
Abstract
Background:
While tibial tubercle osteotomy (TTO) is a highly effective treatment for patellofemoral malalignment, some patients may have recurrent symptoms after surgery. To date, there are little data on revision TTO (rTTO) and its outcomes.
Purpose:
To evaluate the (1) reasons for and (2) complications following rTTO.
Study Design:
Case series; Level of evidence, 4.
Methods:
This was a retrospective review of patients who underwent rTTO from a single high-volume patellofemoral surgeon between 2016 and 2023. All included patients had a minimum of 3 months of follow-up data. Demographic characteristics, indications for primary and revision surgery, operative characteristics, concomitant procedures, range of motion at 6 and 12 weeks postoperatively, radiographic data, and complications were collected.
Results:
There were 16 knees (14 patients) that underwent rTTO, including 10 (63%) for persistent malignment (all of which had chondral damage requiring concomitant intervention) and 6 (38%) for fracture/nonunion. The knees undergoing rTTO for malalignment were 90% female, compared with 33% female for fracture/nonunion (P = .04). For persistent malalignment rTTO, the only complication (10% [1/10]) was arthrofibrosis (0°-65° at 6 weeks postoperatively), requiring arthroscopic lysis of adhesions (0°-140° at 12 weeks postoperatively). Within the follow-up available (median, 2.2 years; range, 9 months-5.3 years), there were no cases of new or recurrent patellar instability after rTTO. Similarly, at a median follow-up of 1.2 years (range, 4 months–3.0 years), all 6 knees that underwent rTTO for fracture/nonunion achieved union, with delayed union requiring percutaneous bone marrow grafting at 4 months postoperatively being the only complication in this cohort.
Conclusion:
Patients who underwent rTTO demonstrated low complication rates and high union rates in this study. There was a high prevalence of chondral damage requiring concomitant intervention among patients undergoing rTTO for persistent malalignment. While rTTO is a relatively rare procedure, these data suggest that it can be a safe and effective option for patients with recurrent symptoms or fracture/nonunion after primary TTO.
Patellofemoral (PF) malalignment may lead to a number of sequelae, including insidious anterior knee pain, PF chondral damage (ranging from focal PF chondral defects to diffuse PF osteoarthritis), and/or PF instability. 24 These conditions may cause significant disability and are especially prevalent in young women. 6 Originally developed to treat PF instability, 9 the tibial tubercle osteotomy (TTO) has been established as a versatile procedure that may be used to address a range of PF pathologies. 24
In the setting of isolated PF chondral pathology, an anteromedializing (AMZ) TTO may be used to directly unload the PF joint, providing direct pain relief7,11,13 or “protecting” a concomitant cartilage restoration procedure.2,24 In the setting of patellar instability, patients with a laterally positioned tibial tubercle (ie, increased tibial tubercle–trochlear groove [TT-TG] distance3,4) may benefit from an AMZ-TTO to improve patellar tracking. Similarly, in patients with concomitant patellar instability and patella alta, a TTO with distalization (TTO-d) improves patellar position within the trochlear groove, thereby increasing bony stability.12,14,19 Notably, the cause of PF instability is often multifactorial, and definitive surgical treatment may involve a combination of bony realignment, cartilage restoration, and soft tissue procedures (eg, medial PF ligament [MPFL] reconstruction [MPFLR]).
Numerous prior studies have demonstrated that TTOs are effective at achieving their aims for both symptomatic PF chondral damage and PF instability.11,16,24 Moreover, prior studies have found TTOs to be safe, with rates of major complication such as fracture, nonunion, hardware failure, and so forth, ranging from 2% to 6%.1,17,20,23 TTOs do occasionally fail to improve symptoms, however, and there is a paucity of data on outcomes and complications after revision TTO (rTTO). Therefore, the purpose of this study was to evaluate the (1) reasons for and (2) complications after rTTO.
Methods
The protocol for this study was approved by our institutional review board. This was a retrospective review of a consecutive series of patients who underwent rTTO from October 2016 to April 2023 by a single high-volume PF surgeon (S.M.S.) at a tertiary referral center. Inclusion criteria consisted of patients who underwent rTTO for any indication. Exclusion criteria consisted of <3 months of clinical follow-up. Follow-up was defined as time from surgery to our last clinical contact with the patient in the medical record. The start time was chosen because it reflected our institution’s transition to its current electronic medical record system, such that complete data were available.
Surgical Indications
Patients were divided into 2 groups based on surgical indication: (1) rTTO for malalignment or (2) rTTO for fracture/nonunion. Patients undergoing rTTO for malalignment had demonstrated a completely healed primary osteotomy site at the time of revision and were indicated for rTTO because of persistent symptoms in the setting of residual malalignment. Patients undergoing rTTO for fracture/nonunion had not demonstrated complete radiographic healing of the primary osteotomy site (eg, secondary to fracture or nonunion) and were indicated for revision in an attempt to achieve appropriate healing. All fractures/nonunions were evaluated/confirmed with computed tomography scans.
Patients with persistent malalignment underwent either anteromedializing rTTO (AMZ-rTTO) alone, rTTO with distalization (rTTO-d), combined anteromedializing rTTO with distalization (AMZ-rTTO-d), or lateralizing TTO with distalization (LAT-rTTO-d). Patients underwent AMZ-rTTO alone if they had symptomatic PF chondral damage and/or recurrent patellar instability in the setting of persistent coronal plane malignment due to a lateralized tibial tubercle (TT-TG distance, ≥15 mm) without significant patella alta (Caton-Deschamps Index [CDI], <1.3). Patients underwent rTTO-d if they experienced recurrent patellar instability in the setting of persistent patella alta (CDI, ≥1.3) without coronal plane malignment (TT-TG distance, <15 mm). Patients underwent AMZ-rTTO-d if they had symptomatic PF chondral damage or persistent patellar instability in the setting of persistent combined coronal plane malignment (TT-TG distance, ≥15 mm) and patella alta (CDI, ≥1.3). Patients underwent LAT-rTTO-d if they had symptomatic PF chondral damage and/or new medial patellar instability in the setting of coronal plane malignment due to an overly medialized tibial tubercle (TT-TG distance, ≤0 mm) and patella alta (CDI, ≥1.3). Patients undergoing rTTO for fracture/nonunion generally underwent rTTO in situ with the goal of achieving healing rather than improving alignment.
Surgical Technique
In brief, the rTTO for malalignment was performed similarly to standard TTO techniques.19,23,27 An anterolateral incision was made from the tibial tubercle to the lateral aspect of the patellar tendon insertion, incorporating the prior scar when possible and maintaining adequate skin bridges if the prior scar could not be utilized. If the primary TTO screws were present, removal of hardware was performed. For AMZ-rTTO, an approximately 30° to 45° shingle was then cut, leaving a periosteal hinge distally, and the tibial tubercle was translated anteromedially. For LAT-rTTO, the wedge-shaped shingle was cut anterolateral to slightly posteromedial at 30° and translated laterally. For distalization, electrocautery was utilized to release the periosteum lateral and medial to the tibial tubercle. The periosteum was cut distally at 5 cm from the tubercle and a periosteal elevator was used to peel the periosteum distally to 6 cm. A wedge-shaped shingle was cut with a sagittal saw to create a 5-cm wedge-shaped shingle, with a second cut at approximately 6 cm. The distal bone fragment was removed, and an Evans wedge was cut down to the corresponding amount of distalization and tamped into the proximal aspect of the osteotomy, creating a bony buttress. The bony fragments excised from the distal tip of the osteotomy were placed in the medial and lateral aspects of the osteotomy as an autograft. For all techniques, the tibial tubercle was secured with 2 screws utilizing a lag technique through the tibial tubercle aiming 15° distally. 27 Fluoroscopy was used to confirm the screw length and position.
The rTTOs for fracture or nonunion were handled on a case-by-case basis but generally encompassed the following principles: debridement of the fracture site while maintaining bone stock, removal of hardware from any ununited pieces and maintenance of hardware in areas of bony union, re-creation of appropriate alignment of the shingle and/or fragments, maintenance of the periosteum, and creation of compression across the fragments with fixation. Depending on the case, hardware constructs varied significantly based on fixation requirements and included screws, longitudinal one-third tubular plates, transverse contoured 2.4-mm and 2.7-mm plates, suture cerclage, and suture anchor augmentation. Additionally, biological augmentation was performed via a combination of iliac crest bone graft, bone marrow aspirate concentrate, demineralized bone matrix putty, and/or bone morphogenic protein (BMP) augmentation as indicated by the specific case.
When concomitant procedures were performed, sequencing generally was as follows: knee arthroscopy with or without knee arthrotomy, with or without patellar-sided MPFL anchor placement, with or without cartilage restoration procedures (eg, rTTO), with or without femoral-sided MPFL tunnel placement and fixation.
Postoperative Management
AMZ-rTTO patients were nonweightbearing with the brace locked in extension for ambulation for 4 weeks, whereas patients with rTTO-d, AMZ-rTTO-d, LAT-rTTO-d, and fracture/nonunion revision were nonweightbearing with the brace locked in extension for ambulation for 6 weeks (1 patient with fracture/nonunion was cylindrically casted). The brace was worn during sleep for the first week for all patients. In the majority of cases, physical therapy began 1 week postoperatively (2-3 times per week), and the crutches and brace were eventually discontinued under physical therapy supervision after the aforementioned time periods were met. A continuous passive motion machine was used for all patients with a concurrent cartilage restoration procedure. Aspirin 81 mg daily was prescribed for deep vein thrombosis (DVT) prophylaxis for most cases; rivaroxaban 10 mg daily or aspirin 325 mg daily was used in a subset of higher-risk patients.
Data Collection
The electronic medical records were retrospectively reviewed. Patient characteristics that were collected included age, sex, body mass index (BMI), laterality, smoking status, and oral contraceptive use. Preoperative characteristics included indication for index surgery, concomitant procedures performed at the time of index surgery (when available), indication for revision surgery, time from primary to revision surgery, radiographic healing of the primary TTO, TT-TG distance as measured on preoperative axial magnetic resonance imaging (MRI) scans, 29 and CDI as measured on sagittal preoperative MRI scans. Operative characteristics included the rTTO technique utilized, concurrent procedures, number and size of screws for shingle fixation, amount of medialization (in mm), amount of distalization (in mm), and tourniquet time. Postoperative characteristics included DVT prophylaxis regimen, weightbearing status, rehabilitation protocol, length of clinical follow-up, and time from rTTO to data collection.
The primary outcome measure was overall complication rate. Complications included reoperation, nonunion, delayed union, arthrofibrosis, DVT, broken hardware, fracture, wound complications, sensory deficits, fascial hernia, hematoma, or quadriceps dysfunction. Removal of hardware after complete healing is standard of care in our clinical practice and was not considered a complication. Secondary outcomes included range of motion (ROM) at 6 weeks and 12 weeks postoperatively as measured by the attending surgeon.
Statistical Analysis
Categorical variables are reported as frequencies with percentages, and continuous variables are reported as means or medians with ranges, as appropriate. Differences in demographic variables between patients who underwent rTTO for malalignment versus fracture/nonunion were compared using Fisher exact tests or Student t tests, as appropriate. A P value < .05 was considered statistically significant. All statistical analyses were performed in SAS Version 9.4 (SAS Institute).
Results
There were 16 knees (14 patients) that underwent rTTO during the study period: 10 (63%) for persistent malignment and 6 (38%) for fracture/nonunion. The overall cohort characteristics and a comparison between knees that underwent rTTO for malalignment versus fracture/nonunion are shown in Table 1. The majority of the knees (69%) were female; however, male knees were significantly more likely to undergo rTTO for fracture/nonunion than malalignment (67% vs 10%; P = .04). The mean time to revision was also significantly different: 12.3 years (range, 8 months-21 years) for persistent malalignment compared with 1.8 years (range, 1 month-9.4 years) for fracture/nonunion (P = .01). When excluding 1 outlier patient who had a fracture 9.4 years after primary surgery, the mean time to revision in the fracture/nonunion cohort was 3.5 months (range, 1-5 months; P < .001 in comparison with the persistent malalignment group). Eleven (69%) of the primary surgeries were performed for a chief complaint of patellar instability (7 of which had confirmed concurrent MPFLR, 3 of which had a concurrent lateral release without MPFLR, and 1 for which concurrent surgical procedures were unavailable), while 5 (31%) were performed for a chief complaint of isolated symptomatic chondral damage. The primary surgeon in this study performed the original surgery for 4 of the 6 knees undergoing rTTO for fracture/nonunion, while the primary surgeries for all 10 malalignment revisions were performed by surgeons who are not authors of the paper.
Cohort Characteristics Overall and According to Reason for rTTO a
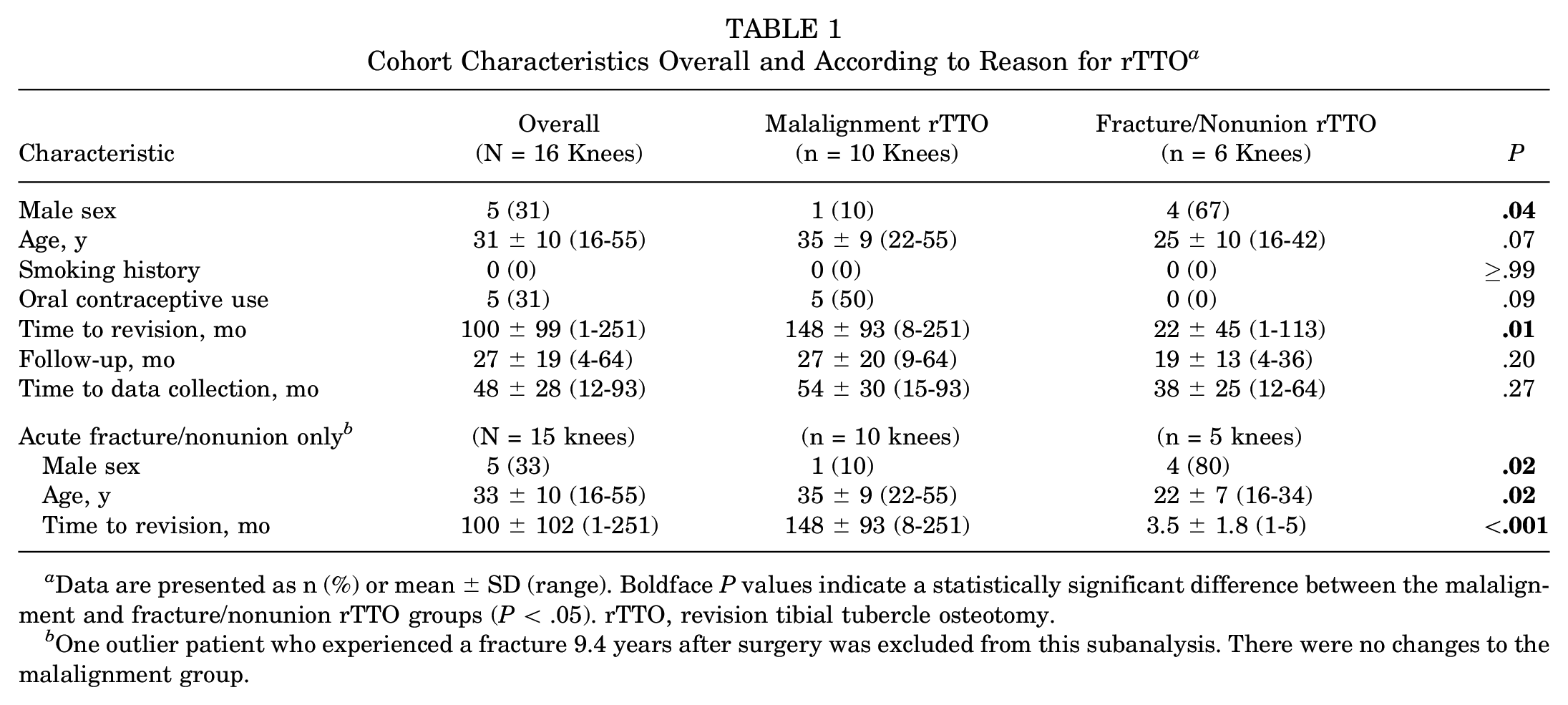
Data are presented as n (%) or mean ± SD (range). Boldface P values indicate a statistically significant difference between the malalignment and fracture/nonunion rTTO groups (P < .05). rTTO, revision tibial tubercle osteotomy.
One outlier patient who experienced a fracture 9.4 years after surgery was excluded from this subanalysis. There were no changes to the malalignment group.
Malalignment rTTO
Overall, 9 of the 10 (90%) rTTOs or persistent malignment occurred in female knees. All 10 knees demonstrated PF pain, and 6 (60%) knees demonstrated recurrent PF instability (5 lateral instability, 1 medial instability). All 10 rTTOs underwent concurrent procedures to address articular cartilage. Five knees underwent concurrent osteochondral allograft (OCA) procedures (2 patella, 2 trochlea, and 1 patella and trochlea), 2 knees underwent patellar matrix-induced autologous chondrocyte implantations, 2 knees underwent trochlear juvenile particulated cartilage (1 case concurrent with trochlea OCA), and 1 knee underwent PF joint arthroplasty. Six (60%) knees (all 6 of the cases with recurrent instability) underwent concurrent MPFLRs with hamstring allograft. One (13%) knee underwent concurrent distal femur osteotomy for severe genu valgum.
Among the rTTOs for persistent malalignment, 5 (50%) knees underwent AMZ-rTTO, 3 (33%) knees underwent AMZ-rTTO-d, 1 (10%) knee underwent rTTO-d, and 1 (10%) knee underwent LAT-rTTO-d. Nine of the 10 (90%) knees underwent fixation with two 4.5-mm screws, while two 3.5-mm screws were utilized for 1 (10%) knee. The mean tourniquet time was 79 minutes for the entire procedure. Table 2 shows the preoperative alignment and postoperative realignment measurements by rTTO type.
Preoperative Alignment Measurements and Amount of Operative Realignment for Malalignment rTTO (n = 10 Knees) a

Data are presented as means unless otherwise noted. CDI, Caton-Deschamps Index; rTTO, revision tibial tubercle osteotomy; TT-TG, tibial tubercle–trochlear groove.
The mean follow-up was 2.7 years (median, 2.2 years; range, 9 months-5.3 years). The mean ROM at 6 weeks after rTTO was 1° to 103° (extension range, 0°-10°; flexion range, 65°-125°) (Table 3). The mean ROM at 12 weeks was 0° to 130° (extension, 0° for all; flexion range, 120°-140°). All (100%) rTTOs for malalignment achieved union. The only complication (10% [1/10]) was arthrofibrosis (65° of flexion at 6 weeks), which was successfully treated with arthroscopic lysis of adhesions (0°-140° at 12 weeks). Within the follow-up available for this cohort, there were no cases of new or recurrent patellar instability after rTTO in the records examined.
Outcomes After Malignment rTTO (n = 10 Knees) a
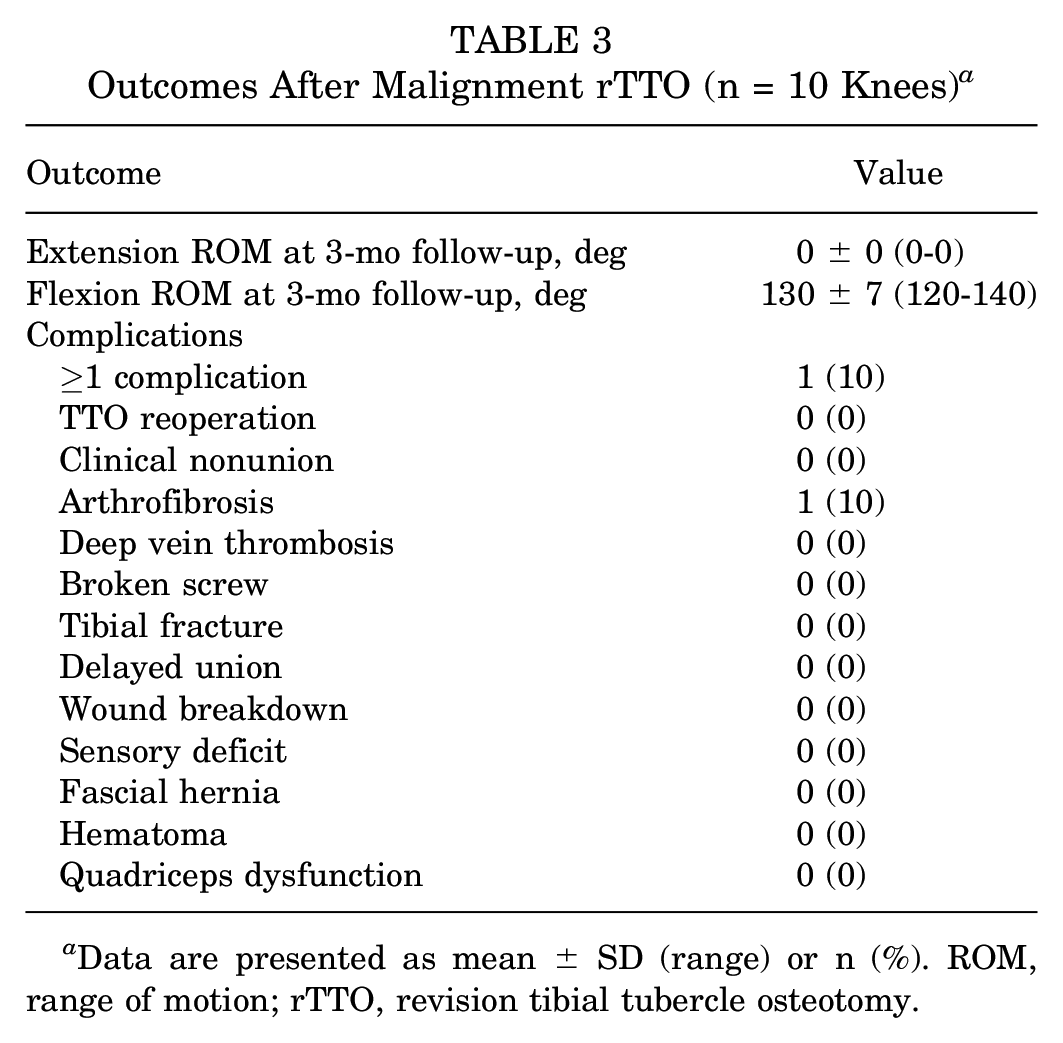
Data are presented as mean ± SD (range) or n (%). ROM, range of motion; rTTO, revision tibial tubercle osteotomy.
Fracture or Nonunion rTTO
Five of the 6 (83%) rTTOs for fracture/nonunion were performed within 6 months of the primary surgery (mean time from primary surgery for those 5 knees, 3.5 months), while 1 was performed 9.4 years after the primary surgery. Three (50%) patients sustained direct trauma to the knee resulting in fracture of the shingle/tubercle (2 within 3 months of primary surgery, one 9.4 years after primary surgery), 1 (16.7%) patient sustained a nonunion of the osteotomy site, 1 (16.7%) patient demonstrated partial union with incomplete healing of the proximal aspect of the osteotomy at 3 months postoperatively (with no additional bony bridging after 2 additional months of nonoperative measures), and 1 (16.7%) patient demonstrated screw cutout within 6 weeks of the primary TTO. Each patient underwent revision fixation tailored to their specific injury pattern with various types of augmentation, as discussed above. The patient who was evaluated with a fracture 9.4 years after primary surgery underwent concurrent application of juvenile particulated cartilage for a patellar chondral defect; no other patients with fracture/nonunion underwent concurrent cartilage procedures. Serum 25-hydroxyvitamin D levels were available for all patients other than the 2 who sustained direct trauma to the tubercle <3 months after surgery; the median level was 25.0 ng/mL (range, 12.8-55 ng/mL), with 3 of the 4 patients having vitamin D levels <30 ng/mL.
The mean follow-up was 1.6 years (median, 1.2 years; range, 4 months-3.0 years). Five of the 6 (83%) patients achieved union after the rTTO alone. The patient with primary nonunion at the osteotomy site had persistent lack of healing 4 months after rTTO; the patient then underwent percutaneous autologous bone marrow grafting at this time. The patient subsequently went on to heal and was cleared for full activity. There were no other complications in this patient cohort. At the final follow-up, all patients (6/6) demonstrated complete healing. There were no cases of recurrent fractures or nonunion after rTTO.
Discussion
The principal findings of the current study were as follows. In a small cohort of patients treated by an experienced PF surgeon, (1) rTTO for symptomatic persistent malalignment was associated with low complication rates, no episodes of recurrent instability, and high union rates; (2) patients undergoing rTTO for persistent malalignment had high rates of PF chondral damage (100%), with many also experiencing recurrent patellar instability (60%); (3) rTTOs for fracture/nonunion had a low complication rate and high union rate; and (4) rTTO for nonunion/fracture appeared to occur more commonly in young male patients. These results have a number of implications for sports medicine surgeons moving forward.
The most important finding of this study was the low complication rate and high union rate after rTTO. Complications after primary TTO have also been found to be relatively rare in the literature. In a systematic review of 787 primary TTOs by Payne et al, 20 the overall complication rate was 4.6%, with refracture (1%), nonunion (0.8%), and wound complications (0.8%) being the most common. Similar findings were seen in a meta-analysis by Knapik et al. 12 The current study extends these findings to the revision setting. While the exact incidence of these complications cannot be determined given the relative rarity of both complications and rTTO surgery, the results of the current study demonstrate that complications are not substantially more common when performing rTTO rather than primary TTO. The only complication seen in the current study for patients undergoing rTTO for malalignment was arthrofibrosis at 6 weeks postoperatively (65° of flexion in 1 patient with concurrent cartilage repair), which was successfully managed with arthroscopic lysis of adhesions (140° at 12 weeks). Of note, this was one of the first cases in our cohort, and we previously did not start physical therapy until the 4- to 6-week time point; we changed our protocol to start physical therapy at the 1-week time point and have had no subsequent instances of arthrofibrosis. Notably, neither of the prior systematic reviews reported the overall incidence of arthrofibrosis after TTO, which may be related to prior studies not classifying this as a formal complication. A recent single-institution study by Lundeen et al, 17 however, did report a 10.4% incidence of arthrofibrosis after primary TTO, consistent with the 10% rate seen in the current study. Taken together, our results suggest that rTTO can be performed safely in carefully indicated individuals.
With respect to union rate, rTTO yielded a 100% rate of osseous union for both persistent malalignment and fracture/nonunion in this series. This is particularly noteworthy because if rTTOs had demonstrated a high risk of nonunion, performing them for persistent malalignment might not be worth the risk. Similarly, all fracture/nonunion rTTOs in our cohort ultimately healed. These patients are generally faced with no other option but to undergo revision surgery as they either have experienced failure or are unlikely to heal on their own. Nevertheless, we recognize the technical demands of these procedures, often performed in patients with complex PF pathologies, and the risks and benefits of rTTO should be considered carefully and discussed at length with patients in the clinical setting.
The patients in this cohort were most commonly experiencing significant PF defects requiring cartilage restoration, with 60% of malalignment rTTOs also experiencing recurrent patellar instability. While controversy exists regarding whether TTO should be performed concurrently with MPFLR in the setting of PF malalignment,5,15,18,21 prior studies have suggested that there is a lower rate of recurrent instability and reoperation if TTO is also performed.8,10,22 For example, in a recent large database study of 3480 isolated MPFLRs and 615 MPFLRs with TTO, Ryan et al 22 found that the addition of TTO to MPFLR was associated with a >50% reduction in revision MPFLR surgery. To this end, patients with persistent malalignment and concurrent instability after primary TTO may be indicated for rTTO. In our study, all patients undergoing rTTO for malalignment had elevated TT-TG distances and/or CDIs, and after addressing this persistent malignment, there were no subsequent episodes of recurrent instability within the follow-up available in this study. Similarly, there is strong support for addressing malalignment in the setting of PF cartilage restoration,2,24,25 and all patients in our cohort undergoing rTTO for malalignment underwent concurrent procedures to address PF chondral damage. Although it is difficult to know the exact natural history of the cartilage wear these patients experienced, these findings highlight the risk of chondral damage in patients with PF malalignment and may underscore the importance of achieving adequate correction with primary TTO.
While this study was not designed to assess risk factors for requiring rTTO, the demographic breakdown observed in our study was noteworthy. Namely, patients undergoing rTTO for fracture/nonunion were significantly more likely to be men than women. Patients undergoing rTTO for a fracture/nonunion in the acute period were also significantly younger than patients undergoing rTTO for persistent malalignment. It could be theorized that young men are at a higher risk of nonunion/fracture after TTO for both behavioral and physiological reasons. Namely, adolescents may have a greater propensity to disregard medical advice, 26 while men may have greater quadriceps muscle strength and body weight, both increasing force across the osteotomy site. Future work should formally investigate this relationship, and if it does bear out, young male patients may need to be specifically counseled or have modified rehabilitation programs to help prevent fracture/nonunion after primary TTO.
There are little data on the overall incidence of rTTO. In the aforementioned study by Ryan et al 22 of a national sample of 615 patients with patellar instability undergoing MPFLR with TTO, there was only a 0.8% incidence of revision MPFLR. The need for rTTO was ostensibly much lower. In a study of 183 primary TTOs by 35 surgeons at a single institution, Gorbaty et al 8 reported 4 (2.2%) revisions for nonunion, 2 (1.1%) revisions for tibial tubercle fracture, and 1 (0.5%) revision for persistent malalignment. The relatively higher nonunion rates in that study compared with prior systematic reviews12,20 may have been related to the large number of surgeons performing a low volume of surgeries, with some performing as few as one. 8 While there is limited evidence on the optimal management of delayed or nonunion TTOs, when patients are evaluated with nonunion or fracture recalcitrant to nonoperative measures, the current results suggest that improved alignment and bony union can be achieved with rTTO.
Importantly, 1 patient with fracture/nonunion did experience delayed union, which was successfully managed with percutaneous autologous bone marrow grafting. Although the complexities of this case are beyond the scope of the current study, achieving union in this patient was expected to be a substantial challenge, and various tools used included preoperative metabolic bone evaluation, intraoperative use of BMP-augmented bone graft, and postoperative utilization of bone stimulation and teriparatide treatment. Notably, while teriparatide was intended to start immediately postoperatively, insurance approval could not be obtained until 6 weeks postoperatively, and it is conceivable that earlier treatment may have made a difference. Nevertheless, when evidence of substantial union was not seen by the 4-month postoperative time point, fluoroscopically guided closed injection of bone marrow aspirate concentrate was performed at the osteotomy site, and union was ultimately achieved in this patient without any additional surgery.
Limitations
There are several limitations to this study. As a retrospective observational study, it is not able to support any causal conclusions. 28 Nevertheless, to our knowledge, this is the largest cohort of rTTOs described to date, and this study is the first to report on rTTO in patients experiencing recurrent symptoms or fracture/nonunion, providing valuable information about the safety and efficacy of this procedure. Next, given the rarity of rTTO, sample size was inherently limited. However, these cases are from a high-volume PF surgeon, and obtaining a substantially larger sample would likely require a large database study, which has its own inherent limitations and may not be able to capture valuable information (eg, preoperative radiographic alignment, specific concurrent cartilage procedures, and postoperative ROM). Nonetheless, while this study suggests that complications are not overwhelmingly common, the individual complication rates in this study cannot be interpreted as the exact complication rates after rTTO given the limited sample size. Relatedly, long-term follow-up was unavailable, and the long-term complication rate could be slightly higher than seen here. Additionally, follow-up was based on our last clinical contact with the patient in the medical record (rather that patient telephone calls), and it is possible patients that could have sought care elsewhere after we saw them last. Furthermore, subjective patient-reported outcome data were not available. Finally, these results may not be generalizable for surgeons who perform fewer primary and rTTOs.
Conclusion
Patients who underwent rTTO demonstrated low complication rates and high union rates in this study. There is a high prevalence of chondral damage requiring concomitant intervention among patients undergoing rTTO for persistent malalignment. While this is a relatively rare procedure, these data suggest that rTTO can be a safe and effective option for patients with recurrent symptoms or fracture/nonunion after primary TTO.
Footnotes
Final revision submitted July 29, 2024; accepted August 30, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.H.G. has received research support from Cartiheal, JRF Ortho, Moximed, Organogenesis, and Vericel; consulting fees from Bioventus, Flexion Therapeutics, JRF Ortho, Moximed, Smith & Nephew, and Vericel; nonconsulting fees from Bioventus, Flexion Therapeutics, Moximed, Organogenesis, Smith & Nephew, Linvatec, Pacira Pharmaceuticals, and Vericel; honoraria from JRF Ortho and Fidia Pharma USA; royalties from Organogenesis; and has stock/stock options in Engage, Smith & Nephew, and Stryker. S.M.S. has received research support from Miach and Vericel; consulting fees from Flexion Therapeutics, Miach, Smith & Nephew, and Vericel; nonconsulting fees from Miach and Smith & Nephew; honoraria from JRF Ortho and Vericel; and stock/stock options in Engage and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital for Special Surgery (reference No. 2020-2123).