteristics a

Data are reported as mean ± SD unless otherwise indicated. ACL, anterior cruciate ligament; BMI, body mass index; DB, double bundle; N/A, not available; PCL, posterior cruciate ligament; PLC, posterolateral corner; PMC, posteromedial corner; SB, single bundle.
There were 41 injured knees in total, 5 were acute cases and 36 were chronic cases. In the acute cases, 4 knees required PMC repair, and 1 required PLC repair at the first stage surgery in group 2.2,25 We performed simultaneous ACL and PCL reconstructions at the second stage. One knee that underwent an initial PMC repair had residual valgus laxity and underwent PMC reconstruction at the time of the bicruciate reconstruction. In the chronic cases of the 36 knees, 15 knees underwent combined ACL and PCL reconstruction, 13 knees underwent combined ACL, PCL, and PMC reconstruction, and 8 knees underwent combined ACL, PCL, and PLC reconstruction at the time of surgery (Table 1). Preoperatively, complete peroneal nerve palsy was identified in 1 patient and 2 patients in groups 1 and 2, respectively.
Preoperative Examination
After administration, radiographic evaluations, including MRI and CT were performed as soon as possible to determine surgical strategies (Figures 1 and 2). Manual reduction was performed if the patient showed knee dislocation. Then, anterior, posterior, valgus, and varus instability tests were performed under stress radiograph in the radiation room. CT angiography was performed if the patient showed any suspected signs of popliteal arterial injury.

Step-by-step preoperative examination using plain radiographs, stress radiograph, magnetic resonance imaging (MRI), and computed tomography (CT) angiography for a 21-year-old male patient who suffered right knee dislocation injuries caused by a traffic accident. (A, B) Plain radiographs showing the knee dislocation. (C) Stress radiograph showing grade III varus instability of the knee. (D) Coronal MRI showing the posterolateral structure injury and the dislocation of the lateral meniscus (yellow arrow). (E) Sagittal MRI showing anterior cruciate ligament and posterior cruciate ligament injuries (yellow arrow). (F) Angio-CT revealing the continuity of the popliteal artery.

Manual evaluation under anesthesia for the 21-year-old male patient. (A) Hyperextension of the knee. (B) Anterior instability of the knee at 90° of knee flexion. (C) Posterior instability of the knee at 90° of knee flexion. (D) Varus instability of the knee at 0° of knee extension.
Surgical Procedure
Each patient underwent diagnostic arthroscopy immediately before knee surgery. Diagnostic arthroscopy was performed with standard anterolateral (AL) and anteromedial (AM) parapatellar portals to confirm that there was ACL and PCL injury. Meniscal lesions and avulsion fractures were treated arthroscopically if observed.
Acute Primary Repair
In the acute cases, patients were treated by 2-stage procedures. In the first stage, we performed a repair of the PMC or PLC within 3 weeks of injury after swelling had subsided. Surgical management was based on preoperative findings of varus and valgus manual stress radiographs with the patient under anesthesia. An examination under anesthesia was performed by using the contralateral knee as the control. The collateral ligament injuries were graded on valgus or varus laxity to manual stress at 30° of knee flexion. 22 A grade III stress test indicated >10 mm of opening on the medial or lateral side of the joint. Primary repair of the PMC or the PLC was performed. The patient was placed in a supine position on the operating table under general anesthesia. A pneumatic tourniquet was applied to the proximal thigh. Through a medial or lateral longitudinal curved skin incision, damaged structures were carefully identified. Concerning the PMC injury, damage to the deep MCL, the sMCL, the posterior oblique ligament (POL), the medial head of the gastrocnemius, and the medial joint capsule were identified and repaired using a suture anchor (JuggerKnot soft anchor system; Zimmer Biomet) and pullout sutures. If there was a bony fragment attached to the ligament, polyethylene sutures were passed through the ligament and bone fragment, and the fragment was secured by passing the sutures through a single tunnel at the ligament attachment site. Regarding the PLC injury, damages to the LCL, the popliteal tendon, the popliteofibular ligament, the biceps femoris tendon, the lateral head of the gastrocnemius, and the lateral joint capsule were identified and repaired using a suture anchor and pullout sutures (Figure 3). For patients with peroneal nerve palsy, an initial neurolysis was performed, followed by primary repairs of extra-articular ligaments.

Primary repair of the PLC complex for the 21-year-old male patient. (A) Lateral curved skin incision. There is complete rupture of the iliotibial band. (B) Avulsion fracture of the distal attachment of the lateral collateral ligament, popliteofibular ligament, and biceps tendon complex (yellow arrow). The peroneal nerve was identified (white arrow). (C) The lateral meniscus was sutured following reduction (white arrow). (D) Suture anchors were fixed to the fibular head (white arrow). (E) The posterolateral corner is fixed by suture anchors.
Postoperative Management After Primary Repair
Postoperative management after this first stage of surgery included immobilization using a soft knee brace at 10° of flexion in a position that prevented posterior subluxation for 2 to 4 weeks. Patients began isometric muscle-strengthening exercises, such as patellar setting and straight-leg raising, the day after surgery. Range of motion (ROM) exercises using continuous passive motion devices were commenced at the beginning of the second to third postoperative week. 8 Partial weightbearing with a hinged knee brace was then allowed 4 weeks after surgery. Full weightbearing was permitted 6 weeks after surgery. Once full ROM was obtained, the patients were surgically treated by a second-stage operation.
Staged Reconstruction
In the second stage, simultaneous single-bundle (SB) or double-bundle (DB) ACL and SB or DB PCL reconstructions were performed. If the harvest semitendinosus tendon was of insufficient thickness (<6 mm doubled) or length (<240 mm), an SB reconstruction was performed. The details of this procedure have been previously described in the literature.20,70,71 For ACL and PCL reconstruction, the semitendinosus and gracilis tendons of the ipsilateral and contralateral knees were harvested using a tendon stripper. For SB ACL graft preparation, the semitendinosus tendon was doubled with side-by-side sutures, and the thickest portion of the gracilis tendon was also doubled (4 strands). For DB ACL graft, the semitendinosus tendon was cut into 2 parts. The distal half of the semitendinosus tendon was doubled (2 strands) with side-by-side sutures and used for the AM bundle graft, and the remaining proximal half of the semitendinosus tendon was also doubled (2 strands) and used for the posterolateral (PL) bundle graft. Both the free ends were firmly sutured side by side at 3 different sections, using the circumferential ligation technique with 2-0 polyester threads (WAYOLAX, Matsudaika). 71 A commercially available polyester tape (Leeds-Keio Artificial Ligament; Neoligament) was then rigidly connected with 2-0 polyester threads (WAYOLAX) in series with the sutured end, using the original “hybrid” technique.72,73 An Endobutton CL-BTB (Smith & Nephew Endoscopy) was attached at the looped end. The tendons were fashioned having a length ≥60 mm. The graft diameter was, respectively, 7 mm and 6 mm in AM and PL bundle ACL graft and 8 to 10 mm in SB ACL graft (Figure 4). Another pair of tendons was used for PCL reconstruction, and the graft was prepared in a similar manner to a length of ≥70 mm. Polyester tapes were passed around each end of the tendon loop and rigidly connected with No. 2 polyester threads. 33 The graft diameter was, respectively, 8 mm and 7 mm in AL and posteromedial (PM) bundle PCL graft and 9 to 11 mm in SB PCL graft (Figure 4).

Autologous tendon grafts. (A) Bone–patellar tendon–bone graft. (B) Single-bundle (SB) anterior cruciate ligament (ACL) graft. (C) Double-bundle (DB) ACL graft. (D) SB posterior cruciate ligament (PCL) graft. (E) DB PCL graft. (F) Superficial medial collateral ligament graft.
In ACL reconstruction, appropriately sized ACL femoral and tibial tunnels were created using a commercially available guide (Wire-navigator; Smith & Nephew). 71 The ACL femoral tunnels were created using a transtibial technique employing an offset guide (Transtibial Femoral ACL Drill Guide; Arthrex).
PCL reconstruction was performed using the outside-in technique. 20 The tibial tunnel of the PCL was created using a hole-in-1 guide (ACUFEX Director PCL Tibial Aimer; Smith & Nephew Endoscopy) under fluoroscopy. We used 2 tibial tunnels for the DB technique. A guidewire was inserted from the point approximately 2 cm distal to the ACL tibial tunnel on the proximal tibia to the tibial attachment of the PCL. Then, the guidewire was over-reamed to the measured graft size. The SB femoral tunnel was created at the center of the AL bundle attachment using an outside-in guide (ACUFEX Director PCL Femoral Aimer; Smith & Nephew Endoscopy) through a small incision made over the medial femoral condyle. DB femoral tunnels were created at the centers of the AL and PM bundle attachments. A guidewire was inserted into the femoral attachment of the PCL. The guidewire was then over-reamed with a cannulated reamer to the measured graft size. Regarding graft placement, the PCL grafts were fixed using the Leeds-Keio ligament stapled on the femoral and tibial sides. The ACL grafts were fixed on the femoral side using the Endobutton CL-BTB (Smith & Nephew) and using the Leeds-Keio ligament stapled on the tibial side (Figure 5). First, the PCL graft was tensioned manually at 90° of knee flexion by applying an anterior drawer force to the tibia to obtain an anatomic position. The Surgeon should conform a reduction of tibial sagging. Second, the 60-N force was applied to the ACL graft using the tension meter. The relative position between the femur and the tibia in the lateral view was intraoperatively evaluated using fluoroscopy. When the position was found to be abnormal, the position was corrected to the normal one (contralateral side) by increasing or decreasing the applied tensions to the ACL and PCL grafts. Finally, keeping the tension value on the grafts, the knee was positioned at 10° of knee flexion. A surgeon (E.K.) simultaneously secured all grafts to the medial aspect of the proximal tibia with 2 spiked staples using the turnbuckle stapling technique.
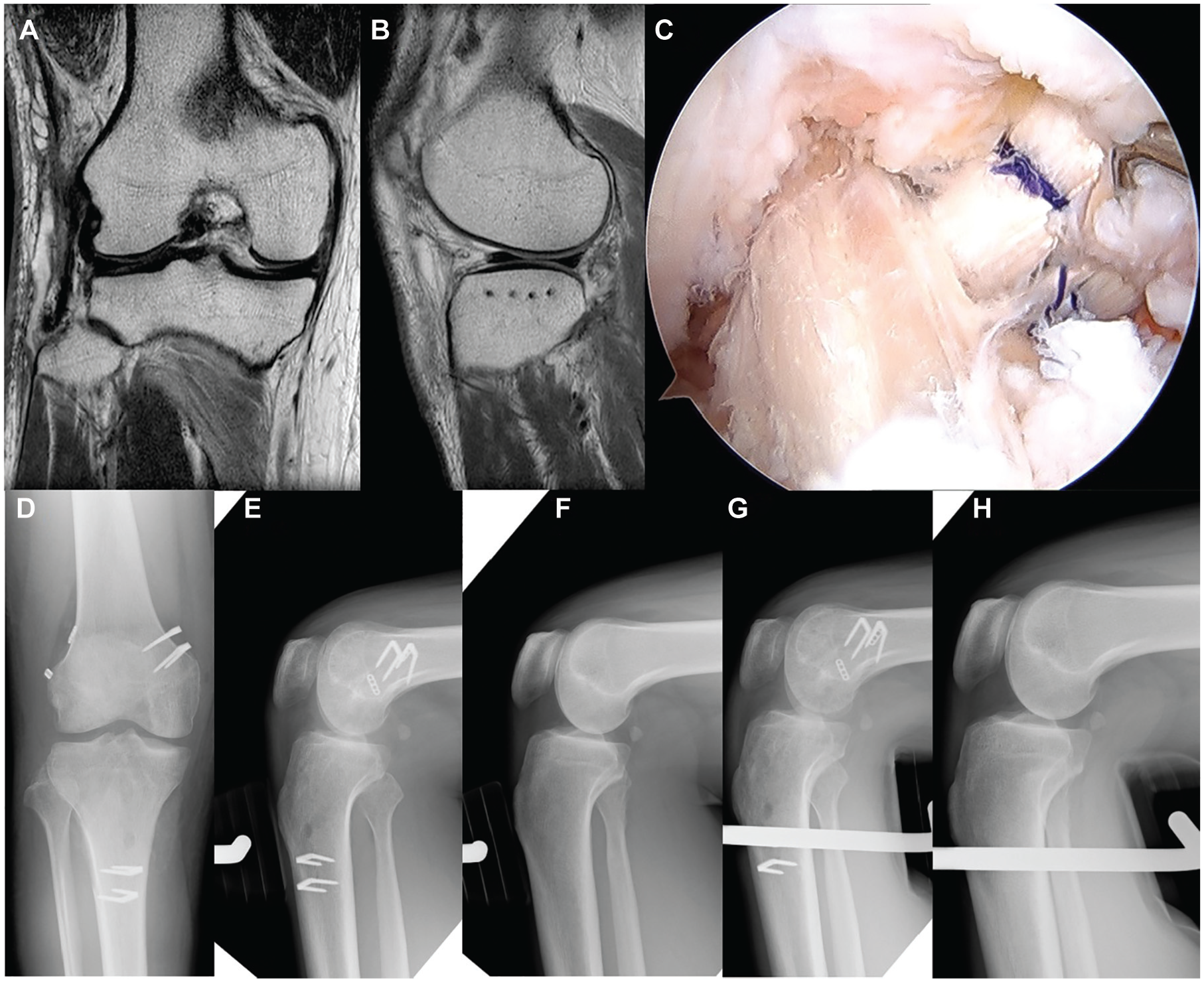
Double-bundle anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) reconstruction after primary repair of the posterolateral corner (PLC) for the 21-year-old male patient. (A, B) Magnetic resonance imaging showing the healing of the PLC complex and lateral meniscus. (C) Arthroscopic view of double-bundle ACL and PCL reconstruction of the hamstring tendon grafts. (D) Postoperative anteroposterior radiograph. (E, F) Lateral stress radiograph of the affected and unaffected knees with an applied posterior drawer force of 134 N. (G, H) Lateral stress radiograph of the affected and unaffected knees with an applied anterior drawer force of 133 N.
Chronic Stage Reconstruction
In the chronic cases, patients with grade III instability had their injured ligaments reconstructed simultaneously. ACL and PCL were reconstructed in the same manner described above. We selected an appropriate ipsilateral or contralateral autogenous tendon graft from the semitendinosus and gracilis tendons, the bone–patellar tendon–bone (BTB), or the biceps femoris tendon for each of the injured ligament (Table 2).
Graft Choice in Chronic Stage Reconstruction a

ACL, anterior cruciate ligament; BTB, bone–patellar tendon–bone; PCL, posterior cruciate ligament; PLC, posterolateral corner; PMC, posteromedial corner; ST, semitendinosus tendon; STG, semitendinosus and gracilis tendons; N/A, not available.
PMC Reconstruction
In the knee with ACL/PCL/PMC reconstruction, we harvested a BTB graft from the ipsilateral knee in addition to the hamstring tendon harvest described above (Figure 4 and Table 2). Then, a BTB graft was used for ACL reconstruction and hamstring tendon grafts were used for PMC and PCL reconstructions (Table 2). After all tunnels for bicruciate ligament reconstruction were created, we made 2 tunnels for PMC reconstruction before implanting the grafts for cruciate ligament reconstruction.
PMC reconstruction was performed using the previously reported sMCL reconstruction. 32 To fashion a doubled semitendinosus tendon graft for PMC reconstruction, we used the previously reported hybrid technique. Briefly, the semitendinosus tendon was doubled. Then, polyester tape was passed through the tendon loop. An Endobutton and the polyester tape or an adjustable cortical fixation system (ACL TightRope RT; Arthrex) was attached at the looped end. The length of the tendon portion of the hybrid graft was approximately 100 to 120 mm, and the diameter was 6 to 7 mm (Figure 4).
For PMC reconstruction, a small longitudinal incision was made on the medial femoral condyle to create a femoral tunnel located slightly proximal and posterior to the femoral medial epicondyle (Figure 6). A guidewire was drilled at the center of the femoral attachment of the sMCL on the medial femoral condyle. Special care was taken to avoid penetrating this guidewire through the femoral tunnels previously created for cruciate ligament reconstruction. This guidewire was over-reamed with a 4.5-mm cannulated drill (Endobutton drill, Smith & Nephew). After the tunnel length was measured with a scaled probe, a 20-mm socket was made by over-reaming with a cannulated drill, which had a diameter that matched the graft’s diameter. To create a tibial tunnel, the incision previously made for harvesting the hamstring tendon was used. A guidewire was drilled at a distal point of the tibial attachment of the sMCL. This attachment site was located approximately 6 cm distal to the medial joint line. Another small longitudinal skin incision was made along the AL edge of the tibia. The tibial guidewire was over-reamed with the size of the graft cannulated drill.

Posteromedial corner reconstruction. (A) The graft was secured on the outer cortex of the femur. (B) The tibial end of the graft was passed through distally and pulled out from the distal skin incision.
After each graft for the cruciate ligament reconstruction was placed into the femoral tunnel through the tibial tunnel and fixed at the femoral side, the hybrid graft for PMC reconstruction was implanted into the femoral tunnel, and the femoral end of the graft was fixed with an EndoButton. The PMC graft was passed deep to the sartorial fascia. The polyester tape of the tibial side of the graft was passed through the tibial tunnel and changed the direction to the AM aspect of the tibia through a subcutaneous tunnel. All the tibial ends of the grafts were tensioned with manual maximal forces and fixed together onto the AM aspect of the tibia with 2 spiked staples. In the case of ACL/PCL/PMC reconstruction, the tibial ends of the PCL and PMC grafts were secured with 2 spiked staples, and the tibial suture of the ACL graft was secured with a cancellous bone screw through the double-spike plate (Smith & Nephew Endoscopy).
PLC Reconstruction
For the PLC reconstruction, the biceps femoris tendon graft was used as the modified Clancy method according to previous studies.6,20,34 After the iliotibial band was retracted anteriorly, the injured LCL was identified. The peroneal nerve was carefully released from the proximal fibula and the posterior biceps femoris tendon. The anterior half of the biceps femoris tendon was released from the proximal portion. Then, the biceps femoris tendon graft was created. The fibular insertion of the biceps femoris tendon was preserved. The proximal end of the biceps femoris tendon was divided into 2 portions longitudinally. An adjustable cortical fixation system was rigidly connected to the proximal portion of the biceps femoris tendon graft (Figure 7). A guidewire was inserted at the proximal attachment of the LCL, which on the femur was located slightly proximal and posterior to the femoral lateral epicondyle. It is essential that the surgeon avoid tunnel convergence to the femoral ACL tunnel due to overlapping.17,18,54 The femoral tunnel for the PLC reconstruction was created with a 4.5-mm cannulated drill. After a measurement of femoral tunnel length, the femoral socket was created to the graft diameter using a cannulated drill (Figure 7). After the graft for cruciate ligament reconstruction was placed into the femoral and tibial tunnels and fixed at the femoral side, the graft for PLC reconstruction was implanted into the femoral tunnel, and the femoral end of the graft was fixed with an EndoButton. In the case of ACL/PCL/PLC reconstruction, the tibial ends of the ACL and PCL grafts were secured according to bicruciate reconstruction. The graft for the PLC reconstruction was also tensioned at 30° flexion for the final graft fixation, avoiding the varus position.

Posterolateral (PLC) reconstruction. (A) An adjustable cortical fixation system was constructed to the proximal portion of the biceps femoris tendon graft. (B) The graft for PLC reconstruction was implanted into the femoral tunnel.
Postoperative Management
Postoperative management was performed according to an original rehabilitation protocol. 70 Rehabilitation after the chronic-stage surgery, included knee brace immobilization at 10° of knee flexion for 2 weeks. Partial weightbearing was permitted 2 weeks after surgery. Full weightbearing was allowed after 4 weeks postoperatively. We used a long-leg hinged dynamic knee brace for prevention of posterior subluxation until 3 months after surgery. After 12 weeks postoperatively, several types of athletic exercise (strength and balance training, cycling) were gradually allowed, although no running was allowed until 6 months after surgery. Return to full sports activity was generally permitted at 12 months after surgery.
Clinical Evaluation
Each patient underwent clinical examination ≥2 years after surgery. One experienced orthopaedic surgeon (Y.M.) who was not involved with the surgery examined the patients and evaluated the knee function. Anteroposterior knee laxity was examined with the KT-2000 arthrometer (MEDmetric) and stress radiography. Total anteroposterior displacement with an applied anterior or posterior force of 133 N was measured at 20° and 70° of knee flexion with the KT-2000 arthrometer. Stress radiographs were obtained in 90° of knee flexion with an applied anterior or posterior force of 133 N with a Stryker knee laxity tester. The tibial displacement relative to the femur was measured on lateral radiographs. The ratio of the length from the anterior of the tibial plateau to the midpoint of the femoral posterior condyles and anterior to the posterior tibial plateau was indicated as a percentage (Figure 8). 20 To assess objective varus and valgus instabilities, we performed a stress radiograph examination under varus and valgus stress with the knee at 20° of flexion using the Telos device. The degree of total joint space opening was calculated according to the method previously reported.32,52 Concerning the International Knee Documentation Committee (IKDC) objective evaluation, the degree of joint line opening was changed compared with the contralateral side. 21 Peak isokinetic torques of the quadriceps and hamstring were measured at an angular velocity of 60 deg/s using Cybex II (Lumex) in both knees after surgery. Mean muscle torque, as measured 3 times postoperatively in the involved knee, is presented as a percentage of the uninvolved knee’s value. The Lysholm score, the objective IKDC evaluation form, and the Knee injury and Osteoarthritis Outcome Score (KOOS 50 ) were used to evaluate postoperative knee function. Activity levels before injury and at the follow-up period were also evaluated using the Tegner score. 59

Evaluation of the femorotibial position on a stress radiograph in 90° of knee flexion. A line was drawn along the tibial plateau (a), and another line parallel to the tibial plateau (b) was drawn from the anterior tibial plateau to the overlapped mediolateral femoral posterior condyles. The ratio of the length from the anterior tibial plateau to the midpoint of the femoral posterior condyles and anteroposterior tibial plateau was indicated as a percentage.
Statistical Analysis
An a priori power analysis was performed. Based on our previous studies,20,34,70 a sample size of 41 patients (41 knees) was calculated to have 80% power to test the hypothesis. All data are presented as means ± SD. The paired Student t test was used to assess the difference between the injured knee and the opposite knee. The Mann-Whitney U test and the chi-square test or Fisher exact test were used to test for significance. The significance level was set at P = .05. All statistical analyses of the data were performed using the statistical software JMP Pro (Version 11.0).
Results
Additional Treatment
Partial meniscectomy was performed for unstable meniscal tears in 6 and 7 knees in groups 1 and 2, respectively. Meniscal suture was performed in 2 and 6 knees in groups 1 and 2, respectively. Debridement was performed for fragmentation of the cartilage in 1 and 4 knees in groups 1 and 2, respectively. No treatment was administered for softening or fissuring of the articular cartilage.
Knee Stability
The side-to-side difference in the total anteroposterior translation measured at 20° and 70° of knee flexion significantly improved postoperatively in both groups (group 1: P < .0001, P = .0033; group 2: P < .0001, P < .0001). The postoperative side-to-side difference in the total anteroposterior translation measured at 20° and 70° averaged 2.0 mm and 2.0 mm, and 3.2 mm and 2.2 mm, in groups 1 and 2, respectively (Table 3). There were no significant differences in the postoperative anteroposterior laxity between the groups.
Knee Stability a

Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate a statistically significant difference between pre- and postoperative values, and the 2 study groups (P < .05). AP, anteroposterior; IKDC, International Knee Documentation Committee; Post, postoperative; Pre, preoperative.
Preoperative data vs final follow-up data in group 1.
Preoperative data vs final follow-up data in group 2.
Preoperative data in group 1 vs preoperative data in group 2.
Final follow-up data in group 1 vs final follow-up data in group 2.
The relative femorotibial position on the anterior and posterior stress radiographs measured at 90° of knee flexion significantly improved postoperatively in both groups (group 1: P = .0115, P = .0007; group 2: P = .0004, P < .0001) (Table 3). The postoperative position on the anterior and posterior stress radiographs averaged 63.2% and 62.4%, and 55.2% and 52.8%, in groups 1 and 2, respectively. The relative femorotibial positions in groups 1 and 2 showed no significant differences in comparison with that in the uninjured knee (P = .5536, P = .0601, mean; 61.9% and 56.4%, in anterior and posterior stress radiographs, respectively). There were no significant differences in the postoperative position on the anterior and posterior stress radiographs between the groups.
In the valgus stress test, the preoperative medial joint opening measured at 20° of knee flexion was significantly greater in group 2 than in group 1 (P < .0001). This value significantly improved postoperatively in group 2 (P < .0001) (Table 3). The total postoperative medial joint opening measured at 20° of knee flexion averaged 7.4 mm and 7.7 mm, in groups 1 and 2, respectively (Table 3). There were no significant differences in the postoperative medial joint opening between the groups. None of the patients showed a side-to-side difference of >5 mm in the medial joint opening.
In the varus stress test, the preoperative lateral joint opening measured at 20° of knee flexion was significantly greater in group 2 than in group 1 (P = .001). This value significantly improved postoperatively in group 2 (P = .0093) (Table 3). The total postoperative lateral joint opening measured at 20° of knee flexion averaged 8.8 mm and 9.4 mm, in groups 1 and 2, respectively. There were no significant differences in the postoperative lateral joint opening between the groups. None of the patients showed a side-to-side difference of >5 mm in the lateral joint opening.
Clinical Outcomes
No patients showed a loss of knee extension of >5°, while 4 patients in group 2 revealed a loss of flexion of >16° (Table 4). Any patient did not require a manipulation or lysis of adhesions.
Objective and Subjective Clinical Results a

Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate a statistically significant difference between pre- and postoperative values, and the 2 study groups (P < .05). ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; Post, postoperative; Pre, preoperative; QOL, Quality of Life; Sport/Rec, Sport and Recreation.
Pre-operative data vs final follow-up data in group 1.
Pre-operative data vs final follow-up data in group 2.
Pre-operative data in group 1 vs preoperative data in group 2.
Final follow-up data in group 1 vs final follow-up data in group 2. The dash indicates ≥ .99.
The Lysholm score, the IKDC evaluation, all subscales of the KOOS, the Tegner activity score, and the isokinetic peak torque of the quadriceps and hamstring muscles significantly improved postoperatively in both groups (P < .0001) (Table 4). The postoperative Lysholm score averaged 93.0 points and 88.0 points, in groups 1 and 2, respectively. In the IKDC evaluation, 19 (group 1, 7; group 2, 12), 17 (group 1, 8; group 2, 9), and 5 (group 1, 0; group 2, 5) knees were graded as A, B, and C, respectively (Table 4). The Lysholm score, the IKDC, and all subscales of the KOOS, the Tegner score, and the isokinetic peak torque of quadriceps and hamstring muscles did not differ between the 2 groups.
Postoperative Complications
At the final follow-up, 3 patients who had common peroneal nerve palsy in groups 1 and 2 showed functional recovery. During surgery, there were no serious complications such as iatrogenic cartilage injuries, serious malposition of the tunnels, graft fixation failure, vascular injuries, fractures, and deep vein thrombosis in either group. Four patients in group 2 revealed a loss of flexion of >16°. Three patients who had acute intra-articular infections in group 2 were treated by arthroscopic synovectomy within 2 weeks postoperatively, and continuous irrigation treatment 31 was performed without the graft removal. The method utilized a crisscross flow-reversal system using a double tube that prevented obstruction of the tube. There were no complications related to contralateral graft harvest.
Discussion
The most important finding of the present study was that there were no significant differences in the postoperative knee stability and clinical outcomes between bicruciate reconstruction and bicruciate and collateral ligament reconstruction/repair groups. MLKI along with bicruciate ligament rupture (MLK 2 and MLK 3) can be safely performed using autografts. The Lysholm overall clinical scores were favorable, and the postoperative knee stability was found to be good without a loss of knee extension of >5°.
Recently, outcomes after combined bicruciate reconstruction have been widely reported.16,23,36,57 A variety of surgical techniques have been described using ipsilateral or contralateral autografts and allografts. Several authors63,66 advocate for use of autografts due to the lower failure rate compared with allograft, particularly in young adult patients. Other authors recommend allograft, to avoid sacrificing ipsilateral native tissue in an already severely compromised knee; or contralateral grafts, which may affect the patient’s mobility and rehabilitation after surgery.15,46 However, they are not always available in every country. We selected the hamstring tendon or the BTB autografts for ACL and PCL reconstruction. We prefer to use multistrand hamstring tendon hybrid graft for PCL reconstruction because of the size, superior structural properties, and easy passage through the bony tunnel. Based on previous biomechanical sudies,33,70 the hybrid graft constructed using this technique has strength comparable with the BTB graft secured with interference screws. However, one of the critical issues when using the autograft is potential graft-site morbidity as >2 graft constructs are needed in combined ligament reconstruction. Although we could safely use multiple grafts according to the algorithm as shown in Table 2, we should be very careful not to cause the postoperative functional disability of the knee. Objective and subjective clinical outcomes of the present study were comparable with previous studies.14,57,65
In this study, we used a commercially available polyester tape (the Leeds-Keio Artificial Ligament) in our bicruciate reconstructions. However, we did not use this tape as an artificial ligament or an augmentation device, but as one of the fixation devices for the hamstring tendon graft to the bone. Specifically, the tape was connected in series with the doubled or quadrupled tendon using our original technique,72,73 and only the autogenous tendon portion was placed across the joint. It is well known that weak points of the hamstring tendon graft fixed with sutures to the bone are (1) low stiffness of the graft-suture-bone complex, (2) rapid relaxation of the graft tension after surgery, and (3) difficulty in tension control during graft fixation. The so-called hybrid graft was used to improve upon these weak points. Namely, the femoral graft–tibial complex with the hybrid graft involves the following advantages according to biomechanical properties with the tensile test and the cyclic loading test33,44,69: (1) higher stiffness and stronger ultimate load than the complex with the suture method; (2) more resistance to the graft tension relaxation; and (3) clinically, an acceptably long and thick hybrid graft can be fashioned by surgeons with a relatively short or thin autogenous tendon, and the hybrid graft can be more easily fixed to the bone, applying a tension quantified by using a tensiometer to the graft.
Previous studies reported PMC reconstruction using allograft, autograft, and artificial ligament.1,10,23,35,41,56 Yoshiya et al 74 reported sMCL reconstruction using single semitendinosus and gracilis tendons secured with an interference screw and Endobutton. They reported favorable clinical results in which the symptoms according to the IKDC criteria were rated normal or nearly normal in 88% of the patients, and all patients had a side-to-side difference of the medial joint opening that was ≤2 mm. LaPrade and Wijdicks 38 also noted that sMCL reconstruction using semitendinosus autograft has been reported to restore near-native stability to the medial side of the knee. Kitamura et al 32 reported on sMCL reconstruction using a semitendinosus tendon hybrid autograft for chronic medial knee instability. The present study showed there were no significant differences in the postoperative medial joint opening between the groups. None of the patients showed a side-to-side difference of >5 mm in the medial joint opening. A potential weakness of our MCL reconstruction is that we did not reconstruct the POL. The POL has an important role in medial stability of the knee,7,68 although the sMCL is a primary static stabilizer resisting valgus stress and assisting in restraining rotation.64,67 Recently, a few studies have introduced anatomic reconstruction techniques for both the sMCL and the POL.29,41 However, no clinical studies have been conducted to compare the superiority of the sMCL and POL reconstruction to the isolated sMCL reconstruction. In addition, the clinical outcome of our procedure was comparable with those of other anatomic reconstruction procedures.29,41 Therefore, the present study suggested that reconstruction of the POL is not a prerequisite for good clinical outcomes in these complex knees.
Recently, chronic PLC deficiency has been treated by reconstructions with various levels of combined injury of the knee to restore the functions of the damaged structures. The Larson reconstruction 39 is commonly performed using the hamstrings tendon. 45 Clancy and Sutherland 6 reported PLC reconstruction with biceps femoris tendon using an interference screw or a tendon anchor. Kim et al 55 reported a favorable clinical outcome of biceps femoris tendon rerouting technique for PLC instability. Fanelli and Edson 13 also reported that PLC reconstruction with biceps femoris tenodesis and PL capsular shift was effective treatment for PLC insufficiency. LaPrade et al 37 introduced a 3-strand PLC reconstruction. Recently, Jakobsen et al 26 reported that a new 4-strand PLC reconstruction has been developed. Miyatake et al 45 reported that the rotational knee laxity in response to both external rotation and posterior translation load were significantly better after the 4-strand PLC reconstruction than after the modified Larson reconstruction. Biomechanical stabilities were significantly better in the 3- or 4-strand PLC reconstruction than in the Larson procedure. However, a 3- or 4-strand PLC reconstruction technique has complex procedures, such as invasive tunnel creation, necessities of long autograft or allograft. Therefore, the authors selected the simple technique of the modified Clancy methods for PLC reconstruction in chronic MLKIs according to previous studies.20,34 However, a long-term follow-up examination is needed for PLC reconstruction, particularly concerning external rotation instability.
Regaining the appropriate femorotibial position is one of the most important factors, but it is very difficult to obtain in combined knee instabilities because the only way to control the femorotibial position is by tensioning the grafts. 43 The importance of tensioning and fixation of the graft on clinical outcome has been reported in isolated ACL or PCL reconstruction procedures because improper tensioning may cause graft failure or functional loss of the knee joint. Because MLKIs are uncommon, there are no controlled or randomized studies to clarify how much tension should be used at the time of the graft fixation. If only 1 cruciate ligament were reconstructed in combined ligament injuries, it might cause permanent anterior or posterior subluxation as well as an incorrect rotational position. On reconstructing multiple ligaments, some authors recommend that the PCL should be tensioned first at 70° to 90° of knee flexion because it is the primary stabilizer. 65 We use a simultaneous tensioning technique of both cruciate ligaments at 90° of knee flexion and make sure of the anatomic position by radiographs during surgery. However, we cannot be certain that this technique would result in a better clinical outcome. The tensioning and fixation of the grafts are of vital importance and should be studied clinically and biomechanically to clarify the degrees of knee angle and tensioning force. To the best of our knowledge, there is no consensus regarding the best protocol for the sequence of graft fixation in this procedure. Many authors recommend PCL graft fixation first, 57 but others support initial ACL graft fixation followed by PCL graft fixation. 5 Some authors recommended simultaneous tensioning of the ACL and PCL grafts.42,70 Kim et al 28 found that higher functional scores could be achieved when the grafts were tensioned simultaneously, compared with patients treated with a PCL-first approach.
Recently, anatomic repair and reconstruction procedure in MLKIs have shown superior outcomes compared with older techniques. Tzurbakis et al 60 evaluated the midterm results of surgical treatment in different groups of patients with MLKI as follows: group A included ACL and PMC injuries, group B included ACL or PCL and PLC injuries, and group C consisted of ACL and PCL with PMC or PLC injuries. Although no statistically significant differences were observed in the clinical results among the groups, patients who had IKDC grade as C and D were 10%, 30%, and 33%, in groups A, B, and C, respectively. Cain et al 3 reported that the 2-ligament and >2-ligament groups did not significantly differ in IKDC score or proportions with successful return to sport in American football players. Everhart et al 12 reported that among studies without Schenck grade IV or V injuries, return to work with no or minimal modifications was higher than studies that included Schenck grade IV and V patients. In this study, there were no significant differences in the clinical outcomes between groups 1 (MLK 2) and 2 (MLK 3). However, according to the IKDC rating, 5 patients in group 2 were classified as nearly abnormal. One important factor contributing to the unfavorable IKDC rating in 5 patients was that knee contracture had already existed before surgery. Poploski et al 47 reported that loss of ROM was the most common postoperative complication after treatment of MLKI. Postoperative rehabilitation for MLKIs, which typically involves a period of nonweightbearing and delayed initiation of ROM exercises, may also contribute to loss of ROM. This result indicated that the initial treatment and rehabilitation in the acute stage after injury are of importance for the second surgery.
Limitations
There were certain limitations in this study. Factors that may have influenced the results of this research included the fact that this was a retrospective, nonrandomized study. Additionally, the cohort included a relatively small number of cases (N = 41), which were divided into 2 study subgroups. Furthermore, there was heterogeneity in the age of the patients (mean age, 31 years; range, 16-60 years). Multiple different techniques (SB and DB) for ACL or PCL reconstruction were performed, and MLKIs are relatively rare and complex and thus challenging to treat. Moreover, there were insufficient data on long-term clinical outcomes (the mean follow-up period was 31.8 months), which were crucial to assess the lasting efficacy of the surgical intervention. Beyond these limitations, however, the present study suggested that by performing collateral ligament surgery, group 2 became equivalent to group 1, so they showed similar outcomes after bicruciate reconstruction.
Conclusion
There were no significant differences in the knee stability and clinical results after bicruciate reconstruction between those with and those without collateral ligament surgery. Reconstruction of bicruciate MLKIs with repair or reconstruction of associated collateral ligament injuries improves clinical outcomes.
Footnotes
Acknowledgements
The authors appreciate Howard Tarnoff, professor emeritus, for proofreading the English draft.
Final revision submitted August 14, 2024; accepted September 11, 2024.
Presented in part at the 12th biennial Congress of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine, Cancun, Mexico, May 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: Centre for Sports Medicine, Hokkaido University Hospital, has the following financial relationships to disclose: grant/research funding from Japan Tissue Engineering, Co, Ltd, Japan; KYOCERA, Co, Japan; Olympus Terumo Biomaterials, Co, Japan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hokkaido University Hospital (No. 0170163).