
Abstract
Background:
Surgical outcomes for proximal hamstring avulsion injury (PHAI) are well documented, yet comparative analyses with nonsurgical approaches remain scarce.
Purpose:
To compare the functional outcomes between surgical and nonsurgical interventions for PHAI.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This comparative study, conducted at a sports surgery center between January 2012 and July 2021, focused on patients with primary PHAI. The study was a retrospective analysis of prospectively collected data. Group selection involved utilizing propensity score matching to compare an arm of patients who were surgically treated (indications included patients with complete injury, patients with partial injury with >2 cm of retraction, and patients for whom 6 months of nonsurgical treatment failed) with another arm of patients who refused surgery. The primary outcome was evaluated using the Parisian Hamstring Avulsion Score (PHAS). The secondary outcomes included the Tegner Activity Scale (TAS) score; University of California, Los Angeles (UCLA) score; rate and quality of return to sport (RTS); and patient satisfaction.
Results:
The study included 32 patients (mean age, 55.8 years [SD, 8.4 years]) in the nonsurgical treatment arm and 95 patients in the surgical treatment arm (mean age, 53.4 years [SD, 7.7 years]) (P > .05). The interval from injury to treatment was 5.7 months (SD, 9.6 months) for the surgical group and 12.7 months (SD, 25.9 months) for the nonsurgical group (P > .05). At the final follow-up (nonsurgical group: mean, 56.5 months [SD, 28.2 months]; surgical group: mean, 50.7 months [SD, 33.1 months]), the PHAS was significantly higher in the surgical group (mean, 86.3 [SD, 13.7]) compared with the nonsurgical group (mean, 69.8 [SD, 15.1]) (P < .0001). Higher activity scores were also observed in the surgical group for the TAS and UCLA scores (P = .0224 and P = .0026, respectively). A higher percentage of the surgical group (68.4%) returned to sports compared with the nonsurgical group (46.9%) (P = .0354), with a greater proportion in the surgical group returning at the same or higher level (67.7% vs 26.7%) (P = .0069). Additionally, a higher satisfaction level was reported by patients in the surgical group (89.5%) in contrast to the nonsurgical group (25%) (P < .0001). Three patients in the surgical group experienced complications (2 reruptures and 1 hyperesthesia at the pudendal nerve territories). Odds ratios (ORs) indicated that patients in the surgical group were significantly more likely to achieve or exceed median scores for the PHAS (OR, 6.79; P < .001), TAS score (OR, 2.29; P = .045), and UCLA score (OR, 3.63; P = .003), as well as to RTS at any level (OR, 2.46; P = .031) or at the preinjury level or higher (OR, 6.04; P < .001).
Conclusion:
This study demonstrated that surgical treatment of PHAI significantly enhances long-term functional scores, including the PHAS, TAS score, UCLA score, satisfaction, and RTS, at a mean follow-up of >4 years compared with nonsurgical treatment.
Registration:
NCT02906865 (ClinicalTrials.gov identifier)
Proximal hamstring avulsion injuries (PHAIs) are debilitating injuries affecting primarily the young athletic population.7,8,18 Because of the increased sports activity among the older population, these injuries are increasingly being seen. 4 The treatment choice for PHAI is influenced by the degree of retraction, type of tear (partial or total), lesion chronicity, and associated symptoms. 13 The accepted indication for nonsurgical treatment of PHAI is a partial tear with <2 cm of retraction or patients with low functional demand.3,14,15
The outcomes of surgical treatment for PHAI have been widely reported in the literature, demonstrating benefits in terms of patient-reported outcome measures (PROMs), return to sport (RTS), and patient satisfaction.4,6,9,12,18 These studies have reported overall complication rates ranging from 0% to 50%, as documented in the systematic review by Jokela et al. 6 Additionally, specific complications such as rerupture and sciatic nerve irritation have been reported at rates of 1.2% and 3.5%, respectively.4,10 However, most of the existing literature involves descriptive studies without a control group, making these results susceptible to publication bias, and there is a significant lack of reports on nonoperative treatment outcomes or comparisons between these treatment modalities.3,4,6,18 A 2018 systematic review by Bodendorfer et al 3 highlighted this gap, noting that among the identified studies, 22 exclusively addressed operative management of PHAI, 1 study focused solely on nonoperative treatment, 5 and only 1 included both operative and nonoperative treatment groups, although it was an abstract presentation. In the same year, 2 retrospective case-control studies were published by the same research team, advocating improved outcomes with surgical treatment of complete injuries, 15 along with a 40% conversion-to-surgery rate for partial injuries of <2 cm. 14 In contrast, a recent prospective nonrandomized, nonmatched study by van der Made et al 17 reported comparable results at 1 year postoperatively between both modalities after a shared decision-making process, challenging the existing literature that advocates surgery for its benefits.
The primary aim of the study was to compare the functional outcomes of patients treated for PHAI with surgery or nonsurgically, particularly focusing on patients who opted for nonsurgical treatments despite meeting the surgical indications, as measured using the Parisian Hamstring Avulsion Score (PHAS). 11
The secondary aim involved the evaluation of additional outcome parameters including the Tegner Activity Scale (TAS) score, 16 the University of California, Los Angeles (UCLA) score,1,21 and the rate and quality of RTS, as well as patient satisfaction and perception of improvement.
Methods
Study Design
This was a single-center case-control study, conducted at a sport surgery center between January 2012 and July 2021. It is part of the French Proximal Hamstring Avulsion Surgery Cohort Study (PHAS; ClinicalTrials.gov identifier: NCT02906865).
Inclusion and Exclusion Criteria
All consecutive patients who were evaluated for the first time with primary PHAI, were indicated for surgical treatment, and chose either surgical or nonsurgical management (refused surgery) were eligible for inclusion.
Exclusion criteria included patients <18 years of age, those with a follow-up period of <1 year since treatment, patients evaluated with a bony avulsion of the ischial tuberosity, patients requiring a reconstruction using allograft augmentation, those who had undergone previous surgeries on the hamstrings, and those who were unwilling to participate in the study.
Decision-Making and Indication
A decision-making algorithm was used to guide the management strategy. Initial surgical management was offered to patients evaluated with complete avulsions or partial avulsions in which tendon retraction exceeded 2 cm or those who had persistent significant pain and weakness after 6 months of nonsurgical treatment. Patients refusing surgery were followed and treated nonsurgically.
Partial avulsion was defined as the involvement of either the conjoint tendon or the semimembranosus tendon, and complete avulsion referred to the involvement of both the conjoint tendon and the semimembranosus tendon. 4
Throughout the treatment process, a shared decision-making approach was adopted involving the patient, allowing for continuous reassessment of treatment effectiveness and adjustments based on clinical progression and patient feedback.
Technique of Nonsurgical Treatment
Nonsurgical management included resting, applying ice, undergoing physical therapy, and occasionally undergoing platelet-rich plasma injections, followed by gradually returning to normal activities over roughly 4 months. Each patient in this group followed a uniform rehabilitation protocol, beginning with early mobilization and gentle range of motion and flexibility exercises, advancing to strengthening exercises, and advancing to RTS activities within a 6- to 12-week time frame. Regular 6-week assessments were conducted to monitor the progress of rehabilitation and overall recovery. Surgical treatment was offered each time when the criteria for surgical indication were met.
Surgical Technique and Postoperative Rehabilitation Protocol
All surgical procedures were conducted under spinal anesthesia by the senior surgeon (N.L.), adhering to the method outlined by Lefevre et al. 7 After the operation, patients were equipped with an articulated knee brace adjusted to 40° of extension for the initial 3 weeks. The postoperative rehabilitation followed the protocol established by Lefevre et al, 7 starting with isometric exercises aimed at strengthening the quadriceps and hamstring muscles, maintaining a knee flexion of 30° to 45°. Gradually, an additional 10° of extension was incorporated each week. Full weightbearing activities were introduced at the 6-week mark. The rehabilitation program began with passive exercises, transitioning to active exercises after 6 weeks. By the end of this period, patients progressed to dynamic quadriceps exercises within a closed kinetic chain and active-assisted hamstring exercises. In the 12th- to 16th-week window, patients were encouraged to start brisk walking and possibly light jogging, focusing on building hamstring strength through isokinetic exercises before shifting to eccentric exercises. Typically, from the 16th to the 32nd week, athletes were able to resume their usual sports activities.
Outcome Measures and Evaluation
The primary outcome measurement was the PHAS 11 at the last follow-up after PHAI treatment as compared between both groups of the study. The PHAS is a 36-item score, grouped in 9 categories, designed to assess the functional status of patients with PHAI. It has a scale ranging from 0 to 200, which is then converted to a 100-point scale for ease of interpretation and comparison. 11
The secondary outcome measures included other outcome parameters including the TAS score 16 and the UCLA score,1,21 the rate and quality of RTS (based on patient perception), and the complication rate, as well as patient satisfaction and perception of improvement. The TAS and the UCLA activity scale are both 10-point scales used to evaluate a patient’s level of sports activity.
When significant differences emerged between the 2 groups, we determined the odds of each treatment method delivering superior outcomes. For continuous variables (PHAS, UCLA score, and TAS score), a better outcome was defined as exceeding the highest median value for each score, and the odds ratio for surpassing this threshold was computed.
For categorical variables (RTS), patients were categorized into 2 groups: those returning to sports at the same level and those who did not return or returned at a lower level. The study then determined the odds of each treatment strategy enabling a return to the same sports level.
Data Collection
Data were collected prospectively using the internet-based software WebSurvey that was accessed and filled out by both surgeons or fellows (for physical examination, imaging, and surgical findings) and patients (for descriptive characteristics and scores).
The collected data included the characteristics of the study population, such as age, sex, body mass index, level of sport, accident circumstances, time to surgery, type of rupture, and tendon retraction on MRI scans.
Acute injuries were defined as an injury presentation delay of <28 days.
Ethics Consideration
After the decision for nonsurgical versus surgical treatment, each patient provided informed consent to participate in the study. The study was approved by the local institutional ethics committee.
Participants and Sample Size
During the study time frame, 624 patients were treated surgically, and 34 were treated nonsurgically; of them, 98 were excluded (18 bony avulsion, 35 revision surgery, and 45 allograft). Of the 526 remaining patients, 105 (19.9%) were lost to follow-up. Application of the propensity score matching technique at a 3:1 ratio yielded 32 patients in the nonsurgical treatment arm and 95 patients in the surgical treatment arm (Figure 1). One patient in the nonsurgical group did not have a corresponding third match among the patients who underwent operation.
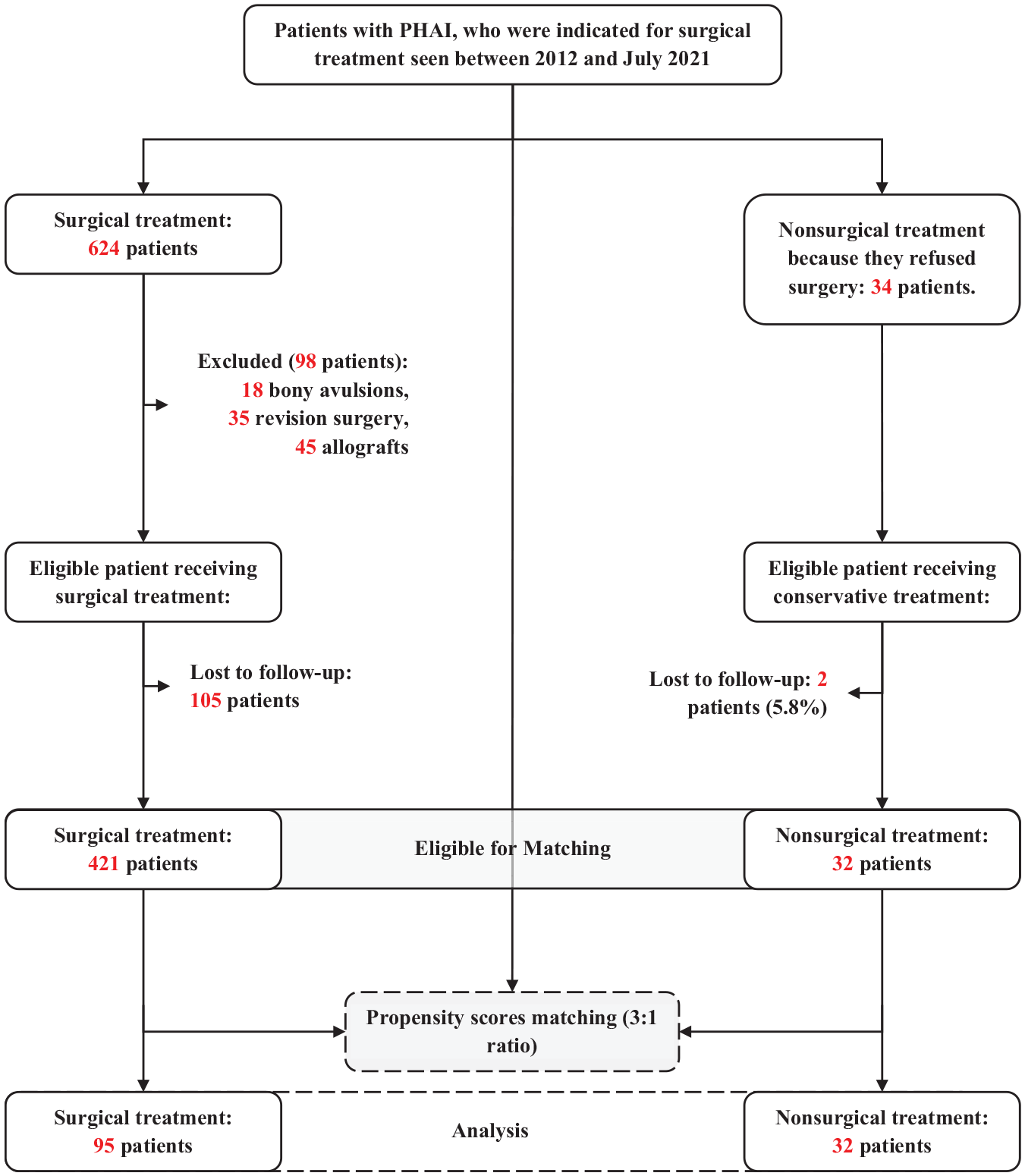
Flowchart of the study. PHAI, proximal hamstring avulsion injury.
Statistical Analysis
The study population was matched using a propensity score to minimize selection bias in the 2 groups of reconstruction techniques. Matching was performed using a logit scale with a caliper width of 0.2. The matched variables included age, sex, TAS score before injury, acute or chronic injury, type of rupture (complete or partial), and delay of follow-up.
Categorical variables, presented as frequency and percentage, were compared using the Pearson chi-square test or Fisher exact test, depending on group sizes. Continuous data, presented as mean and standard deviation, were compared using appropriate statistical tests, either the Student t test or the Mann-Whitney U test.
The functional scores were dichotomized based on their respective medians. Logistic regression analyses were conducted to determine the odds ratio of achieving the median scores and RTS within the group of patients who received an operation as opposed to the group that did not.
A P value of <.05 was considered statistically significant. All statistical analyses were performed using R software (Version 4.2; R Foundation for Statistical Computing).
Results
Patient Characteristics
In the surgical group, the mean age was 53.4 years (SD, 7.7 years), marginally lower than in the nonsurgical group, in which it was 55.8 years (SD, 8.4 years) (P > .05). The preinjury TAS and UCLA scores were similar in both groups (P > .05). The interval from injury to treatment was 5.7 months (SD, 9.6 months) for the surgical group and 12.7 months (SD, 25.9 months) for the nonsurgical group (P > .05). Chronic injuries were prevalent in both groups (Table 1). The mean follow-up period was 50.7 months (SD, 31.1 months) for the surgical group and 56.5 months (SD, 28.2 months) for the nonsurgical group (P > .05). Four patients in the surgical group initially decided on nonsurgical treatment, which failed, and then decided on surgical treatment.
Characteristics of the Study Population a
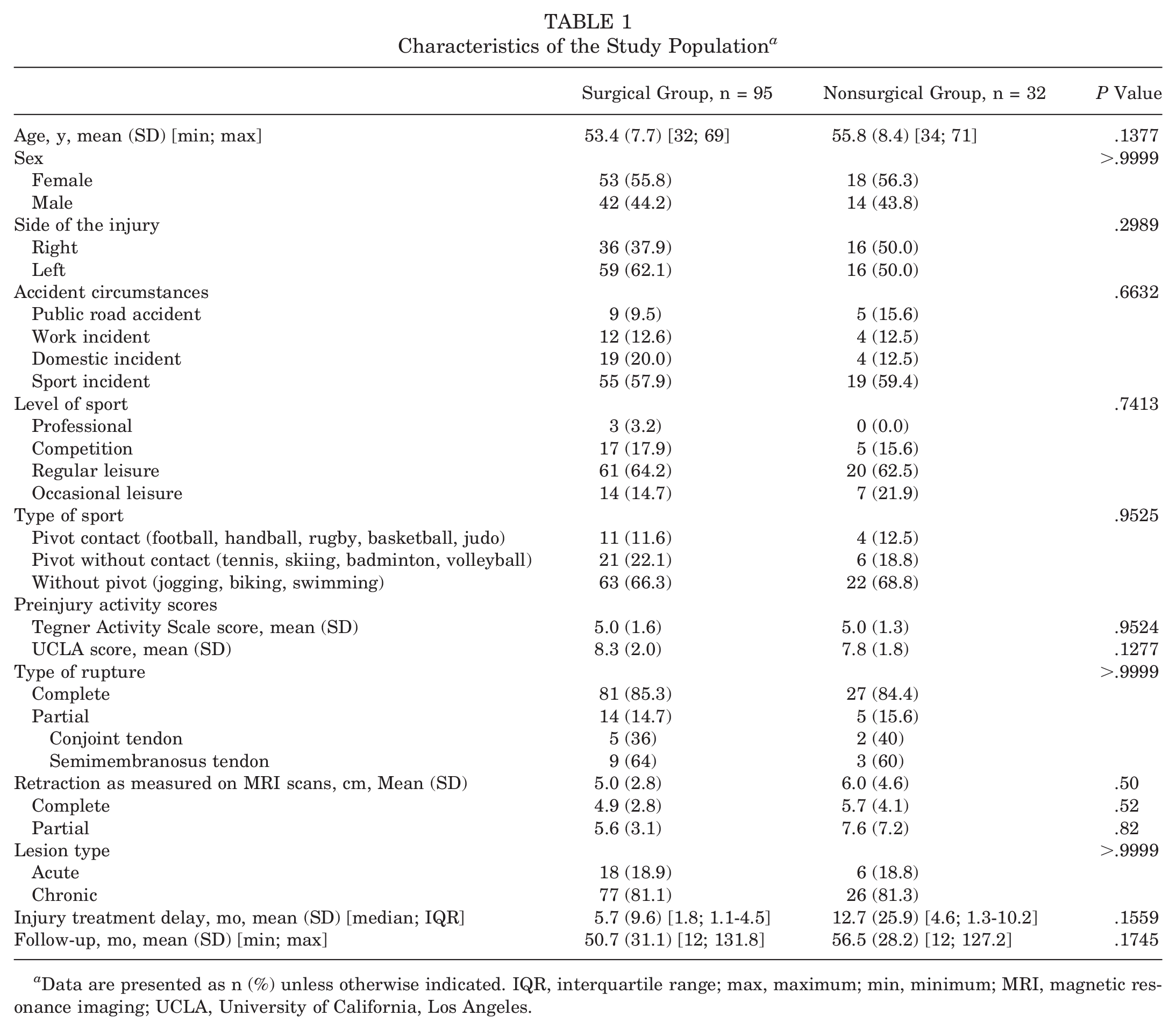
Data are presented as n (%) unless otherwise indicated. IQR, interquartile range; max, maximum; min, minimum; MRI, magnetic resonance imaging; UCLA, University of California, Los Angeles.
PHAS Values at the Final Follow-up
At the last follow-up, the PHAS was markedly higher in the surgical group (mean, 86.3 [SD, 13.7]) compared with the nonsurgical group (mean, 69.8 [SD, 15.1]; P < .0001). For complete injuries, the surgical group again had higher PHAS values (mean, 85.8 [SD, 14.4]) versus the nonsurgical group (mean, 68.3 [SD, 13.5]) (P < .0001). For partial injuries, there was a trend favoring surgical treatment, with the surgical group showing a higher mean PHAS of 89.4 (SD, 8.9) compared with 77.8 (SD, 21.8) in the nonsurgical group, although this did not reach statistical significance (P = .49) (Figure 2).
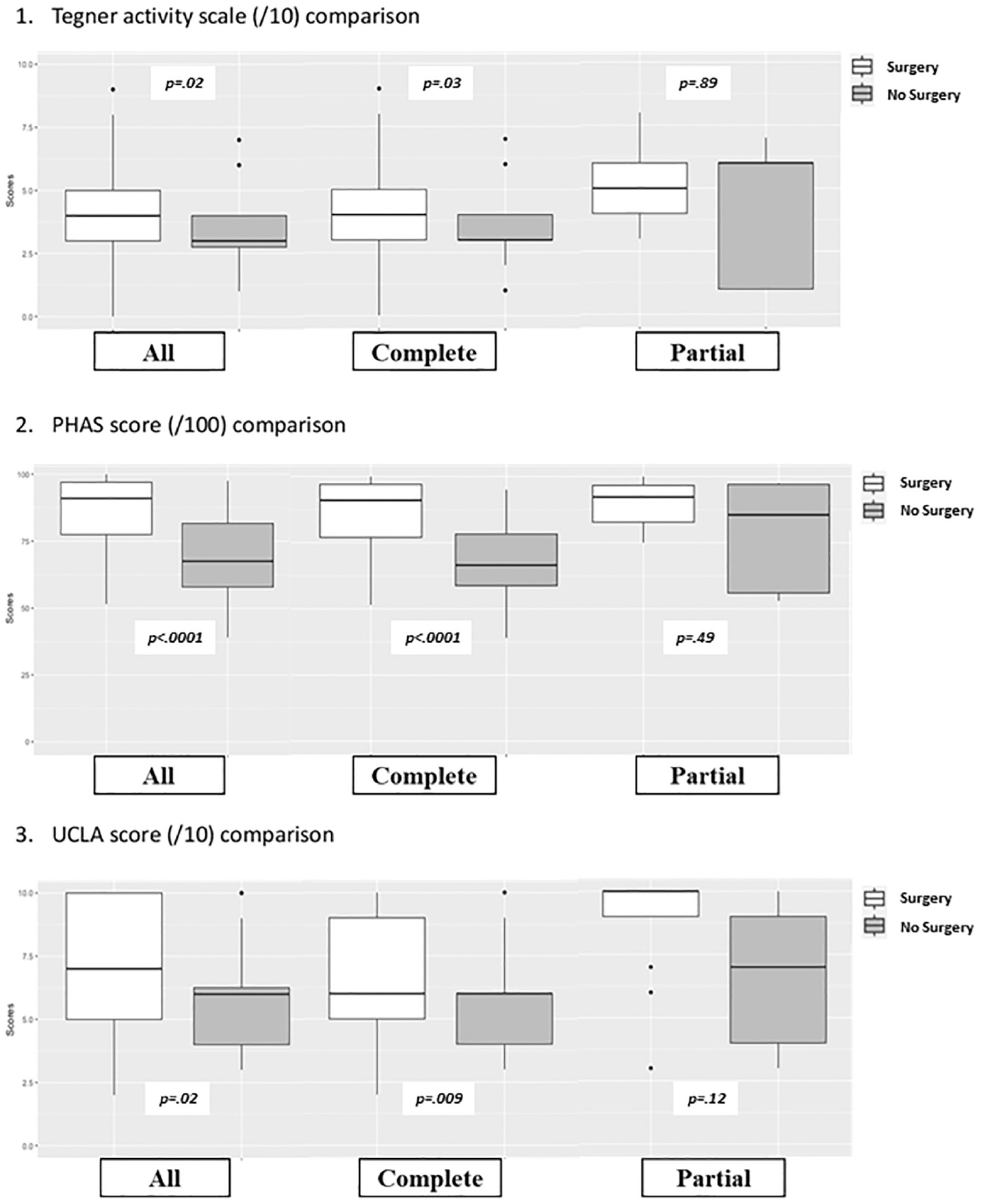
Functional outcomes at the last follow-up. PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California, Los Angeles.
Other Functional Scores and Outcomes
Activity Scores
The TAS score was significantly higher in the surgical group, with a mean of 4.2 (SD, 1.8) compared with 3.4 (SD, 1.7) in the nonsurgical group (P = .0224). Similarly, the UCLA score of the surgical group was higher (mean, 7.2 [SD, 2.4]) than that of the nonsurgical group (mean, 5.7 [SD, 2.0]) (P = .02) (Figure 2). For complete injuries, surgical group had higher TAS (mean, 4.0 vs 3.3; P = .03) and UCLA (mean, 6.9 vs 5.5; P = .009) scores compared with nonsurgical group. For partial injuries, the differences in TAS (mean, 5.1 vs 4.2; P = .89) and UCLA (mean, 8.8 vs 6.6; P = .12) scores were not statistically significant (Figure 2).
Return to Sport
The study found that 68.4% (65/95) of patients in the surgical group were able to RTS, compared with 46.9% (15/32) in the nonsurgical group (P = .0354) (Table 2). In terms of quality of RTS, 67.7% (44/65) of those who returned to sports in the surgical group were able to perform at the same or a higher level, but only 26.7% (4/15) of the nonsurgical group who returned to sports achieved the same level (P = .0069).
Return to Sport, Satisfaction, and Personal Perception of Improvement at the Last Follow-up a
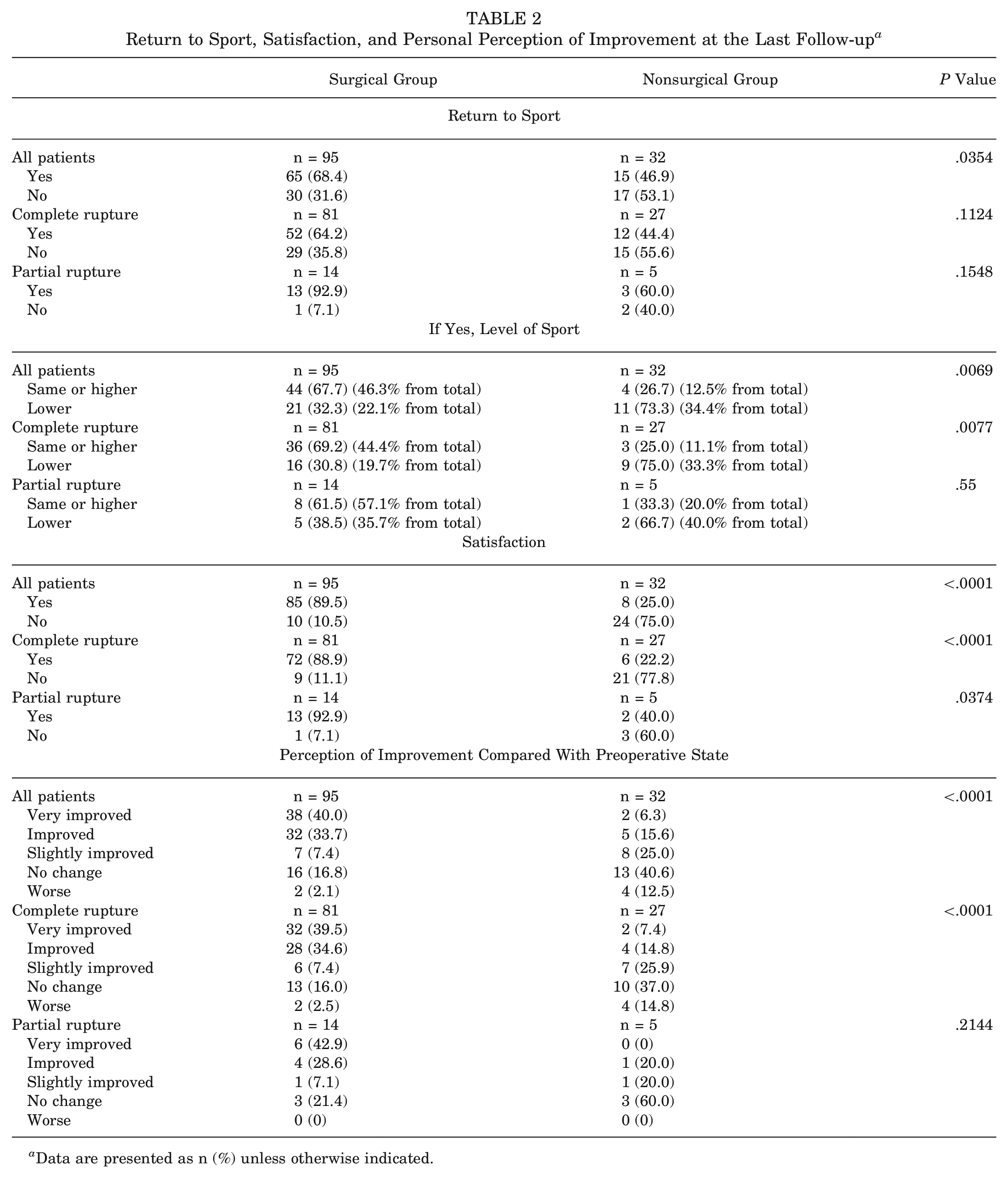
Data are presented as n (%) unless otherwise indicated.
Satisfaction
In the surgical group, a high level of satisfaction was reported by 89.5% (85/95) of the patients, compared with only 25% (8/32) in the nonsurgical group (P < .0001). Notably, a significantly larger proportion of the surgical group felt “very improved” (40.0%) or “improved” (33.7%) compared with the nonsurgical group, where only 6.3% felt “very improved” and 15.6% “improved” (P < .0001).
The details for both partial and complete injuries regarding these outcomes are delineated in Table 2. Notably, for partial ruptures, patient satisfaction emerged as the only variable with a statistically significant difference; 92.9% of the surgical group (13/14) reported satisfaction, compared with the 40.0% (2/5) of the nonsurgical group (P = .0374).
Complications
Three patients in the surgical group experienced complications: one developed a compressive hematoma that was complicated by a rerupture necessitating revision surgery; another experienced a rerupture complicated by a pulmonary embolism, which responded to nonsurgical treatment; and the third experienced pudendal nerve paresthesia, manifesting as ipsilateral hyperesthesia that resolved after 45 days of symptoms.
Odds Ratio of Achieving or Exceeding the Highest Median Scores of the PHAS, TAS Score, and UCLA Score
For the PHAS, the highest median score observed was 87.0 in the surgical group. Patients in this group had 6.79 times the odds of surpassing this score (95% CI, 2.70-19.7; P < .001) compared with those in the nonsurgical group.
Similarly, in the case of the TAS score, where the highest median score for the surgical group was 4.0, these patients had 2.29 times the odds of achieving or exceeding this median (95% CI, 1.02-5.34; P = .045) compared with the nonsurgical group.
In addition, for the UCLA score, with the surgical group having a median of 6.0, the odds of achieving or exceeding this median was 3.63 times higher in the surgical group (95% CI, 1.53-9.38; P = .003) than in the nonsurgical group.
Odds Ratio of RTS in Surgical Versus Nonsurgical Groups
The surgical group was 2.46 times more likely to return to any level of sport (95% CI, 1.09-5.64; P = .031) compared with the nonsurgical group. Furthermore, the operated group had 6.04 times the odds of returning to sport at the same or a higher level (95% CI, 2.16-21.6; P < .001) compared with the nonoperated group.
Discussion
The main finding of this study is that surgical treatment of patients with PHAIs offers better functional outcomes, as measured using the PHAS, compared with nonsurgical treatment.
This study stands out as one of the first case-control PHAI studies to use a matching technique to robustly compare outcomes of surgical and nonsurgical treatments. To our knowledge, it appears to be based on the largest sample size per treatment arm compared with existing studies.
These findings align with those of previous studies advocating surgical treatment for PHAI.2-4,7,8,19,20 Yet, the majority of the literature on this topic is composed of noncomparative studies, which tend to provide descriptive results that lack robustness, with only a handful of articles offering comparative analysis3,14,15,17 (Table 3). Interestingly, our data involved a cohort predominantly characterized by chronic PHAI, with approximately 81.7% of patients undergoing treatment a mean of 5.7 months after injury. This aspect is crucial to highlight, as it demonstrates the efficacy of surgical intervention even in a primarily chronic setting, outperforming nonsurgical treatment.
Comparative Studies Available in the Literature Comparing Surgical With Nonsurgical Treatment of PHAI a
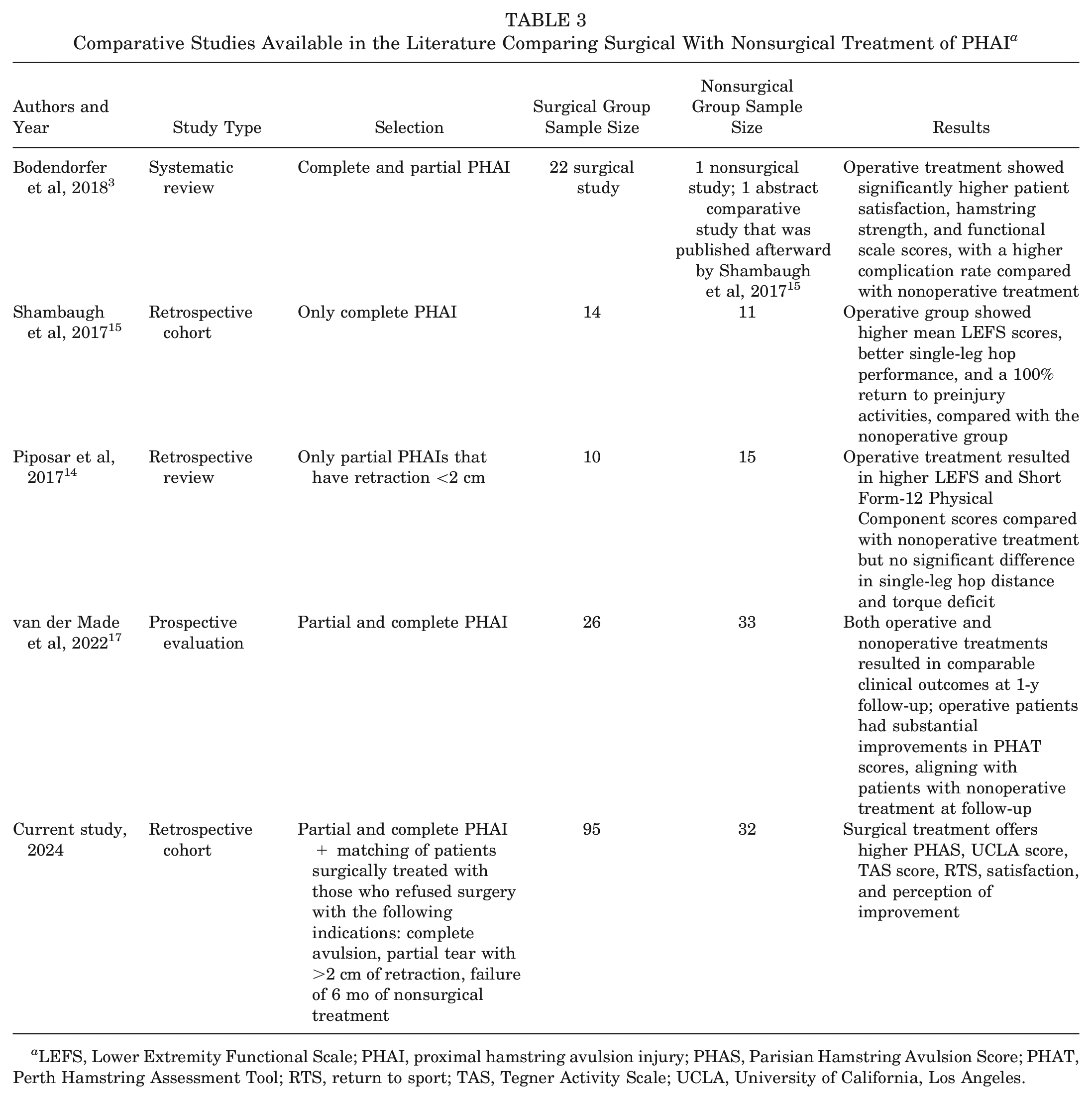
LEFS, Lower Extremity Functional Scale; PHAI, proximal hamstring avulsion injury; PHAS, Parisian Hamstring Avulsion Score; PHAT, Perth Hamstring Assessment Tool; RTS, return to sport; TAS, Tegner Activity Scale; UCLA, University of California, Los Angeles.
One of the earliest comparative studies on this topic was a nonmatched case series by Shambaugh et al 15 in 2017, focusing on patients with complete PHAIs. They compared outcomes between 14 surgically treated and 11 nonsurgically treated patients, finding higher mean Lower Extremity Functional Scale (LEFS) scores (74.71 vs 68.50) and greater strength recovery in the surgical group over a mean follow-up of 3.65 years (SD, 2.11 years). 15 In our study, predominantly involving complete PHAIs and using the PHAS, a similar trend was observed; after matching patients based on age, sex, preinjury TAS score, injury type (acute/chronic, complete/partial), and follow-up delay, the surgical treatment’s superiority was again evident. In a study by Piposar et al, 14 patients with partial PHAI tears and <2-cm retractions were evaluated (15 nonsurgical vs 10 surgical). The study found significantly better subjective PROMs (LEFS and Short Form-12 scores) in the surgical group, although objective measures like single-leg hop distance and torque deficit showed no significant difference. Notably, 40% of the nonsurgically treated patients eventually needed surgery because of persistent symptoms. The authors concluded that both treatment modalities can be offered in a similar scenario. 14
Both studies14,15 were limited by sample size and low level of evidence. Furthermore, RTS rate and quality and activity scores such as the TAS and UCLA scale were not reported. In our study, featuring a larger sample size, superior outcomes were consistently demonstrated in the surgical group across all parameters, including higher TAS and UCLA scores, along with improved rates and quality of RTS and satisfaction scores. However, the analysis of partial tears was less robust, as challenges were encountered in matching an adequate number of partial tear cases in the surgical group during the propensity score matching process. Despite this, our data did demonstrate higher satisfaction rates in patients with surgically treated partial tears.
Interestingly, our study’s findings can be contrasted with those of van der Made et al, 17 who conducted a prospective evaluation over a 1-year period including both partial and complete PHAIs and found comparable results when a shared decision-making process was utilized. However, it is important to note that their follow-up duration was limited to 1 year, and the study included 26 patients in the surgical group and 33 patients in the nonsurgical group. Their study showed no significant difference in 1-year Perth Hamstring Assessment Tool scores between groups (surgical group: mean, 80 [SD, 19]; nonsurgical group: mean, 80 [SD, 17]). It is noteworthy that they included patients without restriction to the type of injury, essentially comparing the outcomes of their decision-making strategy (eg, patients not indicated for surgery per their protocol were compared with those indicated for surgery). Contrarily, our data showed that, even when shared decision-making was applied and when patients were informed about the potential for inferior clinical outcomes with nonsurgical treatment, patients in the nonsurgical group had significantly worse results at the long-term follow-up (at the mean 3-year follow-up).
Existing indications for the treatment of PHAI are often based on isolated descriptive reports that compare their results with the existing literature. For example, Hofmann et al 5 in 2014 reported outcomes from 19 patients who underwent nonsurgical treatment for complete PHAI. Their findings showed moderate LEFS scores, reduced hamstring strength, and a slight decline in single-leg hop test performance. Despite this, the authors suggested that patients with complete injury can be treated nonsurgically initially if they accept a decline in strength. 5 Our study builds on these results, as patients in our study who refused surgery were found to have lower satisfaction scores in the long term and consistently lower PROMs.
Our study revealed a significant difference in RTS capabilities between both groups, in favor of surgical treatment (68.4% compared with 46.9%). The rate of RTS after surgery is slightly lower than that reported in literature series, with a cumulative rate of 84.5%, as reported by Hillier-Smith and Paton. 4 This may be attributable to the older mean age of our study population. Additionally, the predominance of chronic injuries in our cohort, which are traditionally linked to less favorable outcomes, 4 could further explain the lower rate of RTS observed in our study. Conversely, the literature reports less frequently on RTS after nonsurgical treatment; for instance, Hofmann et al 5 reported an RTS rate of 70.6% (12/17 patients). van der Made et al 17 reported that 33% (11/33) of patients returned to sports at the same level, but 12% (4/33) did not, with 48.48% (16/33) returning at a lower level and 6% (2/33) not having engaged in sports before surgery. Similarly, the lower rates in our study may be attributed to the older age of our study population and the extended follow-up period, which could be seen as a barrier to sports engagement in this age group.
It is noteworthy that surgical intervention carries an additional 3% risk of complications, which in this study included issues such as rerupture and paresthesia. This rate is comparable with the rate reported in the literature.4,12
Limitations
The limitations of our study include a relatively small sample size and the retrospective nature of the analysis. The lack of randomization is another limitation; however, we mitigated this through the use of matching techniques. Additionally, there was a predominance of chronic and complete injuries in this cohort, which may limit the generalizability of our findings. This suggests a need for future research that includes a broader spectrum of injuries, particularly more acute cases and more partial injuries, to enhance the applicability of the results across different patient scenarios.
Conclusion
This study demonstrated that surgical treatment of patients with complete PHAI injury and those with partial injuries and retraction of >2 cm significantly enhances long-term functional scores, including the PHAS, TAS score, UCLA score, satisfaction, and RTS, at a mean follow-up of >4 years compared with nonsurgical treatment.
Footnotes
Submitted January 21, 2024; accepted June 3, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. is a consultant for WebSurvey Society, Paris, France. A.H. is a consultant for Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Data Accessibility Statement
Data are available on reasonable request.