
Abstract
Background:
While patients receiving workers’ compensation (WC) often exhibit lower postoperative functional outcomes after orthopaedic surgery, this has not been completely explored with proximal hamstring avulsion injury (PHAI).
Purpose:
To (1) investigate the impact of patients with WC status on the functional outcome of PHAI repair and (2) identify risk factors for worse outcomes after PHAI repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study focused on adults >18 years who underwent primary PHAI repair between 2008 and 2021 and had minimum 2-year follow-up data. Patients were divided into a WC group and a control group matched based on age, Tegner score, injury type (chronicity and tendon involved), and follow-up duration. The primary outcome measure was the Parisian Hamstring Avulsion Score (PHAS), with secondary outcomes including return-to-work metrics, activity levels measured by the Tegner and University of California at Los Angeles scores, and complications. The association between WC status and having worse postoperative outcomes (work changes, PHAS scores in the bottom 25% of cases, delayed return to work, or complications) was assessed, and the model that showed a statistically significant association with WC status was included in a multivariate analysis to adjust for confounders.
Results:
Overall, 104 patients (51 WC and 53 controls), with a mean age of 49.56 ± 9 years and a mean follow-up of 58.99 ± 44.61 months, were included. PHAS scores improved significantly after repair in both groups, yet WC patients exhibited lower postoperative PHAS scores (158.78 ± 34.43) than did control patients (171.77 ± 32.17; P = .049). Regression analysis revealed that patients with WC had a significantly higher risk of scoring in the bottom 25% (<150.75) on the PHAS (odds ratio [OR], 2.81 [95% CI, 1.09-7.28]; P = .033). On multivariate analysis, injury chronicity emerged as a significant risk factor for PHAS scores of <150.75 (OR, 8.09 [95% CI, 2.07-31.59]; P = .003), while the direct impact of the WC status was reduced (OR, 2.13 [95% CI, 0.75-6.07]; P = .155).
Conclusion:
The lower functional outcomes seen in patients with WC were not significant after adjusting for confounders, with injury chronicity being the key factor affecting postoperative results. No association was detected between WC status and return-to-work metrics.
Proximal hamstring avulsion injury (PHAI) is becoming increasingly diagnosed in both active individuals and athletes.7,11,15,18 PHAIs are usually caused by an accident that leads to hip flexion while the knee is hyperextended, such as in a split injury or sudden acceleration.3,4,18 The diagnosis is usually made through ultrasound or magnetic resonance imaging (MRI). PHAI management is guided by the extent of the injury and the amount of retraction.8,20 Complete injuries involving both the conjoint and semimembranosus tendons are treated surgically,9,11,15,21,25 while partial injuries involving either tendon with <2 cm of retraction are initially treated nonoperatively.2,19,23
Surgical treatment of PHAI has been favorable in improving functional outcomes, patient-reported outcome scores, and return to sports.9,11,15,18,21,25 Several studies have investigated the prognostic factors associated with poor outcomes in PHAI; the most consistently demonstrated factor is the chronicity of the injury, which has been associated with lower functional outcomes and more complications.7,11,13 In addition, complete injuries have been linked with reduced rates of returning to sports among professional athletes 18 and a higher incidence of complications. 9 Another significant factor influencing prognosis is the severity of tendon retraction.28,29
Despite its potential impact, the influence of workers’ compensation (WC) status on outcomes after PHAI repair has been minimally investigated, with only a handful of studies delving into this area.12,26 On the other hand, research in various orthopaedic fields has indicated that patients receiving WC generally report poorer functional outcomes and have longer recovery durations compared with those without WC status.5,6,10,22 This has particularly been shown in patients with rotator cuff injury, 22 isolated biceps tendinosis, 5 and degenerative disc disease. 6
This study aimed to investigate the impact of WC status on the functional outcome of PHAI repair as compared with the outcomes of a control group without WC status. We also aimed to identify the risk factors of having worse PHAI repair outcomes in these populations. We hypothesized that WC status would not be associated with lower PHAI outcomes.
Methods
Study Design and Inclusion
This study was a retrospective, monocentric, matched cohort study conducted at a sports surgery referral center from 2008 to 2021. It targeted patients who underwent surgical treatment for PHAI. The study was approved by the local ethics committee, and written informed consent was obtained from patients to participate in the study.
The inclusion criteria encompassed all adult patients aged >18 years old who underwent primary repair for PHAI and had a minimum follow-up period of 2 years. The exclusion criteria were patients who underwent revision surgery, those who received graft augmentation for repair, those with bony injuries, noninsertional PHAI, and patients who refused surgery.
Two groups were established based on the cause of the accident leading to PHAI: a WC group and a control group. A patient in the WC group was defined as an individual who received WC due to a PHAI from an accident occurring at work.
Indication for Surgery
Indications for surgery encompassed all patients with complete PHAI, those with partial injury showing >2 cm of tendon retraction, or those not improving after 6 months of nonoperative treatment. A complete injury was defined as an injury involving all hamstring tendons (semimembranosus and conjoint tendons). Nonoperative treatment was reserved for patients with partial injury along with retraction of <2 cm. Tendon retraction was measured on MRI. All diagnoses were made by clinical examination and MRI.
Surgical Technique and Postoperative Rehabilitation Protocol
Most surgeries were performed by a senior surgeon (N.L.), with the remainder carried out by 2 other senior surgeons from the same team (Y.B. and A.H.); all surgeons were experienced in PHAI surgery. The surgical approach utilized was in accordance with the technique outlined by Lefevre et al. 14 After surgery, all patients followed a standardized rehabilitation protocol.
Postoperatively, patients were fitted with an articulated knee brace allowing full flexion but blocking the last 40° during extension for the first 3 postoperative weeks. Rehabilitation commenced with isometric exercises to strengthen both the quadriceps and hamstrings while maintaining knee flexion between 30° and 45°. A gradual increase in extension by an additional 10°, was allowed each week. Full weightbearing was introduced 6 weeks postoperatively. By the end of 6 weeks, the program advanced to dynamic quadriceps exercises within a closed kinetic chain and active-assisted hamstring exercises. Between the 12th and 16th postoperative weeks, patients were encouraged to engage in brisk walking and light jogging, emphasizing hamstring strength through isokinetic exercises, eventually progressing to eccentric exercises. From the 16th to the 32nd week, athletes typically resumed their regular sports activities.
Participants and Sample Size
The study population was matched using a propensity score to minimize selection bias in the WC and control groups. Propensity score matching was performed using R software Version 4.2 (R Core Team). All patients meeting the inclusion criteria were considered eligible for the propensity-matching process. Participants were matched on a 1 to 1 ratio, and matching was performed using a logit scale with a caliper width of 0.2. The matched variables included age, sex, Tegner activity scale before the injury, type of injury in terms of chronicity (acute or chronic), and type of rupture (complete or partial), and follow-up duration. During the study period, there were 72 patients with WC among 690 patients. Of these, 98 were excluded for various reasons—18 for bony avulsion, 35 for revision surgery, and 45 for allograft use. This left 592 patients, out of which 103 patients (17.7%) were lost to follow-up. The use of the propensity-score matching process resulted in 53 patients in the WC group and 53 in the control group. After the matching process, 2 patients from the WC group dropped out of the study (Figure 1).
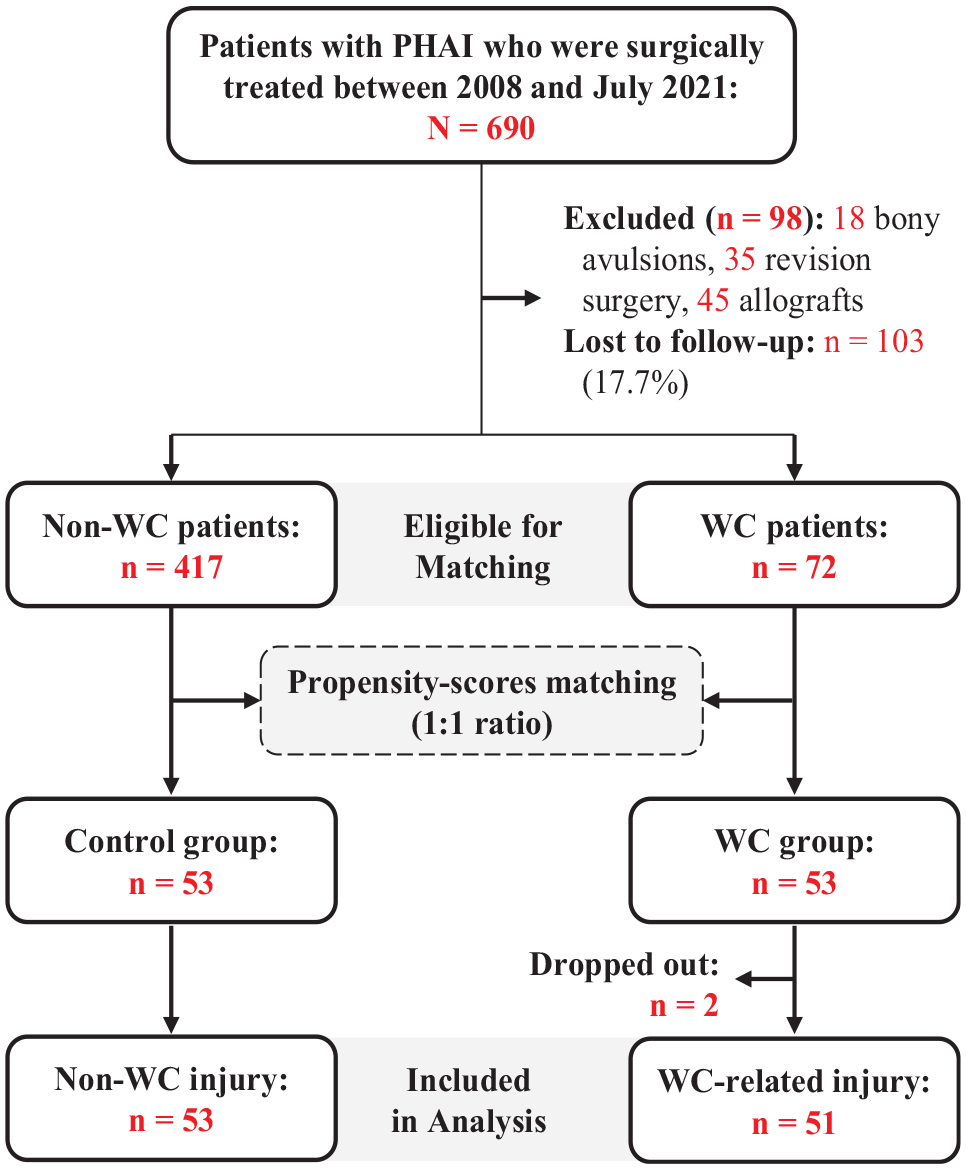
Flow chart of the cohort. PHAI, Parisian hamstring avulsion injury; WC, workers’ compensation.
Data Collection
Data were collected prospectively using online software (Web survey) accessed and filled both by patients for history, descriptive data, and patient-reported outcome scores, and by surgeons for physical examination, imaging results, and surgical findings. The collected data encompassed a range of variables—including descriptive data; occupation; preinjury and preoperative scores; and specific PHAI characteristics, such as the type of injury (partial vs complete), chronicity of the injury (acute vs chronic), the time elapsed until surgery, and degree of tendon retraction. Chronicity was specifically defined as an injury-to-surgery delay exceeding 28 days.
The level of occupational activity was categorized into low, intermediate, or high based on the physical demands associated with each profession, according to the criteria established by Steeves et al. 24
Outcome Measures
The primary outcome was assessed using the Parisian Hamstring Avulsion Score (PHAS) 17 at the last follow-up. The PHAS—a comprehensive 36-item score with 9 categories and an overall score ranging from 0 to 200—is used to measure the functional status of patients with PHAI. Secondary outcome measures comprised the rate and quality of return to work, the time taken to return to work, and the rate of complications—including rerupture, deep venous thrombosis, and sciatic nerve palsy. Additional outcome measures included the Tegner activity scale and the University of California at Los Angeles (UCLA) activity scale. Both the Tegner 27 and UCLA1,30 activity scales are 10-point systems evaluating the patient’s level of sports activity, with higher scores indicating higher levels.
In addition, we investigated the association between WC status and having worse postoperative outcomes, defined as having a PHAS score lower than that of quartile 1 (bottom 25% of the population) at the last follow-up, not returning to work or changing work, having a return-to-work time that was longer than that of the quartile 3 (time to return to work >75% of the population), experiencing rerupture, or experiencing a complication.
Statistical Analysis
Statistical analyses were conducted using Datatab software (DATAtab e.U.). Continuous variables, represented as means with standard deviations or medians with interquartile ranges, were analyzed using the independent t test or the Mann-Whitney U test, depending on the distribution of data. Categorical variables, presented as frequency (percentage), were assessed using the chi-square test or the Fisher exact test as deemed appropriate. The significance level was established at P < .05.
Statistical analysis was expanded to include logistic regression to evaluate the odds ratio (OR) of experiencing worse postoperative outcomes. The logistic regression models were constructed for the various outcomes—PHAS scores lower than that of quartile 1, not returning to work, changing work, return-to-work time longer than that of quartile 3, rerupture, and complications. Each model aimed to assess the impact of WC status compared with control.
The model that showed a statistically significant association with WC status was chosen as an outcome of interest and was further studied in a multivariate regression analysis to assess risk factors while adjusting for confounders. The regression analysis estimated the ORs of having worse results, with 95% CIs calculated. Univariate regression analyses were conducted before fitting the multivariate model to identify potential confounding variables, with a significant association with the outcome at P < .2.
Sample Size Justification
To assess the return-to-work rate, sample size calculations were based on the study by Johnson et al, 12 anticipating a return rate of 70% in the WC group and 94.1% in the control group, with a balanced enrollment ratio. With an alpha of .05 and targeting an 80% power (β = 0.2), the necessary sample size was determined to be 39 participants per group, leading to a total of 78 participants. This ensured an 80% chance of identifying a significant difference between groups.
Given the absence of previous studies utilizing the PHAS score, a post hoc power analysis was performed using a paired t test to evaluate the study’s capability to discern changes in postoperative PHAS scores across groups. An effect size of 0.39 was calculated from mean differences and pooled standard deviations. With 104 observations and maintaining a 5% significance level (α = .05), this analysis achieved a power of 0.98 (98%), indicating a high probability of detecting the observed effects.
Results
Patient Characteristics
The characteristics of the 104 study patients are detailed in Table 1. Other than accident circumstances, both the WC and control groups were comparable, showing a mean age of 49.56 ± 9 years, a mean follow-up of 58.99 ± 44.61 months, and predominantly intermediate occupational activity levels at 55.77%.
Patient Characteristics a

Data are presented as mean ± SD or n (%) unless otherwise indicated. The bold P value indicates a statistically significant difference between the WC and control groups (P < .05). BMI, body mass index; IQR, interquartile range; MRI, magnetic resonance imaging; PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California at Los Angeles; WC, workers’ compensation.
1 soccer player and 1 sports coach.
1 dancer, 1 rugby player, and 1 military servicemember.
PHAS Results
Both groups showed significant pre- to postoperative improvements in PHAS scores (P < .05) (Figure 2 and Table 2). Patients in the WC group exhibited lower postoperative PHAS scores than those in the control group (158.78 ± 34.43 [WC] vs 171.77 ± 32.17 [control]; P = .049). The mean difference in PHAS outcomes between the control and WC groups for the PHAS was 12.99 points (95% CI, 2.15-23.83 points).

Graphs showing the pre- and postoperative outcome scores in the WC and control groups. The box represents the IQR, the solid horizontal line represents the median, the dashed horizontal line represents the mean, the whiskers represent the range within 1.5× IQR, and the dots represent outliers. IQR, interquartile range. PHAS, Parisian Hamstring Avulsion Score; WC, workers’ compensation.
Comparison of Postoperative Outcomes Between the WC and Control Groups a
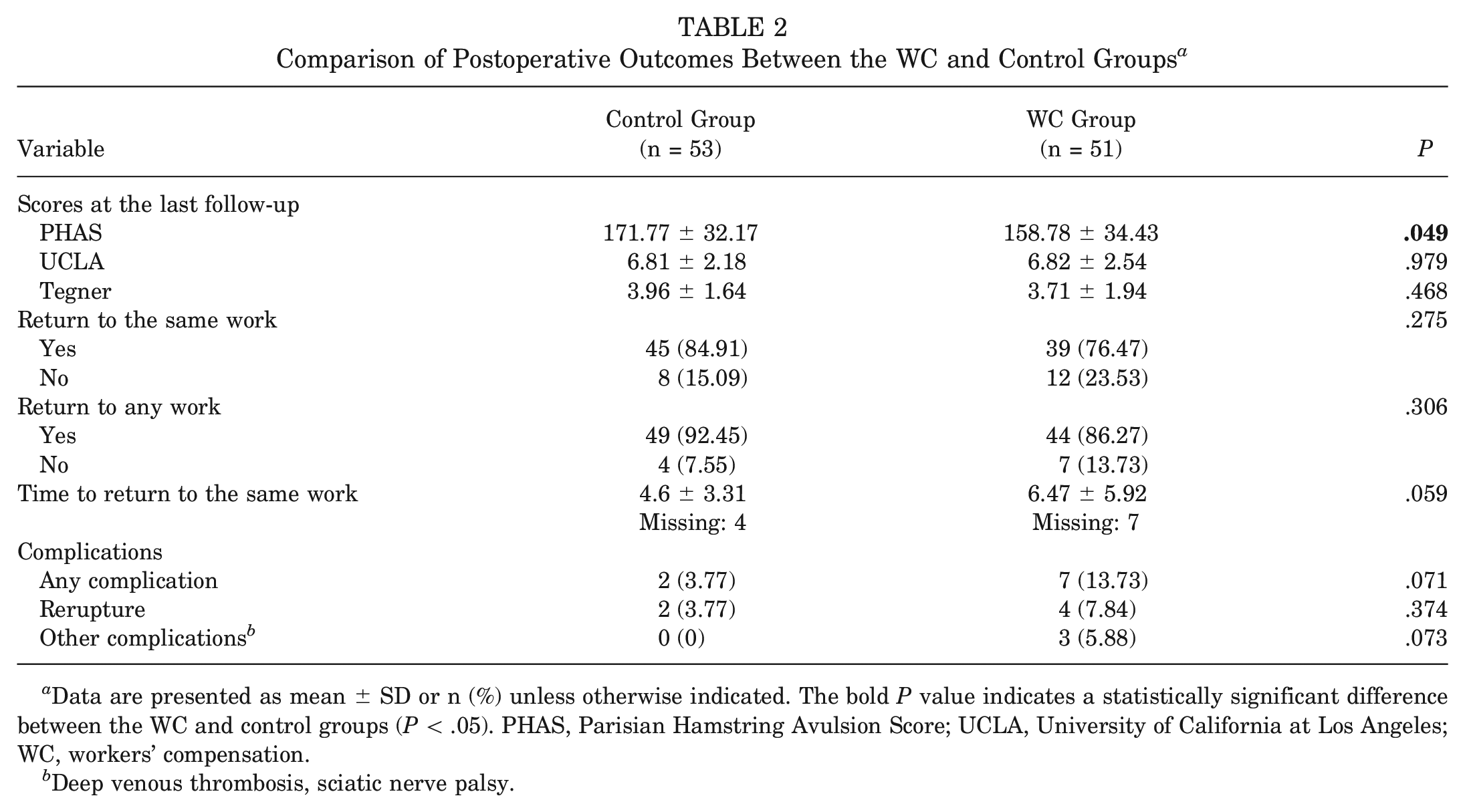
Data are presented as mean ± SD or n (%) unless otherwise indicated. The bold P value indicates a statistically significant difference between the WC and control groups (P < .05). PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California at Los Angeles; WC, workers’ compensation.
Deep venous thrombosis, sciatic nerve palsy.
Other Outcomes
Both groups showed significant improvements on the Tegner and UCLA scales (P < .05). At the last follow-up, no significant group differences were observed in the UCLA (P = .979) and Tegner (P = .468) scores or the rate of return to the same or any work. A trend toward a longer time to return to work was observed in patients with WC compared with controls (6.47 ± 5.92 vs 4.6 ± 3.31 months, respectively; P = .059), as well as a trend toward a higher incidence of complications in the WC group compared with the control group (13.73% vs 3.77%, respectively; P = .071), including reruptures (7.84% [WC] vs 3.77% [control]; P = .374) and other complications (2 deep venous thrombosis and 1 sciatic nerve palsy in the WC group vs none in the control group; P = .073).
Regression Analysis of the Impact of WC Status on Variables Defined as Worse Postoperative Outcomes
The quartile 1 for the PHAS score was 150.75. The OR for having a PHAS of <150.75 was significantly higher in the WC group at 2.81 (95% CI, 1.09-7.28; P = .033) (Table 3). For other outcomes, the odds of not returning to work, changing work, and delayed return to work were not significantly different for the WC group. The WC group had a higher risk of rerupture (OR, 2.17 [95% CI, 0.38-12.4]; P = .384) and complications (OR, 4.06 [95% CI, 0.8-20.55]; P = .091), although this difference was not statistically significant.
Regression Analysis Models for Evaluating the Impact of WC Status on the Odds of Having Worse Patient Outcomes a

OR, odds ratio; PHAS, Parisian Hamstring Avulsion Score; WC, workers’ compensation.
Risk Factors of Having Worse Outcomes (PHAS of <150.75)
The outcome of interest chosen for the risk factor analysis was having a PHAS of <150.75. The univariate regression analysis identified occupational activity classification (OR, 3.21 [95% CI, 0.75-13.69]; P = .114) and injury chronicity (OR, 7.52 [95% CI, 2.08-27.17]; P = .002) as potential confounders (Table 4). The multivariate regression analysis showed that injury chronicity was the only risk factor associated with a PHAS of <150.75 (OR, 8.09 [95% CI, 2.07-31.59]; P = .003), while the impact of WC status was decreased below the level of statistical significance (OR, 2.13 [95% CI, 0.75-6.07]; P = .155) (Table 4).
Risk Factors of Having Worse Outcomes (PHAS of <150.75) a
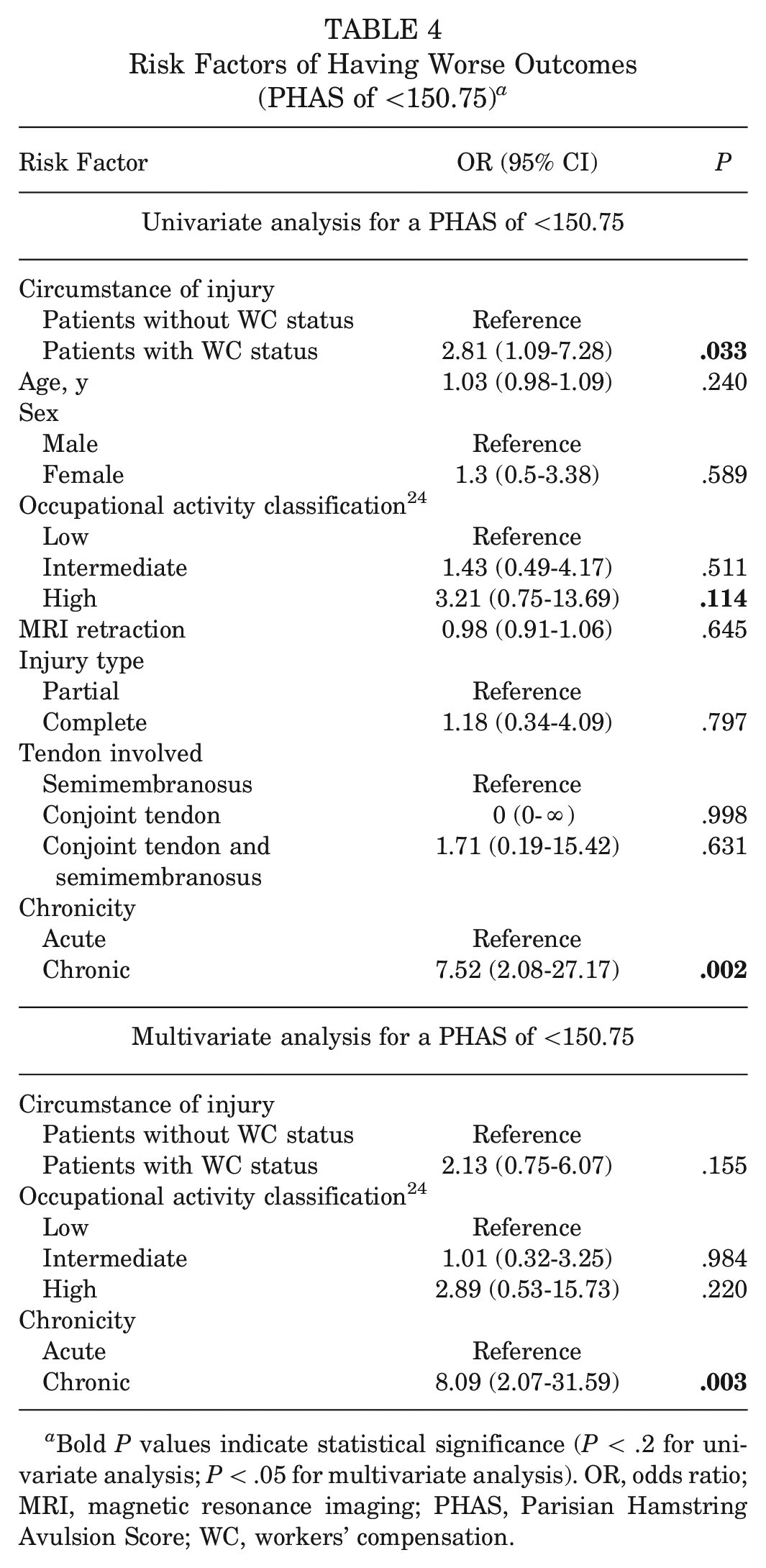
Bold P values indicate statistical significance (P < .2 for univariate analysis; P < .05 for multivariate analysis). OR, odds ratio; MRI, magnetic resonance imaging; PHAS, Parisian Hamstring Avulsion Score; WC, workers’ compensation.
Discussion
The main finding of this study was that while patients in the WC group initially appeared to have lower postoperative functional PHAS outcomes, the significant effect of WC on this outcome is lessened after adjusting for confounding factors. The analysis ultimately identifies the chronicity of the injury as the primary risk factor for worse postoperative outcomes.
Our results distinguish from the existing literature suggesting the limited potential impact of the WC status on the functional outcomes of PHAI surgery.12,26 Specifically, Johnson et al 12 compared 20 patients with WC with matched controls based on age, sex, and type of injury and suggested that patients with WC undergoing open repair for complete PHAI experienced lower functional outcomes as measured by the Marx activity rating scale and Lower Extremity Functional Scale (LEFS) scores. 12 However, the authors acknowledged in their discussion that they did not account for the activity level while analyzing these results; groups with different functional outcomes can have different baseline activity levels, which may act as confounders. In our study, which included a larger sample size, we addressed this limitation by adding the Tegner activity level to the matching criteria. Furthermore, we performed a multivariate analysis, which adjusted for all confounders including the occupational activity level, and found that functional outcomes did not significantly differ between groups. This finding was echoed by Sullivan et al, 26 who compared 10 patients with WC with 20 matched non-WC individuals with PHAI and found no significant difference in physical recovery outcomes as measured by the LEFS and the Hip Outcome Score. However, they reported significantly lower mental health outcomes in the WC group as measured by the 12-Item Short Form Health Survey mental component score (49.28 ± 9.97 vs 54.26 ± 9.69; P = .032) and a longer duration for patients with WC to return to full-duty work 26 (21 ± 9 vs 9 ± 8 weeks; P = .005).
One important aspect to consider is the higher degree of chronicity found in patients with WC, which may well relate to delays in care because of their WC status (insurance vs WC authorization process). In the few studies addressing this subject, there is indeed more chronic injury in the WC group. Notably, in the study by Johnson et al, 12 a total of 15 out of 20 patients (75%) in the WC group had chronic injuries. This finding was also mirrored in our study, where the injuries in 33 out of the 51 patients in the WC group (64.71%) were chronic, although it had little impact on the results found in the present study, as patients were matched according to the chronicity level.
Despite no statistical difference in functional outcomes, patients with WC showed a delayed return to work. This may be due to economic incentives, as patients with WC might benefit longer from compensation, reducing the urgency to return. In addition, the WC process can delay treatment and clearance.
While Johnson et al 12 demonstrated a reduced rate of return to work and a longer recovery period in patients with WC, our study did not find an association between WC status and return-to-work metrics, despite achieving the sample size needed for a power of >80%. This discrepancy may be attributed to several factors and limitations in the study by Johnson et al, such as the small sample size and an unclear definition of “return to work”—a limitation we addressed by specifically reporting the rate of return to the same work as well as to any work. In addition, in the Johnson et al study, patients were not matched based on follow-up duration, meaning that having patients with only 1 year of follow-up in 1 group and those with longer follow-ups in another could skew the odds of return. The same issues apply to the study by Sullivan et al, 26 who matched groups only by age, sex, and body mass index.
Our study contributes further evidence to the existing body of knowledge, highlighting the significant negative impact of chronicity on the outcomes of PHAI.7,11,18 Multivariate analysis is associated with an eightfold increase in the odds of having a PHAS score in the lowest quartile. This claim is supported by several studies and meta-analyses on the subject. For instance, Lefevre et al 16 investigated the risk factors of rerupture in a cohort of 740 patients and found that those operated on after 32 days had 2.5 times the odds of developing the rerupture complication, and surgery after 28 days doubled the odds of this complication. Our findings build on these by demonstrating that patients operated on after 28 days are 8 times more likely to be in the bottom 25% of PHAS outcomes. Furthermore, a systematic review by Belk et al 7 reported a trend toward a higher rate of return to sports in patients with early intervention. Similarly, a systematic review by Hillier-Smith and Paton 11 found that acute intervention was associated with a lower incidence of rerupture and a higher percentage of return to sports.
In the broader context, a meta-analysis by De Moraes et al 10 revealed that patients with WC undergoing orthopedic surgeries face a 2-fold greater risk of unsatisfactory outcomes (relative risk, 2.08 [95% CI, 1.54-2.82])—including pathologies such as lumbar spine disorders, rotator cuff tears, and other musculoskeletal conditions. However, this generalized finding was not applicable in the case of PHAI in our study.
Limitations
This study is constrained by its retrospective analysis, although the data collection was conducted prospectively. The absence of randomization presents another limitation; however, this issue was addressed by employing a matching technique to adjust for confounders. While a sample size calculation was conducted with a focus on the rate of return to work, the study’s sample size may still be considered small for assessing other outcomes. In addition, the presence of athletes at a professional level in both groups (specifically, 1 soccer player and 1 sports coach in the control group and 1 dancer, 1 rugby player, and 1 military servicemember in the WC group) could act as a confounding factor affecting outcomes.
Despite these limitations, this research represents, to our knowledge, the largest comparative study on the topic to date. It is further strengthened by being based on calculated sample size, with rigorous matching criteria, and including multivariate analysis.
Conclusion
The lower functional outcomes seen in patients with WC were not significant after adjusting for confounders, with injury chronicity being the key factor affecting postoperative results. Furthermore, no association was detected between WC status and return-to-work metrics.
Footnotes
Final revision submitted July 8, 2024; accepted September 6, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. has received consulting fees from Websurvey. A.H. has received consulting fees from Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Groupe Hospitalier Pitie-Salpetriere (reference No. CPP IDF VI).