
Abstract
Objective. To measure the sagittal alignment of the tibial tubercle through the sagittal tibial tubercle–trochlear groove (sTTTG) distance in patients with and without patellar chondral lesions. Design. Patients treated with patellofemoral cartilage restoration or repair procedures were retrospectively reviewed (group 1; N = 17). A control group of patients (group 2; N = 20) undergoing partial meniscectomy with normal patellar cartilage was included. An asymptomatic patellar chondrosis group (group 3; N = 15) was identified as patients undergoing partial meniscectomy with patellar cartilage wear. The sTTTG was measured on the preoperative axial T2 magnetic resonance imaging (MRI) sequence. The first point was the nadir of the anterior trochlear cartilage, and the second point was the anterior tibial tubercle. A line was drawn between these points, perpendicular to the posterior condylar axis. Comparisons were made between the 3 groups using analysis of variance testing with Bonferroni corrections. Significance was defined as P < 0.05. Results. The mean sTTTG was significantly more posterior in group 1 (5.9 ± 5.5 mm posterior to the trochlear groove) relative to group 2 (0.8 ± 5.3 mm posterior; P = 0.018). The mean value for group 3 (2.7 ± 5.3 mm posterior) fell between group 1 and 3 but was not significantly different from group 1 (P = 0.31) or group 2 (P = 0.89). There were no significant differences with regards to sulcus angle, Caton-Deschamps Index, TTTG, or knee flexion angle on the MRI scan. Conclusions. A more posteriorly positioned tibial tubercle was observed in patients with patellar cartilage lesions relative to those with intact patellar cartilage. Intermediate positioning was observed in patients with asymptomatic patellar chondral wear. Level of Evidence. Level 3 diagnostic study.
Introduction
Anterior knee pain (AKP) is a common complaint, responsible for over 7% of orthopedic clinic visits. 1 In a high percentage of AKP patients, the pain may be assigned to the patellofemoral (PF) articulation. This pain negatively influences participation in athletic activities, with 74% of patients limiting or stopping their activities due to patellofemoral pain. 2 Though multifactorial, a subset of patellofemoral pain may be attributed to a cartilage defect. 3 Isolated chondral lesions of the patella have been reported in over 20% of patients younger than 40 years undergoing knee arthroscopy. 4 When symptomatic, these lesions may be successfully treated with a wide range of therapeutic strategies; however, the etiology for development of isolated patellar chondral lesions remains unclear in some patients and may be the first expression of a genetic predisposition to cartilage wear.
Common treatments for patellar cartilage defects can include cartilage transplantation as well as tibial tubercle osteotomies (TTO). The purpose of the TTO is to offload the cartilage defect as has been demonstrated by many authors. Similarly, the outcomes of cartilage transplantation or TTO alone are inferior to the combination of the 2 procedures.5,6 While TTOs are commonly performed with PF cartilage restoration, this osteotomy lacks guiding metrics, including measurements in non-affected patients, measurements in affected patients, and guidance for amount of correction to perform.
Tibial tubercle positioning is an anatomic factor that is known to contribute to abnormalities at the PF joint.7,8 Lateralization of the tibial tubercle is one risk factor for recurrent lateral patellar instability and in cases with distal-lateral cartilage wear this has been assigned to excessive lateral loading. 7 The tibial tubercle–trochlear groove (TTTG) and tibial tubercle-posterior cruciate ligament (TTPCL) distances are measurements (computed tomography [CT] or magnetic resonance imaging [MRI]) to gauge the magnitude of lateralization and help guide surgical treatment decisions.7-9 An additional risk factor for developing patellofemoral arthritis is increased patellar height (patellar alta). This decreases the overall amount of contact area leading to increased stress (force per unit of area) on the patellofemoral articulation. Surgical interventions have sought to optimize the PF forces through distalizing, proximalizing, medializing, anteriomedialing, and straight anteriorizing. Maquet 10 was the first to suggest anteriorizing the tibial tuberosity would decrease PF contact forces. Similarly, a relatively posteriorized tibial tubercle may affect the loading of the patellofemoral joint as suggested by the predictable development of PF arthritis after posterior medialization as in the case of the ill-fated Hauser procedure. 11
The purpose of this study is to measure the sagittal alignment of the tibial tubercle (sTTTG) relative to the femoral trochlea in patients with and without arthroscopically confirmed patellar chondral lesions. Concurrently, other factors such as patellar height, sulcus angle, and knee flexion angle will also be determined. We hypothesize that the sTTTG would be significantly larger (relatively posteriorized tibial tubercle) in patients with patellar chondral lesions relative to those with intact patellar cartilage with all other measures being equal.
Methods
Surgical case logs of 2 senior authors at a single institution were searched retrospectively to identify patients with PF cartilage repair or restoration procedures between October 2010 and August 2017 (group 1). A total of 38 knees in 35 patients were identified. For patients with bilateral involvement, 1 knee was selected at random for inclusion. Patients were excluded if there was a history of patellar instability (N = 7), knee flexion angle greater than 10° on MRI scan (N = 8), or no available MRI for review (N = 3). Patients did not have any significant radiographic changes and defects were focal as seen on MRI. A separate control group (group 2; N = 20) was identified who had undergone knee arthroscopy and partial meniscectomy within this time frame and with normal patellofemoral cartilage as verified by arthroscopy. We also identified a group of patients (group 3; N = 15) who underwent arthroscopic treatment for partial meniscectomy and were noted to have asymptomatic patellar chondral abnormalities. All procedures were approved by our institutional review board.
Preoperative MRI studies were reviewed for all patients. The sTTTG distance was measured on the axial T2 sequence ( Fig. 1 ). The first point was identified at the nadir of the trochlear groove, on the anterior surface of the trochlear cartilage, and the second point was marked at the anterior aspect of the tibial tubercle. A line was drawn between these points, perpendicular to the posterior condylar axis ( Fig. 2 ). This measurement was performed independently by 2 orthopedic surgeons with fellowship training in sports medicine. One reviewer made all measurements twice, separated by at least 2 weeks.
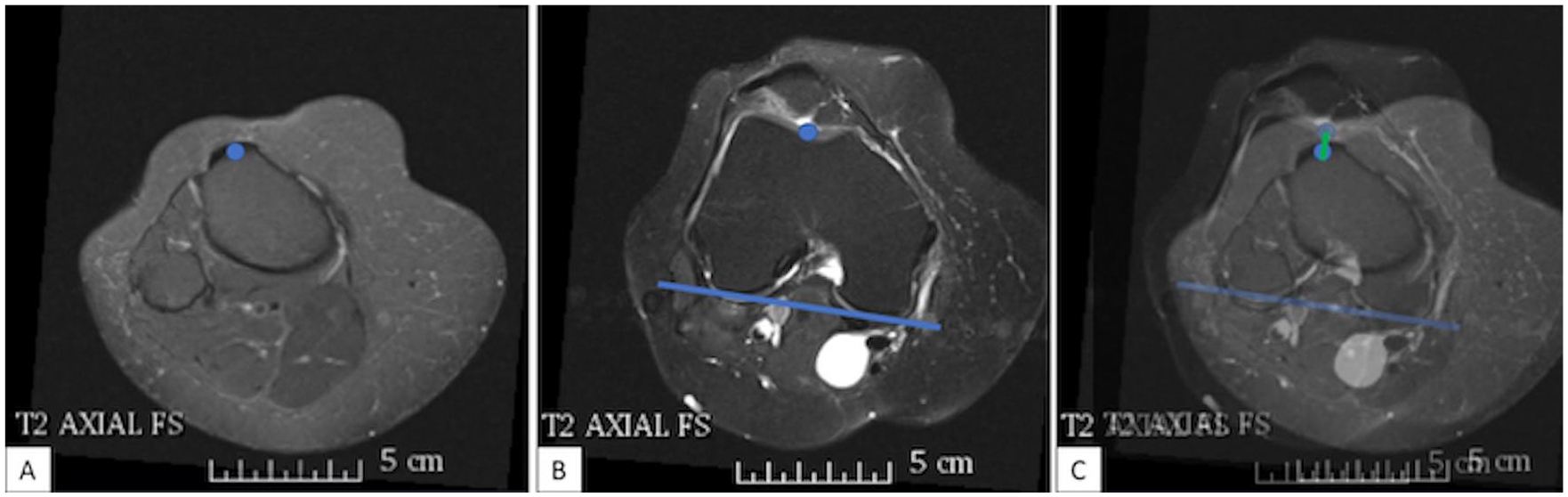
The measurement of the sagittal tibial tubercle–trochlear groove (sTTTG) distance is outlined. First, the central aspect of the tibial tubercle is marked (
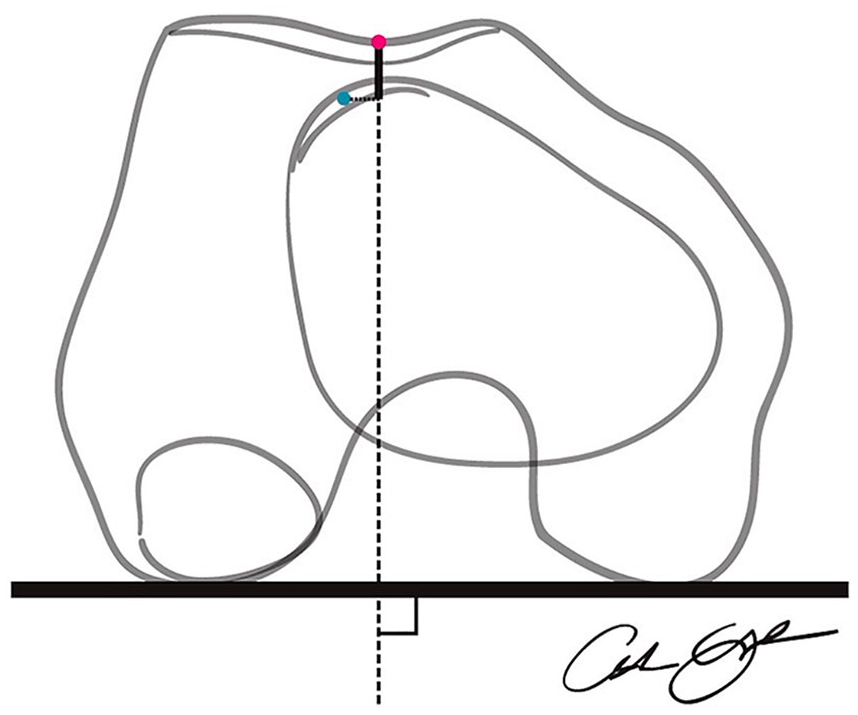
A schematic is shown for drawing the sagittal tibia tubercle–trochlear groove (sTTTG) measurement. The distance in the anteroposterior plane between the tibial tubercle and the cartilage of the femoral trochlea is measured as a representation of the sagittal alignment of the patellofemoral joint.
Additional measurements on the MRI were performed by a single observer and included the standard tibial tubercle–trochlear groove distance (TTTG) and sulcus angle. The knee flexion angle was measured on the mid-sagittal image as the angle subtended by the long axes of the femur and tibia. Caton-Deschamps Index (CDI) was measured on preoperative radiographs to assess patellar height.
Demographic information was collected for all patients, including age, sex, height, weight, and body mass index. From the operative report, the size and grade of the patellar cartilage lesion was recorded for the PF cartilage repair group and verified intact patellar cartilage on the operative records of the control group.
Statistical Analysis
Summary statistics were calculated for demographic variables. Analysis of variance (ANOVA) tests with Bonferroni corrections were performed to compare continuous demographic variables between the 3 groups. Fisher exact tests were used to test for differences in the categorical variables between the 3 groups. Intraclass correlation coefficients were calculated to evaluate both intra- and interobserver reproducibility of the sTTTG measurement. These values were interpreted according to prior descriptions with >0.75 suggesting excellent reproducibility. 12 After confirming similar measurements, the mean of the 3 sTTTG measurements was used for further analyses. Comparisons between groups 1, 2, and 3 were made for the sTTTG and other radiographic measurements using ANOVA tests with Bonferroni corrections. All statistical analyses were performed using Stata (v14; College Station, TX). Significance was defined as P < 0.05.
Results
There were 17 patients who met inclusion and exclusion criteria for analysis in group 1. Patients in group 1 (PF cartilage repair group) were significantly younger than both groups 2 and 3 (meniscectomy groups) (group 1: 33.2 ± 9.6 years; group 2: 52.7 ± 8.7 years; group 3: 52.9 ± 9.4 years; P < 0.001 for group 1 vs group 2 and group 3) ( Table 1 ). There were no differences with regard to sex, height, weight, and BMI. The PF cartilage repair group was composed of 2 grade 2 lesions, 14 grade 3 lesions, and 10 grade 4 lesions. Treatment in group 1 consisted of an anteromedialization tibial tubercle osteotomy in 12 patients (64.7%), autologous chondrocyte implantation (ACI) to the patella in 10 patients (52.9%), trochlear ACI in 5 patients (29.4%), patellar chondroplasty in 4 patients (29.4%), and microfracture in 1 patient (5.9%).
Demographics.
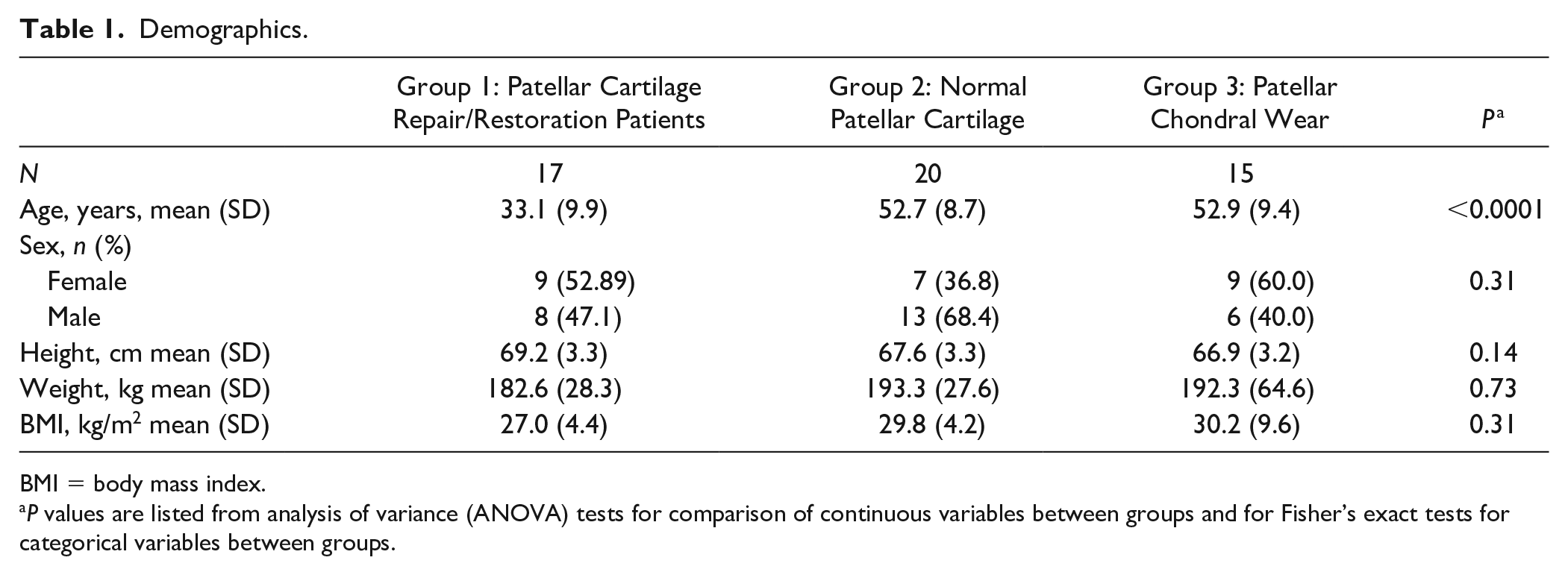
BMI = body mass index.
P values are listed from analysis of variance (ANOVA) tests for comparison of continuous variables between groups and for Fisher’s exact tests for categorical variables between groups.
The mean sTTTG was significantly more posterior in group 1 (5.9 ± 5.5 mm posterior to the trochlear groove) relative to group 2 (0.8 ± 5.3 mm posterior; P = 0.018) ( Table 2 ). The mean value for group 3 (2.7 ± 5.3 mm posterior) fell between groups 1 and 3 but was not significantly different from either group 1 (P = 0.31) or group 2 (P = 0.89). There were no significant differences between groups with regard to sulcus angle, CDI, TTTG, or knee flexion angle on the MRI scan. There was no correlation between knee flexion angle and sTTTG (Spearman’s ρ = −0.12; P = 0.40).
Radiographic Measurements.
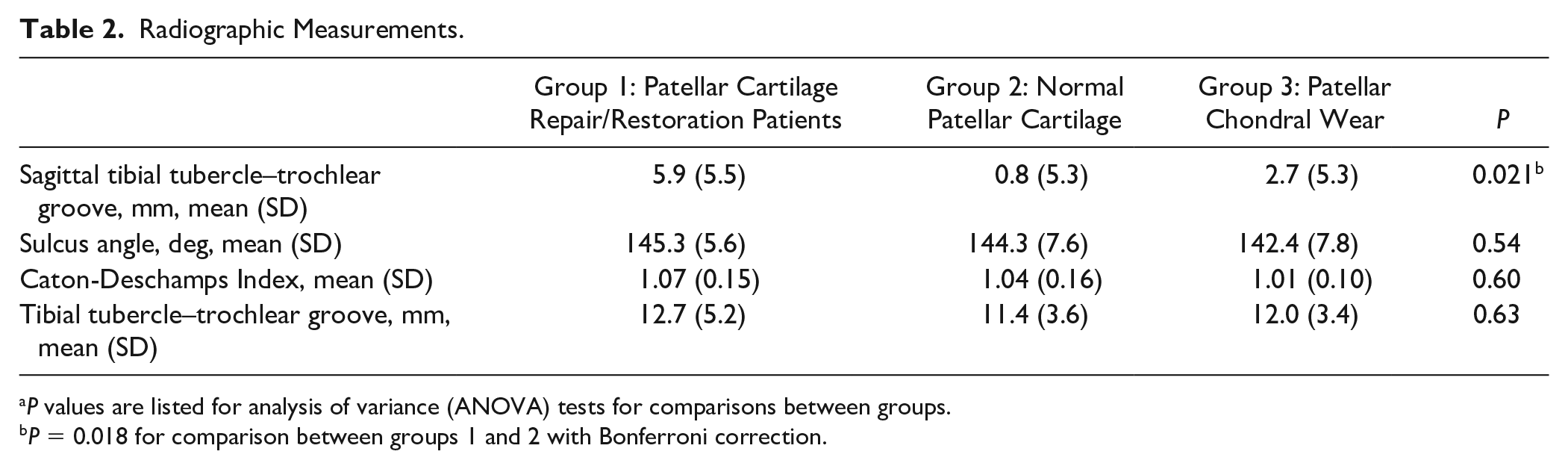
P values are listed for analysis of variance (ANOVA) tests for comparisons between groups.
P = 0.018 for comparison between groups 1 and 2 with Bonferroni correction.
The intraobserver reproducibility of the sTTTG measurement was 0.98 (95% confidence interval [CI] 0.96-0.99), which indicates excellent agreement between readings. Interobserver reproducibility was 0.90 (95% CI 0.78-0.95), also indicating excellent agreement.
Discussion
The sTTTG groove distance was significantly larger in patients with isolated PF chondral lesions relative to a control group with arthroscopically-verified normal patellar cartilage. This difference represents a more posteriorly aligned tubercle relative to the trochlea, which may correspond with increased joint reactive forces at the patellofemoral articulation. This measurement of potential sagittal overload may be important for surgeons to consider when treating patients with PF chondral abnormalities.
The PF joint and extensor mechanism are complex biomechanical systems. While it is understood that the patella acts as a dynamic fulcrum of the extensor moment, a multitude of factors that have been previously described can affect the extensor moment and patellofemoral contact pressures. 13 These include sagittal measurements such as the patella–patella tendon (P-PT) angle, patella alta (as measured with Insall Salvati or CDI), anterior-posterior thickness of the patella, and patellar morphology.14-17 However, it is unclear how all these factors relate to one another and ultimately to increased patellofemoral contact pressures. Our results showed no differences in CDI measurement between groups, suggesting that this sagittal measurement is not associated with sTTTG. Although not explored within this study, theoretically a posterior tibial tubercle as described by group 1 would decrease the P-PT angle and increase patellofemoral contact pressures. Future studies will be needed to explore the relationship between sTTTG and other sagittal measurements that can affect patellofemoral joint biomechanics.
Alterations of patellofemoral contact pressure can be addressed with tibial tubercle osteotomy procedures. The anteromedialization osteotomy is commonly performed to treat PF chondral lesions, patellar instability, and PF arthritis.18-20 Displacing the tibial tubercle anteriorly results in decreased mean and maximum contact pressure across the patellofemoral joint. 21 Mean contact pressures decrease throughout a full range of knee flexion, while also shifting the cartilage contact point medially. 22 Maquet 10 reported that displacing the tubercle anteriorly by 2 cm results in 50% decrease in force across the patellofemoral articulation in early flexion, while Bandi 23 described 26% reduction in compression force with 1 cm anterior displacement. Trochlear contact pressures decrease significantly with a direct anteriorization osteotomy. 24 Cohen et al. 25 demonstrated that simulated contact stresses after tibial tubercle transfer procedures are variable between patients. The degree of medialization is often modified based on the magnitude of lateralization of the tubercle, though an anatomic measurement to guide the degree of anteriorization is not routinely used. This sTTTG measurements may allow for more precise preoperative measurement and tailored osteotomy based on the individual bony anatomy.
Tanaka et al. 26 recently reported a similar measurement with relation to patients with patellofemoral instability. They found that patients with symptomatic patellofemoral instability have a significantly more posterior tibial tubercle with a mean value of almost 9 mm. Similar to our control group, they reported a near-zero value for patients with asymptomatic knees (−0.5 mm in their study relative to 0.8 mm in our study). This sTTTG measurement is likely important for both patients with PF cartilage lesions and PF instability.
Patients treated with anteromedialization with and without cartilage restoration report high levels of satisfaction and excellent outcomes. The osteotomy plane may be varied to allow for differential amounts of anterior and medial translation. General recommendations for the magnitude of anteriorization range from 10 to 15 mm, limited by skin problems and patellar tilt caused by excessive anterioirization.27-29 This 1 cm anteriorization is supported by findings from Nakamura et al. 30 that demonstrate the contact stress areas in the PF joint shows minimal changes for a 1 cm anteriorization but decrease with greater degrees of anterior displacement. The results of the current study highlight the differential sagittal alignment of the tibial tubercle and may point to this measurement as a key factor to consider in osteotomy planning. However, there was a range of values for the sTTTG measurement in the group with patellar chondral lesions.
Changes in tibiofemoral alignment influence loading of the patellofemoral joint. Posterior cruciate ligament injuries result in a posterior translation of the tibia relative to the femur and lead to both PF pain and accelerated degenerative changes at the PF articulation.31,32 The insertion of the patellar tendon, as observed in the current study, occurs at a variable location relative to the sagittal axis of the tibia. A more posteriorly positioned tibial tubercle was observed in the group with isolated patellar chondral defects, suggesting that these patients experience greater contact forces across the patellar cartilage. While there appears to be a relationship between this measurement and the presence of a patellofemoral cartilage defect, there is a wide range of morphologic variability at the PF joint. Trochlear dysplasia is an important factor in both patellar instability and PF cartilage defects.33,34 Patellar shape has been studied extensively with inconclusive relationships between the Wiberg classification and chondral injury. 35 Patellar height is also an important determinant of PF kinematics and may influence cartilage wear.17,36 The sTTTG does appear to be an additional important contributor to development of PF cartilage defects.
This study should be interpreted with a clear understanding of potential limitations. First, this is a retrospective review of a relatively small cohort and we did not associate the sTTTG measurement with postoperative clinical outcomes. The small sample size and differences between groups are major limitations of this study. Our control group was selected to include patients with arthroscopically confirmed intact patellar cartilage. This cohort is significantly older than the group with patellar chondral lesions, though in some ways this difference may even strengthen our observations, as the control group has preserved patellar cartilage despite an additional 2 decades of potential wear. We also cannot definitively say that the patients in the control group will not have patellar cartilage lesions in the future, as we observed only a single time point. We specifically excluded patients with prior patellar instability to remove the possibility of traumatic chondral injuries. The sTTTG measurement may also be subject to variations in knee positioning at time of imaging. The TTTG distance does vary with knee flexion. 37 We excluded patients with greater than 10° of knee flexion on MRI scan and observed no correlation between knee flexion and the sTTTG measurement in this data set. The sTTTG measurement is subject to change with tibial alignment relative to the femur, including in the setting of ACL or PCL injury with anterior or posterior tibial translation, respectively. Other conditions, such as trochlear dysplasia or a history of Osgood-Schlater’s disease, may alter this measurement. We did also observe variation in this measurement within groups, as evidence by the standard deviation of approximately 5 mm in each group. This variation could be because the sTTTG measurement is an absolute measurement and could therefore be affected by body size or joint size. Prior studies of TTTG measurements have found that joint size, but not body size, affects this measurement.38,39 Future studies are needed to analyze if the sTTTG measurement has similar relationships. Finally, in this study, we are unable to measure such factors as relative quadriceps, hamstring, and hip abductor strength, as well as patellar size and other measures of PF biomechanics, which may influence force across the PF joint.
Conclusions
In conclusion, the sTTTG measurement may provide important information regarding the sagittal balance of the patellofemoral joint. On average, a more posteriorly positioned tibial tubercle was observed in patients with patellar cartilage lesions relative to those with intact patellar cartilage. Intermediate positioning was observed in patients with asymptomatic patellar chondral wear.
Footnotes
Authors’ Note
Investigation performed at Rush University Medical Center.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drew A. Lansdown received fellowship-related educational support from Smith & Nephew and Arthrex, Inc., and hospitality-related payments from Tornier/Wright. Jack Farr is a paid consultant for and receives research support from Active Implants; is on the editorial or governing board of the American Journal of Orthopedics; receives IP royalties and is a paid presenter or speaker for Arthrex, Inc.; is a paid consultant for Cartiheal; is on the editorial or governing board of Cartilage; is a paid consultant for Exactech; receives research support from Fidia; has stock or stock options in MedShape, Inc., is a paid consultant for, receives research support from, and is a paid presenter or speaker for Moximed; receives research support from Norvartis; is a paid consultant for, is a paid presenter or speaker, and receives IP royalties from Organogenesis; has stock or stock options in Ortho Regenerative Tech, Inc.; is a paid consultant for Regentis; is a paid consultant for Samumed, Inc.; receives publishing royalties, financial or material support from Springer and Thieme Medical Publishers, Inc.; is a paid presenter or speaker for Vericel; receives research support from ZimmerBiomet; and is a paid consultant for Zipline. Brian J. Cole receives research support from Aesculap/B. Braun; is on the editorial or governing boards of the American Journal of Orthopedics and the American Journal of Sports Medicine; receives IP royalties, is a paid consultant, and receives research support from Arthrex, Inc.; is a board or committee member of the Arthroscopy Association of North America; receives other financial or material support from Athletico; is on the editorial or governing board of Cartilage; receives IP royalties from Elsevier Publishing; is a board or committee member of the International Cartilage Repair Society; is editor only and is on the editorial or governing board of the Journal of Shoulder and Elbow Surgery and the Journal of the American Academy of Orthopaedic Surgeons; receives other financial or material support from JRF Ortho; receives research support from the National Institutes of Health (NIAMS & NICHD); receives publishing royalties, financial or material support from Operative Techniques in Sports Medicine; has stock or stock options in Ossio; is a paid consultant for, receives research support from, and has stock or stock options in Regentis; and receives other financial or material support from Smith & Nephew. Adam B. Yanke receives research support from Arthrex, Inc., and Organogenesis, and is a paid consultant for JRF Ortho.
Ethical Approval
All procedures were approved by our institutional review board.
Informed Consent
Not applicable.
Trial Registration
Not applicable.