
Abstract
Background:
Secondary meniscal tears are a well-described sequela of delay in anterior cruciate ligament (ACL) reconstruction (ACLR) after ACL injury. This study aimed to evaluate whether preoperative conservative interventions (ie, crutches, bracing, and physical therapy) are associated with a reduced risk of secondary meniscal pathology in pediatric patients.
Hypothesis:
Preoperative conservative interventions of the ACL-deficient knee would be associated with fewer secondary meniscal tears in pediatric patients undergoing delayed (≥8 weeks postinjury) ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All pediatric patients (age, <18 years) undergoing primary ACLR with a single surgeon between October 1, 2013, and January 31, 2022, were retrospectively identified. The exclusion criteria were as follows: previous ipsilateral knee injury; multiligamentous knee injuries; or time frommagnetic resonance imaging to surgery ≥52 weeks. Adherence to conservative management recommendations (ie, crutches, bracing, and physical therapy) was assessed through medical record review. Secondary meniscal injuries were defined as major tears that were discovered intraoperatively and required repair or substantial meniscectomy. Meniscal tears that occurred concomitantly with ACL rupture and were detectable on the initial (<3 weeks after injury) magnetic resonance imaging scans were not considered secondary. In total, 71 pediatric patients (35 girls; 36 boys) were included.
Results:
A total of 70 patients (99%) underwent ≥1 conservative interventions before ACLR—including 37 (52%) who used crutches, 47 (66%) who used bracing, and 69 (97%) who received physical therapy. There were no differences in use of conservative interventions between those who underwent early ACLR and those who had delayed ACLR (P > .05). Delayed ACLR was associated with a greater risk of medial, but not lateral, meniscal tears compared with early ACLR (P = .04). Overall, 15 secondary meniscal tears were observed intraoperatively in 14 patients—including 4 medial and 11 lateral tears. Knee bracing was associated with fewer lateral meniscal tears in patients undergoing early ACLR (6% vs 35%; P = .008), with multivariate regression analysis yielding an adjusted odds ratio of 0.06 (95% CI, 0.006-0.57; P = .015). The use of crutches was associated with fewer medial meniscal tears in patients undergoing delayed ACLR (0% vs 37%; P = .017). Since no new medial meniscal tears were observed in patients who used crutches, the adjusted odds ratio could not be calculated.
Conclusion:
Bracing and crutches were associated with the preservation of the menisci in the ACL-deficient knee in pediatric patients undergoing early and delayed ACLR, respectively. Surgeons should strongly encourage adherence to these conservative modalities in patients awaiting operative reconstruction to reduce the risk of secondary meniscal pathology.
Keywords
Anterior cruciate ligament (ACL) rupture is one of the most common sports injuries in the pediatric population, and it has increased by 2% annually over the past 20 years. 3 While isolated ACL tears represent a large proportion of these injuries, meniscal tears often occur simultaneously. 9 Further, loss of structural support from the ACL confers excessive translational stress onto the menisci, greatly increasing the risk of secondary meniscal tears in the postinjury period.2,16,18
Delayed ACL reconstruction (ACLR) has been strongly associated with a higher risk of secondary meniscal pathology in patients of all ages.12,14,17,20,31 Importantly, patients who develop meniscal injuries after ACL rupture experience worse long-term outcomes—including a greater incidence of early onset osteoarthritis and inability to return to sports.7,8,21,26 Historically, definitive surgical reconstruction was often purposefully delayed to allow for physeal maturation in skeletally immature patients, as early operative intervention may lead to angular deformity or leg-length discrepancy caused by physeal disruption.1,4,19,28,29 With the adoption of physeal-sparing techniques, it is now rarely necessary to delay ACLR until skeletal maturity, but delays still occur because of patient, surgeon, and medical resource factors. Therefore, protecting the ACL-deficient knee in the interim between initial injury and surgical reconstruction remains a pertinent challenge, especially in the pediatric population. 15
Although it is standard practice to impose activity and sports limitations after ACL injury, conservative interventions—such as bracing and crutches—are recommended primarily on an as-needed basis to treat pain or instability in patients with planned reconstruction.10,24 Therefore, the value of these conservative modalities in bridging patients from injury to surgery remains incompletely understood. This study aimed to evaluate whether initial conservative intervention is associated with a lower risk of secondary meniscal injury in pediatric patients with ACL tears awaiting definitive ACLR. We hypothesized that patients who undergo delayed ACLR but are prescribed conservative management strategies before surgery would experience a lower incidence of secondary meniscal tears.
Methods
Ethical Approval
Approval for this retrospective cohort study was obtained from our institutional review board.
Patient Selection and Data Extraction
We searched electronic medical records from our academic tertiary care center to identify all pediatric patients (<18 years) who underwent primary ACLR (Current Procedural Terminology code 29888) for a grade 2 or 3 Lachman test, with a single surgeon (R.J.L.) between October 1, 2013, and January 31, 2022. Demographic and injury characteristics extracted included age, sex, body mass index (BMI), and ACL injury laterality. In the senior author’s practice (R.J.L.), all patients are required to undergo at least 1 physical therapy session before ACLR, whereas crutches and bracing are offered as optional modalities. Use of conservative management strategies (ie, crutches, bracing, and physical therapy) before surgery was assessed through medical record review.
We reviewed initial magnetic resonance imaging (MRI) scans (<3 weeks after injury) for the presence or absence of meniscal tears at the time of injury. All MRI scans were interpreted by a single board-certified pediatric orthopaedic surgeon (R.J.L.) to control for interoperator variability. Dictated operative reports were subsequently reviewed to determine the presence or absence of meniscal tears visualized arthroscopically at the time of surgery. Secondary meniscal injuries were therefore defined as major tears that were discovered intraoperatively but not detected on the patient’s initial MRI scan. Despite being the “gold standard” for intra-articular soft tissue evaluation, MRI does not have perfect sensitivity (78%-89%) or specificity (88%-95%) for meniscal tears. 27 Thus, we disregarded minor pathology that was discovered intraoperatively (defined as mild fraying or tears requiring meniscectomy of <25% of the width of the meniscus) but may have been missed on the initial MRI.
We excluded patients with a history of an ipsilateral knee injury, an unknown date of injury, an unknown MRI date or findings, time of MRI to surgery ≥52 weeks, an MRI date of >3 weeks postinjury, polytraumatic (ie, intra-articular fracture, dislocation) injuries, or multiligamentous knee injuries. In total, 81 patients were excluded—including 33 with a previous ipsilateral knee injury, 18 with unknown injury date, 18 with MRI scans performed >3 weeks after the initial injury, 3 with incomplete MRI data, and 8 with polytrauma or multiligamentous knee injury, and 1 with congenital ACL absence.
In total, 71 pediatric patients were included (Table 1). There were 35 (49%) girls and 36 (51%) boys. The mean (± SD) age at surgery was 14.9 ± 1.8 years. A power analysis demonstrated that a total sample size of 68 would be sufficient to detect a 20% difference between groups with 80% power (beta-risk = 0.2) at an alpha level of .05.
Demographic, Injury, and Treatment Characteristics a
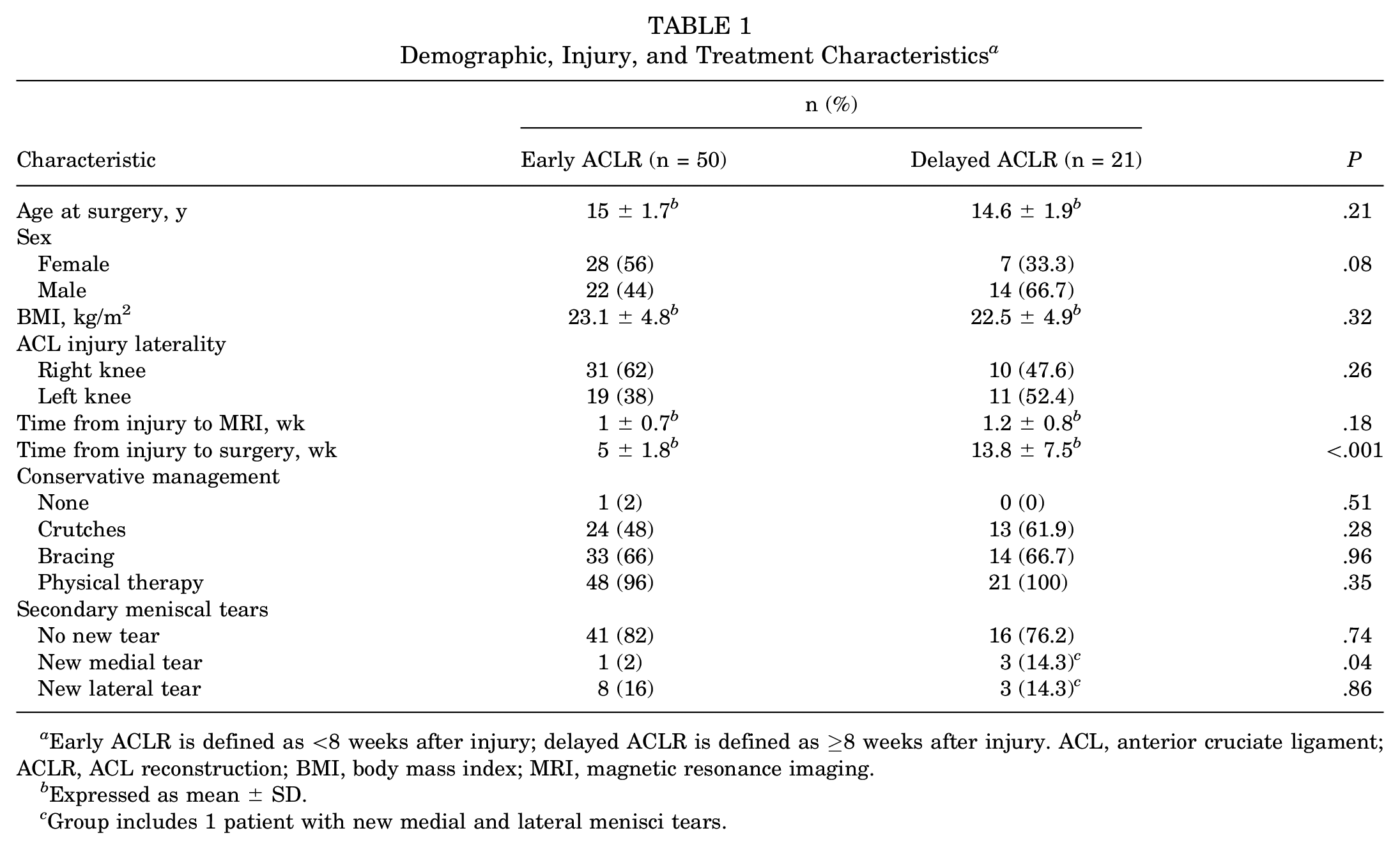
Early ACLR is defined as <8 weeks after injury; delayed ACLR is defined as ≥8 weeks after injury. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; BMI, body mass index; MRI, magnetic resonance imaging.
Expressed as mean ± SD.
Group includes 1 patient with new medial and lateral menisci tears.
Definitions and Primary Outcome
Operative delay was defined as ACLR performed ≥8 weeks after injury. The primary outcome was new secondary meniscal injuries, defined as major tears discovered intraoperatively but not detected on the initial (<3 weeks postinjury) MRI scan. Major meniscal tears were defined as those that required repair or substantial meniscectomy (>25% of the width of the meniscus).
Statistical Analysis
We compared the incidence of secondary meniscal tears in patients who underwent early ACLR with those who underwent delayed ACLR. Subsequently, we analyzed the association between each type of conservative intervention (eg, crutches, bracing, and physical therapy) and the risk of secondary meniscal tears. Since some patients used multiple conservative interventions, the analyses for each modality were conducted independently (eg, patients who used bracing were compared with patients who did not use bracing, regardless of crutch use). After stratifying patients based on ACLR timing, we repeated the analysis. Separate analyses were conducted for medial tears, lateral tears, and combined medial and lateral tears. Student t tests and Pearson chi-squared tests were used for univariate analysis of continuous and categorical variables, respectively. Multivariate logistic regression was performed to calculate the adjusted odds ratio of secondary meniscal tears after conservative treatment while controlling for age, sex, BMI, and time to MRI. The significance level was determined at α = .05. All analyses were performed with Stata statistical software, release 17 (StataCorp LLC).
Results
Patient Injury and Operative Characteristics
Of the 71 pediatric patients in the study, 50 (70%) underwent early ACLR, with a mean (SD) time of 5 ± 1.8 weeks from injury to surgery (Table 1). A total of 21 patients (30%) underwent delayed ACLR, with a mean time of 13.8 ± 7.5 weeks from injury to surgery. The mean time from injury to initial MRI scan was 1 ± 0.7 weeks and did not differ significantly between the early and delayed ACLR groups (P = .18). Also, 70 patients (99%) underwent initial conservative management before reconstruction—including 37 (52%) who used crutches, 47 (66%) who used bracing, and 69 (97%) who received physical therapy. There were no differences in the use of conservative interventions between the early and delayed ACLR groups (all P >.05). Overall, 15 secondary meniscal tears were observed intraoperatively in 14 patients—including 4 medial and 11 lateral tears. On bivariate chi-squared analysis, delayed ACLR was associated with a greater risk of secondary medial but not lateral meniscal tears compared with early ACLR (P = .04).
Conservative Interventions Before Early ACLR
Among patients who underwent early ACLR, knee bracing was associated with a lower overall incidence of new meniscal tears 9% (3/33) compared with 35% (6/17) among those without bracing. Specifically, bracing was associated with significantly fewer lateral meniscal tears—6% (n = 2) versus 35% (n = 6) (P = .008) (Figure 1). After controlling for age, sex, BMI, and time to MRI in a multivariate logistic regression model, the adjusted odds ratio of secondary lateral meniscal tears after knee bracing was 0.06 ([95% CI, 0.006-0.57]; P = .015). No difference was observed in the incidence of medial meniscal tears with any intervention.
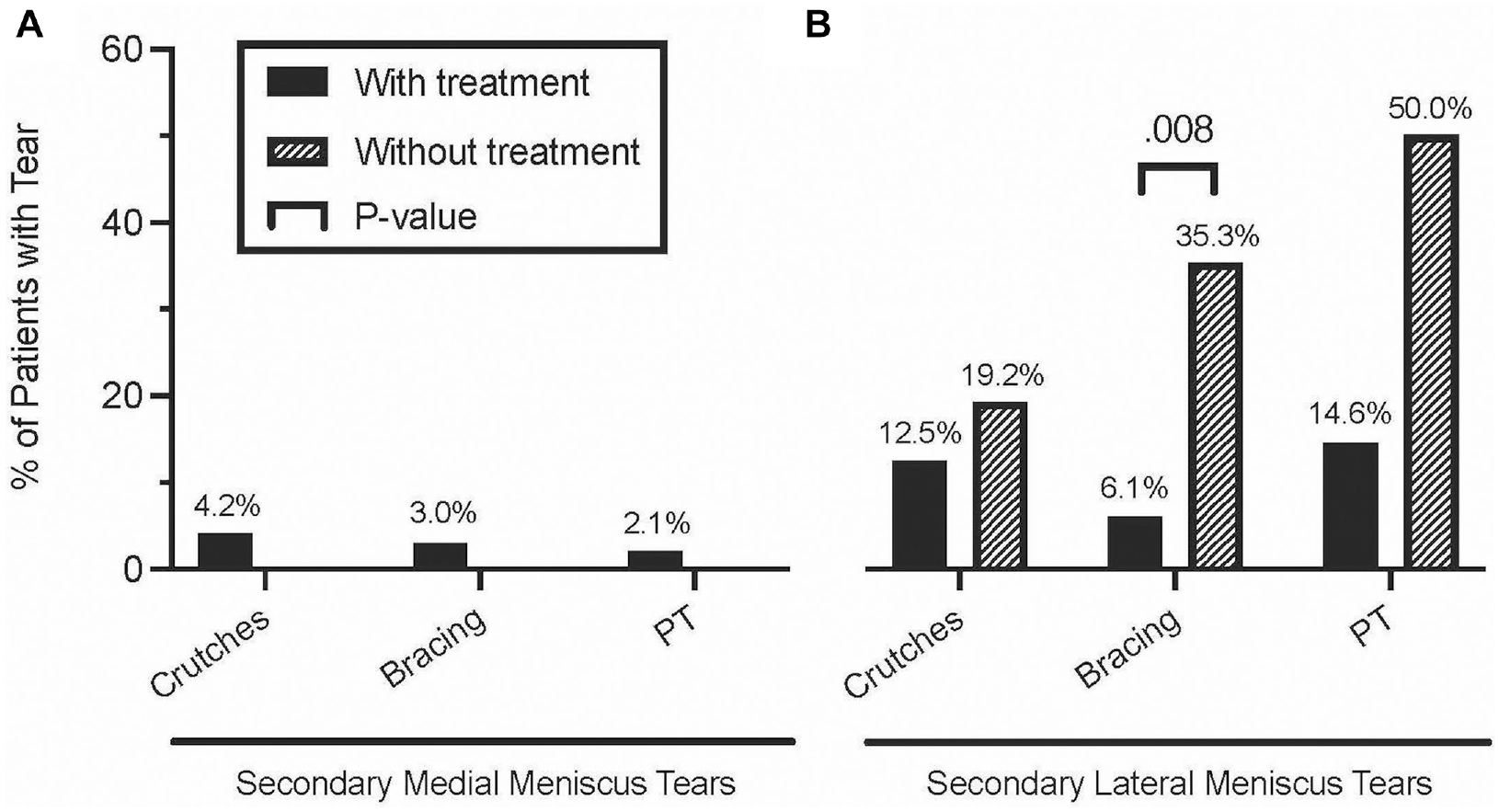
The incidence of secondary (A) medial meniscal tears and (B) lateral meniscal tears with or without conservative management before early ACLR (<8 weeks after injury). ACLR, anterior cruciate ligament reconstruction; PT, physical therapy.
Conservative Interventions Before Delayed ACLR
Among patients who underwent delayed ACLR, the use of crutches was associated with a lower overall incidence of new meniscal tears—8% (1/13) compared with 62% (5/8) without crutches. Specifically, crutches were associated with significantly fewer medial meniscal tears—0% (n = 0) versus 37% (n = 3) (P = .017) (Figure 2). Since no new medial meniscal tears were observed in patients who used crutches (0/13), an adjusted odds ratio could not be calculated. Interestingly, knee bracing was not associated witht the risk of medial or lateral meniscal tears. No control group was available for physical therapy in the delayed ACLR cohort.

The incidence of secondary (A) medial meniscal tears and (B) lateral meniscal tears with or without use of conservative management before delayed ACLR (≥8 weeks after injury). NA indicates that no control patients were available in this cohort (ie, did not receive PT). ACLR, anterior cruciate ligament reconstruction; PT, physical therapy.
Discussion
In our study, knee bracing was associated with a lower risk of lateral meniscal tears in patients undergoing early ACLR (6% with bracing vs 35% without bracing), and the use of crutches was associated with a lower risk of medial meniscal tears in patients undergoing delayed ACLR (0% with crutches vs 37% without crutches). These findings suggest that protection of the knee joint with bracing and/or crutches immediately after ACL rupture is effective in preserving the menisci, even in patients with planned early surgical reconstruction.
Numerous studies have shown that nonoperative treatment alone is insufficient for complete ACL rupture, leading to poor functional outcomes and ongoing instability, especially in patients returning to high-level sports.11,23,25,30 However, the value of conservative interventions in bridging patients from injury to surgery is incompletely understood. Only 1 study, by Kolin et al, 18 has examined this question, finding that crutches were associated with a lower risk of medial and lateral meniscal tears (adjusted relative risk, 0.47 [95% CI, 0.34-0.64] and 0.67 [95% CI, 0.54-0.84], respectively). However, the authors’ analysis was limited by the fact that they did not isolate patients with intact menisci on postinjury MRI; it is, therefore, unclear which meniscal lesions occurred during the initial injury versus which lesions developed secondarily. In 2004, Woods and O’Connor 32 published the results of a protocol involving bracing (in addition to rehabilitation exercises and strict abstinence from sports) to permit the delay of reconstruction until skeletal maturity, but their control group consisted of patients who underwent early reconstruction. They did not directly compare the risk of secondary meniscal injury to patients who underwent delayed reconstruction without interim bracing.
Although it is standard practice to impose activity modifications after ACL injury, bracing and crutches are often optional for patients with planned reconstruction.10,17 Indeed, in our study, only 52% of patients used crutches, and 66% used bracing. The data here suggest that bracing and crutches do have value in reducing the risk of secondary meniscal injury. Although we did not include long-term follow-up in this study, the preponderance of evidence in the literature demonstrates that secondary meniscal injury after ACL rupture is strongly associated with worse clinical outcomes—including chondral degeneration, early-onset osteoarthritis, recurrent instability, and inability to return to preinjury activity levels.12,18,27,28 Moreover, adherence to nonoperative interventions likely discourages premature return to sports, which is a major independent risk factor for the development of secondary intra-articular derangement. 22 In fact, restriction of activity level is likely a key indirect benefit of protected weightbearing with bracing/crutches since exact patient activity level could not be controlled in this nonrandomized study. However, it is unclear whether the clinical benefit observed was due to alterations in the biomechanics of the ACL-deficient knee joint or simply due to activity restriction. Nevertheless, the findings of our study underscore the importance of bracing and crutches after ACL rupture, and surgeons should offer these conservative modalities to patients awaiting operative reconstruction.
The differential effect of bracing and crutches in patients undergoing early and delayed ACLR, respectively, may be explained by what is already known about the biomechanics of the knee joint. Several studies have shown that lateral meniscal tears are typically seen early in the postinjury period, whereas medial meniscal tears are a consequence of chronic ACL deficiency.2,6,13 It follows somewhat logically that the modality with the greatest benefit to patients undergoing early ACLR (ie, bracing) reduces the risk only of lateral meniscal tears because medial meniscal tears do not occur until later. Conversely, the modality with the greatest benefit to patients undergoing delayed ACLR (ie, crutches) should reduce the risk of medial meniscal tears.
The medial meniscus serves as a secondary stabilizer against anterior translation of the tibia and therefore endures excessive translational stress after ACL injury, a likely contributor to medial meniscal tears in the ACL-deficient knee. 2 However, in a biomechanical study of chronically ACL-deficient knees, Beynnon et al 5 reported that functional bracing was not effective in reducing the abnormal anterior translation of the tibia relative to the femur when transitioning from nonweightbearing to weightbearing postures. This may explain why, in our study, bracing provided negligible protection of the medial meniscus.
Limitations
There are several limitations to our study. First, the sample size was small (n = 71) and the sample included only pediatric patients, which may limit the generalizability of the findings. Second, selection bias may be present, because patients with more pain and instability would, in theory, be more likely to use crutches and/or bracing. However, if present, this bias would make it more likely to observe meniscal tears in patients who opt to use conservative interventions because such patients would be more likely to have more severe injuries. Therefore, this limitation would not undermine the finding of a lower risk of meniscal tears in patients who used bracing or crutches. (If anything, it might mask the magnitude of the benefit.) Third, any delays in ACLR at the senior author’s practice are typically due to patient preference or availability; thus, patients with more pain and instability may choose to undergo definitive surgical intervention sooner than those with milder symptoms. Fourth, although we used detailed, systematically recorded clinical notes to evaluate adherence to conservative treatments, this information is ultimately based on patients’ narrative accounts and therefore may be inaccurate. In addition, it does not detail the exact patient activity level. However, bracing and crutches are typically prescribed on an as-needed basis, and patients have little incentive to be untruthful about their use of these modalities. Fifth, MRI has imperfect sensitivity (78%-89%) and specificity (88%-95%) for the detection of meniscal tears. 27 To address this, we selectively ignored minor pathology discovered intraoperatively that might have been missed on the initial MRI. Sixth, the presence or absence of meniscal tears on initial postinjury MRI was assessed in a binary fashion; thus, worsening meniscal tears would not be captured in this analysis. Last, different definitions of operative delay are possible. Given that the mean time from injury to surgery in our sample population was 7.6 weeks, we chose a threshold of 8 weeks; our findings might differ with longer or shorter periods of operative delay.
Conclusion
This study aimed to determine whether preoperative conservative interventions were associated with a reduced risk of secondary meniscal pathology in the pediatric ACL-deficient knee. We found that knee bracing was associated with a lower risk of lateral meniscal tears in patients undergoing early ACLR, whereas the use of crutches was associated with a lower risk of medial meniscal tears in patients undergoing delayed ACLR. Our findings suggest that protection of the knee joint by limiting mobility and weightbearing activity immediately after ACL rupture is effective in preserving the menisci, even in patients with planned surgical reconstruction. Surgeons should therefore offer these conservative modalities to pediatric patients awaiting operative reconstruction.
Footnotes
Acknowledgements
The authors thank Sandra Crump, MPH, in the Editorial Services group of The Johns Hopkins Department of Orthopaedic Surgery, for editorial assistance.
Final revision submitted July 22, 2024; accepted August 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.J.L. has received research support from Vericel and education support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Johns Hopkins Medicine (IRB00301240).